
Abstract
Problem or pathological gambling from a mental health perspective is defined by the American Psychiatric Association DSM-IV as ‘persistent and recurrent maladaptive gambling behaviour that disrupts personal, family and vocational pursuits’ [1]. Estimates of the prevalence of problem gamblers in the Australian adult population average around 2% across the States and Territories [2]. Similar rates in the USA and Canada estimated 1–2% of the adult population met the diagnostic criteria for pathological gambling [3]. Prevalence estimates are expected to rise further with increasing accessibility to gambling activities and legalization of new forms of gambling [4].
Treatment protocols and outcome studies for problem gambling have increased in recent years [5,6], however, there remain inconsistencies in results between studies and limited empirical support for specific types of treatment [7,8]. Whilst randomized controlled trials are often considered the ‘gold standard’ in treatment studies, generalizability of results to heterogeneous populations may be limited due to strict inclusion and exclusion criteria for participant study eligibility [9]. Further development of an evidence base for treatments of problem gambling requires complementary assessment methods including treatment effectiveness and treatment outcome studies. Treatment effectiveness studies assess efficacious treatments implemented in clinically diverse populations. Outcome studies report client outcomes and treatment characteristics, provide the opportunity to disseminate findings to other jurisdictions and inform quality improvement processes [10].
Treatment attrition rates present another significant challenge, as it has been estimated that up to 50% of problem gamblers will drop out of treatment [11,12] and a recent systematic review identified 12 studies that had addressed this issue [11]. Findings from the review indicated that there was little or no strong evidence for a number of variables including age, unemployment, gender, education and relationship status being related to treatment drop out. For the variables social support, duration of gambling, anxiety, and impulsivity, each was supported by one study as being significant predictors of treatment drop-out. A more recent study further supported impulsivity as a significant predictor of treatment drop-out [13]. Sensation-seeking has been proposed as a related construct to impulsivity with emphasis on novelty and intensity components [14]. Previous research has established intensity seeking as a strong predictor of problem gambling behaviour in young adults [15]. Further investigations into these and other potential predictors of treatment drop-out will benefit research and treatment of problem gambling.
In this article we report on the first evaluation study for the Statewide Gambling Therapy Service (SGTS) in South Australia. The primary treatment modality is a specific type of behaviour therapy called exposure therapy (ET). Behavioural therapy is based on the theory that problem gambling is the result of the development of a psychophysiological ‘urge’ to gamble, analogous to craving in substance addiction and anxiety in anxiety disorders, all of which have psychological and physiological (arousal) components in response to environmental triggers or cues. Exposure therapy has been established internationally as one of the most effective psychological treatments for anxiety disorders such as agoraphobia, social phobia, and obsessive–compulsive disorder, and of equal or superior efficacy to cognitive behaviour therapy when applied to problem gambling [16].
The theoretical mechanism of behavioural therapy is de-conditioning of the urge using exposure to gambling cues, and response prevention (resisting gambling) which results in habituation of the urge within a session and ultimately extinguishing of the urge if the exposure task is repeated. Remission of problem gambling occurs by eliminating the gambling ‘urge’ rather than through a reduction in gambling cognitions [17,18].
Objectives of this study include evaluation of gambling-related outcome measures covering various domains of clients’ experiences and identifying characteristics associated with treatment drop-out. Whilst not an empirical investigation of treatment efficacy with formal conclusions able to be drawn, it is an exploration of client progress, or ‘a natural history of client change’ [19] following treatment engagement with SGTS.
Methods
Service and participants
The participants in this study were adults (n = 127) who at baseline presented to the Statewide Gambling Therapy Service (SGTS) in South Australia seeking treatment for their problem gambling. The outpatient SGTS programme was inaugurated in 2007 and offers one-on-one therapy for problem gamblers in key metropolitan and rural regions that are associated with significant problem gambling activity. The service is staffed by a psychiatrist and therapists with professional backgrounds in psychology, nursing, or social work. All therapists have post graduate qualifications in cognitive behaviour therapy [17].
Assessment and treatment
On first presentation to SGTS clients are provided with a screening interview to assess suitably for admission into the treatment programme. The interview is comprised of a gambling focused cognitive behavioural assessment including DSM IV criteria for identifying problem gambling. Clients are also assessed for any co-morbid mental health problems such as alcohol dependence, anxiety and depression.
Treatment specifically targets the urge to gamble and on extinguishing this urge through a programme of graded urge exposure therapy (ET) [17]. The principles of ET are applied using graded tasks so the urge to gamble experienced at various stages of treatment is manageable. The initial procedure comprises a therapist guiding the client through a scene, which is usually audiotaped and then instructing the client to imagine a typical gambling scenario (imaginal exposure). The client is asked to rate his or her urge to gamble at regular intervals while verbalizing the scenario and to stay with the urge until habituation occurs. Once the client has habituated to the urge in imagination, clients habituate to their urge to gamble using a variety of live tasks at gambling venues (in-vivo exposure) to challenge the triggers of their urges [17].
Exposure therapy tasks are repeated regularly as a homework exercise for 5 to 7 weeks. Such tasks routinely last from 30 minutes to one hour with this time reducing as habituation to the urge to gamble is achieved [18]. Clients are seen weekly by a therapist, homework is reviewed and tasks regraded or new tasks agreed on. As the client progresses through treatment, set tasks become increasingly more challenging. By the end of treatment the aim is for the client to have mastered the urge to gamble, enabling them to feel comfortable being alone in a gambling venue with money in the close proximity of gaming machines and not requiring any modifying factors to help cope with their urge to gamble.
