
Abstract
Keywords
After decades of deinstitutionalization, an extensive body of evidence-based research has established strategies for the treatment and rehabilitation of schizophrenic disorders. These strategies can markedly reduce clinical, social and carer morbidity as well as the costs of mental health resources. However, few services provide more than a pharmacotherapy component, and evidence-based psychosocial support is seldom applied in a manner that achieves the results obtained in clinical trials [1, 2]. Several reviews of the clinical trial literature have concluded that individuals with schizophrenia should be provided with: (i) the optimal dose of antipsychotics; (ii) strategies to educate themselves and their caregivers, usually relatives, about methods for effectively coping with environmental stresses; (iii) pharmacological and psychological strategies for persisting residual symptoms; and (iv) assertive home-based management to help prevent and resolve major social needs and crises, including episodes of symptoms [3–7].
Despite strong scientific support for the routine implementation of these ‘evidence-based’ strategies including psychosocial rehabilitation, this is seldom applied in the manner associated with the best results in the clinical trials [4]. In 1994, an international collaborative group was established with the goal of promoting the routine use of evidence-based strategies for mental disorders with continued evaluation of clinical, social, carer and economic outcomes. This collaboration became known as the Optimal Treatment Project (OTP) and preliminary results are published elsewhere [2, 8].
On the other hand, few long-term follow-up studies have been conducted on patients discharged after long periods in psychiatric hospitals. Most of the previous studies were anecdotal or polemical, and there is a relative lack of well-constructed outcome studies to support or refute the validity of deinstitutionalization [9]. In the UK, deinstitutionalization has been occurring in the context of a national health service plan, providing organized community care. The most comprehensive study for assessing the effects of the closure of mental hospitals was carried out in London in the 1980s (the Team for the Assessment of Psychiatric Services study) [9–11]. In Australia, the National Mental Health Strategy recommends the provision of care in the least restrictive setting. Hobbs et al. [12, 13] previously reported detailed results regarding comprehensive community care, accommodation, 24-hour supervision and funding provided. The extensive documentation provided by other social environments enables clear comparisons of a wide range of clinical and social variables to be made between patient relocation programs of this kind.
Japan still has a huge number of psychiatric beds. Consequently, psychiatric services remain predominantly hospital-based. A decline in hospital beds was observed from 1994, but the total number of inpatient beds is still 2.9 per 1000 people [14], compared with 0.9 in the UK and 0.5 in the US [15]. Such reliance on hospital-based psychiatry is a barrier to the development of community-based psychiatry. However, according to several surveys [16], about 30% of patients in psychiatric hospitals have been capable of living within the community with available community support programs. Even though the rationale for a transition from hospital-based to community-based psychiatry services can be understood from a policy-making perspective, the actual resettling of institutional residents raises questions about the program's feasibility, the potential benefits for patients, public safety and costs [17].
In 2002, the Sasagawa Project was established to make the transition from a hospital to a residential facility while ensuring both the quality and continuity of care for long-stay patients with the goal of promoting the routine use of evidence-based strategies for the mental disorders of people discharged from the mental hospital. This is an ongoing, prospective, pragmatic, observational study that has been developed to provide clinical information about Japanese inpatients with schizophrenia. The treatment strategies of Sasagawa Project were based on those of the OTP. We previously published a preliminary report on the closure of a longstay hospital and the community tenure of the 78 patients discharged in the first year of the Sasagawa Project [18]. Here, we present the clinical and social outcomes 2 years after the hospital closure.
Method
Subjects
The criteria for selection and the sociodemographic characteristics of the patients who took part in this study have been reported in detail elsewhere [15]. The study design and treatment protocols for the hospital closure were also described in the same paper. In total, 94 people were discharged from Sasagawa Hospital when it closed on 31 March 2002; 78 people with schizophrenia were followed up in the present study. All 78 patients (51 men) were diagnosed by ICD-10 [19] as having chronic schizophrenia (paranoid type 34, residual type 42, simple type 2) by two independent psychiatrists. The mean score of Global Assessment for Functioning (GAF) [20] was 57.5 (range: 25–82), and the mean positive, negative and general scores of Positive and Negative Syndrome Scale (PANSS) [21] were 9.0 (7–25), 19.0 (7–29), and 26.5 (16–41), respectively. These 78 people with chronic schizophrenia were then prospectively evaluated throughout a 5-year period. The Institutional Review Board approved the study's protocol. The study was explained to the patients by the principal investigators. Written informed consent was obtained from all patients before participation in the project.
