
Abstract
The disproportionate ‘indirect’ cost burden of schizophrenia has been widely acknowledged, attributable in large part to social and occupational dysfunction [1, 2]. Vocational rehabilitation, which seeks to address this dysfunction, is widely viewed as an essential component of rehabilitative care for persistently ill psychiatric populations [3]. A range of models have been endorsed to facilitate functional recovery; however, cost-effective studies of vocational rehabilitation programs are lacking.
Supported employment, in which training occurs at the job site after placement, has replaced much traditional ‘train then place’ vocational rehabilitation. Supported employment has shown superior success in placing patients in competitive employment, with one review [4] reporting a 37% increase in placement rates relative to traditional approaches. However, between 41% and 77% of supported employment clients terminated their placement within 6 months, suggesting that at least for some individuals, barriers remain and other vocational models should be explored. Neurocognitive deficits may be at least partly responsible for these limitations: they predict supported employment success [5] and are correlated with capacity to work [6, 7]. Neurocognitive deficits are strong predictors of the amount of support and contact needed among supported employment recipients [5], ratings of work performance [8, 9] and overall work outcome [6, 10].
Prior to the supported employment movement, community-based vocational training programs and ‘sheltered workshops’ were widespread. Their disfavour arose from poor outcomes both clinically and occupationally among patients with schizophrenia [11], and led to widespread adoption of psychiatric rehabilitation, in particular the Boston University Model in the 1990s which posited that better outcomes resulted when vocational activity was patient-driven, individually tailored to personal interests and abilities, and occurred in mainstream environments [12]. Traditional sheltered workshops, initially designed to serve the needs of developmentally disabled populations, failed to adhere to these principals and proved inadequate for psychiatric populations. Work tasks were often menial and inadequately matched to the far broader range of vocational skills and interests characteristic of a psychiatric population. Vocational training programs used outdated donated and second-hand equipment employing obsolete technologies that are no longer used in competitive industry. In the presence of neurocognitive deficits which interfere with transfer of skills across different environments [13], training in outdated methods is unlikely to result in successful long-term employment. Also, many vocational training programs employed scripted curricula with rigorous deadlines for acquiring skills that were ill-suited to the often fluctuating course of psychiatric disorders.
The Nassau Day Training Program (NDTP) was developed in the mid-1980s adhering to seven principals that had been specified by one of the authors (ED) in response to the above concerns.
The program is a business that is useful to the community, entailing a range of work opportunities.
The business is located in the community.
The business uses state-of-the-art equipment and technology comparable to any competitive venture.
The business maintains links to competitive industry (e.g. membership in trade organizations) with the goal of accessing mainstream jobs or work enclaves.
Training and work components are maximally flexible with respect to sequencing and duration of training phases, cognisant that clinical setbacks will occur.
A system exists for responding to status needs of those who achieve competitive industry work standards (e.g. employee ID card, a formal paycheck, legitimate sick days, medical leave of absence and vacation time).
There is no formal time limit – productive participants may remain indefinitely. Nevertheless, mainstream work (with or without job coaching) is encouraged and facilitated, ongoing individualized support is available and there is an open return policy.
The Nassau Day Training Program was founded as a micrographics and document processing training program located in a light industrial/residential area in suburban Long Island, New York. Microfilming was selected as the initial business and training activity as there were numerous local employers and a robust market for client work opportunities among the many service industries in the region. In spite of the advent of digital imaging, now added among the program's range of training and work opportunities, microfilm continues to be the preferred document storage and retrieval system for legal records. Hence training, paid in-house contractual work and supported employment in the microfilm industry remain important elements of the program. A range of types and levels of work opportunities, some unrelated to micro-filming, are also maintained to accommodate the population's mix of ability levels. The program has a non-selective admission policy (mandated owing to its funding source), so that any patient having a psychiatric diagnosis and resultant disability, who desires services and is able to abide by some basic operational rules, must be admitted to the program without discrimination.
The training program of NDTP offers a flexible learning hierarchy, and performance up to industry standards is required to complete training. Participants can move through and among each of the program's phases as needed, remaining in each as long as indicated by their skills, clinical status and wishes. Phases include assessment, pre-vocational training, work adjustment training, specific skill learning, sheltered on-site employment, industry wage employment (on-site or in a work enclave in the community) and competitive work with or without job coaching. The program's leadership maintains industry contacts in the region with both current and potential clients and employers. Participants who achieve competitive employment standards and do not immediately find or want mainstream job placements are paid at least the legal minimum wage for contract work undertaken by NDTP. These participants are formally hired by the program, wear employee photo identification badges, receive a biweekly paycheck along with the program's professional and clinical staff and are eligible for promotion to supervisory positions within microfilming or office work. Participants meeting minimal standards may be engaged in sheltered on-site employment at a subminimum wage that is based upon productivity.
Below we explore the cost–benefit of this program, based on a retrospective naturalistic time series study conducted in 1994, focusing on the subset of participants having schizophrenia. Our interest in re-examining this previously unpublished work arose from the emergence of relatively disappointing supported employment outcomes for our most cognitively impaired schizophrenia program participants, which suggest to us alternative vocational program models that may be more suitable for at least a subset of these patients.
For the present study, we hypothesized that participation in NDTP for at least 1 year would be associated with an increase, relative to prior periods, in rate of work and earned income and a decrease in use of high-cost services including hospitalization and day treatment.
Method
Participants with a referral diagnosis of schizophrenia or schizoaffective disorder (SZ/SA) and admitted to the program between 1 January 1988 and 1 July 1993 (n = 197) comprised the study cohort. Diagnoses of SZ/SA stably represent approximately 30% of admissions and 40–50% of enrollees (reflecting the longer length of enrolment relative to non-SZ/SA participants). This study was approved by the Long Island Jewish Medical Center Human Subjects Review Board. To assure adequate program exposure for examining efficacy, only cases enrolled in the program for a minimum of 12 months (not necessarily uninterrupted) were included in the interview portions of the study. Cases thus eligible for inclusion (n = 76) and those not eligible (n = 121) were then compared on demographic variables, duration of illness and most recent hospitalization which were obtained from charts. All data were de-identified upon entry into the computer database.
Further data were collected only among eligible participants who provided written informed consent, using three methods: (i) questionnaire (completed by the patient and/or family and/or case workers); (ii) patient interview (a 2–4 hour interview conducted by a skilled clinical interviewer utilizing time-line follow-back methods linked to signifi-cant life events, hospitalizations, jobs, etc. [Robert E. Drake, personal communication, 1994] and [14]); and (iii) chart review (NDTP records for all cases, and for that subset who received services at Hillside Hospital, clinic records, hospitalization records and continuing day treatment records). Inconsistencies among sources were resolved by further questioning of the patient and/or clinicians where possible. Cases with significant unresolved inconsistencies between sources or inadequate reliable data to reconstruct the observation period were excluded from analysis.
Detailed information was ascertained on vocational activity, mental health service use (inpatient and outpatient) and independent living for the period beginning 2 years prior to admission to NDTP to the selected endpoint date of the 1 September 1994. With the exception of earned income (see below), these results were examined across six 1-year timeframes described, along with available number of cases for each variable type in Table 1. The ascertainment method assured that all patients are included for ‘program timeframes’ one, two and three (admission year and the 2 years prior to admission). Successively, fewer cases were available for subsequent periods. A program timeframe was treated as valid for analysis in a given case only if a full year of data were available.