Design and procedure
Participants were recruited from consecutive referrals to SGTS in the time period March to September 2008. To be eligible, clients had to have been assessed as treatment-seeking problem gamblers at screening interview and suitable for admission into the treatment programme. Baseline measures were collected following the screening interview and consenting to participate in the study. Follow up assessments were conducted by mailed questionnaires at 1, 3, 6 and 12 months. Final follow up was dependent on the time of recruitment into the study, with participants completing either 6 or 12 month measures as their final assessment by study completion in March 2009. The study was approved by the Flinders Clinical Research Ethics Committee.
To improve participant response rates to mailed questionnaires, multiple contacts were implemented [20]. A letter was sent to each participant one week after the mailing out of a questionnaire. The purpose of this letter was to thank those who had returned their questionnaires and act as a reminder for those who had not. At three weeks, a further letter was sent only to participants with unreturned questionnaires. A final follow up occurred at five weeks with a telephone call to participants who had not returned questionnaires. The purpose of the call was to see if the participant had any questions about the study and to offer the mailing out of a further set of questionnaires if needed. As incompatible results may arise from different data collection modes [21] the opportunity to complete questions on the phone was only offered where an improvement in response rates was considered more probable in light of participants previous response patterns. Also, as response rates to mailed questionnaires have been shown to improve significantly with the provision of unconditional token ‘incentives’ [20], each participant was mailed an honorarium gift voucher with follow up questionnaires.
Baseline variables
Baseline demographic variables were gender, age, marital status, highest education level, employment status, and living arrangements. Data for duration of gambling problem and type of gambling were also collected.
Treatment drop-out
Treatment drop-out was defined using a common approach based on attendance at a specific number of sessions [11]. Prior to study commencement, SGTS clinicians determined an appropriate cut-off number of sessions for classifying clients as treatment drop-outs as 3 or less including the first screening attendance. Frequency distribution of session attendances for the cohort in this study included a 25th percentile of 3 sessions, median of 5, and 75th percentile of 9, and an inter-quartile range of 6 sessions. Overall, 41 (32%) participants were classified as treatment drop-outs with 7 (17.1%) of these completing initial screening and baseline measures only and 12 (29.3%) completing 2 or 3 sessions and baseline measures.
Candidate predictor variables of treatment drop-out included demographics, duration of problem gambling, and the following baseline self-report measures.
Social support
The Multidimensional Scale of Perceived Social Support (MSPSS) is a 12-item self-report questionnaire containing three sub-scales (significant other, family, and friends sub-scales). Research has shown the MSPSS has good reliability, factorial validity and adequate construct validity [22].
Trait anxiety
The Trait Anxiety Inventory form Y-20 is a 20-item self-report measure designed to record level of trait anxiety. Studies have shown the scale has good reliability measured by test–retest coefficients and sound validity [23].
Sensation seeking traits
The Arnett Inventory of Sensation Seeking (AISS) is a 20-item self-report questionnaire that measures sensation-seeking personality trait. Within the tool there are two subscales, intensity and novelty, consisting of 10 items each. The scale has been shown to be free from social desirability bias [24].
Outcome measures
Short and mid-term outcomes was assessed by means of validated self-report measures at baseline and 1, 3, 6, and 12 months. A brief description of validated measures specific to gambling problems is presented in the following paragraphs.
Victorian Gambling Screen
The Victorian Gambling Screen (VGS) is a self-reported questionnaire measuring the extent to which gambling behaviour has impaired the client's life. It comprises three sub-scales (enjoyment of gambling, harm to partner and harm to self) with a total of 21 items. For the purposes of this study, only the harm to self sub-scale was used as an outcome measure. This sub-scale has been validated for use in Australia. Concurrent validity indicates the scale correlates highly with the South Oaks Gambling Screen (SOGS) at 0.97 but extends the score range. A cut-off score of 21 or higher identified a participant as a problem gambler [25]. It was chosen as the problem gambling outcome measure because it was developed and validated in Australia and it has a one month time frame for reporting, enabling measurement of change during and after treatment.
A recent study confirmed the subscale as a reliable and valid screening tool of gambling severity in treatment-seeking problem gamblers. Robust internal validity was found with a Cronbach's alpha of 0.89. A principal component analysis confirmed the factor structure, and a high degree of concurrent validity was found with measures of psychological distress. It also had greater reliability in identifying severity of problem gambling compared to the South Oaks Gambling Screen (SOGS) [26].
Gambling Related Cognition Scale
The Gambling Related Cognition Scale (GRCS) is a 23-item self-report questionnaire that records common thoughts associated with problem gambling. Higher scores indicate increased cognitive distortions with a range of 0–161. A comparison with the South Oaks Gambling screen indicated the scale has good psycho-metric properties in measuring gambling cognitions in a non-clinical sample [27].
Gambling Urge Scale
The Gambling Urge Scale (GUS) is a self-report questionnaire measuring the extent of gambling urge. Higher scores indicate greater urges to gamble with a range of 0–42. Research into concurrent, predictive and criterion-related validity of the GUS suggest the GUS is a valid and reliable instrument for assessing gambling urges among non-clinical gamblers [28].
