
Abstract
Objectives:
This study aimed to (1) examine the strength of the association between mental disorders/mental health problems, risk behaviours and tobacco smoking among Australian adolescents, (2) compare rates of tobacco smoking among Australian adolescents with major depressive disorder, attention-deficit/hyperactivity disorder and/or conduct disorder in 2013/14 vs 1998, and (3) identify the extent to which an association between tobacco smoking and mental health problems among adolescents can be attributed to non-mental health risk factors.
Methods:
The study utilised data from the first (1998) and second (2013/14) child and adolescent components of the National Surveys of Mental Health and Wellbeing. Both surveys identified nationally representative samples of Australian young people aged 4–17 years, living in private dwellings. Information was collected from parents and 13- to 17-year-olds about mental disorders, mental health problems, risk behaviours and tobacco smoking.
Results:
In the 2013/14 survey, the rate of current tobacco smoking among those with a mental disorder was 20% compared to 5% in those without a mental disorder. Rates were highest for young people with conduct disorder (50%), major depressive disorder (24%) and anxiety disorders (19%). In 2013/14, 38% of current tobacco smokers had a mental disorder and 32% reported self-harm and/or suicidal ideation vs 10% and 5%, respectively, among adolescents who had never smoked. Females with mental disorders or reporting self-harm or suicidal ideation had higher rates of current smoking than males. Other significant factors associated with current smoking included school-related problems, binge eating and having had more than one sexual partner.
Conclusion:
While smoking rates in 13- to 17-year-olds with mental disorders had declined since 1998, the strength of the association between mental disorders and smoking had increased, especially among females. Our findings highlight the need to address the tobacco smoking among adolescents with mental disorders, particularly females.
In 1998/99, three times as many Australian adolescents with mental disorders smoked tobacco compared with those without mental disorders (Lawrence et al., 2010). Results from prospective studies of Australian adolescents in the 1990s also suggested that anxiety and depressive symptoms predicted experimentation and later daily smoking (Patton et al., 1996, 1998). In the past, tobacco use has also been linked to both self-harming behaviour and suicidality in adolescents (Hawton et al., 2012). However, during the last two decades, there has been a substantial decrease in the rate of tobacco smoking among adolescents in the general community. As such, it is unclear whether the previously strong association between tobacco smoking and mental health problems is still present among these adolescents.
There is also evidence that despite the lack of gender differences in overall smoking rates in the general population, adolescent females with mental health problems are more likely to smoke than males. For example, results from the US National Health and Nutrition Examination Survey (NHANES) (1999–2004) showed that rates of either depression or anxiety disorder did not vary significantly by smoking status for adolescent males, but rates of these disorders were 4 times higher among adolescent females who had ‘ever’ compared to ‘never’ smoked. Female smokers also had the highest levels of severe impairment associated with depression and anxiety (Richardson et al., 2012).
One of the major reasons young people give for smoking is managing stress (Holliday and Gould, 2016), especially females who are also more likely to smoke to stay thin (Simantov et al., 2000). According to the latest Mission Australia Youth Survey Report (Carlisle et al., 2019), ‘coping with stress’ was the biggest personal issue, with 6 in 10 females vs around one quarter of males aged 15–19 years being very or extremely concerned. Females were also more concerned than males about school and study problems, body image and mental health. Furthermore, studies have documented increasing levels of stress, distress and depression, especially in adolescent females in recent cohorts (Bor et al., 2014; Sawyer et al., 2018). These trends heighten concerns about the use of tobacco and other substances to cope with stress, negative emotions and mental health problems (Amos and Bostock, 2006; Lawrence et al., 2010; Pettigrew et al., 2017). In a US national sample, co-occurring polysubstance use and mental health symptoms was significantly higher in girls than boys (Maslowsky et al., 2014). Other factors found to be associated with adolescent smoking include low socio-economic status, low self-esteem, family disruption, parent and peer smoking, poor academic performance, rebelliousness, low levels of parental control and emotional support and pro-smoking media including film (Banzer et al., 2017; Choquet et al., 2007; Duncan et al., 2018; Towns et al., 2017; Wellman et al., 2016).
Studies examining smoking trends over time among individuals with mental disorders have largely focused on adults. Until recently these studies indicated that in contrast to reductions in the general population, there had been relatively little change in rates of smoking among adult smokers with mental disorders or with high levels of psychological distress (Cook et al., 2014; Kulik and Glantz, 2017; Lawrence and Williams, 2016; Szatkowski and McNeill, 2015). However, evidence of a more substantial decline in smoking rates in those with and without mental illness was reported in an analysis of successive Adult Psychiatric Morbidity Surveys 1993–2014 in the United Kingdom (Richardson et al., 2019). There are also signs of a reduction in smoking prevalence among adults with non-psychotic disorders from the two most recent Australian National Health Surveys 2011/12 to 2014/15 (Greenhalgh et al., 2018). Despite this, the excessive disease burden associated with tobacco smoking such as cardiovascular disease, respiratory disease and cancer remains disproportionately high among adults with mental disorders, and contributes substantially to the reduced life expectancy observed among this group, an average of 16 years for males and 12 years for females (Lawrence et al., 2013b). A significant omission in this area is that none of the studies above examined tobacco smoking trends among adolescents or young people with mental disorders. As such, although it is known that rates of tobacco smoking among young people as a whole have declined in recent decades (Guerin and White, 2018), it is not known whether this decline includes young people with mental disorders. This is important to understand as rates of common child and adolescent mental disorders have been relatively stable over time, notwithstanding an increase in adolescent depression (Sawyer et al., 2018). Tobacco smoking is usually initiated in adolescence, thus coinciding with a typical onset period for depression. Experimentation in adolescence is strongly linked with daily smoking, and psychiatric morbidity is associated with faster progression to regular smoking (Cohn, 2018; Patton et al., 1998), making early experimentation (from the first puff) an important focal point for both research and prevention efforts (Wellman et al., 2016).
This study had three aims: (1) to examine the strength of the association between mental disorders/mental health problems, risk behaviours and tobacco smoking among 13- to 17-year-olds in Australia, (2) to compare rates of tobacco smoking among Australian 13- to 17-year-olds with major depressive disorder (MDD), attention-deficit/hyperactivity disorder (ADHD), and/or conduct disorder (CD) in 2013/14 and 1998 and (3) to identify whether the association between tobacco smoking and mental health problems among adolescents can be attributed to factors other than their mental health. The latter is an important issue for interventions aiming to reduce tobacco smoking among young people with mental health problems because of the possibility that the association is a by-product of smoking rates being higher among young people experiencing social disadvantage who typically also have higher rates of mental health problems. As adolescent females with mental health problems smoke tobacco more than males, and time trends point to increasing distress in young females (Bor et al., 2014; Sawyer et al., 2018), we examined smoking rates separately by gender.
Although previous population studies have reported associations between mental health problems and tobacco smoking, and between socio-economic factors and smoking in adolescence, none have assessed a comprehensive set of socio-economic, psychosocial, educational, mental health and behavioural factors within the one study and used this information to examine the question of which factors are most strongly related to smoking status (Banzer et al., 2017; Choquet et al., 2007; Lawrence et al., 2010; Richardson et al., 2012; Simantov et al., 2000).