Number (and percentage) of cases actively enrolled at each program timeframe, and number of cases available in each year studied for employment, hospitalization and combined services
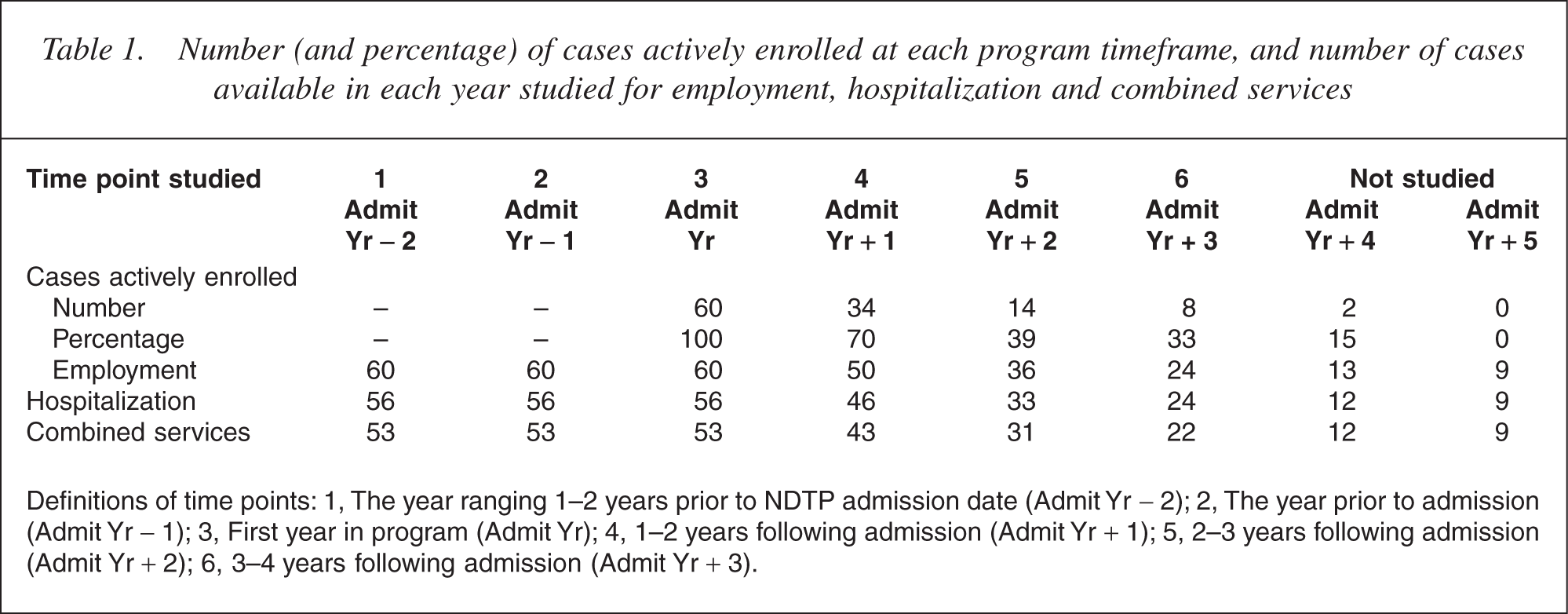
Definitions of time points: 1, The year ranging 1–2 years prior to NDTP admission date (Admit Yr −2); 2, The year prior to admission (Admit Yr −1); 3, First year in program (Admit Yr); 4, 1–2 years following admission (Admit Yr + 1); 5, 2–3 years following admission (Admit Yr + 2); 6, 3–4 years following admission (Admit Yr +3).
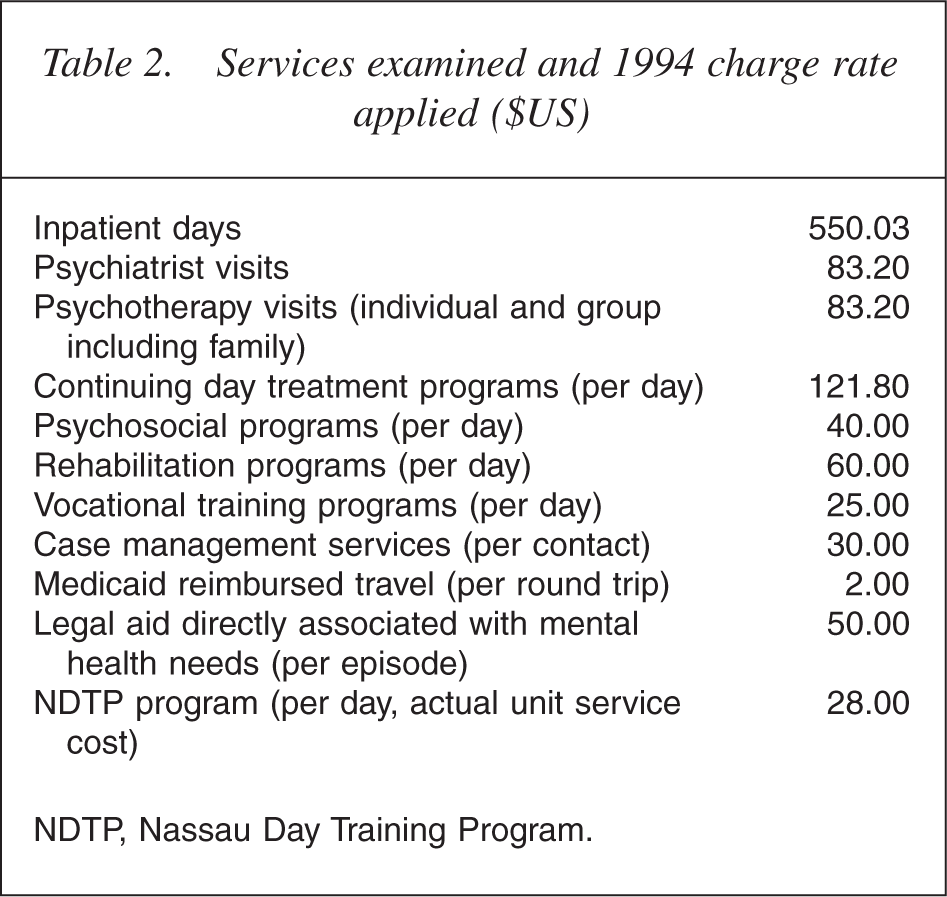
Service use data were aggregated into total number of units of each service type within each 1-year program timeframe (1 through 6). As it was not always possible to obtain precise records for each ambulatory visit retrospectively, we used scheduled visits rather than actual visits. This method results in a universal overestimation of the actual services provided which inflates estimates of charges so that total cost estimates can only be used for comparison from one timeframe to another, and not as indicators of actual cost. For this reason we refer to estimated costs as ‘relative cost units’ throughout the remainder of this report. Data on vocational training programs (including NDTP) and supported education were treated as mental health services for purposes of this analysis. After quantifying number of units of each service type within each timeframe, each service unit was multiplied by its then current 1994 Medicaid payment rate or reasonable estimate of rate for non-Medicaid services (see Table 2 for services included and rates applied).
