
Abstract
Over the past 20 years a range of community-based housing options has emerged in Australia to meet the needs of individuals with varying levels of psychiatric disability. These tend to reflect a continuum of service intensity from independent living arrangements to residential facilities with 24 hour staffing (such as community care units in Queensland and Victoria). Within this array of service provision, supported accommodation is becoming increasingly popular for those with more severe problems. The approach combines stable housing and clinical services with the added ingredient of ‘in home’ support provided by visiting workers, typically employed through the non-government (NGO) sector. These ‘non-clinical’ support staff work in collaboration with mainstream mental health services and assist people to access required services in their local community, manage day to day living activities and sustain their tenancies.
While most states in Australia have established some form of supported accommodation, there has been a paucity of research on the outcomes of such programmes. One exception has been the evaluation of the Housing and Support Initiative (HASI) in New South Wales [1]. HASI is based on a three-way partnership between NSW Health, the Department of Housing and the non-government sector. Stage one of the programme provided support to 100 people with high levels of disability. A follow-up evaluation found that while the programme produced improvements in physical and psychological health, the most significant outcome was a 90% decrease in inpatient bed days for those individuals enrolled in the programme. However, it is possible that more functional clients were selected for the programme and there may have been inconsistencies in the way the programme was established across the state.
Studies conducted overseas also demonstrate that clients in supported accommodation tend to have fewer readmissions to hospital and fewer days in inpatient care once admission becomes necessary [2]. Those studies that did evaluate other domains such as symptoms and clinical functioning found that these components were unlikely to improve despite the increase in service intensity [2–3]. While there was a trend for general functioning such as Activities of Daily Living (ADLs) and self-care to improve, the extent of this improvement did not reach significance in the studies reviewed. Indeed, social networks tended to decline following the introduction of support services as support staff replaced some of the functions provided by family and friends.
The present study was designed to assess the clinical and social outcomes for 181 individuals with psychiatric disability in the 7 year period since joining Project 300, a state-wide supported accommodation programme in Queensland.
Project 300
Project 300 was established in Queensland in 1996 with the aim of relocating (from the three stand-alone hospitals) 300 long-stay clients to their community of origin or choice. However, only 194 clients were relocated in the initial phase of the programme and these form the study group for the current evaluation. (It should be noted that the remaining 106 clients have since been relocated in two subsequent phases of the programme.) Many of the individuals enrolled in Project 300 had tried unsuccessfully to re-enter the community under previous hospital downsizing schemes. While clinical support was provided through normal case management services and/or shared care with local general practitioners, non-clinical support was provided through the non-government sector.
Method
The study employed a repeated measures longitudinal design. Data concerning changes in clinical, social and vocational outcomes were collected prospectively from the same clients 6 weeks prior to discharge and again at 6, 18, 36, and 84 months post-discharge. Clients were discharged into the programme over a period of 4 years (1996–1999) and followed up by a trained research assistant on the anniversary of their entry into the programme. Data were collected using a battery of standardized measures completed by case managers and through individual interviews with a research assistant. Information concerning the level of disability support provided (i.e. hours per week) was supplied for each individual by the agencies providing such support. The evaluation was approved by the relevant ethics committees in each of the health service districts concerned.
