
Abstract
Keywords
The use of psychotropic medication in children and adolescents has increased substantially over recent decades, with a number of studies reporting a two–threefold increase in use [1, 2]. In 2004 it was reported that spending on psychotropic medications for children and adolescents overtook both antibiotic and asthma categories [3]. Although medications used to treat attention-deficit–hyperactivity disorder (ADHD) were reported to exhibit the greatest increases in use, there have also been demonstrated increases in utilization of other key drug groups, especially atypical antipsychotics [4] and antidepressants such as the selective serotonin re-uptake inhibitors (SSRIs) [5, 6]. Substantial increases in use of psychotropic medications for children and adolescents have also been reported in psychiatric inpatient units [7].
One area that has been little examined within this context is the use of pro re nata (PRN, or ‘as needed’) sedation. PRN sedation allows nurses to provide medications in a timely manner, to treat acute distress or behavioural problems [8, 9]. In child psychiatric units PRN sedation is a commonly used intervention, with drug utilization studies reporting that up to 80% of young people receive PRN sedation during psychiatric admission [8, 10, 11]. Despite the widespread use, little evidence supports use of PRN sedation, especially in young people. Procedures for good clinical practice are not always used for PRN sedation, with many studies reporting that indications for use are poorly recorded in clinical records [9, 11, 12], potentially allowing nursing staff to administer medication for a purpose not intended by the prescribing physician [13]. Additionally, it has been suggested that PRN medications are overused and may not be necessary [14].
Despite the importance of understanding changes in practice over time, few studies have examined changing trends in use of PRN sedation in young people. To address this issue, the present study (i) examined the use of PRN sedation in a child and adolescent psychiatric inpatient unit, (ii) assessed changes in patterns of utilization over time, and (iii) examined whether changes in use of PRN sedation were related to changes in patient demographics, diagnoses or use of routine psychotropic medications.
Methods
Study site
The study site was the inpatient facility of a child and youth mental health service based in Brisbane, Australia. The unit is a 10-bed, child and adolescent psychiatric, tertiary care, inpatient unit. The unit provided short to medium duration admissions including stabilization of crisis presentations, planned diagnostic assessments and brief intensive therapy. Care was provided by a multidisciplinary team of medical, nursing and allied health staff who specialize in child and adolescent mental health. Based on national and institutional ethics guidelines, this evaluation met criteria for, and was conducted as, a quality assurance activity.
Data extraction
An audit of PRN sedation utilization was conducted for two time periods: April 2002–September 2003, designated wave I; and October 2004–December 2005, designated as wave II. All admissions occurring during these time periods were identified, and medical charts were used to extract data on PRN sedation (drug prescribed and number of doses received) using a standardized data collection template. Other information collected from charts included demographics (age, gender, ethnicity, living with at least one parent), clinical characteristics (diagnoses, history of abuse, history of suicide attempt), admission duration, and use of routine medications. Initial data from wave I has been published elsewhere [11].
The original medication charts for writing PRN prescriptions within the unit did not include a specific area for designating the indication for PRN medications; instead, the prescriber could choose to add this information within the area for documenting drug type and dose. Partway through wave II a new medication chart was introduced, which incorporated a designated area for recording the indication of PRN medication. To assess whether this change in medication chart led to improved documentation of indications for PRN sedation within wave II, we also collected data on whether any indication was documented in the prescription and which medication chart (older or newer) was used.
Statistical analysis
Statistical analysis examined differences between the two waves, with regard to both utilization of PRN sedation, patient characteristics and use of routine medications. During the study period some patients were admitted on more than one occasion to the unit. Statistical comparisons between groups utilized only the first admission for each patient. Nonetheless, descriptive information about use of specific drugs for PRN sedation incorporated data from all patient admissions within each time period. Group comparisons were conducted using χ2 analysis for categorical variables (e.g. proportion of patients receiving PRN sedation, sex) and student's t-test for continuous variables (e.g. no. doses received, age). Diagnoses were grouped as internalizing disorders (mood disorders and anxiety disorders), externalizing disorders (ADHD, conduct disorder, and oppositional defiant disorder) and developmental disorders (mental retardation, pervasive developmental disorders and learning/communication disorders). Using logistic regression, independent predictors of PRN sedation use were identified, and strength of effect was quantified using odds ratios. For all analyses, alpha was set at 0.05. We note that as part of t-test analyses, the statistical programme (SPSS; SPSS, Chicago, IL, USA) examines variance in the scores for each group. When the variance is different between groups, SPSS amends this difference and provides an adjusted set of statistics, including degrees of freedom. For this reason, a number of t-tests reported in the results exhibit disparate values for the degrees of freedom.
Results
Patient characteristics
One hundred and twenty-one patients were reviewed within wave I, and 133 in wave II. In wave I the average patient age was 13.31 years (SD = 3.41, range = 2.1–19.5 years); in wave II the mean age was 13.69 years (SD = 2.91, range = 5.8–18.0 years). More than half were female in each wave (wave I, 56.2%; wave II, 60.9%). Seven patients were Aboriginal or Torres Straight Islander (three in wave I; four in wave II). Patient characteristics are described in Table 1. There was a reduction in the proportion of patients diagnosed with an internalizing disorder (χ2=4.79, p < 0.05). Between wave I and wave II there was a reduction in the proportion of patients receiving typical antipsychotics (χ2=4.20, p < 0.05), an increase in the proportion of patients receiving mood stabilizers (χ2=3.97, p < 0.05), and a trend suggesting a small increase in number of patients receiving stimulants (χ2=3.00, p = 0.08). No other group differences were observed with regard to age, sex, living situation, admission duration, diagnoses of externalizing or developmental disorders, history of abuse, history of suicide attempt, use of psychotropic medications (Table 1).