Services examined and 1994 charge rate applied ($US)
To correct for the possibility that observed changes in hospital use reflected secular trends and not program impact, length of stay trends were also examined for a comparison group of patients discharged from Hillside's inpatient service for each calendar year studied.
We studied vocational functioning as annual number of months of salaried work (part-time or full-time, mainstream or non-mainstream), and earned income. Salaries from all years were corrected to 1994 levels, the study endpoint year, using the Consumer Price Index (US Department of Labor, Bureau of Labor Statistics; http://www.bls.gov/cpi/home.htm). Note that we wished to capture the impact of the illness itself, as well as NDTP, on work history. Thus, in the case of earned income, rather than reporting on program timeframes, data were aggregated (annualized) to the following five lifetime timeframes:
Age 18 to illness onset (18 to onset) Illness onset to 1 year prior to admission (Onset to admit Yr −1) Year prior to admission (Admit Yr −1) Admission year (Admit Yr) One year following admission to program discharge (Admit Yr + 1 to dc).
Statistical analyses examining program-related effects over time employed mixed models repeated measures analysis of variance with annualized vocational, service or cost data as dependent variables and time as the repeated factor. Post-hoc analyses examined t-values for differences of least squares means.
Results
Comparisons of patients excluded versus included based upon 12-month minimal stay criterion
A total of 76 program participants met all inclusion criteria, of whom 40 were no longer enrolled and 36 were still enrolled at the time of this study. Comparing these 76 cases with those cases who were excluded from study because of less than 12-month program enrolment (n = 121), yielded no significant differences in age, education, gender, age at onset of psychiatric illness or age at first psychiatric hospitalization. However, the excluded group had significantly longer (F = 5.04, p = 0.03) and more recent (F = 10.35, p = 0.00) hospitalization prior to admission to NDTP than those patients who did stay in the program at least 12 months (Table 3).
Demographic and chronicity variables comparing patients enrolled for less than or equal to 12 months (n = 121) versus those enrolled for greater than 12 months (n = 76). Units are mean (SD)
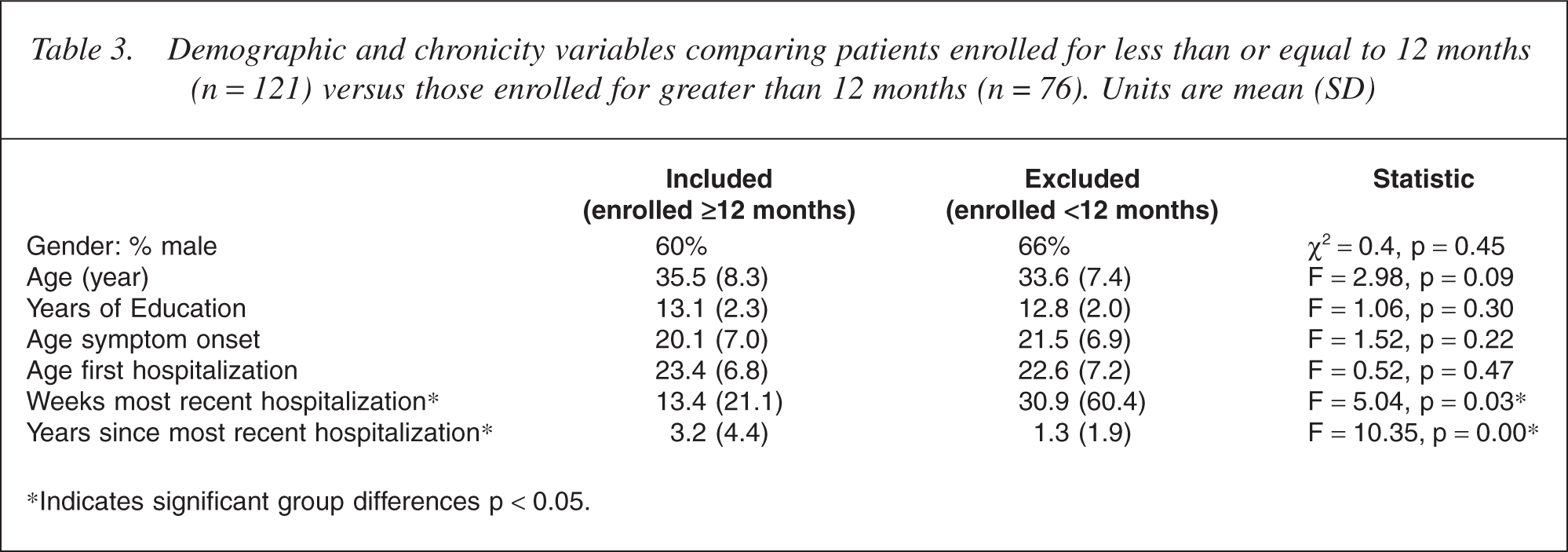
∗Indicates significant group differences p <0.05.
The profile of reasons for leaving NDTP also differed between those having short tenure and those who remained for at least a year, as shown in Table 4. Chi-square comparing the included versus the excluded groups on all reasons for discharge showed a non-significant trend (χ2 [df = 6] = 11.98, p < 0.10). When reasons for leaving the program were grouped according to the type (negative, neutral, or positive reason), the included and excluded groups differed significantly (χ2 [df = 2] = 10.02, p < 0.01) with the excluded group having a higher frequency of adverse reasons and the included group having more positive reasons for leaving.