As problem gambling impacts on a range of domains in a gambler's life [29,30], we selected further self-report measures to assess outcomes in areas of emotional/mental health, relationships, and employment. A brief description of each measure is presented in the following paragraphs.
Depression Anxiety and Stress Scale
The Depression Anxiety and Stress Scale (DASS-21) is a 21-item self-report questionnaire which measures depression, anxiety (state) and stress. Final scores indicate levels of depression (0–9 = normal to 28+ = extremely severe), stress (0–7 = normal to 20+ extremely severe) and anxiety (0–14 = normal to 34+ = extremely severe). A composite measure of general psychological distress can be calculated by adding each of the subscale scores. Normative data has been collected for Australian populations and the DASS has been validated against other Beck Depression and Anxiety Inventories [31].
Alcohol Use Disorders Identification Test: Self-Report Version
The Alcohol Use Disorders Identification Test (AUDIT) is a non-diagnostic 10-item questionnaire indicating hazardous alcohol use. Final scores range from 0 indicating abstainer, < 8 indicating low risk alcohol use, 8+ indicating risky or harmful alcohol use, 13+ indicating alcohol dependence is likely. The scale reveals specificities and sensitivities superior to those of other self-report screening measures and good test–retest reliability and internal consistency [32].
Work and Social Adjustment Scale
The Work and Social Adjustment Scale (WSAS) is used to measure an individual's perspective of their functional ability/impairment. The scale contains five items which enquire about the degree to which the client's gambling problem affects their ability to function in the following areas: work, home management, social leisure, private leisure, and family and relationships. The score range is 0–40 with higher scores indicating greater impairment. Research into the validity of the scale suggests that WSAS correlates closely with the severity of depression at 0.76 and is sensitive to individual differences and change following treatment [33].
Statistical methods
All statistical analyses were conducted using Stata 11.0 [34]. An initial data analysis was carried out to check for data quality including allowable ranges and errors. Univariate analyses were performed on all variables to identify missing data and to clarify data structure.
Linear mixed modelling (LMM) was used to quantify change over time of the continuous outcome measures of problem gambling. LMM takes into account the inter-individual differences in intra-individual change with repeated responses and uses all the available data on each subject. LMM is also unaffected by randomly missing data and therefore does not require imputation methods [35]. For this study, the mechanism of missing data was assumed to be missing at random (MAR) where the likelihood of a participant dropping out of the study depended on past values of outcome measures, but not on future outcome measures. Both random intercept and random coefficient models were fitted. Models for each outcome variable included time as a continuous covariate and with treatment completion status categorized as either treatment completer or treatment drop-out. A quadratic term for time was also tested to allow for possible non-linear effects where rates of change in outcome measures slowed down over time with a levelling off effect. Final model selection was based on the comparison of nested and reference models with likelihood ratio tests (LRT). To check the assumption of normally distributed errors for each model, standardized residuals were examined. Predicted values for significant outcome variables were calculated from final models.
To facilitate a clinically meaningful interpretation of changes in outcome measure scores, effect sizes (Cohen's d) were calculated from baseline to 3 month follow up or 6 months if data was missing at 3 months [36]. To minimize overestimation of effect sizes due to potentially high correlations across pairs of measures, the equation d = t [2(1 – r) / n]1/2 was used where r is the correlation coefficient [37]. An effect size of 0.2 was considered small, 0.5 as medium, and 0.8 as large.
Measurement variability for each psychometric scale was examined with reliable change indices (RCIs). Using the formula SEdiff = SD1(21/2) (1–r)1/2 where SD1 was the standard deviation at baseline assessment and r was Cronbach's alpha coefficient, each individual's baseline to 3 or 6 month change score was expressed as standard error units of measurement. A reliable change was indicated when individual scores were outside the range of 1.96 times the SEdiff with 95% confidence [38]. Changes not exceeding this range were considered to be attributable to measurement variability.
Binary logistic regression analysis was conducted to assess the extent to which potential predictor variables were related to treatment drop-out. Variable selection commenced with univariate analyses. Using Wald statistics and P values for each univariate model, variables were selected for model advancement based on P < 0.25. This conservative approach was to allow the inclusion of potentially important variables that otherwise may have been excluded with traditional values such as P < 0.05 [39]. Categorical variables with low or zero cell counts in contingency tables were modified as needed. An initial full model was created with variables significant at P < 0.25 and not collinear. Using backward manual elimination methods, variables with the least significant Wald statistic were removed from the model. A comparison of log likelihood values between the fitted model and the full model was conducted for each variable removed. The goal was to construct a model with the fewest number of variables without compromising a reasonable fit of the data.
Results
Participant enrolment and flow
Participants were recruited from 240 consecutive referrals to SGTS during the study recruitment period. Due to an unstable mental state 23 (9.6%) persons met exclusion criteria. Reasons for non-participation by eligible individuals (n = 217) included 50 (23%); declining to participate; 25 (11.5%) attributed to inconsistent application of research protocol; 11(5.1%) classified as unknown; 3 (1.4%) due to limited English; and 1 (0.5%) as homeless. The final study cohort was comprised of 127 (58.5%) individuals consenting to participate. There was a significant difference in gender distribution on participation status, with 67 female (59.3%) non-participants compared to 58 female (45.7%) study participants (χ2 = 4.45, df = 1, p = 0.035), but no differences between the groups in age, primary form of gambling, and duration of gambling problem.