Method
Study population
Data were taken from the first (1998) and second (2013/14) child and adolescent components of the National Survey of Mental Health and Wellbeing. Both were nationally representative samples of Australian children aged 4–17 years, living in private dwellings. Full details of the survey methodology have been published elsewhere (Hafekost et al., 2015; Sawyer et al., 2000). Both surveys were funded by the Australian Government Department of Health.
The second Australian Child and Adolescent Survey of Mental Health and Wellbeing, Young Minds Matter (YMM), was conducted by the Telethon Kids Institute, The University of Western Australia, in partnership with Roy Morgan Research. In total, 6310 parents and carers (primary carers [PCs]) across Australia participated in the survey (55% of eligible households). Where there was more than one child in scope (aged 4–17 years and living in the household at least 50% of the time), the study child was randomly selected by computer. Face-to-face interviews were undertaken in households with PCs (84% female; 81% biological mothers). In addition, young people aged 11–17 years were also asked to participate and complete their own questionnaire (N = 2967; 89% of eligible young people). Detailed questions about smoking were asked of 13- to 17-year-olds (N = 2314).
Data from the first survey were used for comparison with YMM. The first survey was conducted by the University of Adelaide in partnership with ACNeilsen. Face-to-face interviews were conducted with PCs (N = 4509; 70% response rate). Where there was more than one child in scope (aged 4–17 years and living in the household at least 50% of the time), the child whose birthday was closest to the interview date was chosen as the study child. Young people aged 13–17 years completed their own paper-based questionnaires. Subjects included in this analysis were those (N = 1280) completing the Youth Risk Behaviour Questionnaire.
Variables
Tobacco smoking
In both surveys, questions about smoking were sourced from the US Youth Risk Behavior Surveillance System (YRBSS) (Centres for Disease Control and Prevention, 2014). In YMM, all young people aged 11 years and over were asked if they had ever tried cigarette smoking, even one or two puffs. Those that said ‘yes’ who were also aged 13 years and over were asked additional questions. In this paper, we use two measures of smoking. First, we refer to ‘ever smoking’ as ever tried at least one puff, and this question was identical in both surveys. Second, we refer to ‘current smoking’ for those that had smoked on at least one occasion in the past 30 days. Here, there is a slight methodological difference. In the first survey, all respondents were asked questions about smoking in the past 30 days. Whereas, in YMM, these questions were asked only of those that had ever smoked at least once per week in their life, thereby filtering out those that had not. Therefore, the measures of 30-day smoking are not comparable across the two surveys, representing a somewhat more restricted and serious measure of current smoking in YMM.
Child and adolescent mental disorders
In both surveys, 12-month mental disorders were assessed using the Diagnostic Interview Schedule for Children – Version 4 (DISC-IV) (Fisher et al., 1993). The DISC-IV implements the criteria for mental disorders set out in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (American Psychiatric Association, 2000). These criteria are based on sets of clinically significant symptoms associated with impairment of functioning. In the first survey, three modules were completed by PCs: MDD, ADHD and CD. In YMM, PCs completed seven modules: MDD, ADHD, CD and four anxiety disorders (social phobia, separation anxiety disorder, generalised anxiety disorder, obsessive-compulsive disorder). In YMM, adolescents also completed the MDD module. The degree of overlap between parent- and youth-identified cases of MDD was modest, and the prevalence was much higher when information was provided by youth (Lawrence et al., 2015). Both parent and youth reports are regarded as valid assessments (Jensen et al., 1999). To meet the criteria for a mental disorder, a child or adolescent required clinically significant impairment of functioning, operationalised as severe impairment in at least one functional domain or at least moderate impairment in two or more domains. In addition, a new measure of disorder severity was developed for YMM based on an expanded set of items about impact on functioning across four functional domains – at school or work, with friends, impact on family and impact on self, including psychological distress. Severity was classified as mild, moderate or severe (Zubrick et al., 2015).
Emotional and behavioural problems
The Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1994) was completed by PCs and adolescents in YMM. The SDQ provides a brief behavioural screening questionnaire comprising five scales of five items each and refers to 6 months prior to the survey. Items in four of these scales (emotional problems, conduct problems, hyperactivity and peer problems) are added together to generate a total difficulties score. The SDQ was designed so that approximately 10% of children and adolescents fall into the ‘abnormal’ range on the total difficulties score, which indicates that they are at substantial risk of clinically significant problems, with another 10% classed as ‘borderline’ and the remainder considered to be in the ‘normal’ range. Cut-offs were used as specified by the creators of the SDQ, which were based on British population data (Goodman, 1994), but very similar proportions of Australian children and adolescents fall in the ‘borderline’ and ‘abnormal’ ranges.
Psychological distress
Adolescents in YMM reported on their distress levels using the Kessler Psychological Distress Scale (K10), a widely used scale designed to detect differing levels of psychological distress in the general population. It is based on 10 questions about negative emotional states in the previous 4 weeks (Kessler et al., 2003). While high levels of distress are often associated with mental illness, it is not uncommon for some people to experience distress, but not meet criteria for a mental disorder. The Kessler Psychological Distress Scale was scored from 0 to 40 (higher scores indicate greater distress). Using Australian Bureau of Statistics standards, responses were classified into ‘low’, ‘moderate’, ‘high’ and ‘very high’ levels of distress.
Self-harm and suicidal behaviours
In YMM, adolescents were asked questions about self-harm and suicidal behaviours. The questions about self-harm probed lifetime and 12-month occurrence of deliberate self-harm or injury without intending to end one’s own life. The questions measuring self-harming behaviours, while drawing upon existing instruments, were specifically worded and tailored for the survey. Questions about suicidal behaviours were sourced from the YRBSS (Centres for Disease Control and Prevention, 2014) from which measures of 12-month prevalence of suicidal ideation and actual attempt were derived. The initial screening questions for self-harm and suicidal behaviours included a ‘prefer not to say’ option, which was conservatively coded to a ‘no’ for the purposes of this study, likely providing an underestimate of both behaviours.
Statistical analysis
For both surveys, proportions have been weighted to represent all 4- to 17-year-olds in the Australian population and to adjust for patterns of non-response (PCs and youth). Furthermore, in YMM, 16- to 17-year-olds were oversampled and the weights account for this. There were several stages to the analysis:
First, the relationship between smoking and mental health was described by different indicators of mental health status in YMM (mental disorders, SDQ emotional and behavioural problems, Kessler Psychological Distress [K10] and self-harm and suicidal behaviours). The difference in ever and current smoking rates by gender for each mental health indicator was tested using the Rao–Scott adjusted chi-square statistic. Rates of mental health problems among never, ever and current smokers were then calculated by gender.
Second, the relationship between adolescent smoking and mental health in 1998 and 2013/14 was compared by calculating the relative risk (RR) (95% confidence intervals [CIs]) of smoking in adolescents with and without mental disorders at each time point by gender.