Reasons for discharge from NDTP by group
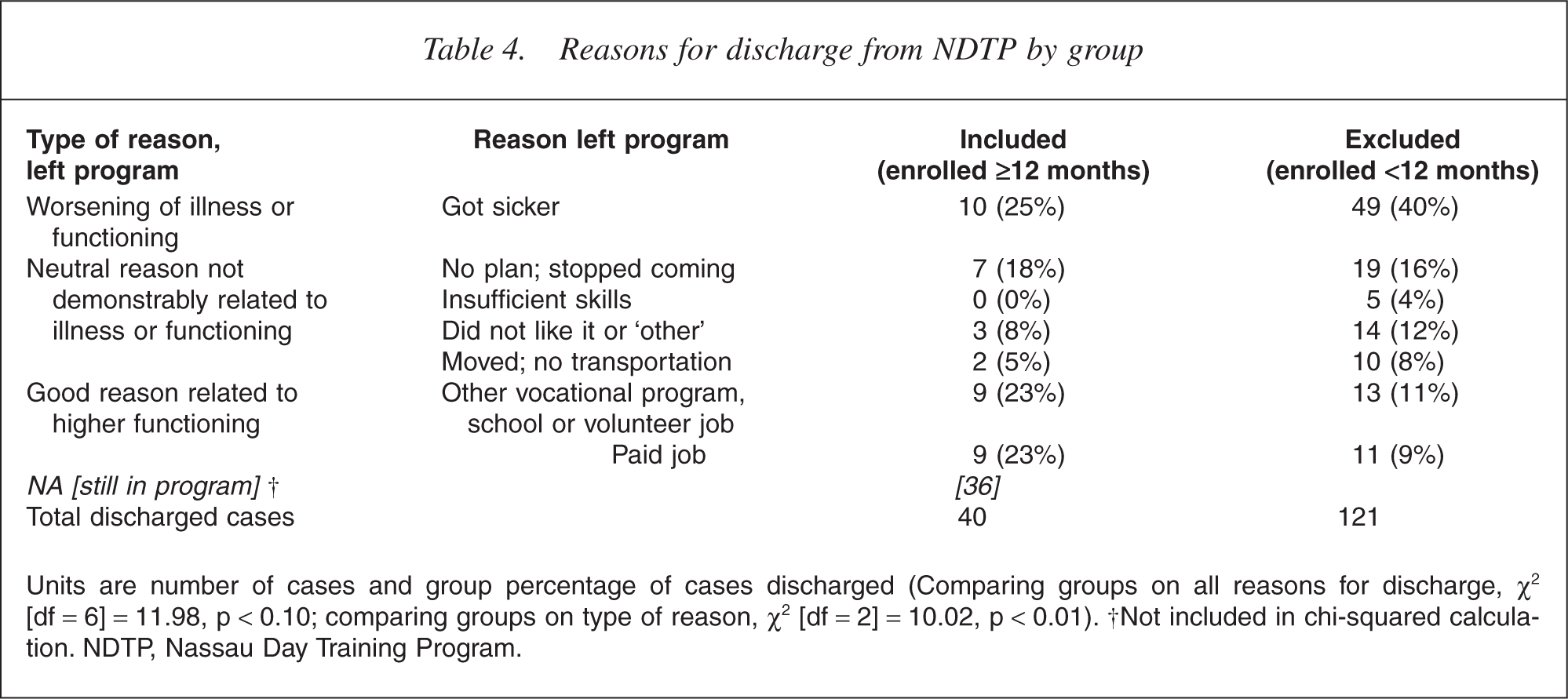
Units are number of cases and group percentage of cases discharged (Comparing groups on all reasons for discharge, χ2[df = 6] = 11.98, p < 0.10; comparing groups on type of reason, χ2 [df = 2] = 10.02, p < 0.01). †Not included in chi-squared calculation. NDTP, Nassau Day Training Program.
Program effectiveness
Sample
Of the 76 cases that met inclusion criteria for the study, 62 were interviewed. Employment data were available for 60 cases, hospitalization data were available for 56 cases, and total relative cost unit estimates for mental health services could be calculated for 54 cases. Of the 16 cases not in the sample, only five refused participation. Four could not be located or were known to have left the region, five were too symptomatic to be interviewed or insufficient chart data were available, and two were interviewed successfully but were dropped because irreconcilable discrepancies were found between sources of data. No subject fees were paid; however, transportation expenses were covered and participants received a free meal (usually pizza) on the day of their interview. Comparisons of missing cases with non-missing cases yielded no significant differences on age (F = 0.1, p = 0.75), age at first hospitalization (F = 0.00, p = 0.95), education (F = 0.38, p = 0.54), duration of most recent pre-enrolment hospitalization (F = 0.05, p = 0.82), time since most recent hospitalization (F = 0.17, p = 0.68), time spent at NDTP (F = 0.96, p = 0.33) and absentee rate at NDTP (F = 1.01, p = 0.32).
Table 1 summarizes the number of available cases within each timeframe and the number of patients (among the cohort of 60 for whom employment data were available) who were still enrolled in the program at each post-admission timeframe. Decrements across time represent the passing of time from date of consecutive admission and not attrition or missing data. Measures of central tendency are only reported through admission year plus 3, where there are at least 22 ases in the smallest cell.
Vocational functioning
Vocational variables included average months per year employed in mainstream and non-mainstream employment within each 1-year timeframe beginning 2 years prior to NDTP enrolment, and mean earned annual income from age 18 until present. Not surprisingly, premorbid employment levels were modest: even those patients who became psychiatrically ill after age 18 were only employed for an average of 4.96 months per year (SD = 4.0) during the years prior to their first hospitalization. As illustrated in Fig. 1, most patients did not work during their first year in the program (1.1 months, SD = 2.8), but the period thereafter showed a statistically significant increase in annual months worked to 5.97 (SD = 4.80), an increase which was sustained among the 36 and 24 patients, respectively, included for the subsequent 2 years. Mixed models repeated measures analysis of variance revealed a significant main effect for time (F = 17.74, p < 0.0001). Post-hoc analyses (differences of least squares means) revealed that number of months employed during each of the 3 years after program enrolment was significantly higher than the year of enrolment (‘Admit Yr’): tvalues ranged from −5.8 to −8.2 (all p < 0.0001), and the three followup years were not different from one another. Admission year was not significantly different from the year prior to enrolment, but was significantly lower than Admit Yr −2 (t = 2.61, p = 0.009). Notably, annual months worked for each of the 3 years subsequent to program enrolment year were significantly higher than during each of the three prior years.
Annualized number of months paid employment, either part-time or full-time, in mainstream and non-mainstream environments.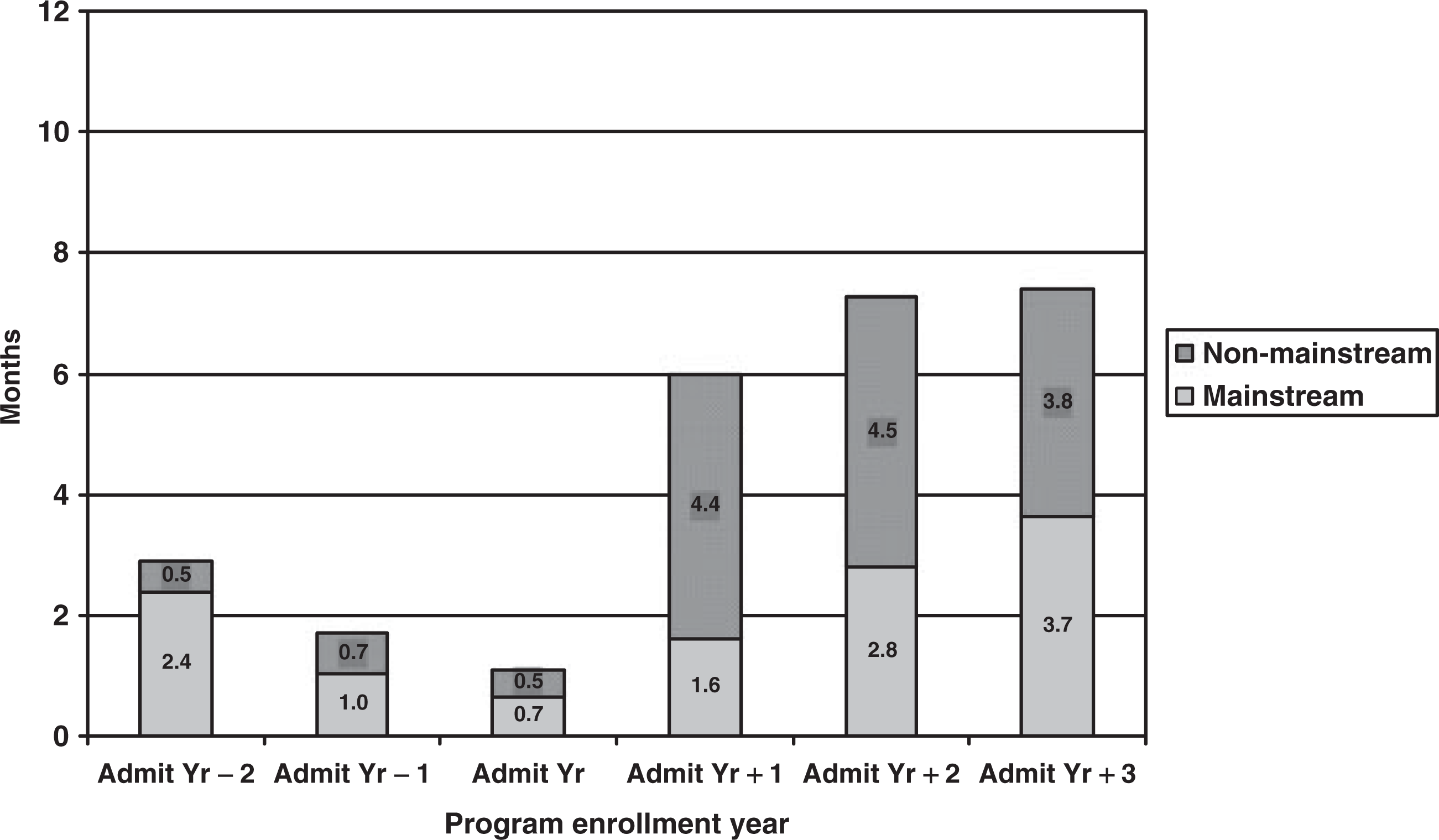
Contributing substantially to the marked second year increase in time spent working are the transitional and work enclave employment opportunities for patients who achieve adequate skills (indicated as non-mainstream work in Fig. 1). As many of these work opportunities are at or below minimum wage and most are part-time, this increase in months gainfully employed did not translate into increases in earned income (Fig. 2).