Overall, median time for participants enrolment in the study was 8.9 months with 50% of participants having times between 7.4 and 9.7 months (IQR = 2.3 months) and 25% less than 7.4 months. Patterns of completed measures for points in time included 91 (71.7%) at 3 months or more and 80 (63%) at 6 months or more. The only different mode of data collection to self-administered questionnaires by mail occurred when two participants completed questionnaires with follow up telephone calls from an investigator on one occasion each.
Baseline data
Demographic and clinical characteristics of the study cohort are presented in Table 1. When compared to problem gamblers participating in a recent population-based cross-sectional study conducted in South Australia [40] there were no significant differences in frequencies of age groups, gender, and education level. For marital status there was a borderline difference at the 5% level between the two groups (χ2 = 7.96, df = 3, p = 0.047) with the SGTS cohort having a greater number of separated/divorced participants. For employment status there was also a significant difference (χ2 = 23.48, df = 3, p < 0.001) with more participants reporting unemployment.
Demographic and clinical characteristics of 127 problem gamblers†
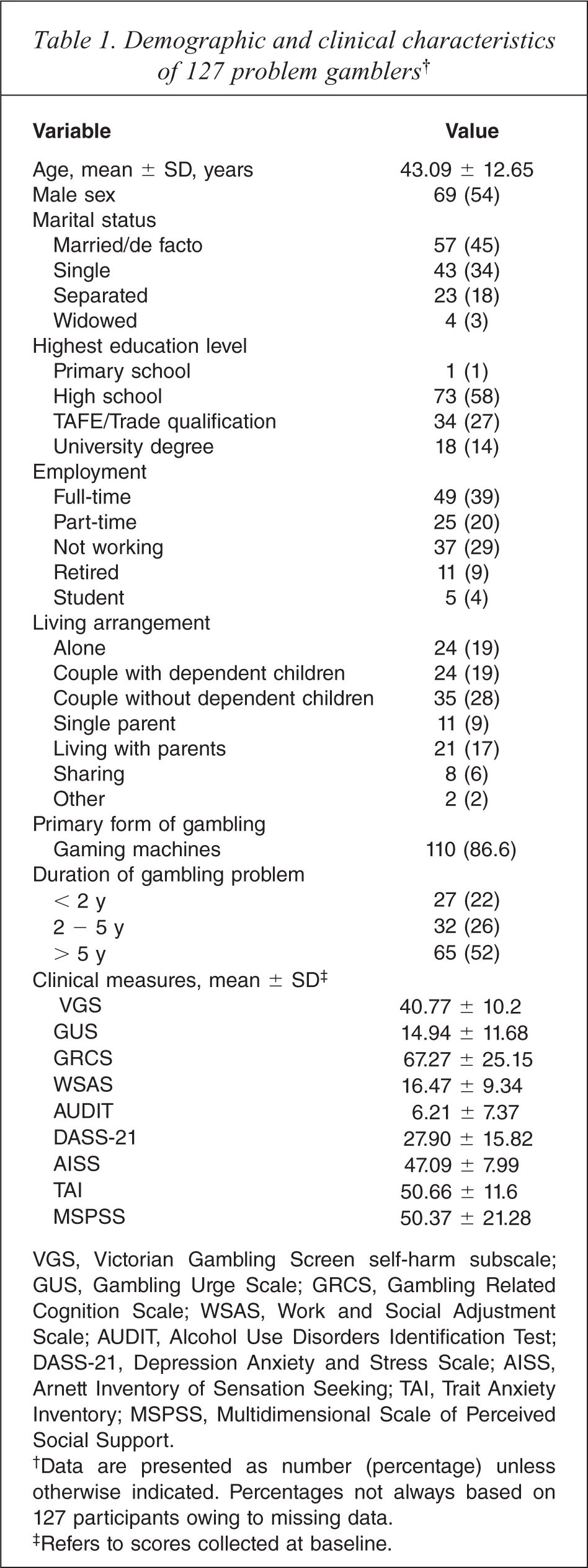
VGS, Victorian Gambling Screen self-harm subscale; GUS, Gambling Urge Scale; GRCS, Gambling Related Cognition Scale; WSAS, Work and Social Adjustment Scale; AUDIT, Alcohol Use Disorders Identification Test; DASS-21, Depression Anxiety and Stress Scale; AISS, Arnett Inventory of Sensation Seeking; TAI, Trait Anxiety Inventory; MSPSS, Multidimensional Scale of Perceived Social Support.
†Data are presented as number (percentage) unless otherwise indicated. Percentages not always based on 127 participants owing to missing data.
‡Refers to scores collected at baseline.
When compared to previous normal population scores [31], baseline DASS means for the SGTS cohort were higher for the depression (mean = 10.79 ± 6.06), anxiety (mean = 6.5 ± 5.42), and stress scales (mean = 10.61 ± 5.8), and in the moderate severity range. The distribution of baseline scores across severity ranges for the depression subscale was 18.9 % (n = 24) in the normal range, 7.1 % (n = 9) in the mild range, 20.5 % (n = 26) in the moderate range, 16.5 % (n = 21) in the severe range, and 37 % (n = 47) were in the extremely severe range.