Third, an exploratory data analysis was undertaken with YMM data using logistic regression models fitted using SAS software. The aim was to determine empirically which of the many, related risk factors and correlates were most strongly associated with current smoking. These were considered in five classes: (1) indicators of mental health and wellbeing (including those described above); (2) socio-economic factors; (3) psychosocial factors; (4) education factors; and (5) other risk behaviours. See Supplemental Table S1 for a full list.
Models were fitted in two steps. The first step involved univariate analysis, resulting in a large number of risk factors being eliminated from consideration if there was no univariate association (p > 0.25) with smoking status (see Supplemental Table S1). From the remaining factors, the most parsimonious best fitting set of variables in each category were chosen by selecting the model that had the lowest deviance. Finally, the best fitting model combining categories of indicators was chosen. Where there were several candidate solutions, the one that minimised the deviance was chosen. Two models were developed. The first model considered the four sets of risk factors excluding other risk behaviours. A second model was then developed including other risk behaviours, given the possibility that these behaviours may be outcomes of the same causal pathways that give rise to smoking behaviours and their presence in the model might obscure associations with other factors that might be more proximal in the causal pathway.
We used the same set of predictors to develop classification tree models. Classification trees or decision trees have become popular in data mining and predictive modelling in situations where the goal is to best predict an outcome rather than test specific hypotheses, and they are useful for generating hypotheses. There are several approaches to modelling using classification trees. We used the ‘rpart’ package within the R language which implements recursive partitioning for classification. This approach subdivides the population into categories that maximise the difference in smoking rates between the categories. As a sensitivity analysis, we also modelled the same data using conditional inference trees using the R ‘party’ package. An advantage of classification trees over logistic regression is that in logistic regression, the odds ratio reflects the RR but not the number of cases that might be correctly predicted without also considering the frequency of occurrence of each predictor. In contrast, classification trees clearly illustrate the proportion of the population that is represented in at risk categories. Separate classification trees were run by gender. It should be noted that in these analyses, we did not aim to establish causality as causal pathways are highly complex and commonly bi-directional in nature.
Results
Association between mental disorders/mental health problems, risk behaviours and tobacco smoking
In 2013/14, 7% of all 13- to 17-year-olds had smoked in the 30 days before the survey (current smokers); 8% of females and 6% of males. Furthermore, about 23% of all 13- to 17-year-olds had ever smoked; 24% of females and 21% of males.
The rate of current smoking among those with any DISC-IV disorder was 20% compared to 5% in those with no DISC-IV disorder (Table 1). Current smoking rates were higher for young people with specific DISC-IV mental disorders: 50% for CD, 24% for MDD, 19% for anxiety disorders and 13% for ADHD. The rate of current smoking for females with any DISC-IV disorder was greater than that for males (24% compared to 15%) but similar if not meeting criteria for a disorder (6% and 5%, respectively). Current smoking rates were also elevated with moderate or severe disorders, an abnormal level of difficulties on the SDQ (past 6 months), very high distress levels, and self-harming or suicidal behaviours in the past 12 months, especially for females.
Proportion of 13- to 17-year-olds who had ‘smoked in last 30 days’ and/or ‘ever smoked’ in 2013/14.
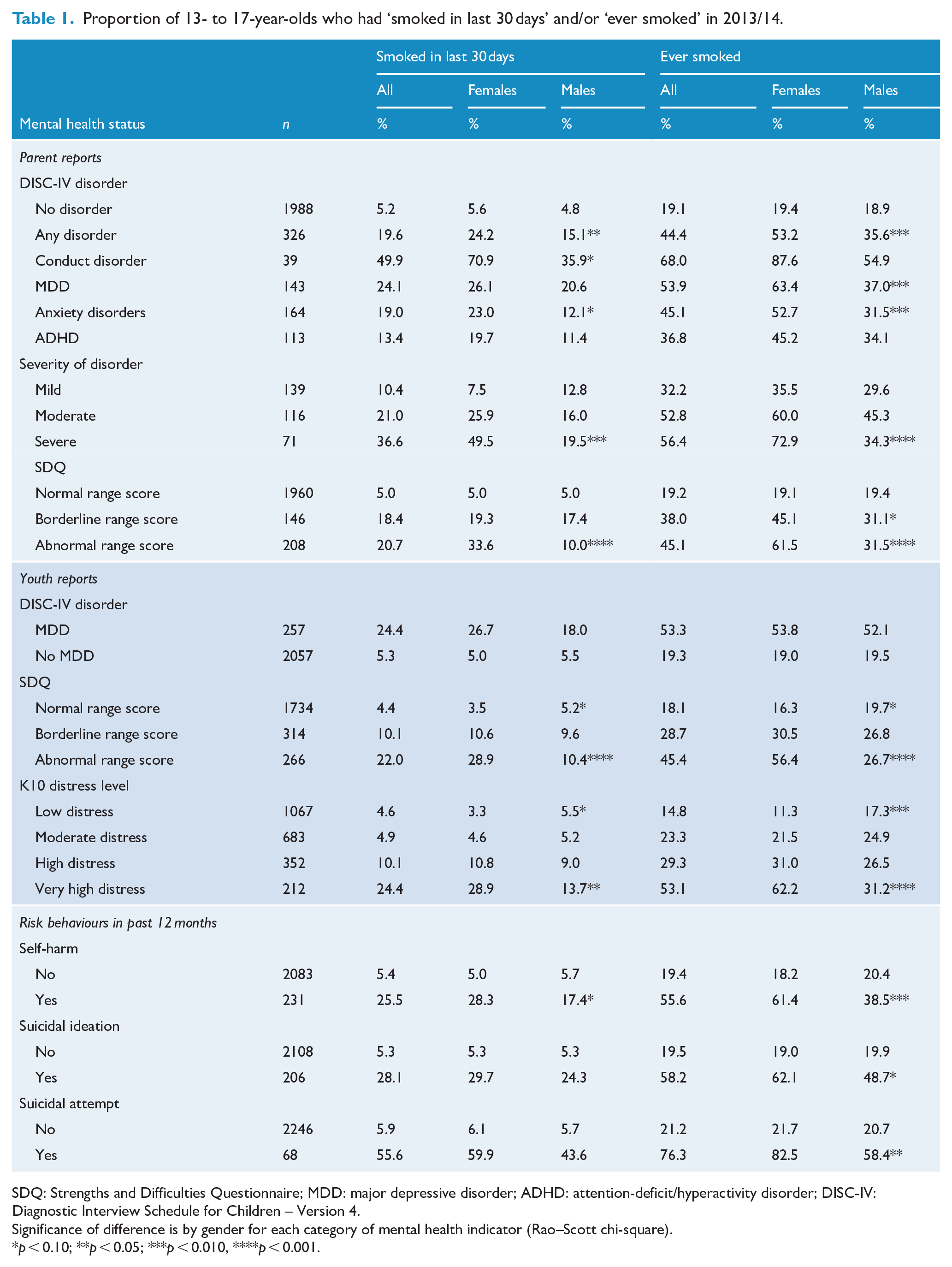
SDQ: Strengths and Difficulties Questionnaire; MDD: major depressive disorder; ADHD: attention-deficit/hyperactivity disorder; DISC-IV: Diagnostic Interview Schedule for Children – Version 4.