Annualized mean earned income across time (in 1994 $US). Note that annual median income for production workers in the US in 1994 is estimated as $19 536 (US Bureau of Labor Statistics, http://www.bls.gov).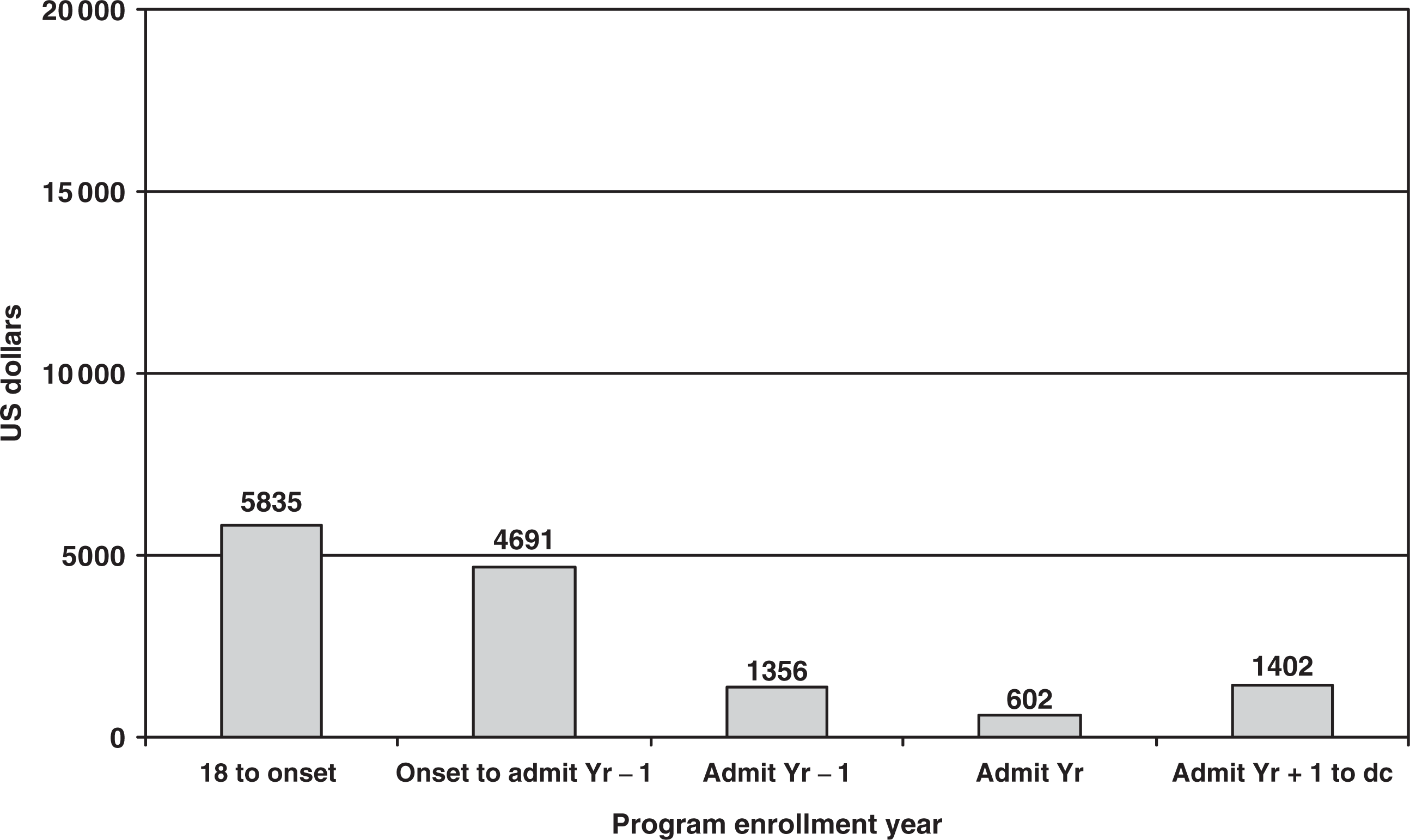
Mixed models repeated measures analysis of variance examining annualized mean income across time showed a significant main effect for time (F = 11.81, p < 0.0001). Post-hoc analyses revealed that earned income was significantly higher during the earliest two time periods studied (18 to onset: mean = $5835, range = $0–27 157; Onset to admit Yr −1: mean = $4690, range = $0–32 712) relative to the year prior to admission and subsequent years (Admit Yr −1: mean = $1357, range = $0–25 331; Admit Yr: mean = $602, range = $0–23 430; Admit Yr + 1 to dc: mean = $1409, range = $0–10 743). These t-values ranged from 3.66 to 5.75 with p-values ranging from 0.0002 to 0.0003. Earned income did not drop precipitously following illness onset as might have been expected, but did deteriorate over the illness course as it was significantly lower during Admit Yr −1 than during each of the two previous time periods studied. Earning capacity was essentially unchanged following program enrolment.
Service use and relative cost units
The most dramatic impact of NDTP enrolment was seen on clinical service and relative cost unit variables. Number of inpatient days (annualized) fell precipitously from the year prior to enrolment to the first year in the program. This rate remained lower in subsequent periods (Fig. 3). Mixed models repeated measures analysis of variance across six time periods (the 2 years before the admission year, the admission year and the following three years) revealed a significant main effect for time (F = 3.46, p = 0.005). Post-hoc analysis showed higher number of inpatient days during each of the 2 years prior to program enrolment (Admit Yr −2: mean = 33.7 [SD = 66.9; range = 0–289]; Admit Yr −1: mean = 28.3 [SD = 64.5; range = 0–316]) relative to admission year and the year that followed (Admit Yr: mean = 2.5 [SD = 8.6; range = 0–46]; Admit Yr + 1: mean = 7.7 [SD = 26.6; range = 0–147]). Admit Yr −2 and Admit Yr −1 were also significantly different from Admit Yr + 2 (mean = 15.5 [SD = 53.0; range = 0–299]) and Admit Yr + 3 (mean = 6.8 [SD = 33.2; range = 0–163]) although these changes might be artifacts of diminishing n's and the disproportionate effects of outliers in later years. The t-values ranged from 2.19 to 3.49 with p-values ranging from 0.0006 to 0.02.