Community care management
The project started 10 months prior to closure of the Sasagawa Hospital. The Sasagawa Hospital was founded for the psychiatric rehabilitation of people with chronic mental illness in 1978. Most of these patients had no relatives willing or able to provide them with a place to live in the community. Most suffered from severe persistent psychotic and residual symptoms and had frequent admissions to the acute unit. The Sasagawa Hospital would close at the end of March 2002. The building would be restructured to provide: (i) a residential facility, the ‘Sasagawa Village’; and (ii) a community support centre called ‘I CAN’. The refurbished buildings would provide living facilities similar to Japanese homes, such as tatami flooring, spa baths, etc. A project team of 23 multidisciplinary members was recruited and a non-profit organization was founded. These two facilities would be managed by the non-profit organization. A range of acute services, such as day–night hospital and community nurse visits, would be provided as necessary by Asaka Hospital. Continuous cognitive behavioural therapies based on the OTP manualized protocols [22] would be provided to patients before and after the hospital closure. An information system would be developed to document the process and outcomes of the project by all members of the multidisciplinary team.
All the professional staff, including two psychiatrists, 11 nurses, two occupational therapists, three social workers, one psychologist, four administrators, in contact with residents of Sasagawa Village were trained to implement the OTP strategies for mentally disordered people living in the community [2, 23]. This included a full range of empirically based treatment strategies that have been associated with improved clinical, social and family outcomes for psychotic disorders (optimal pharmacotherapy, assertive community treatment, psychoeducation, carer-based stress management, social skills training, supported employment and specific cognitive behavioural strategies for persistent residual psychotic and non-psychotic symptoms and behavioural problems).
The training courses for the professional staff were repeated regularly. Residents of Sasagawa Village, participated in training programs focusing on problem-solving of their day-to-day stresses and life changes associated with their efforts to achieve their personal life goals. They also received biomedical and psychosocial treatment strategies to cope with residual psychotic, negative and anxiety symptoms, or antisocial behaviours. Early recognition of exacerbations resulted in assertive intensive care being provided by the professional staff with the support of additional staff from the acute unit at nearby Asaka Hospital.
Psychiatric medical management, community rehabilitation programs and crisis intervention were provided by Asaka Hospital, where hospitalization was available when necessary.
In the Sasagawa Village, the autonomy of patients was respected. The project plan was discussed repeatedly with patients, their families and people who were residents in the neighbourhood of the hospital/residence. Daily personal schedules were planned in meetings between residents and professional staff. Residents were encouraged to pursue daytime activities based on achieving their own personal goals, and most of them attended the day treatment program at Asaka Hospital four times per week. This provided mental and general health education, structured group problem-solving and interpersonal skills training. Nine months after discharge, the residents who wished to work were enrolled in a job-coaching program for sheltered jobs. Although the mean age of the subjects was high, the residents were generally eager to participate in the job-training course. The jobs included laundry assistance, floor cleaning, cooking and delivery, and rubbish sorting. The job courses consisted of several levels from basic training to professional. Earnings were paid depending on the level of training attained. Other activities, including clubhouse programs, leisure activities and adult education courses, were also developed for the residents.
Design
The major aim of this study was to assess the patients' social and clinical outcomes during a 2-year post-discharge period. The patients were assessed at nine time-points on seven scales. All patients were assessed at baseline before discharge and those who did not die were assessed at 1, 3, 6, 9, 12, 15, 18, 21 and 24 months post-discharge. Patients who were hospitalized at the time of follow-up were included, although some of the scales were omitted that were not relevant.
The seven scales and sets of assessments were described in detail by Mizuno et al. [18]. The clinical measures that were used included the GAF [20], the PANSS [21], the Schedule for Assessment of Insight (SAI) [24], the Rehabilitation Evaluation Hall and Baker (REHAB) Scale [25], the Social Functioning Scale (SFS) [26], the Drug Attitude Inventory (DAI) [27] and the Mini-Mental State Examination (MMSE) [28]. Premorbid function was also assessed by modified Premorbid Adjustment Scale [29] at the time of discharge. The amount of neuroleptic medication (chlorpromazine equivalent) and the body mass index (BMI; weight [kg]/height [m2]) were also measured at the time of discharge and throughout the 2-year period.