Client group
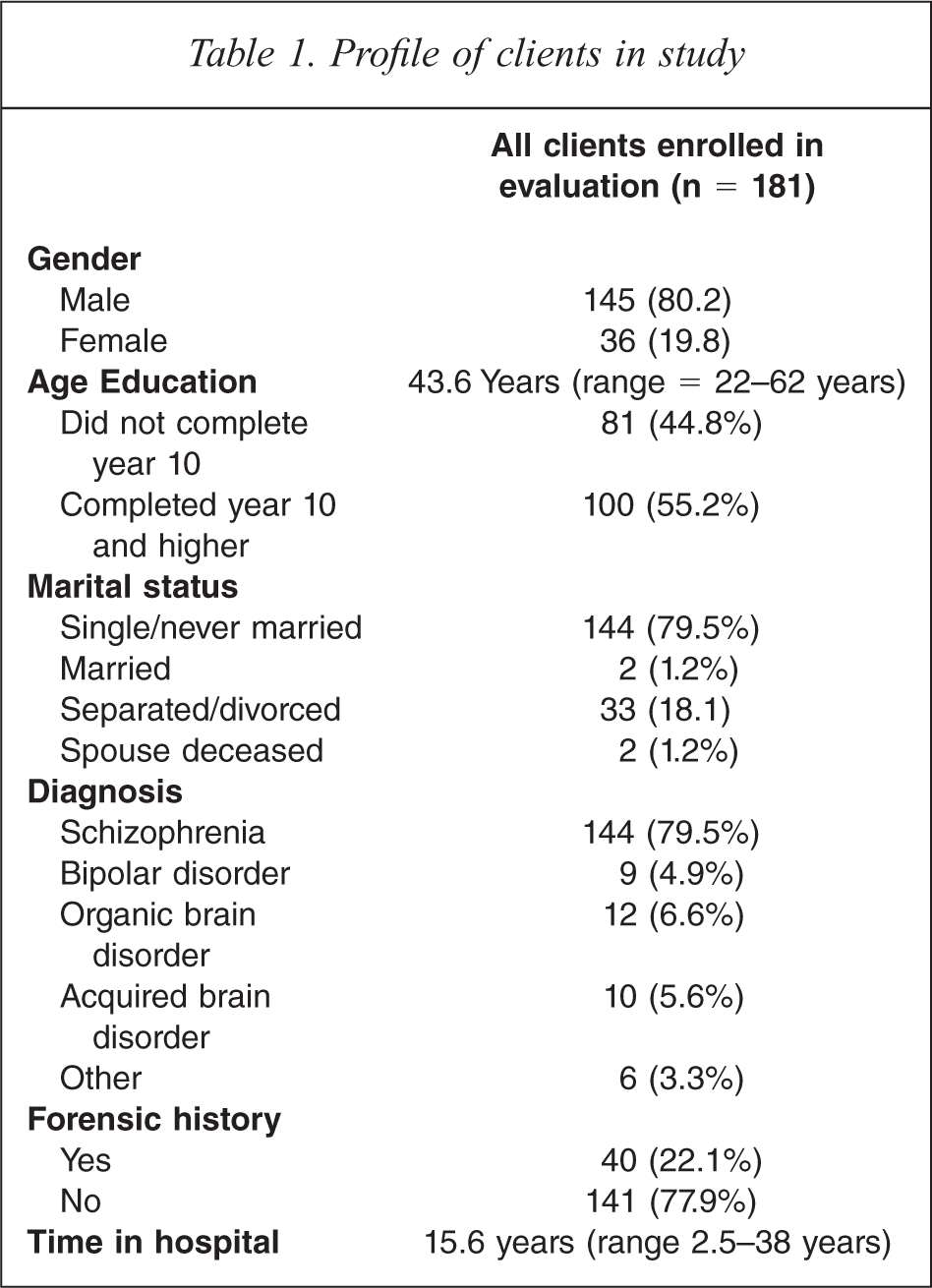
The target group for Project 300 was long-stay clients who had resided in the three stand-alone psychiatric hospitals in Queensland. Some 300 clients were identified as being potentially suitable for discharge (hence the title ‘Project 300’). However, only 194 of the 300 clients were actually discharged. The costs of providing the disability support component were not indexed to inflation and no provision was made for increases in the cost of support services. In addition, while efforts were made to keep allocated support hours below a maximum of 53 hours per consumer per week, 25 of the 194 packages exceeded this due to the severity of disability in the target group. Of the 194 clients discharged, 181 were enrolled in the study. Four left hospital prior to providing consent, three moved to remote locations which made contact prohibitive and six refused to participate. While 89% of the clients enrolled in the programme had resided in hospital for at least the last two years prior to entering the programme, the total time spent (not continuously) in hospital ranged from 2.5 to 38 years (Table 1). The profile of the present sample (male, never married and having a diagnosis of schizophrenia) was in line with that of other long-stay cohorts described in previous resettlement studies in Australia [4] and overseas [5].
Profile of clients in study
Results
The findings presented in this report are mostly descriptive and provide an overview of the main outcomes for the cohort in the initial 7 years since entering Project 300.
Readmissions to long-term care
Nine of the 181 clients in the study sample (4.9%) had been readmitted to long-term care over the 7 year study period. Five of these (2.7%) had returned to their original hospitals and four (2.2%) had been admitted to community care units. In addition, four clients (2.2%) had been admitted to nursing homes due to physical ill health. Only two of the 181 clients followed up had spent a brief period in prison; one for threatening another individual with a knife and one for assaulting a police officer.