Anxiety scores were distributed as 37% (n = 47) in the normal range, 3.2% (n = 4) in the mild range, 20.5% (n = 26) in the moderate range, 16.5% (n = 21) in the severe range, and 22.8% (n = 29) were in the extremely severe range. Stress scores were distributed as 33.1% (n = 42) in the normal range, 11% (n = 14) in the mild range, 22.1 % (n = 28) in the moderate range, 13.4% (n = 17) in the severe range, and 20.5% (n = 26) were in the extremely severe range.
The distribution of baseline scores across severity categories of the AUDIT were 20.5% (n = 26) for abstainers, 48.8% (n = 62) low risk alcohol use, 16.5% (n = 21) risky or harmful alcohol use, and 14.2% (n = 18) with likely alcohol dependence. Stratifying the VGS self-harm subscale with a cut-off at 21 [25] found 96.9% (n = 123) of participants were classified as problem gamblers at baseline.
Outcome measures
Results from final linear mixed models are presented in Table 2 (estimates and confidence intervals). Time and time squared (quadratic term) were significant in all models except AUDIT. Table 3 presents predicted values for each significant outcome variable. Predicted values indicate that improvement occurs at a faster rate from baseline to approximately 3 to 6 months and then slows down with a levelling effect from 6 to 12 months. Reliable change indices and effect sizes were calculated to facilitate a meaningful interpretation of changes in outcome measures. The following paragraphs provide an interpretation of each significant outcome measure.
Linear mixed model estimates (95% confidence intervals) for outcome measures
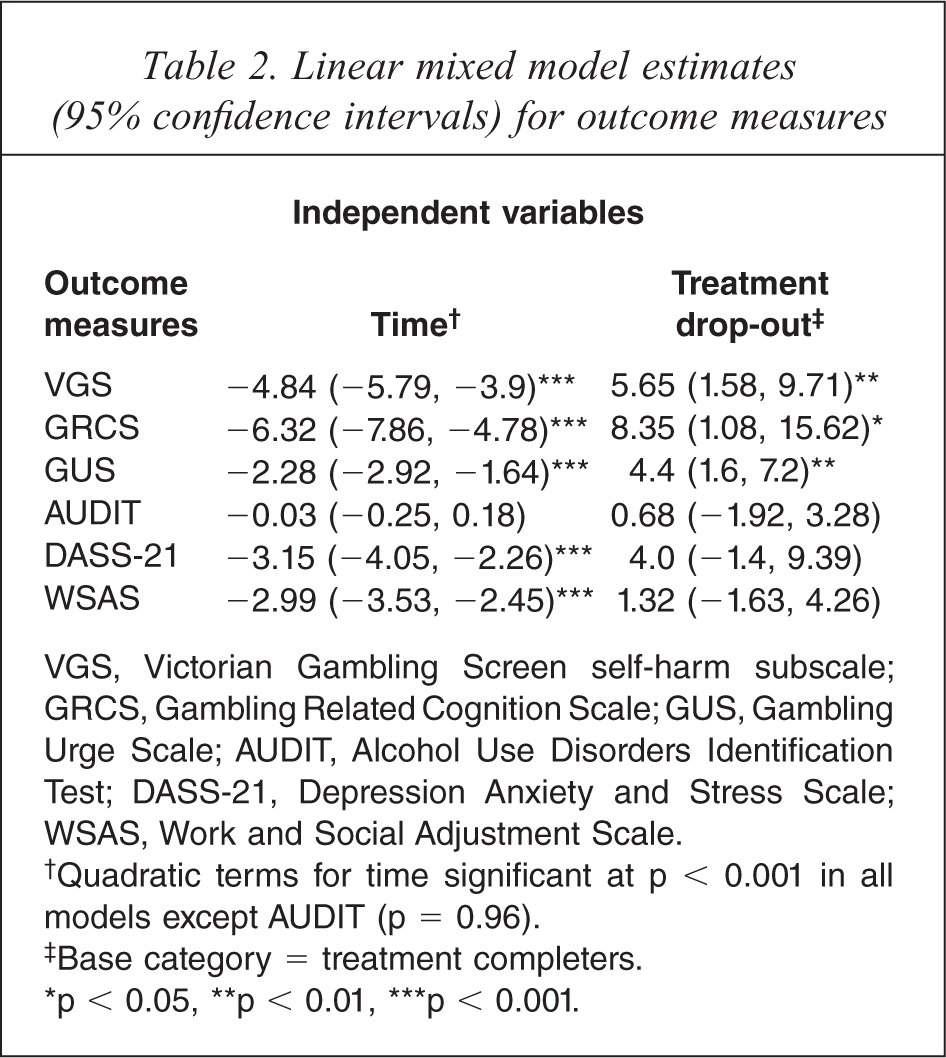
VGS, Victorian Gambling Screen self-harm subscale; GRCS, Gambling Related Cognition Scale; GUS, Gambling Urge Scale; AUDIT, Alcohol Use Disorders Identification Test; DASS-21, Depression Anxiety and Stress Scale; WSAS, Work and Social Adjustment Scale.
†Quadratic terms for time significant at p < 0.001 in all models except AUDIT (p = 0.96).
‡Base category = treatment completers.
∗ p < 0.05, ∗∗ p < 0.01, ∗∗∗ p < 0.001.