Significance of difference is by gender for each category of mental health indicator (Rao–Scott chi-square).
p < 0.10; **p < 0.05; ***p < 0.010, ****p < 0.001.
Rates of tobacco smoking in 2013/14 vs 1998
The rate of having ever smoked in 13- to 17-year-olds with any of the three comparable DISC-IV disorders (MDD, ADHD or CD) was 71% in 1998 and 46% in 2013/14 (Table 2). The RR of ever smoking in those with any DISC-IV disorder compared to no DISC-IV disorder was 1.24 (95% CI = [1.09, 1.40]) in 1998, compared to 2.33 (95% CI = [1.94, 2.79]) in 2013/14.
Rates of tobacco smoking among 13- to 17-year-olds with parent-reported mental disorders a in 2013/14 and 1998.
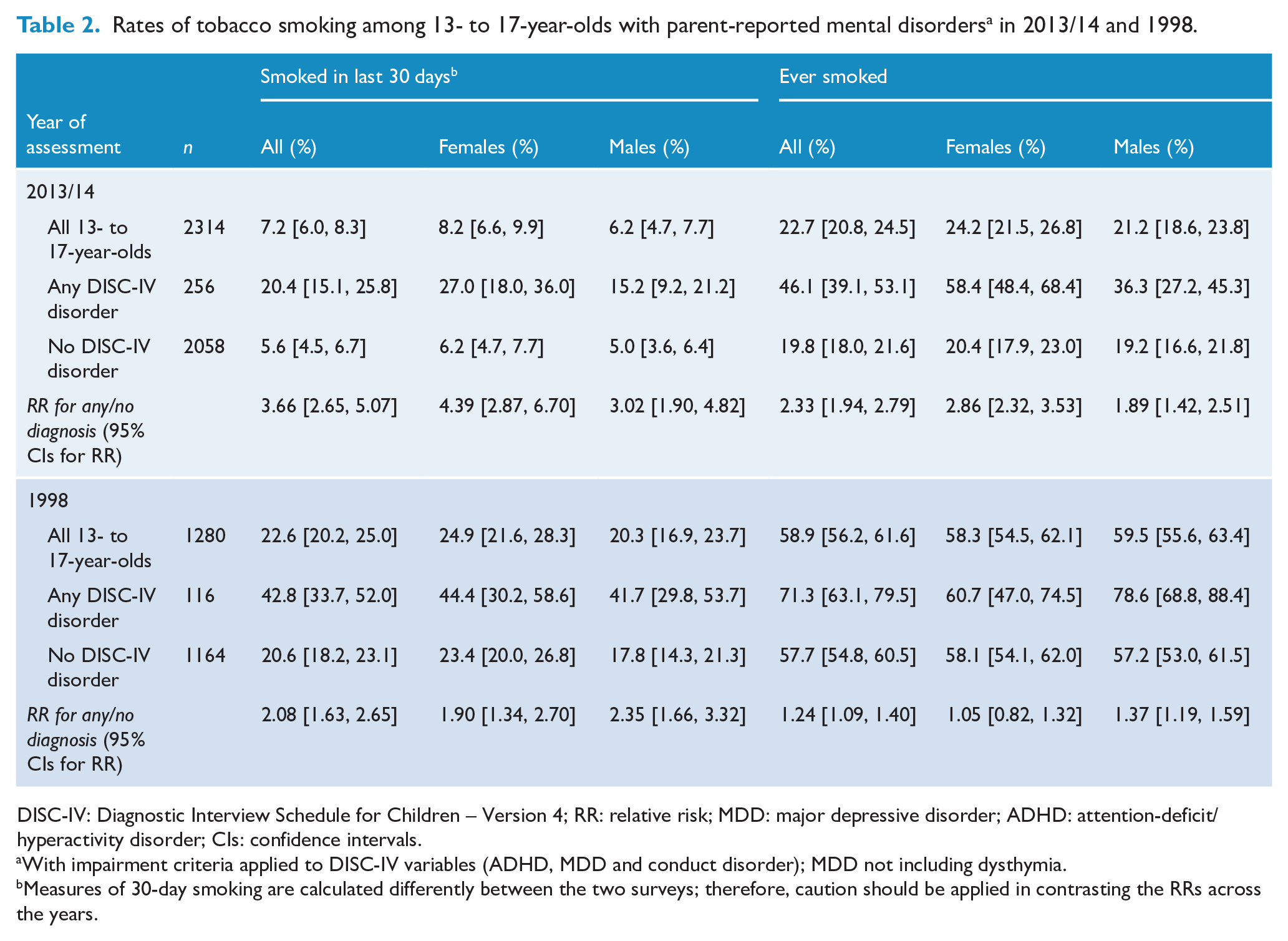
DISC-IV: Diagnostic Interview Schedule for Children – Version 4; RR: relative risk; MDD: major depressive disorder; ADHD: attention-deficit/hyperactivity disorder; CIs: confidence intervals.
With impairment criteria applied to DISC-IV variables (ADHD, MDD and conduct disorder); MDD not including dysthymia.
Measures of 30-day smoking are calculated differently between the two surveys; therefore, caution should be applied in contrasting the RRs across the years.
The size of the increase in risk for ever smoking over the 15-year period by disorder status was larger in females (from RR = 1.05 to RR = 2.86) than in males (from RR = 1.37 to RR = 1.89) (Table 2). Although the rates of current (30-day) smoking have also dropped between surveys, they cannot be directly compared due to methodological differences between the surveys which may serve to exaggerate the magnitude of the difference.
Correlates of tobacco smoking
In the 2013/14 survey, 38% of adolescents who had smoked in the last 30 days had a mental disorder based on parent reports and 34% had self-reported MDD. In contrast, only 14% of those who had never smoked had a mental disorder and only 6% had self-reported MDD. Furthermore, among those who had smoked in the last 30 days, 32% reported self-harm and/or 32% suicidal ideation in the past 12 months vs only 5% in each area among those who had never smoked (Table 3). In all these areas, the differences between adolescents reporting current smoking vs never smoked were greater for females than males.
Prevalence of disorders and self-harming behaviours among 13- to 17-year-olds who ‘smoked in the last 30 days’, ‘ever smoked’ and ‘never smoked’ in 2013/14.