Statistical analysis
The survival and dropout rates for each incident category were illustrated by the Kaplan-Meier method. Survival was defined as time from hospital discharge until the occurrence of any incident that made the continued stay at Sasagawa Village impossible during the 24-month observation period. To examine the effects of time since discharge on the clinical measures, all outcome variables including PANSS, GAF, SAI, REHAB, SFS, DAI, MMSE and chlorpromazine-equivalent drug dosage were compared between 0 and 24 months using paired t -tests or Wilcoxon signed-rank tests after log transformation, when appropriate. A multiple regression analysis was employed to explore the impact of various demographical and clinical factors on outcome measures, such as PANSS, GAF, etc. over the 24-month study period (Δ0–24). The Δ0–24 value was determined by subtracting the outcome index at 24 months from that at 0 months, and was distributed normally. A value of p < 0.05 was considered to be statistically significant. All analyses were done using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA).
Results
Case history profile
During the study period of 24 months, 18 cases had incidents that made their continued stay at Sasagawa Village impossible (Fig. 1). The incidents were classified into three categories: (1) psychotic exacerbations; (2) physical conditions; and (3) accidental deaths.
Four residents had major psychotic or affective exacerbations and were admitted to the acute unit and returned to Sasagawa Village after a few days to couple of months of intensive care; one patient had stupor with psychomotor excitation and three had persecutory delusions about interpersonal issues. Only four (5%) of the 78 patients were readmitted to psychiatric wards because of exacerbations. The average length of readmission was 73.5 days (range: 7–195 days). Twelve people were admitted to hospital with serious physical illnesses. Five did not return to Sasagawa Village because they experienced a worsening of their mental condition or some other complications during hospitalization for intestinal cancer (two cases), an operation for an ossified posterior longitudinal ligament, diabetes mellitus, or a coronary artery bypass graft operation. The other seven were admitted with acute myocardial infarction and diabetes mellitus, angina, adynamic ileus, dysmenorrhea, hepatitis C, or pneumonia (two cases), but all returned to Sasagawa Village after their discharge (range: 3–221 days). One resident committed suicide at Sasagawa Village during a major depressive episode, and one drowned in the garden pool; the circumstances of her death appeared accidental. Kaplan-Meier curves for survival among all patients, dropout by physical condition and incident, and dropout by relapse.