Annualized mean number of days in psychiatric inpatient facility over the study period.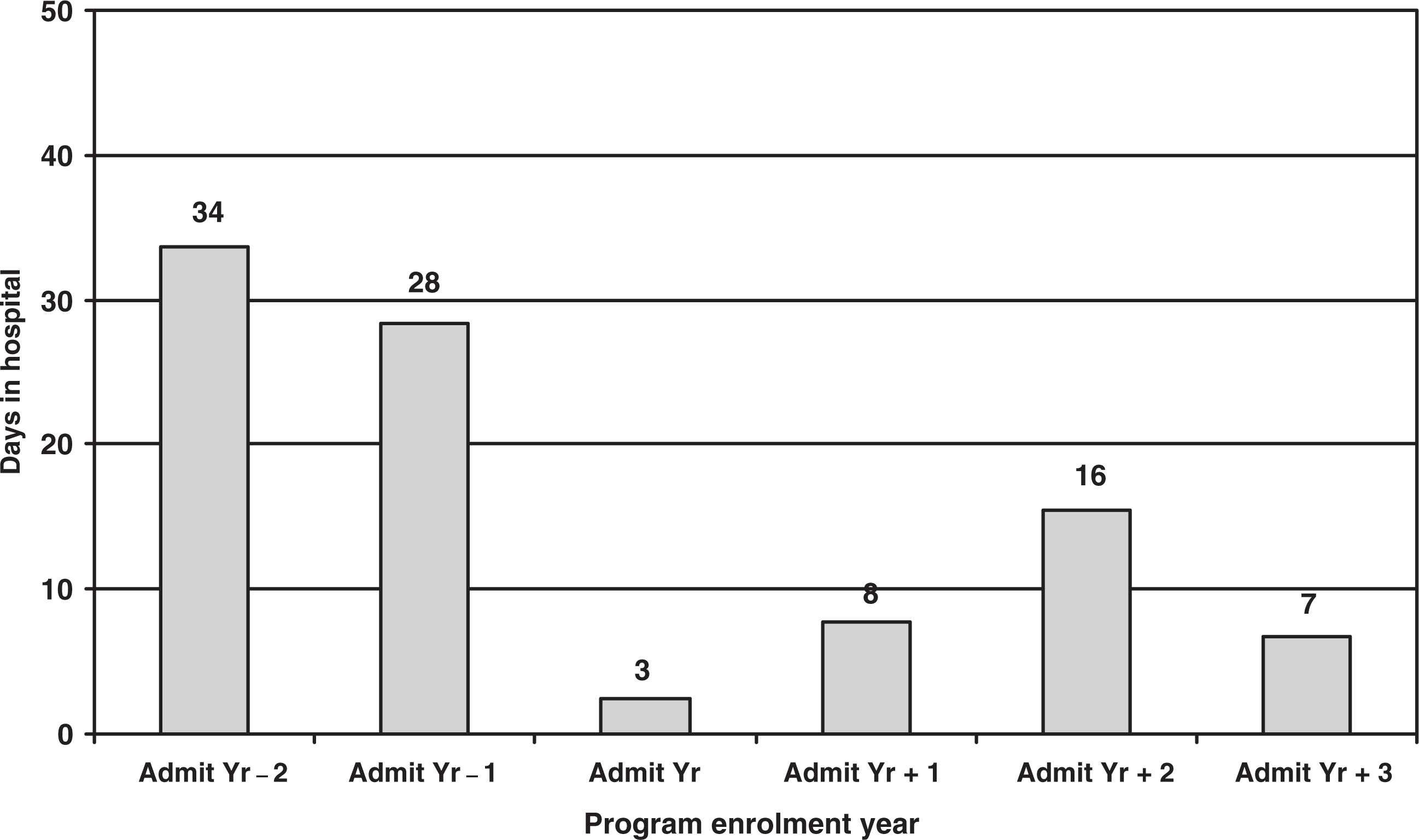
Among the many limitations of a naturalistic study such as this is the fact that secular trends in health-care utilization, rather than the impact of NDTP, could be responsible for the observed reduction in hospital days. Since our study took place over five calendar years, we could examine this in two ways. The first was to analyse the trend in hospital length of stay in clinically and demographically (diagnosis, age, gender and race) matched subgroups of Hillside Hospital inpatient admissions for each of the 5 years covered (30 cases for each year, total n = 150). Mixed models repeated measures analysis of variance revealed no significant trend towards shorter length of stay during the years captured in this study (F = 1.63, p = 0.12; means = 38.4–60.0 days). (This trend is illustrated on the top line in Fig. 4). The second method was to plot annual hospital days by calendar year for those cases in the NDTP sample as a function of enrolment year. This allowed us to examine the possibility that a temporal trend (independent of NDTP enrolment) might have occurred in the NDTP sample. For this purpose, three periods were compared: the 2 years prior to enrolment, the 2 years after enrolment (combining Admit Yr and Admit Yr + 1) and the next 2 years (combining Admit Yr + 2 and Admit Yr + 3). Unfortunately, even when data were combined in this way, there were still insufficient cases in individual enrolment years by calendar year to permit statistical testing of time and enrolment group effects (a mixed models factorial analysis would be required). Descriptively, results (plotted in Fig. 4) confirm that average annual hospital days were consistently lower in each calendar year for years following enrolment compared with pre-NDTP enrolment. The apparent increase in 1993 relative to 1992 in hospital days for the first 2 years postenrolment group is modest in real terms (7.4–15.4 days per year) and probably reflects statistical instability from inadequate cases in each cell. Interestingly, the apparent increase between 1991 and 1992 in number of hospital days prior to NDTP admission maps on to a similar trend (albeit non-significant in both cases) in length of stay among Hillside Hospital admissions for those 2 years. However, note that the units of measure on the Hillside length of stay line is different than the other measures on the figure (reflecting annual days in hospital in the NDTP study cohort, where some were not hospitalized at all and some may have had multiple hospitalization episodes), so no direct comparison can be made.