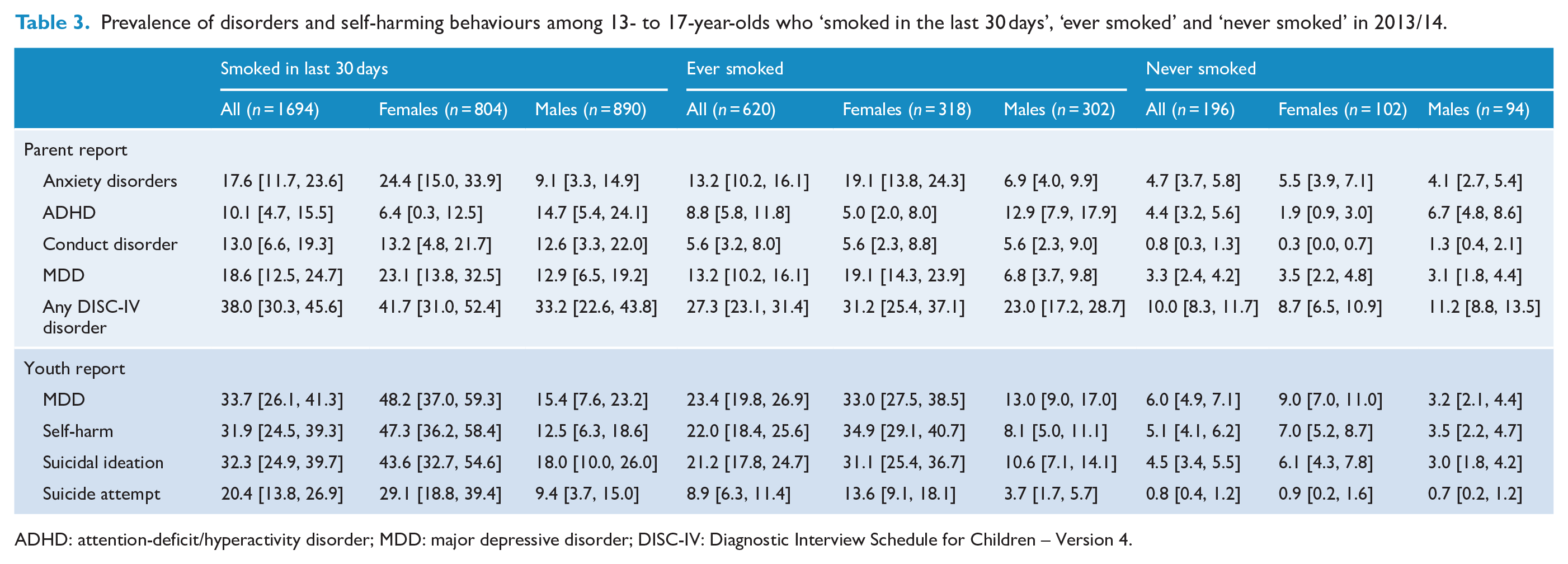
ADHD: attention-deficit/hyperactivity disorder; MDD: major depressive disorder; DISC-IV: Diagnostic Interview Schedule for Children – Version 4.
Exploratory analysis of possible associations between tobacco smoking and factors other than mental health found significant univariate associations with many factors across the five domains considered in the survey (Supplemental Table S1). As many of these factors are strongly correlated, we developed parsimonious multivariate models using the most strongly associated indicators. Using the four domains, excluding other risk behaviours, strongly associated variables included mental health factors (depression severity, CD, hyperactivity); school factors including poor attendance, falling significantly behind the age level in numeracy and having been suspended from school; and having a PC who is a current smoker (Table 4) Including other risk behaviours in the model further identified risky sexual behaviour, binge eating and self-harming behaviours as correlates of current smoking along with poor mental health problems at school and PC smoking.
Predictors of current smoking ‘smoked in the last 30 days’ in 2013/14.
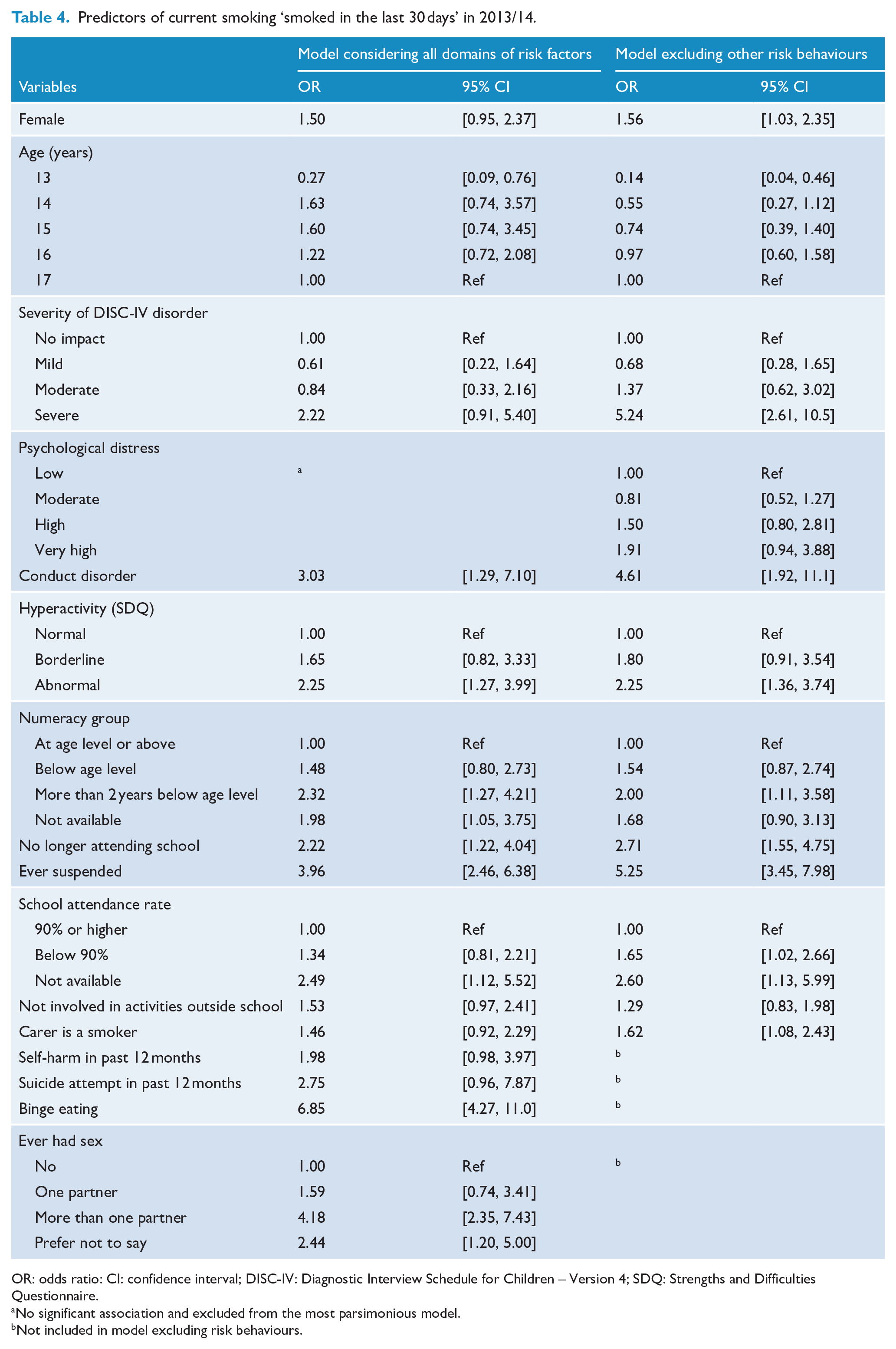
OR: odds ratio: CI: confidence interval; DISC-IV: Diagnostic Interview Schedule for Children – Version 4; SDQ: Strengths and Difficulties Questionnaire.