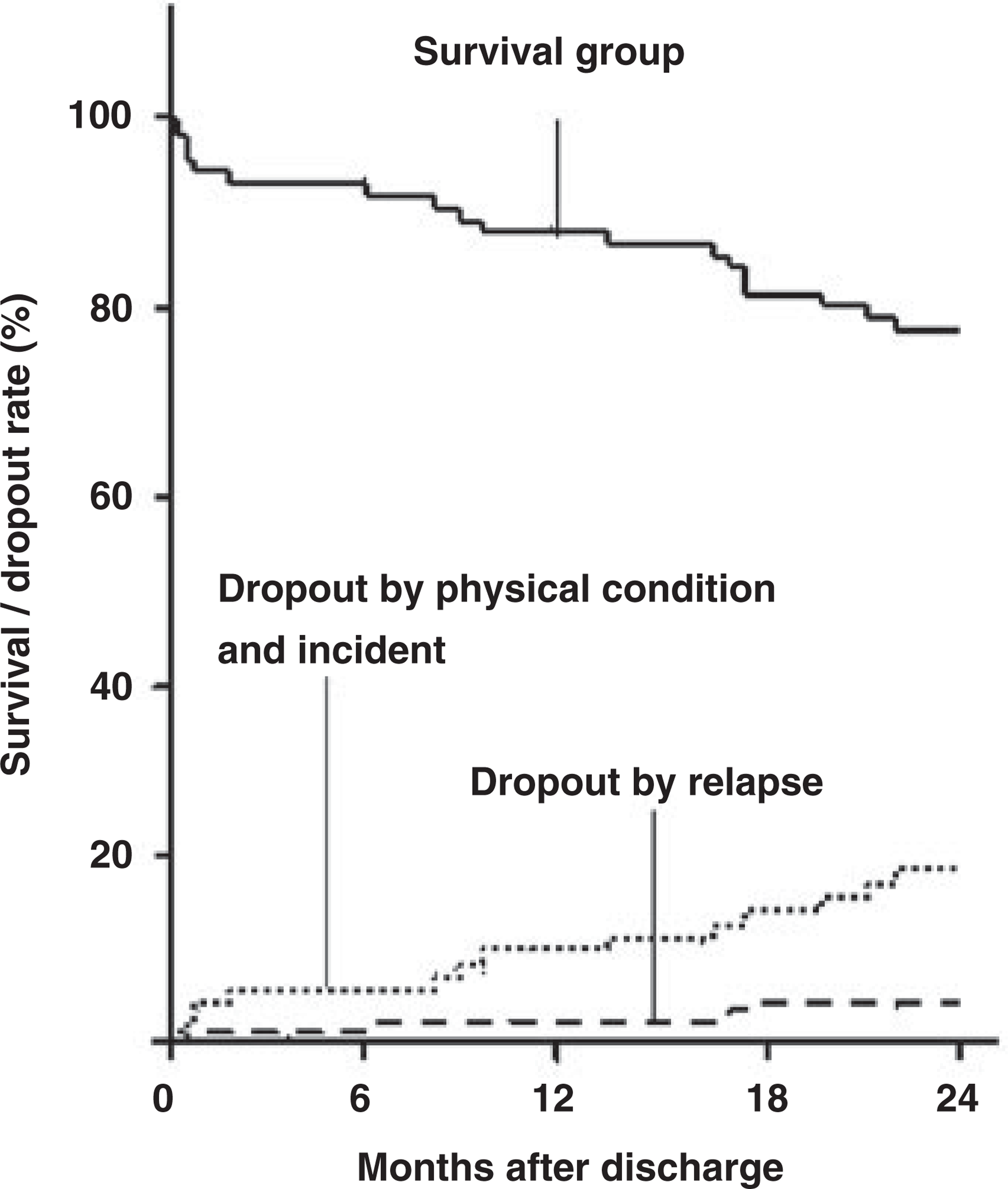
In summary, the outcome of 24 months after hospital closure was as follows: successful community tenure, 60 patients (76.9%); physical illness, 12 patients (15.4%); major exacerbations, four patients (5.1%); deaths by suicide, one or accident, one (1.3%).
Background characteristics of surviving patients
Sixty residents (77%) were not readmitted to mental or physical hospitals during the 2-year follow-up period. The demographical characteristics of these 60 cases were as follows: the mean age was 54.7 years (range: 34–65), and 38 of the residents were men; the mean years of education was 10.5 years (9–16), and three had spouses, 13 other residents had once married; the mean pre-discharge length of stay was 26.0 years (3.8–43.9), and the mean number of admissions was 2.6 (1–6); the mean age at onset of psychiatric problems noted in the medical records was 22.8 years (13–46), and only one person had a history of a suicide attempt; the mean dose of neuroleptic medication prior to discharge (Chlorpromazine mg equivalent) was 661.8 mg day − 1 (66.7–1800.0); the mean MMSE score was 26.0 (17–30); the percentage of their lives spent hospitalized was 47.6% (11.2–71.5).
A comparison of the four cases who were readmitted because of a relapse in their psychiatric symptoms and the 60 surviving residents showed evident differences in the PANSS positive (15.0 and 9.7, respective mean scores) and general scores (33.5, 26.7), GAF (44.0, 58.6) and the Disturbed Speech score of REHAB (8.0, 5.4) at the time of discharge.
During the second year after discharge, two patients moved to facilities for less intensive care, one to a welfare home and another to a normal apartment. Other patients have also expressed the desire to move and become more independent. The staff of Sasagawa Village and the affiliated Asaka Mental Hospital is also working to manage the transition of patients back into the community.
Sheltered jobs
Job coaching was started 9 months after deinstitutionalization. After 2 months of training, including interpersonal communication skills, nine people (six men) have started jobs working as floor cleaning or cooking assistants. One person dropped out of the job-training program after 2 months because of a relapse in her psychotic symptoms, but the remaining residents continued to work and are learning more advanced skills; the other four residents (two men) have also recently started the program.
Longitudinal characteristics of survivors
Outcome measures
The changes in the outcome measures over time are presented in Table 1. The results for demographic, treatment and case history covariates entered into the model are compiled in Table 2.