Readmissions to acute inpatient care
Almost one third (31.1%) of those discharged had spent time in an acute inpatient unit by 6 months post-discharge. This had increased to 60.2% by 7 years post-discharge. The finding that half of those admitted to acute care had been admitted in the first 6 months suggests that the most turbulent period was during the initial 6 months when clients were adjusting to life in the community. The number of admissions ranged from 1 to 13 with 76% of those who required acute care having only one admission to acute care by 7 years. Unfortunately, data concerning the number of days spent in acute care was too unreliable to be considered for the evaluation.
While 60% required acute inpatient care, 40% did not. This is a remarkable result, given that all of the clients had spent the 2 year period prior to Project 300 in a psychiatric hospital and were unable to be successfully discharged through other downsizing programmes.
Clients deceased
Nineteen of the 181 clients followed up (10.5%) died over the 7 year study period, four (2.2%) in the first year post-discharge. The majority of deaths resulted from carcinoma of the lungs and cardiovascular disease, conditions associated with long histories of cigarette smoking and inactivity while in hospital. Three of the 19 committed suicide (all males) and one died in a sporting accident. Suicide did not appear to be related to discharge since the first suicide occurred in a client who had been living in the community for 11 months.
Changes in the intensity and frequency of non-clinical support provided
Data concerning the number of hours of non-clinical support required each week to maintain individuals in their community residence was obtained from the 19 support agencies involved. Support agencies were asked to provide details of the actual hours of support provided directly to the client (in the week the clinical and other measures were completed). The number of hours of direct support provided each week decreased significantly from 26.3 h per person at 6 months post-discharge to 21.5 h at 7 years (F = 5.45, df = 116, p = 0.002). The decrease in support required was not consistent over the study period (Table 2). While there was a decrease of 4.1 h between 6 months and 18 months, the decrease between 18 months and 84 months was 0.9 h. The