No significant association and excluded from the most parsimonious model.
Not included in model excluding risk behaviours.
A classification tree identified groups of young people with very different smoking rates (Figure 1). Being suspended from school, severe depression, CD, having dropped out of school and having either carer (primary or secondary) who smoked defined the high-risk categories for current smoking. For example, of the 1% of young people who had a carer who smoked, who were no longer attending school and had ever been suspended from school, 76% smoked, while in the 86% of young people who had never been suspended, 5% smoked. Separate classification trees were run for males and females (Figure 2). While most of the same key variables were used to classify current smokers for both males and females, severity of depression was the primary selection variable for females; while for males, severity of depression only played a role in the classification tree for older adolescents. For both males and females, a combination of having ever been suspended from school and severe depression identifies a group of adolescents with a very high smoking rate. Additional analysis including other risk behaviours highlighted the clustering of risk behaviours that define youth smoking in this sample including sexual behaviour, school suspension, binge eating, along with high levels of psychological distress and suicide attempts (Figure 3).
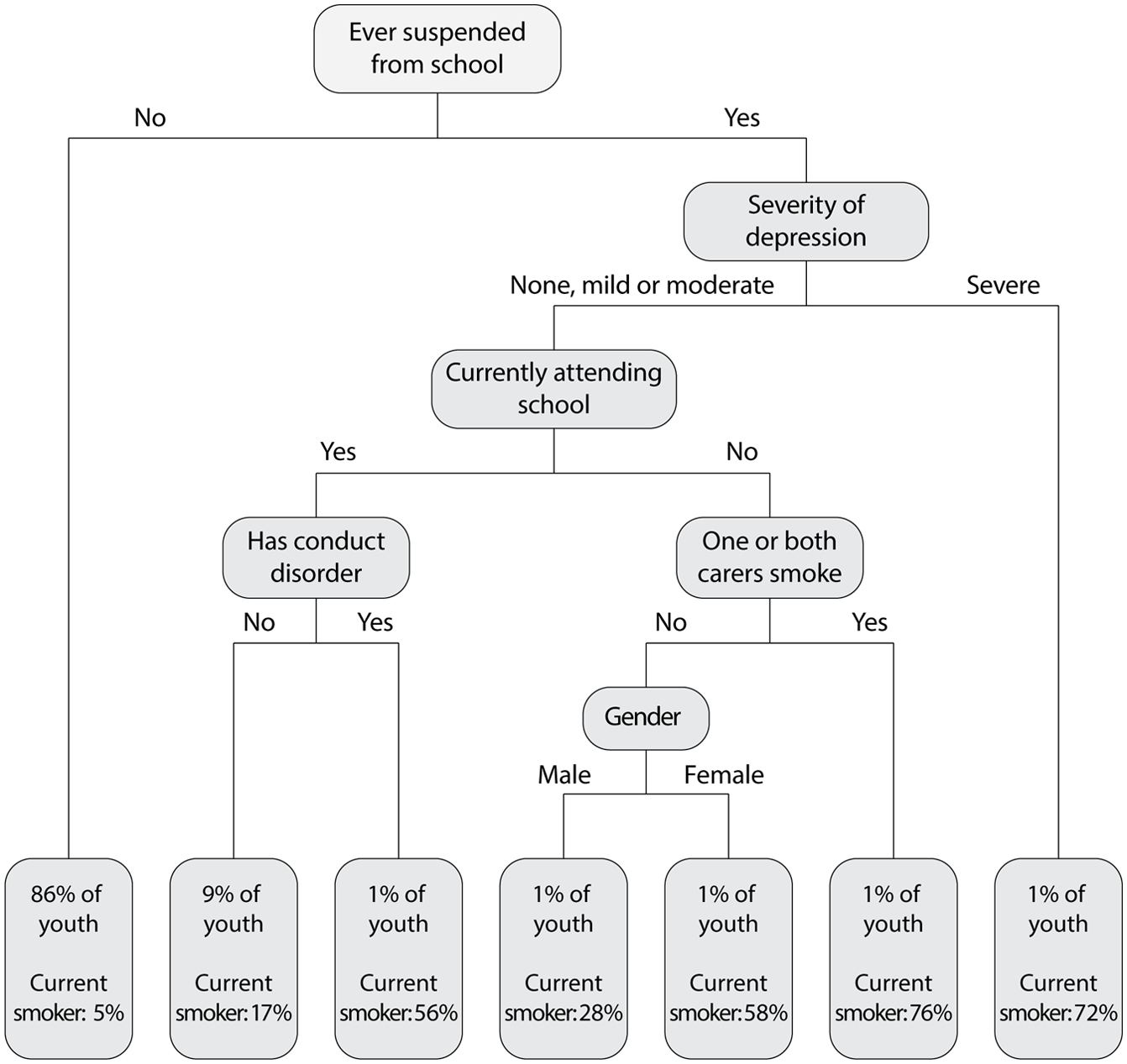
Classification tree for current smoking.
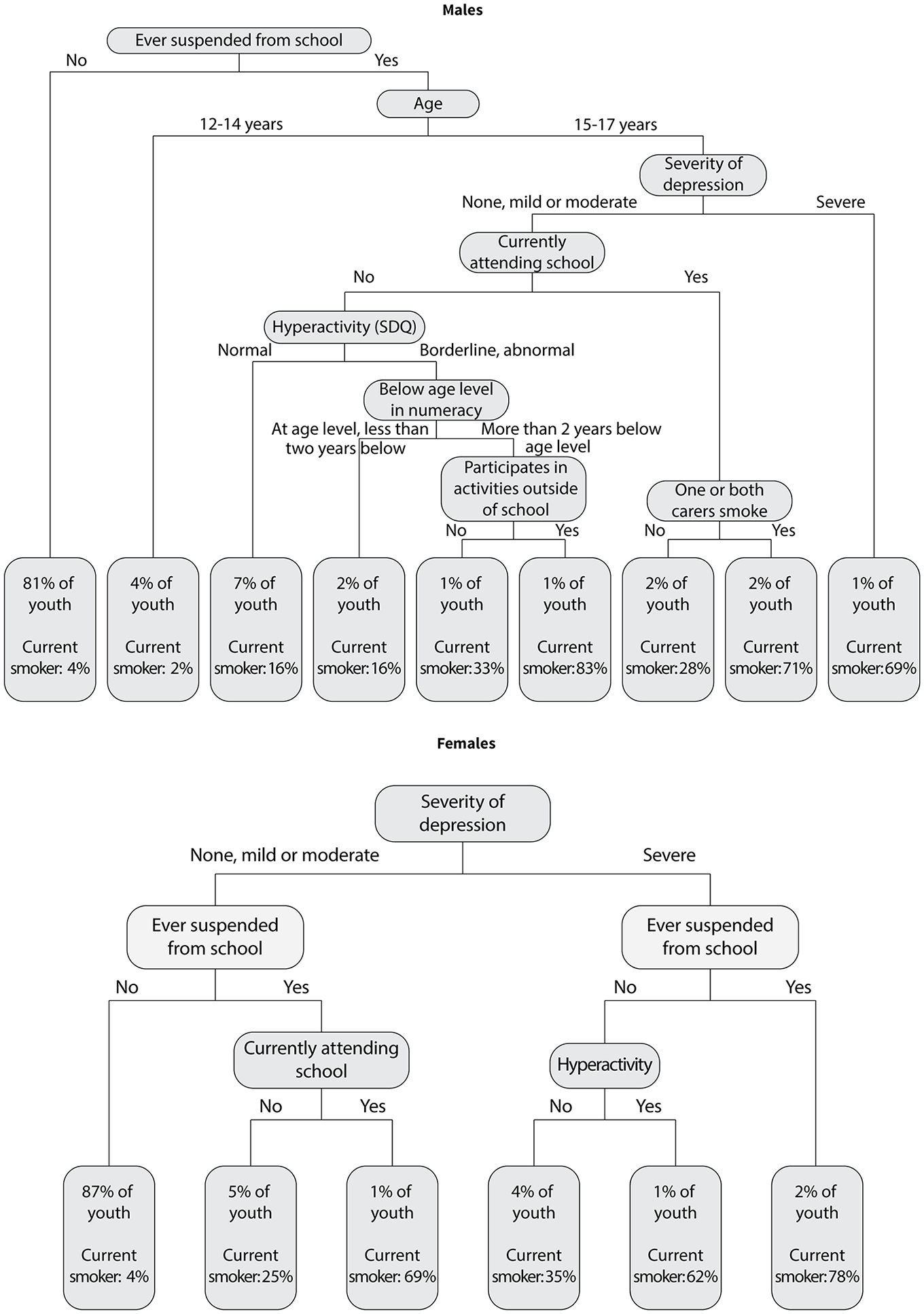
Classification tree for current smoking, by gender.