The changes in the outcome measures over time
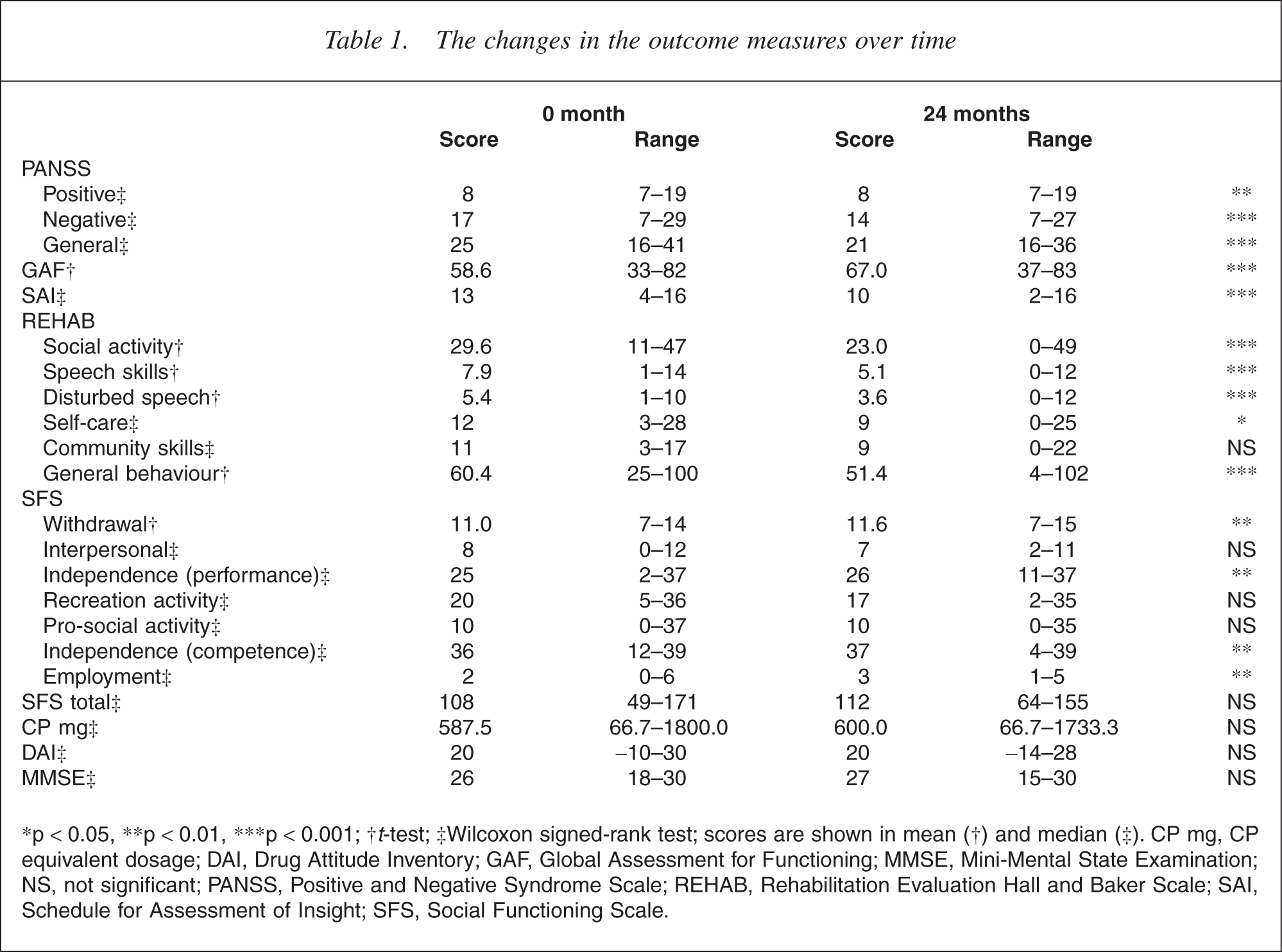
∗p <0.05, ∗∗p <0.01, ∗∗∗p <0.001; †t-test; ‡Wilcoxon signed-rank test; scores are shown in mean (†) and median (‡). CP mg, CP equivalent dosage; DAI, Drug Attitude Inventory; GAF, Global Assessment for Functioning; MMSE, Mini-Mental State Examination; NS, not significant; PANSS, Positive and Negative Syndrome Scale; REHAB, Rehabilitation Evaluation Hall and Baker Scale; SAI, Schedule for Assessment of Insight; SFS, Social Functioning Scale.