Mean annual inpatient days by calendar year for each enrolment year during study period. (LOS, length of stay; NDTP, Nassau Day Training Program.)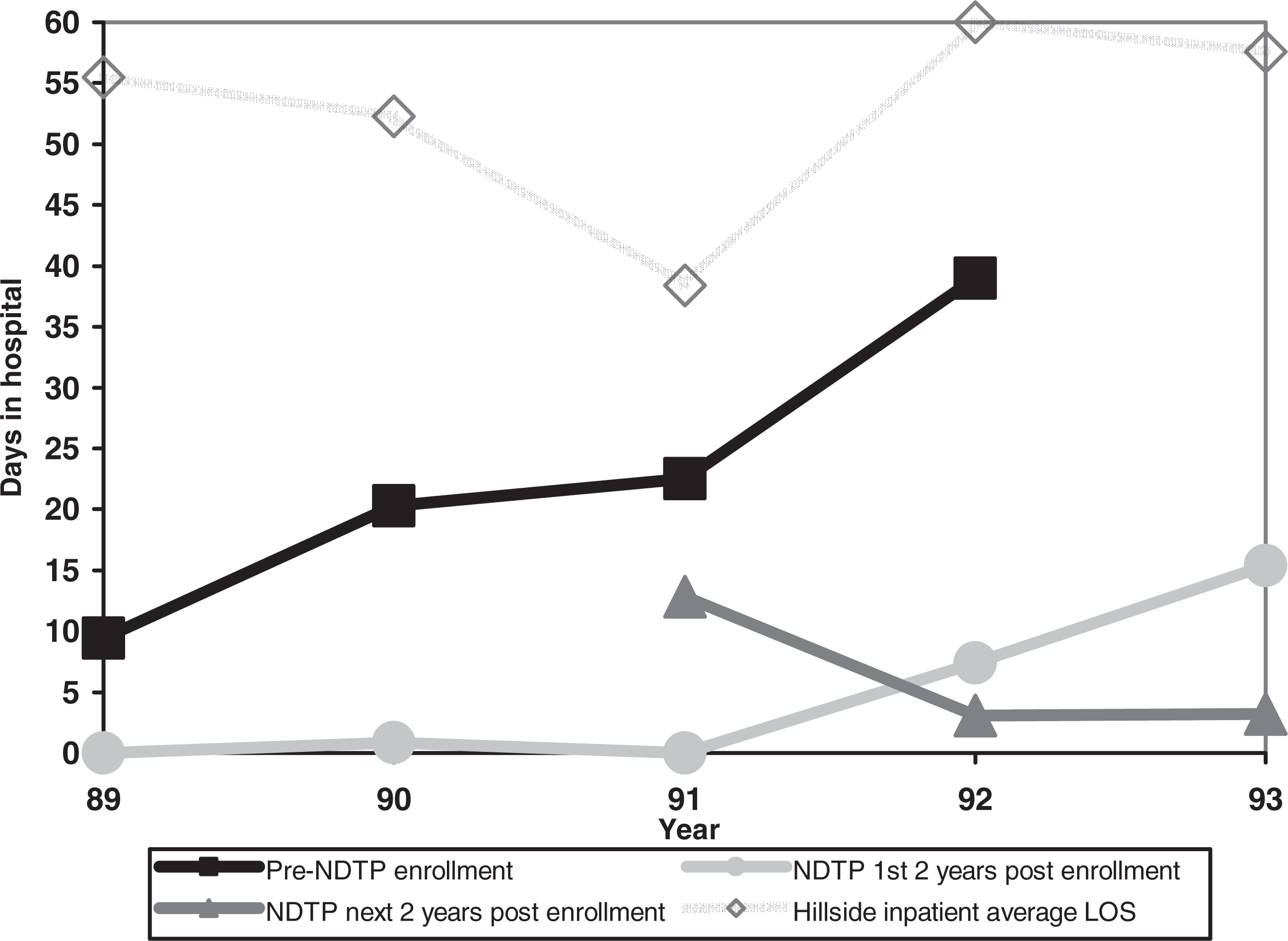
Consistent with the significant decrease in inpatient hospital days following NDTP enrolment, annual charges for combined mental health services fell from means of $30 144 (SD = 36 317) and $29 715 (SD = 34 962) during the first two pre-admission years to $6968 (SD = 6057), $9128 (SD = 9970), $16 401 (SD = 29 977) and $13 415 (SD = 22 011) for subsequent years. Mixed models repeated measures analysis of variance confirms the significance of this trend (main effect for time: F = 7.35, p < 0.0001). Post-hoc analyses reveal significant differences between the 2 years prior to program enrolment and each subsequent year, with t-values ranging from 2.23 to 5.23 and p-values ranging from < 0.0001 to 0.03. Because of skewness and large standard deviations, median values for these timeframes were also examined and are displayed in Fig. 5 with virtually identical trends. This cost reduction is attributable not only to the decrease in inpatient days, but also to the dramatic reduction in more expensive services such as continuing day treatment program visits.
Median annual charge estimates for all services combined across time ($US)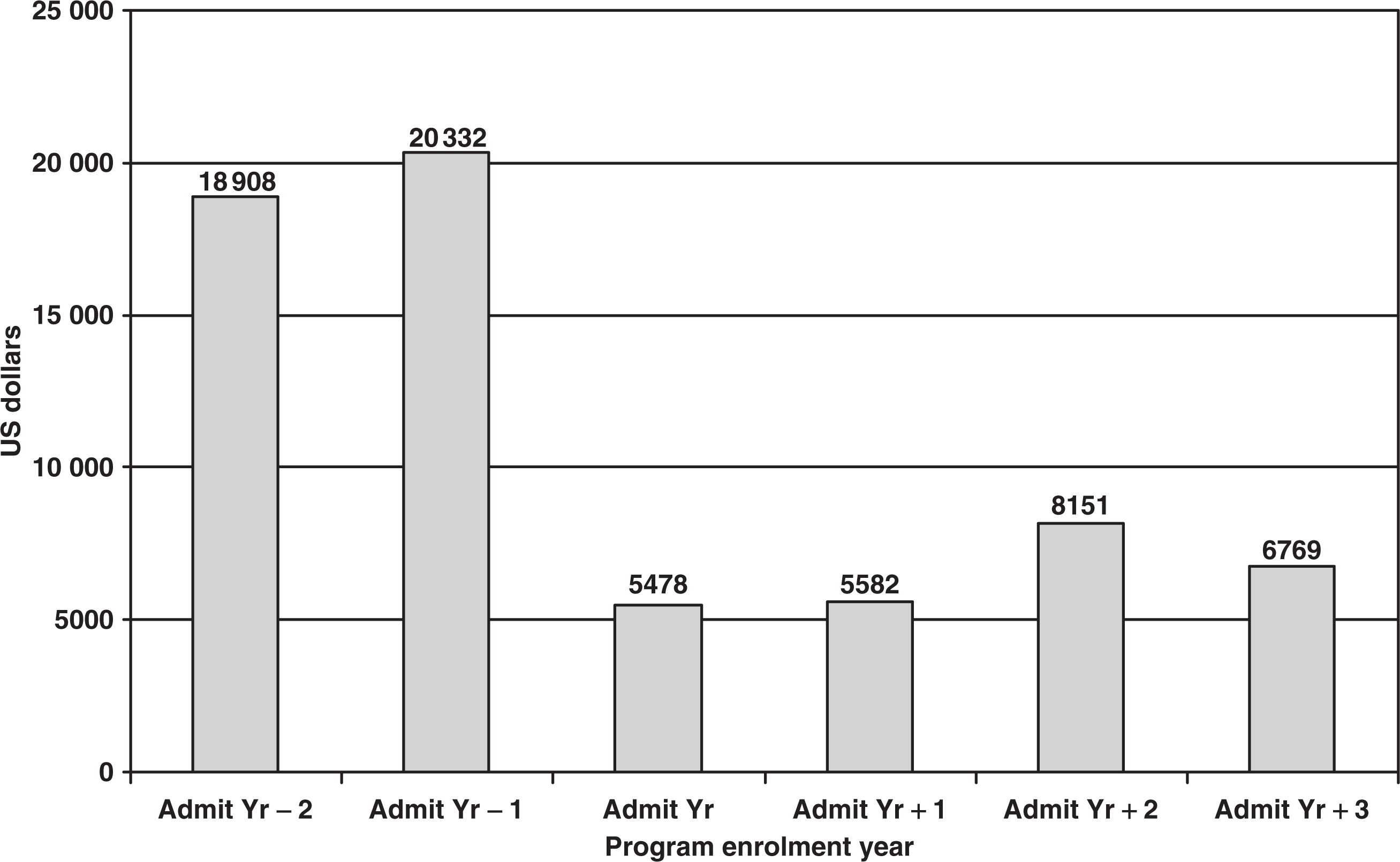
Discussion
These findings indicate that participation in NDTP is temporally associated with an abrupt and statistically significant decrease in relative mental health cost units of more than 70% in 1 year. This is largely attributable to a decrease in hospitalization rate, although an important contributor is the decrease in use of more expensive day treatment programs. Annual months of gainful employment also increased significantly after NDTP enrolment although earned income did not.