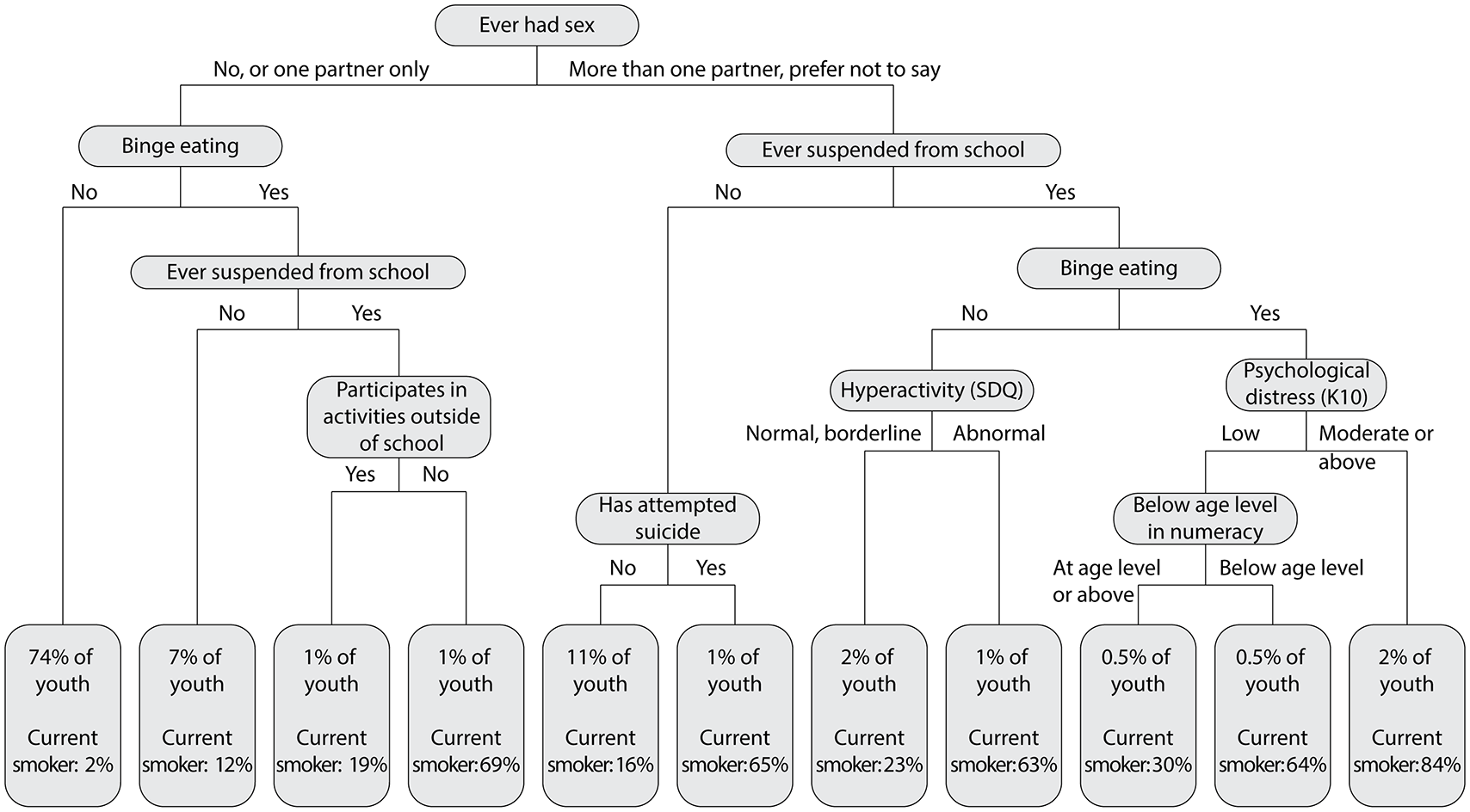
Classification tree for current smoking (including other risk behaviours).
Discussion
There are two key findings in this study. First, although there was a reduction in (ever) smoking tobacco among all 13- to 17-year-olds over the 15 years of the study, the decline was smaller for those with mental disorders (MDD, ADHD and CD). As such, there was a stronger association between tobacco smoking and mental disorders in 2013/14 as compared to 1998. This was particularly evident among females. Second, a high proportion of 13- to 17-year-olds who had smoked during the last 30 days in 2013/14 had multiple problems and risk behaviours, including comorbid mental health problems, self-harming behaviours and significant problems at school (poor attendance, suspension or having dropped out of school).
The strengthening of the association between tobacco smoking and mental disorders, particularly among females reinforces the need to further investigate and target those factors that increase vulnerability in adolescent females. Severe impairment from depression and anxiety may put females more at risk than males for tobacco smoking, as found by Richardson et al. (2012) , and illustrated in our classification tree analysis where depression severity was the primary selection variable for females, not males. These authors speculated that females experiencing depression or anxiety may be more susceptible to the influence of smoking peers, low self-esteem and have greater propensity to self-medicate to manage negative emotions. Patton et al. (1998) also found that females with mental health problems are more likely to smoke in the context of a peer group who smoked than with non-smoking peers. As well, females may be more vulnerable to a lack of parental emotional support (Choquet et al., 2007) or to use smoking for weight management (Amos and Bostock, 2006; Simantov et al., 2000).