The effect of demographic, treatment and case history characteristics on clinical outcome measures (Δ0–24)
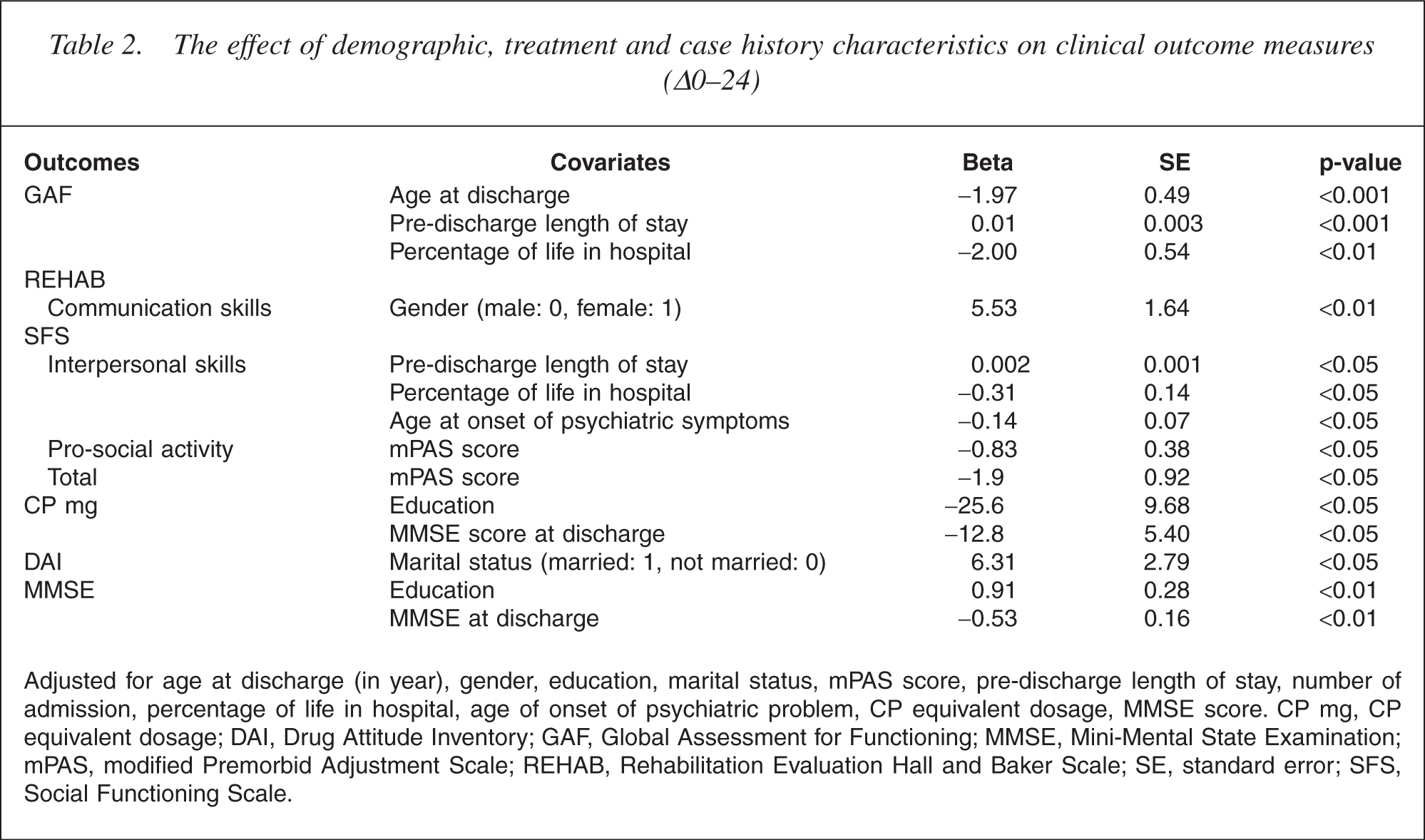
Adjusted for age at discharge (in year), gender, education, marital status, mPAS score, pre-discharge length of stay, number of admission, percentage of life in hospital, age of onset of psychiatric problem, CP equivalent dosage, MMSE score. CP mg, CP equivalent dosage; DAI, Drug Attitude Inventory; GAF, Global Assessment for Functioning; MMSE, Mini-Mental State Examination; mPAS, modified Premorbid Adjustment Scale; REHAB, Rehabilitation Evaluation Hall and Baker Scale; SE, standard error; SFS, Social Functioning Scale.
Positive and Negative Symptom Scales
Two years of community living resulted in a significant reduction in psychiatric symptoms, not only in positive symptoms but also in negative and general symptoms. However, no covariate associated with the difference between the discharge and 24-month PANSS scores was found.