hours of support provided to individuals varied considerably, from 0 h to 109 h per week at 7 years post-discharge. Ten of the clients (5.5%) were receiving no disability support at 7 years. Higher scores on the ‘impairment’ sub-scale of the Health of the Nation Outcome Scales (HoNOS) was a significant predictor of support hours. The allocation of support hours was driven by impaired functioning (cognitive and physical) rather than symptoms.
Differences in mean total scores at 6, 18, 36 and 84 months post-discharge
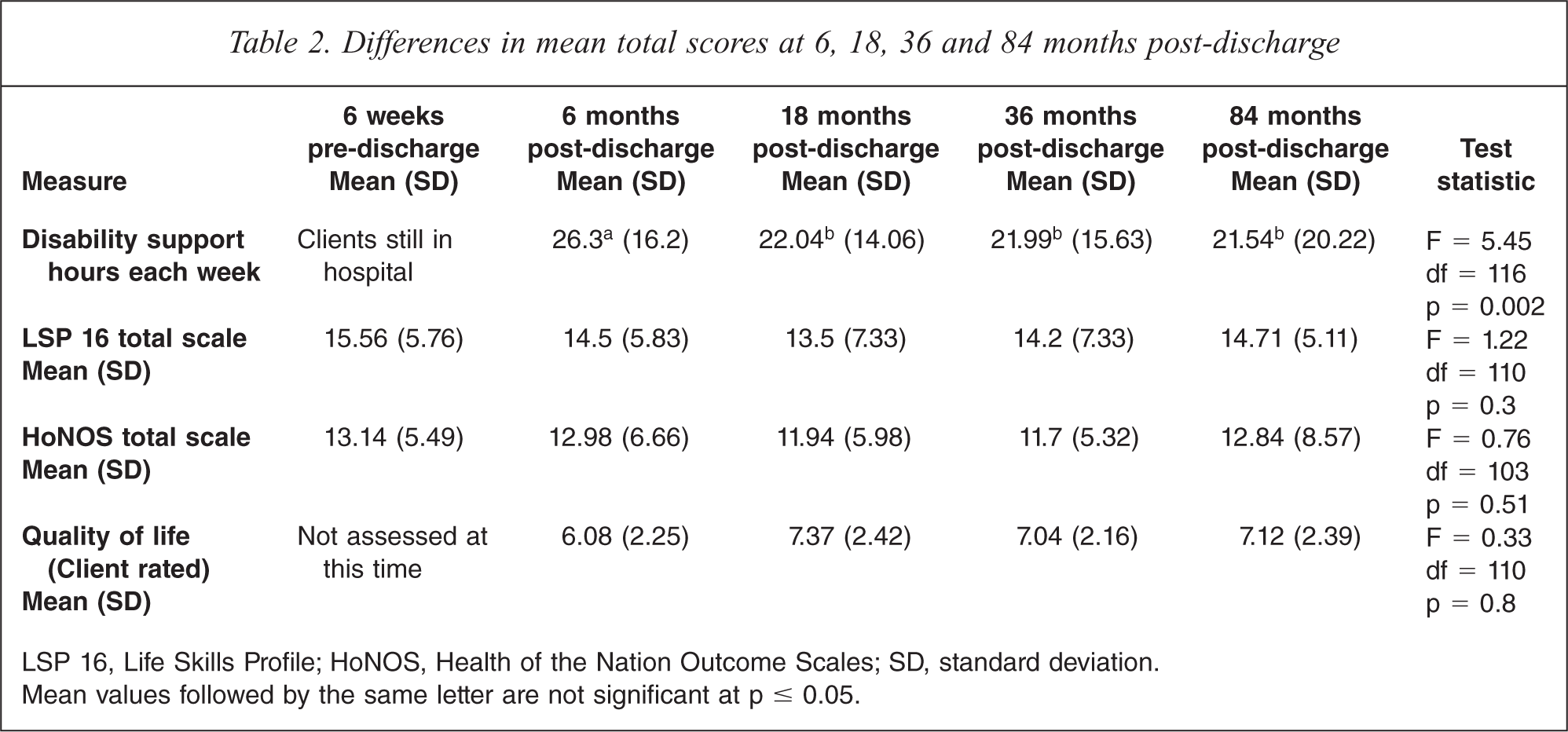
LSP 16, Life Skills Profile; HoNOS, Health of the Nation Outcome Scales; SD, standard deviation.
Mean values followed by the same letter are not significant at p ≤ 0.05.
Changes in functioning over the study period
Clinical functioning was assessed using the 16 item version of the Life Skills Profile (LSP 16) [6] and the HoNOS [7]. While total scores for both the LSP and HoNOS declined over the study period (i.e. clients improved), the extent of this decline was not statistically significant (Table 2).
Changes in client-rated quality of life
Study participants were asked to rate their quality of life using a 10 point visual analogue scale where ‘1’ represented the worse quality of life possible and ‘10’ represented the best quality of life possible. This single scale was derived from the larger quality of life measure developed in the USA by Becker and colleagues [8]. While there was a small improvement in quality of life between 6 months (mean = 6.8) and 36 months (mean = 7.0), there was very little change between 36 months (mean = 7.04) to 84 months (mean = 7.12). At all four assessments, clients rated their quality of life close to a mean of 7 (from a possible total score of 10). This suggests that clients perceived their quality of life as moderately high.
Changes in client satisfaction over the study period
Satisfaction with a number of life domains was assessed on a 7 point scale ranging from − 3 ‘very dissatisfied’ to + 3 ‘very satisfied’. Overall, the cohort was generally satisfied, providing a mean score of 2 for most domains (out of a possible score of 3). Clients were least satisfied with intimacy and most satisfied with their non-clinical support workers (Table 3). There were no significant changes in satisfaction on any of the domains assessed.