Predicted estimates (95% confidence intervals) for each outcome measure by time
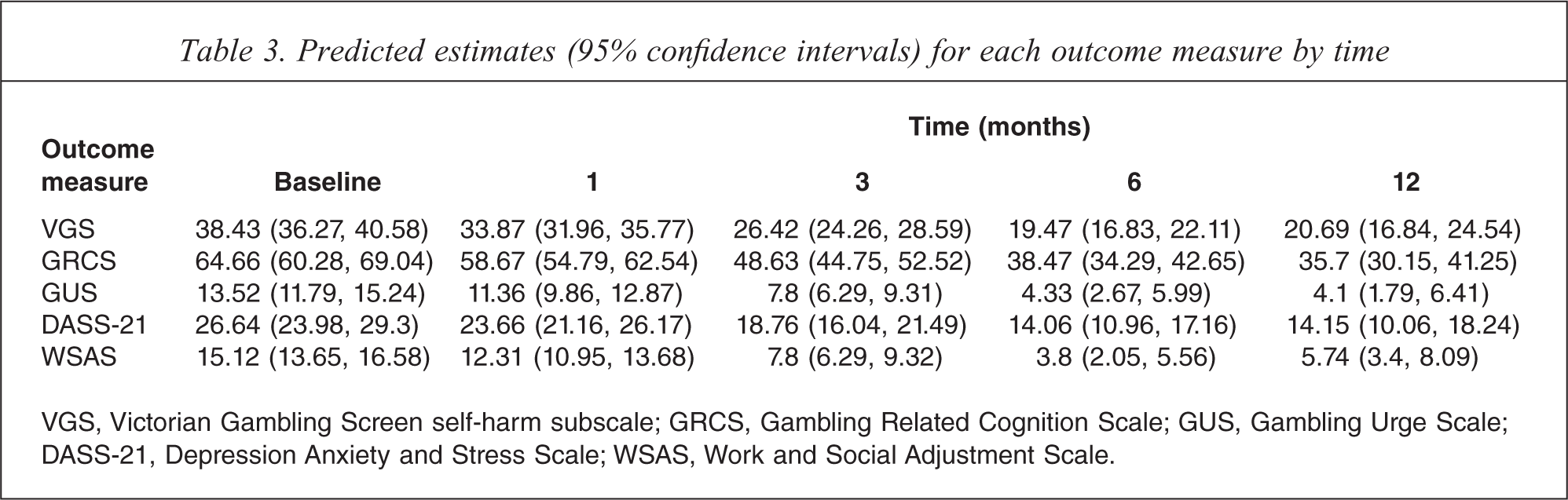
VGS, Victorian Gambling Screen self-harm subscale; GRCS, Gambling Related Cognition Scale; GUS, Gambling Urge Scale; DASS-21, Depression Anxiety and Stress Scale; WSAS, Work and Social Adjustment Scale.
Victorian Gambling Screen harm to self subscale
For each one month change in time a participant's VGS score, on average, would decrease (improve) by 4.84 units. In terms of confidence intervals this decrease could be as low as 3.9 or as high as 5.79 units. Treatment drop-outs at a given time in the study period were, on average, estimated to have higher problem gambling scores by 5.65 units than treatment completers and could be as low as 1.58 or as high as 9.71 units.
For participants with 3 or 6 month VGS scores (n = 82) there was a clinically significant improvement with a large effect size (Cohen's d = 1.27, p < 0.001). A reliable reduction (improvement in symptoms) in scores from baseline to follow up (RCI = 8.9) was found for 57 (69.5%) individuals, while 2 (2.4%) experienced an increase (worsening in symptoms) in scores and 23 (28.1%) with no change.
Gambling-related cognitions
On average, participant scores for gambling-related cognitions (decreased) by 6.32 units for each one month change in time and could be as low as 4.78 or as high as 7.86 units. Treatment drop-outs, on average, had higher scores than treatment completers by 8.35 units at a given time and could be as low as 1.08 or as high as 15.62 units.
At follow up (n = 80) there was a clinically significant improvement in GRCS scores with a large effect size (Cohen's d = 0.86, p < 0.001). A reliable reduction (improvement in symptoms) in scores from baseline to follow up (RCI = 20.91) was found for 37 (46.3%) individuals, while 43 (53.7%) experienced no change.
Gambling urge
For each change in time by one month, urge to gamble scores decreased (improved) on average by 2.28 units and could be as low as 1.64 or as high as 2.92 units. At any given time treatment drop-outs had higher urge scores, on average, by 4.4 units and could be as low as 1.6 or as high as 7.2 units.
At follow up (n = 83) there was a clinically significant improvement in GUS scores with a medium effect size (Cohen's d = 0.77, p < 0.001). A reliable reduction (improvement in symptoms) in scores from baseline to follow up (RCI = 8.57) was found for 33 (39.8%) individuals, while 6 (7.2%) experienced an increase (worsening in symptoms) in scores and 44 (53%) with no change.
Psychological distress
On average, DASS-21 scores measuring general psychological distress decreased (improved) by 3.15 units for each change in time by one month and could be as low as 2.26 and high as 4.05 units. There was no significant effect from participant's treatment completion status on outcome scores measuring psychological distress.