Global functioning
A significant improvement in global functioning was also observed during the 2-year study period (before discharge, 58.6; 2 years after discharge, 67.0; p < 0.001). The age at discharge, the pre-discharge length of hospital stay and the percentage of life spent in hospital were associated with the difference between the pre-discharge and 24-month GAF scores (p < 0.001, p < 0.001 and p < 0.01, respectively). As shown in Table 2, for example, if the age at discharge was 1 year older, the change of GAF score was 1.97 less after 2 years, and if the percentage of life spent in hospital was 1% longer, the change of GAF score was 2.0 less after 2 years.
Insight
Unexpectedly, insight, as assessed using SAI, gradually deteriorated. No covariates could be identified.
Rehabilitation Evaluation Hall and Baker Scale
The Social Activity, Speech Skills, Disturbed Speech, Self-Care and General Behaviour scores improved significantly between the discharge and 24-month scores. Only gender was associated with Communication Skills (p < 0.01); the mean Communication Skills score of men improved 5.53 points more than that of women after 2 years.
Social Functioning Scale
After 24 months of living in the community, Withdrawal, Independence (Performance), Independence (Competence) and Employment improved significantly.
As shown in Table 2, the score of modified Premorbid Adjustment Scale was associated with pro-social activity and the total SFS score. The pre-discharge length of stay, percentage of life spent in hospital, and age at onset of psychiatric problems were significantly associated with the Interpersonal Scores.
Pharmacotherapy
The overall neuroleptic dosage remained unchanged over the 2 years of the follow-up period, and the highest level of education and MMSE scores were associated with the total neuroleptic dosage. If the time spent in education was 1 year longer, the prescribed CP dosage was 25.6 mg less after 2 years; and if the MMSE score at discharge was one point higher, the prescribed CP dosage was 12.8 mg less.
Drug Attitude Inventory
Drug attitude was unchanged over the 2-year follow-up period but was associated with marital status. Married people improved 6.31 points more in DAI scores after 2 years.
General cognitive functioning
The MMSE score remained unchanged over the 2-year follow-up period.
Weight change
The BMI, a parameter of obesity, significantly changed from 24.5 ± 2.73 at discharge to 25.1 ± 2.98 at 24 months thereafter.
Discussion
The Sasagawa Project, a 2-year follow-up study on patients with severe and persistent chronic schizophrenia, suggested that a smooth transition from hospital to community-based care could be undertaken under some conditions in Japan.
During the follow-up period, only four residents had major psychotic or affective exacerbations and were admitted to the acute psychiatric ward. In 2 years after hospital discharge, 77% of the patients remained in community residence without having experienced any interruptions from major exacerbations of their mental disorders or physical illness. No reported incidents of criminal activity, violence or homelessness occurred. Careful planning that minimized social and clinical dislocation may have contributed to this successful transition.
A study on deinstitutionalization for long-term mental illness in Australia [12] showed that high levels of community tenure can be achieved when a well-organized program of hospital closure is undertaken. The community care management strategies used in the Sydney study were similar to those used in our project, with comprehensive community care, accommodation, 24-hour supervision and funding being provided. They reported that 7 of 47 (14.9%) chronic psychotic patients who had been transferred to the community required permanent readmission to hospital during a 2-year follow-up period and 13 patients (37%) experienced at least one temporary readmission. Thirty-five (71.2%) patients remained in a community setting for 2 years, most living in four residences in different areas of the city. Regrettably, the rating scale data from these two studies cannot be compared directly because no common measures exist between them. In the present study, the same facility that had been used as a hospital where the patients had been admitted for long periods was used in the Sasagawa Project, saving capital investment and minimizing the stress of patients having to adapt to a totally new environment. Securing new accommodation for huge numbers of long-stay inpatients is a very difficult issue from an economic perspective in Japan and perhaps in other countries. The transformation of psychiatric hospitals into community residences may facilitate deinstitutionalization.
In Italy, Mastroeni et al. have been engaged in the closing of one of the largest public mental hospitals in Northern Italy [30]. Very similar staff training in evidence-based treatment was employed and an intensive program of rehabilitation provided for 6 months before discharge. This resulted in similar high rates of resettlement and lasting clinical and social benefits throughout a 5-year follow-up period.
These results suggest that goal-orientated interventions focusing on training patients in the skills needed to live in a community may be superior to case management and milieu-type strategies for maintaining community tenure and social functioning.