Differences in mean satisfaction scores at 6, 18, 36 and 84 months post-discharge
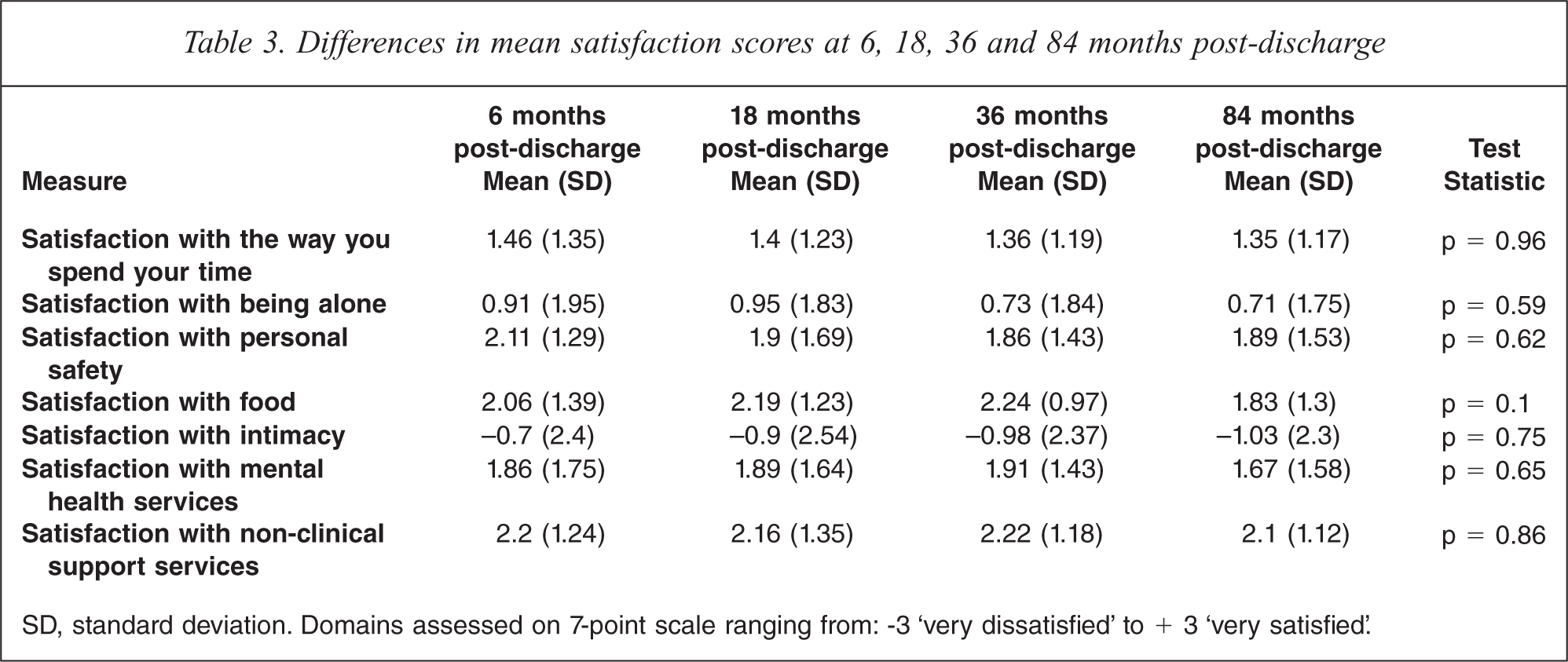
SD, standard deviation. Domains assessed on 7-point scale ranging from: −3 ‘very dissatisfied’ to + 3 ‘very satisfied’.
Changes in vocational outcomes over the study period
Ten of the 181 clients (5.52%) were engaged in paid employment at 6 months, 14 (7.7%) were in paid employment at 36 months and six (3.3%) were in paid employment at 84 months. At 7 years, three of the clients (1.7%) were employed on a full-time basis and the average time in work for all six clients was 17.5 hours per week. Only one client (who held a trade qualification) was employed across all follow-up assessments. These rates of employment are much lower than those reported in previous Australian studies. Data derived from the National Survey of Mental Health and Wellbeing found that 5.9% of individuals with psychotic disorders were in full-time employment, while 12.7% were employed on a part-time basis [9]. A more recent review of population data for individuals with schizophrenia found that 8% were in full-time employment [10].
The proportion of clients with no structured activity (defined as no job, no volunteer work, no study, no hobby) decreased significantly from 60.6% at 6 months to 38.7% at 84 months post-discharge (χ2 = 5.45, df = 112, p = 0.022). While the majority of clients were engaged in activities as much as they desired, about one third were demanding more involvement in structured activities.
Forensic involvement
While 22% of the clients discharged into the programme were under a forensic order at the time of discharge, only five clients (2.7%) committed offences following discharge. Three clients were returned to high/medium secure facilities, one for setting fire to her unit, one for assaulting a police officer and one for assaulting a support worker. The two remaining clients spent brief periods in prison, one for assaulting a police officer and the other for threatening a member of the public with a fishing knife.
The cost of care under Project 300 compared with other community alternatives
The average cost of providing an hour of disability support at 7 years was AUD 42 per hour. This included the cost of direct support to the client and agency overheads (such as staff supervision, administration costs, etc.). Given that the average client received 20 hours of support per week, this would equate to a cost of $840 per week or $43,680 per annum. Data derived from national benchmarking activity [11] suggests that the cost of providing community care (GP and/or case management services) is approximately $7,900 per annum, taking the total cost to $51,580. This excludes the costs associated with readmissions to acute inpatient care since this data was not available. However, the benchmarking data described above indicates that the average length of stay in an acute inpatient unit in Australia is approximately 14 days and the average cost of such a stay is $676 per day, providing a total cost for each admission of around $10,000. We have allocated one admission per client per year and this brings the estimated cost of keeping a client in Project 300 for a year (with one admission to acute care) to $61,580. This compares favourably to keeping the same client in an acute inpatient unit for a year at an estimated cost of $246,700 or a community care unit at an estimated cost of $133,225 per annum.