At follow up (n = 81) there was a clinically significant improvement in DASS-21 scores with a medium effect size (Cohen's d = 0.66, p < 0.001). A reliable reduction (improvement in symptoms) in scores from baseline to follow up (RCI = 8.77) was found for 43 (53.1%) individuals, while 6 (7.4%) experienced an increase (worsening in symptoms) in scores and 32 (39.5%) with no change.
Work and social adjustment
For each one month change in time a participant's work and social adjustment score (WSAS), on average, would decrease (improve) by 2.99 units. In terms of confidence intervals this decrease could be as low as 2.45 or as high as 3.53 units. There was no significant effect from participants’ treatment completion status on WSAS scores.
At follow up (n = 67) there was a clinically significant improvement in WSAS scores with a large effect size (Cohen's d = 1.16, p < 0.001). A reliable reduction (improvement in symptoms) in scores from baseline to follow up (RCI = 10.36) was found for 30 (44.8%) individuals, while 37 (55.2%) experienced no change.
Treatment drop-out
The extent to which potential predictor variables were related to treatment drop-out was assessed using logistic regression. Variable selection for an initial full model commenced with univariate analyses of age, sex, marital status, education level, employment status, living arrangement, duration of problem gambling, and baseline scores on Trait Anxiety Inventory (TAI), Arnett Inventory of Sensation Seeking (AISS), and Multidimensional Scale of Perceived Social Support (MSPSS). Variables significant (P < 0.25) for advancement to a multivariate model were AISS, TAI, and marital status. Removal of further variables resulted in significant differences between log likelihoods and therefore the final model comprised all variables entered into the initial multivariate model.
Table 4 describes the association between predictor variables and treatment drop-out in the final model with odds ratios, 95% confidence intervals, Wald statistics and p values. A significant predictor of treatment drop-out at the p < 0.05 level was the baseline measure of sensation seeking traits (AISS). For each one unit increase on the AISS the odds of participants dropping out from treatment over completing treatment increased by 6% and could be as low as 1% or as high as 11%. Although the indicator variable ‘separated/divorced’ was significant relative to participants married or in a de facto relationship, overall marital status was not a significant predictor (p = 0.139).
Multivariate prediction of treatment completion status
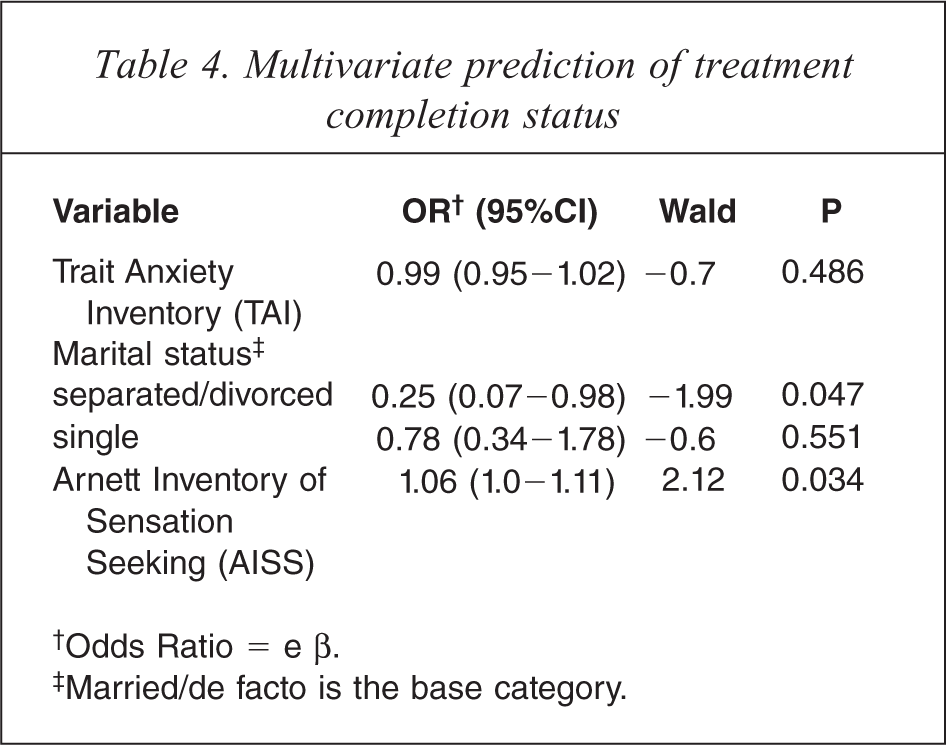
†Odds Ratio = e β.
‡Married/de facto is the base category.
Discussion
The purpose of this study was to measure self-reported gambling-related outcomes and the treatment compliance of help-seeking problem gamblers in order to determine effectiveness of the Statewide Gambling Therapy Service programme in South Australia. Demographic characteristics of the study cohort were comparable with problem gamblers from a previous study in South Australia [40].
Results showed clinically significant improvement from baseline to short and mid-term follow up time points in gambling-related cognitions, urge to gamble, general psychological distress, and impaired functioning with work and social activities. A clinically reliable improvement with large effect size was found for 69.5% of participants with available data on the Victorian Gambling Screen at follow up. Results from a previous study have demonstrated improved outcomes for an exposure with response prevention intervention compared to group cognitive re-structuring and a combined approach in a randomized waiting list controlled trial of 64 pathological gamblers [41]. Treatment success, defined as abstinence or the occurrence of only 1 or 2 episodes of gambling during the study period at 6 month follow up, was found for 10 (62.5%) individuals. Another randomized trial assessing cognitive behavioural therapy (CBT) found 59% of problem gamblers were classified as recovered using combined indices of SOGS scores and dollar amounts wagered to evaluate clinically significant changes during the treatment period [42]. Results of the present study are comparable with other studies of psychological treatments for problem gambling as gambling-related symptoms were shown to decrease for a majority of participants.