This study has several limitations that significantly limit drawing causal conclusions. The study was retrospective; there was no comparison group and random assignment was precluded by the funding source which requires an open door policy for all psychiatrically disabled individuals wishing to participate. Under these conditions, false positive conclusions about program impact can result at several points. First, selection bias towards patients having an interest in return to work may also select individuals for whom change over time was more likely even without program participation. This bias can occur at enrolment, and at discharge for those not meeting the 1-year minimal exposure period for inclusion in our analyses. Second, trends in time series data may reflect secular trends and not the effect of an intervention.
With regard to the first, while program enrollees all shared the diagnosis of SZ/SA and had been ill for nearly 20 years, suffering the typical chronic course, those failing to remain for at least a year had been suffering a more severe recent illness course. They had been hospitalized more recently, had a longer stay in their most recent hospitalization than those who remained at least 1 year, and reasons for leaving the program during the first year suggested that as a group they were less stable at the time of enrolment. As lifetime hospitalization rates were not available for the excluded sample, the possibility that a more severe lifetime course is also present could not be examined. However, we note that in spite of greater illness stability at the time of admission among those included, the included sample were nevertheless a severely and persistently ill group: they had been hospitalized an average of 49 days per year from first onset of illness until 1 year prior to NDTP admission. Even while in the program, 20 of the 76 cases included had interruptions in attendance attributable to hospitalizations or disabling degrees of symptom exacerbation and among these patients there were a total of 37 such interruptions. As noted in the Results section, age at illness onset and at first hospitalization was not different between groups.
Although the program is open at no charge to psychiatrically disabled individuals wishing to participate (independent of clinical status), the NDTP sample is selective in the sense that participants and referring agents choose this program over other day treatment, vocational and psychosocial club opportunities, all of which are available nearby. While our sample is demographically similar to patients attending day treatment programs, there may be other factors (correlated with motivation and interest) that discriminate this sample from the broader outpatient schizophrenia population.
With regard to the second opportunity to draw false positive conclusions about program impact (the possibility that change over time reflects secular trends and not the effect of an intervention), we were able to partially address this point with respect to annual number of hospital days. Hillside Hospital was not undergoing decreases in length of hospital stay for SZ/SA during the years under study. Also, within each calendar year studied, NDTP enrollees had consistently fewer hospital days than later enrollees who had not yet enrolled in that year.
In general, the best predictor of illness (symptom, treatment and functional) course in schizophrenia is the patient's history. While association does not imply causation, NDTP enrolment was associated with abrupt and sustained improvements on several important indicators. In addition to statistically significant reductions in annual hospital days and relative service cost units, NDTP enrolment was followed by a significant increase in time spent in paid work (albeit mostly non-mainstream work) from about 1 month to over 7 months per year for those patients who remained for at least 1 year. The lack of impact of NDTP on earned income was disappointing but understandable in view of the large number of patients sustaining only part-time or below minimum wage ‘transitional’ employment. (For some patients, this may reflect self-imposed work restrictions to avoid the risk of loosing eligibility for public benefits including Medicaid).
To the degree that NDTP may be an ‘active agent’ in improving clinical course, we hypothesize several potential ‘mechanisms of action’: productive activity that has visible societal value provides structured use of time with an emphasis on the patient's own goals, resulting in a sense of purposefulness that reduces the cognitive ambiguity of ‘make work’ environments. Reduction in cognitive ambiguity may reduce decompensation risk. Simultaneously, to the degree that participants are also committed to their work, program adherence is enhanced. Further, early detection of prodromal signs of decompensation and earlier preventative intervention may be facilitated in such an environment where even very subtle changes in mental status quickly become apparent to the patient and coworkers as they are engaged in mission-critical work. These features may directly affect hospitalization rates [15]. Finally, it is possible that cognitively challenging work has a remediative effect on cognition itself, perhaps serving double duty as a kind of ‘cognitive remediation’. Hence, while neurocognitive deficits may limit work outcomes, it is also possible that under certain circumstances, work may itself be remediative. The value of work for the clinical state in dementia praecox was recognized by Emil Kraepelin nearly a century ago when he indicated that ‘occupation alone can preserve by exercise the capabilities which still remain to [patients with dementia praecox]’ [16], p. 281].
A randomized trial comparing an NDTP-like model with supported employment alone would help us determine in a sample of patients wanting gainful employment, whether, how much and for whom there is enhanced benefit of such alternative community-based vocational opportunities. It may be that for schizophrenia patients having marked cognitive deficits, for example, in ‘executive’ functions such as cognitive flexibility and in speed of attentional processing, that alternatives to both the sheltered workshops of the past and the fully mainstreamsupported employment programs replacing them, are needed. Suggesting the importance of alternatives to supported employment is the fact that, even though new NDTP participants may enrol in the program's active supported employment and job development program from the outset, the proportion of patients in this diagnostic group who do so is very small. Even only a modest proportion do so after undergoing training. It is our impression that this is most likely because cognitive and skill limitations restrict these more demanding opportunities. Extended transitional community-based work opportunities (including work enclaves) in high-skill technical areas such as microfilming, represent dignified alternatives to workshops and may, for some patients, also offer a higher probability for long-term success than may be possible with supported employment. Our early observations further suggest that such an approach may be cost-effective. Future studies should aim to estimate the true economic impact of community-based vocational rehabilitation programs, using more refined techniques for evaluation of economic impact [17, 18].
Footnotes
Acknowledgements
Thanks to the patients who participate in this study and the following individuals for their assistance with data collection and data management and analysis: Michael Borenstein, Barbara Napolitano, Nancy Conniff, Suzy Gell, Kenneth Klassert and Eileen Dunne. Helpful criticisms on an earlier version of this manuscript were provided by Carole Siegel, Dave O'Neill, Marvin Herz and Jennifer Beecham. This study was supported in part by NIMH grants MH41960, P30MH60575, John Kane, Principal Investigator and R01MH55585, Judith Jaeger, Principal Investigator.