Discussion
The findings from this evaluation indicate that the majority of those discharged into the supported housing model were still residing in their allocated home at follow up. This is noteworthy given that these same individuals were unable to be discharged under previous relocation programmes and almost all had spent the 2 years prior to the programme in a psychiatric hospital. After 7 years, only a small number had returned to long-term care and almost 40% were able to reside in the community without the need for acute hospital admission. The evidence of successful community adaptation under Project 300 suggests that the provision of disability support actively contributed to successful community tenure.
While the need for acute care decreased, neither the support-worker contribution nor living in the community resulted in improved clinical functioning for the clients as a group. Notwithstanding this, symptoms and functioning did not deteriorate over the study period. The lack of functional gain in the community is in keeping with previous studies which suggest that disability and clinical functioning are unlikely to change in the follow-up period [5]. This may have resulted from an inadequate focus on rehabilitation on the part of both clinical and non-clinical support staff or may reflect illness factors or some combination of the two. The finding suggests the need for a stronger focus on rehabilitation and recovery in programmes such as the one described here.
Two of the underlying themes of deinstitutionalization have been increased client autonomy and social inclusion [12]. While the Project 300 programme was relatively successful in promoting client freedom and autonomy, it appears to have been less successful in promoting social inclusion for those in the programme. Even after 7 years of community living, few clients were employed and a large proportion had no structured activity outside of the home. This demonstrates the difficulty of linking individuals with severe mental illness into the broader community and brings into focus the skills of the disability support sector in being able to address this challenge. Indeed, there is some evidence to suggest that the involvement of support workers may hinder the development of broader social networks since support staff compensate for the lack of a social network [13].
Although there was a significant reduction in the hours of support provided, especially in the early stages of the project, the level of programme support required to maintain clients in the community remains high. It is clear from this and other follow-up studies [14–15] that maintaining people with severe psychiatric disability in the community requires considerable funding, and this needs to be allocated over several years. It is also clear that reductions in the level of support provided may not be feasible in the short term. There is some evidence to suggest that when patients moved from higher to lower intensity services, gains acquired during the provision of higher intensity services are lost [14]. Nonetheless, the overall cost of providing care in this programme was considerably less than inpatient/residential alternatives.
Nineteen of the 181 clients followed up (10.5%) died over the study period, four (2.2%) in the first year post-discharge. The first year mortality rate of 2.2% is similar to previous resettlement studies in Queensland and elsewhere. Findings from a recent evaluation of the Housing and Support Programme (HASP) in Queensland indicate that two of the 175 clients discharged (1.14%) died in the first year post-discharge [17]. In a large scale UK study, 24 of the 670 patients discharged (3.5%) died within the first 12 months of resettlement, while 126 of the 670 patients discharged (18.8%) had died by 5 years post-discharge [14].
It could be argued that higher functioning clients were put forward for Project 300 and this accounted for the outcomes observed. However, discussions with hospital managers suggest that clients with more severe problems were selected for the programme. There was a perception that higher functioning clients could be discharged under other programmes and that those with more severe disability would benefit from the higher levels of care provided through Project 300. However, this cannot be confirmed as measures of disability in those remaining behind in hospital were not collected.
Conclusions
Providing long-stay clients with their own home in the community and an average of 20 hours of non-clinical support through the Project 300 model has been effective in maintaining a cohort of patients with severe disability in the community. Many of the support functions were able to be met by the non-government sector using non-professionally trained support workers. The approach appears to do no harm, is consistent with human rights principles (i.e. least restrictive environment), and is more cost effective than institutional care. However, the programme had little impact on client disability and after 7 years of community tenure, the clients continued to require considerable levels of support. Service provision within Project 300 may not have been potent enough to bring about significant improvements in clinical functioning and overall disability. Future initiatives should encourage greater input from specialist service providers such as those skilled in recreation, building social networks and finding work for people with psychiatric disability.
Footnotes
Acknowledgements