Our findings have important implications for prevention and treatment programmes. Compared with previous generations where tobacco smoking may have been the most significant health risk behaviour in many young people who smoked, present-day adolescent tobacco smokers are often experiencing a cluster of adverse risk factors, of which smoking may not be perceived by them to be the most significant or urgent threat to their health and wellbeing. For instance, when comorbidities include self-harming behaviours or attempted suicide, promotional messaging about the long-term health adverse consequences of tobacco smoking may be less meaningful because of adolescents’ uncertainty and ambivalence about their long-term future (Lawrence et al., 2011). While there were univariate associations between socio-economic factors and smoking, our multivariable statistical models found that mental health, school problems and a few key behavioural variables were stronger predictors of smoking status than socio-economic factors. These findings are consistent with studies of adults which also found the relationship between mental health problems and smoking was not explained by socio-economic factors (Lawrence et al., 2013a).
The high rates of mental disorders and self-harming behaviours among tobacco smokers identified in this study are consistent with results in previous studies (Hawton et al., 2012; Lawrence et al., 2010; Richardson et al., 2012). These and other adolescent studies suggest that the relationship between tobacco smoking and self-harming behaviour is not consistently attributed to underlying mental health conditions (Brunner et al., 2014; Kessler et al., 2007). Tobacco use has been independently associated with suicidality among adults, with early age of first tobacco use representing the greatest risk (Han et al., 2016), especially among females (Korhonen et al., 2018). However, the mechanisms linking smoking and self-harming behaviours remain unclear with possible mechanisms, apart from the link with mental disorders, including shared vulnerability to impulsivity and risk-taking behaviour, the use of both behaviours as ways to cope with emotional distress, level of nicotine dependence, additional substance abuse and neurobiological pathways (Hawton et al., 2012; Korhonen et al., 2018). Despite the complexity and difficulty in establishing clear pathways, a strong link between smoking and self-harming, especially among females, is important from a clinical perspective both with and in the absence of known mental disorder.
Identifying tobacco smoking and providing minimal brief intervention is an important element of clinical practice for health professionals in all settings that help adolescents with mental health problems (The Royal Australian College of General Practitioners, 2011; Towns et al., 2017). Important opportunities exist to identify tobacco smoking and to intervene when young people present at youth mental health services (Brown et al., 2020; Hermens et al., 2013) which may be more acceptable services to young people than stand-alone smoking cessation programmes (Catchpole et al., 2017). Other interventions such as those to reduce parental smoking are proving to be effective in reducing adolescent smoking (The Royal Australian College of General Practitioners, 2011). In addition to preventing initiation, efforts could also be targeted at preventing the transition between experimentation and daily smoking in adolescents (Cohn, 2018; Patton et al., 1998), a process that occurs faster in young people with psychiatric morbidity. While many adult tobacco smokers with mental illness are both motivated and attempt to quit, successful quit rates are very low among adults even with sustained smoking cessation support (Lawrence et al., 2011). In the longer term, programmes that reduce tobacco smoking among adolescents also have the potential to reduce smoking-related morbidity and mortality in adults with mental illness. However, research on smoking prevention and cessation interventions in adolescents is very limited, and almost non-existent in those with mental disorders such as depression (Towns et al., 2017; Witt and Patten, 2018).
It has been argued that gender-sensitive approaches to tobacco control are needed along with a holistic approach to intervention that addresses the range of challenges faced by adolescents including mental health problems (Amos and Bostock, 2006). School-based tobacco intervention has the potential to improve the lives of students across multiple domains, especially for female smokers where impairment in schoolwork and relationships is especially high (Richardson et al., 2012). However, this can only be achieved effectively with proper school resourcing, trained staff and connections with health services. Stress management programmes can help adolescents to steer away from substance use (Holliday and Gould, 2016), and may be particularly effective for females for whom coping with stress is a more prevalent issue.
The strengths of this study include the use of population representative samples with widely used and validated measures of mental health, together with adolescent self-reporting of smoking behaviours and mental health indicators. There are also some limitations. Cross-sectional data preclude determination of causality, so we can only refer to associations and clusters of risk. The slightly different methodology for measurement of current smoking between the two surveys means that the results are not directly comparable in this area. In addition, anxiety disorders were not measured in the first survey, and as such, this study may have underestimated gender differences. Furthermore, we were not able to consider the impact of nicotine e-cigarettes. E-cigarettes were not included in YMM as they were only just coming into the Australian market at the time of the survey data collection in 2013–14. Although commercial sale in retail outlets is illegal in Australia, their use by young people has been increasing. According to the National Drug Strategy Household Survey, 4.3% of 14- to 17-year-old smokers smoked e-cigarettes in 2016 (the earliest Australian figures available), but this had increased to 17.5% in 2019 (Greenhalgh et al., 2020). Based on studies from the United States, where rates of e-cigarette have increased rapidly, there is mixed evidence on the association between e-cigarette use and mental health problems with the emotional and behavioural profile of adolescents who have only used e-cigarettes situated somewhere between non-users and cigarette smokers (Gaiha and Halpern-Felsher, 2020; Leventhal et al., 2016).
In conclusion, our findings reinforce the need for prevention and treatment strategies that recognise common susceptibility in adolescents to mental health problems and substance use issues. Mental health problems and tobacco smoking emerge and develop over the same time period in young adolescents making it a critical period to intervene with both problems.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211009617 – Supplemental material for Tobacco smoking and mental disorders in Australian adolescents
Supplemental material, sj-docx-1-anp-10.1177_00048674211009617 for Tobacco smoking and mental disorders in Australian adolescents by David Lawrence, Sarah E Johnson, Francis Mitrou, Sharon Lawn and Michael Sawyer in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to thank the 6310 families who gave their time to participate in the survey, Rajni Walia, Gerry Bardsley, the team at Roy Morgan Research and the Survey Reference Group for their input into the design and conduct of the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study uses data from Young Minds Matter which was funded by the Australian Government Department of Health. Authors Johnson and Mitrou are supported by the Australian Research Council Centre of Excellence for Children and Families over the Life Course (project number CE140100027). The views expressed herein are those of the authors and are not necessarily those of the Australian Research Council.
Ethical Approval
The Research Ethics Committee at the Women’s and Children’s Hospital, Adelaide, provided ethical approval for the 1998 survey. The research protocol for Young Minds Matter (YMM) was approved by two institutional review boards – the Australian Government Department of Health Human Research Ethics Committee (Project 17/2012) and the University of Western Australia Human Research Ethics Committee (Project RA/4/1/5538).
Data Availability Statement
The Confidentialised Unit Record File (CURF) from the first and second child and adolescent components of the National Survey of Mental Health and Wellbeing is available from the Australian Data Archive website. The first survey CURF can be found here: doi:10.26193/QGXQ47. In the case of the second survey (Young Minds Matter), the CURF can be accessed by researchers who have obtained prior ethics approval for their research: doi:10.4225/87/LCVEU3.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.