Alcohol use scores over time did not change significantly, which is not surprising as baseline AUDIT scores indicated more than 69% of participants were classified as either low risk users or abstainers from alcohol. A population-based cross-sectional study conducted in South Australia [40] found over 91% of problem gamblers self-reported as no or low risk alcohol users. The relatively low rates of moderate to high risk alcohol use in both the SGTS cohort and the cross-sectional survey indicates further research into prevalence rates in problem gambling and co-morbidities such as alcohol use is required. Previous studies have established positive associations between harmful alcohol use and problem gambling [43–45].
We found 41 (32%) of participants were classified as treatment drop-outs. A recent systematic review of psychological treatment drop-out among pathological gamblers found drop-out ranged from 14% to 50% with a median of 38% and weighted average of 32%. A variable for treatment drop-out was included in statistical models to test for effects on outcome measures. With treatment drop-outs defined as participants completing three or less therapy sessions, it was found that this group's scores for gambling urge, gambling screen, and gambling-related cognitions were significantly higher than treatment completers at any given time. However, scores for treatment drop-outs still significantly improved over time on all outcome measures except alcohol use. This may, at least partly, be attributed to some participants classified as treatment drop-outs having experienced therapeutic effects earlier in their treatment programme. Statistical models with significant time and treatment group effects also included a quadratic term indicating an initial improvement occurring at a faster rate followed by an approximate levelling off in the time period 3 to 12 months. Further discussion of the use of exposure therapy in problem gambling may be found in a recent case study report [18] and book chapter [17].
Clinical interpretation of results from treatment compliance effects on outcome measures may be limited due to the definition of treatment drop-out. With two common approaches for defining treatment drop-out (therapist determined and attendance at a specified number of sessions) inconsistencies across the research literature in defining treatment drop-out still remain [11]. Also drop-outs in this study were participants who had engaged in at least one session (initial screening) and therefore did not account for drop-outs prior to commencing treatment. This is also a problem as recently it has been shown that even single sessions can influence outcome significantly [46] and that this could also explain the reduction in outcome measures by the drop-outs in this study. Further research needs to examine the varying definitions of treatment drop-out and associated client characteristics as well as outcomes. Potentially important predictors of treatment drop-out such as environmental stressors and other psychological variables will also need further exploration to improve validity of results.
We also attempted to identify baseline client characteristics associated with treatment drop-out. Candidate predictor variables included demographic variables and baseline measures of anxiety, perceived social support, and sensation-seeking traits. A significant predictor of treatment drop-out was found to be higher sensation-seeking traits. While no previous studies have directly investigated the predictive properties of sensation-seeking in treatment drop-out for problem gambling, a related construct of impulsivity traits has been found to be significantly associated with drop-out [47]. Other studies investigating sensation-seeking and problem gambling have found higher levels associated with gambling types involving skills (for example racetrack gambling) [48], those who bet on several gambling forms [49], and problem gambling in youth gamblers [15]. To improve treatment retention in subgroups of problem gamblers, gambling help services would greatly benefit from further research into factors associated with drop-out including any interaction effects between age, gambling forms, and sensation seeking traits.
Limitations of this study are acknowledged. Whilst significant improvements in self-reported measures have been demonstrated over time for this group, this study is not controlled and therefore we are not able to determine specific causes of the changes being observed. For example, some clients may have received additional support or interventions from other gambling help services across the state such as self-help peer support, financial counselling, and helpline counselling. Also, as a result of treatment and study attrition in follow up, it is possible that the improvements shown are due to the influence of those clients who stayed in treatment longer and participated in follow up assessments. In an attempt to minimize missing data effects on study precision and power we used linear mixed models. Mixed models use all available data and reduce bias that may result with more traditional statistical methods for the analysis of repeated measurements [35].
Also, this study is comprised of limited problem gambling features when compared to agreed minimum features of the Banff consensus [30] for reporting treatment efficacy studies in problem gambling. Outcome measures reported in the present investigation focused on gambling-related problems such as mental health, relationships, and work and social functioning. Other elements that require examination are frequency/intensity of gambling behaviour (for example, net financial loss) and the process of change as a direct result of the treatment. Investigation of potential mediation effects from variables such as client–therapist fidelity will further contribute to our understanding of treatment outcomes for SGTS clients.
In summary, this report begins to define the demographic, treatment compliance and therapy outcomes being achieved for clients in the Statewide Gambling Therapy Service in South Australia. The initial results presented here for a small cohort of clients suggests that those who access and participate in the programme generally achieve significant improvements in their gambling-related problems over time. By better understanding the nature and complexity of the clients accessing this service, it will be possible to structure treatment programmes more specifically in order to engage clients who are in need of support, keep them in treatment for sufficient time to ensure improved outcomes and to tailor the therapy programme to the needs of individual clients.
Footnotes
Acknowledgements
We are grateful to the patients participating in this study and the therapists and administrative staff of the SGTS who collected the data and worked with the patients.