During the planning of this project, we were afraid that the drastic changes in living circumstances might exacerbate the patients' psychiatric symptoms. The results were the reverse, and none of the residents were permanently readmitted because of psychotic exacerbations. Each of the PANSS subscores and the GAF score improved remarkably over the 2-year follow-up. None of the covariates examined were associated with these scores. The total dosage of prescribed neuroleptics remained unchanged over the 2-year follow-up. Thus, these symptom improvements could be regarded as the results of significant changes in lifestyle and the effects of a multidisciplinary team applying a comprehensive approach, including cognitive-behavioural strategies. In particular, the negative symptom score and the general score improved significantly at 24 months after discharge. Similar results were seen for the GAF score.
The deterioration on the measure of insight is puzzling. This may be accounted for by the intensive mental health education provided during the pre-discharge phase that was not followed by regular booster sessions. Thus, initially improved understanding of their mental disorders was not maintained, particularly in this group of elderly chronic patients. Frequently repeated education sessions may be necessary.
Although SFS was developed specifically to evaluate those areas of functioning that were crucial to the community maintenance of individuals with schizophrenia and covered not only the presence of social problems but also the strengths and weaknesses, no remarkable improvement in the SFS total score or the subscores on interpersonal or performance, pro-social activity was seen. Participation in day-care programs, which was strongly encouraged in Sasagawa Village, was associated with a significant improvement of Withdrawal score. Similarly, the job-coaching program begun 9 months after discharge led to a significant improvement in the Employment score during the second year. This result could be seen as disappointing, but the SFS does not evaluate many aspects of daily activities or performance. In previous studies [11, 12], the Social Behaviour Scale [31] was used to evaluate social functioning and similar results were obtained.
According to the REHAB scores, the improvements in self-care, social activities and speech functions were obtained within the first year. However, many residents of Sasagawa Village still require assistance and no significant improvements in the social living skills scores were obtained during the second year. On the other hand, some patients improved to the point where they were able to move to a less intensively supervised group home or a normal apartment. The improvements in living skills must be stimulated and supported by appropriate and crucial need for participation in daily chores.
Interestingly, the DAI scores showed a constant positive attitude to pharmacotherapy, and this attitude was sustained throughout the follow-up period. Intensive psychoeducation on the necessity and efficacy of pharmacotherapy produced good drug adherence, helping to minimize relapses.
As shown in Table 2, the relationship between education, MMSE score at discharge and prescribed neuroleptics are unexpected; that is, higher education and better general cognitive functioning at discharge were associated with an increase in the prescribed neuroleptics at 24 months. To the authors' knowledge, there is no previous research on the relationship between education or intelligence and prescribed medication dosage.
The significant increase in BMI suggests that some of the physical problems may have been exacerbated by poor nutrition. Before the discharge, all the patients' meals were carefully controlled by registered dietitians, as in other Japanese hospitals. After discharge, the patients had to choose what they would eat for meals and snacks. Many patients tended to eat junk food. Psychoeducation on nutrition and cooking school classes in the day-care program were well received by the Village residents. Thereafter, the residents began to pay more attention to their eating behaviour and the increase in the BMI slowed during the second follow-up year (BMI: 25.0 at 12 months, 25.1 at 24 months). Mental health services should pay attention to and investigate physical problems related to the ageing of long-stay patients and nutritional lifestyle changes.
The four cases who were permanently readmitted because of psychiatric relapses had higher scores of PANSS positive and general, lower GAF and higher REHAB Disturbed Speech scores. Although several cases with higher PANSS and lower GAF scores at discharge survived, most of the scores for the above four patients were greater than 1 standard deviation. Higher positive symptoms, lower global functioning scores and Disturbed Speech (sense, clarity and initiation) seem to predict poor adaptation to community living. These characteristics were partially associated with risk factors for failing to resettle long-stay patients in community facilities in the Team for the Assessment of Psychiatric Services study [9–11]. No significant difference in the CP prescribed dosage at discharge was seen between the surviving cases and these four cases, despite the finding by Hobbs [12] that high levels of neuroleptic medication at discharge increase the risk of unsuccessful resettling.
According to the present study, the major factors predicting permanent readmission to a mental hospital in patients resettled in a community facility with comprehensive care was not a deterioration in mental state, but poor physical conditions caused by ageing or unhealthy lifestyles.
Clinical improvements support the community transfer of individuals with long-term mental illness when planned with adequate resources, comprehensive community psychiatric services, rehabilitation programs and access to mental health care on a 24-hour basis [11, 12]. Integrated multidisciplinary approaches and cognitive behavioural rehabilitation aimed at the recovery of social functioning should be further developed.