Patient characteristics
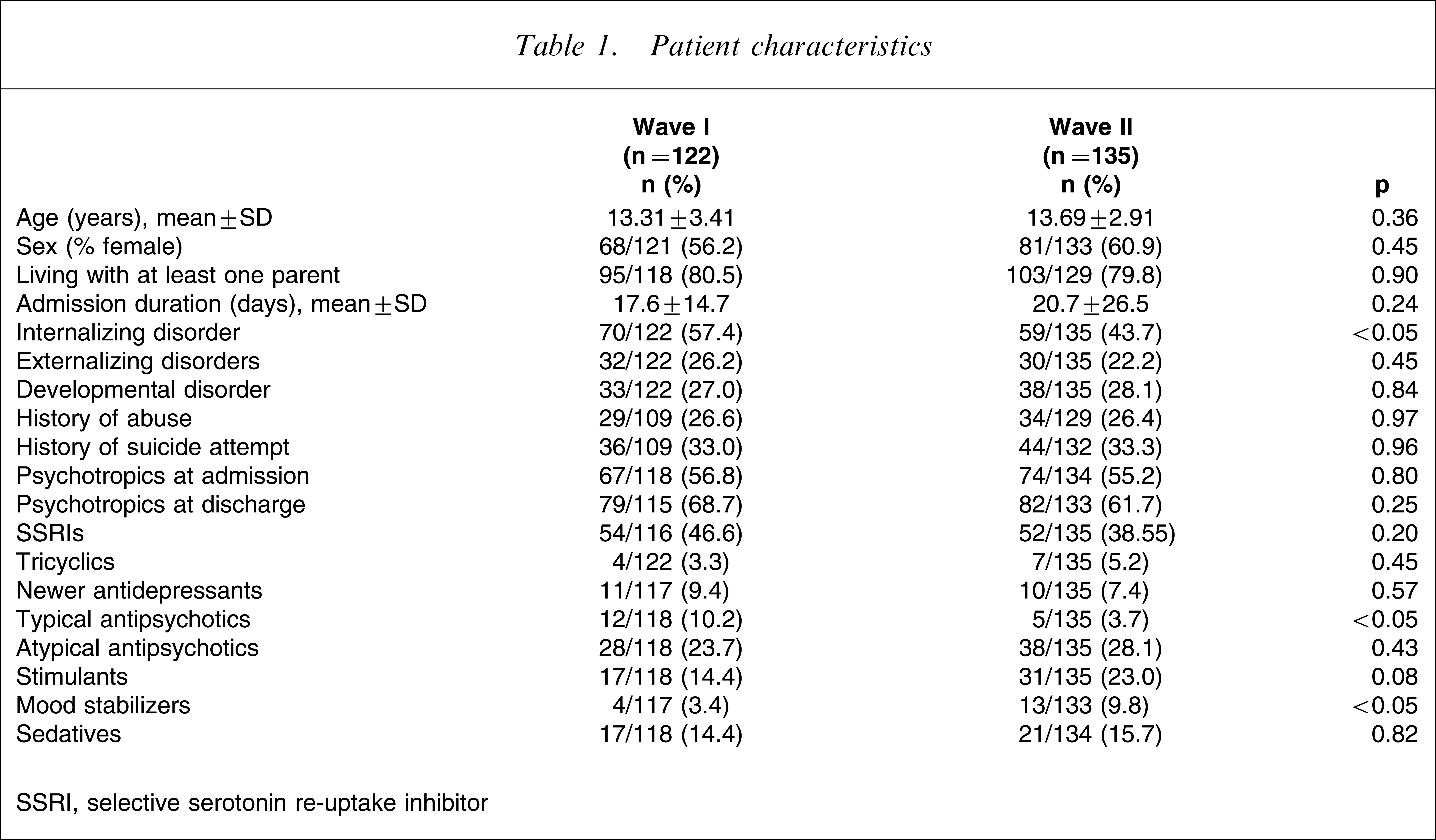
SSRI, selective serotonin re-uptake inhibitor
Utilization of PRN sedation
Over time, there was a significant reduction in the proportion of patients being prescribed PRN sedation (χ2=6.97, p < 0.01) and being given PRN sedation (χ2=11.01, p < 0.01; Table 2). For all patients, there was also a significant reduction in the mean number of PRN drugs prescribed per patient (t = 3.88233, p < 0.001), the number of doses administered per patient (t = 2.62173, p < 0.05) and the number of PRN drugs administered per patient (t = 3.10229, p < 0.01; Table 2). Within wave I the most frequently used drug was chlorpromazine (39.7% of doses, 155/390), followed by olanzapine (21.5%, 84/390). In contrast, the most popular drug used in wave II was diazepam (37.9% of doses, 64/169), followed by olanzapine (21.2%, 36/169; Table 3).
Changes in utilization of PRN medications
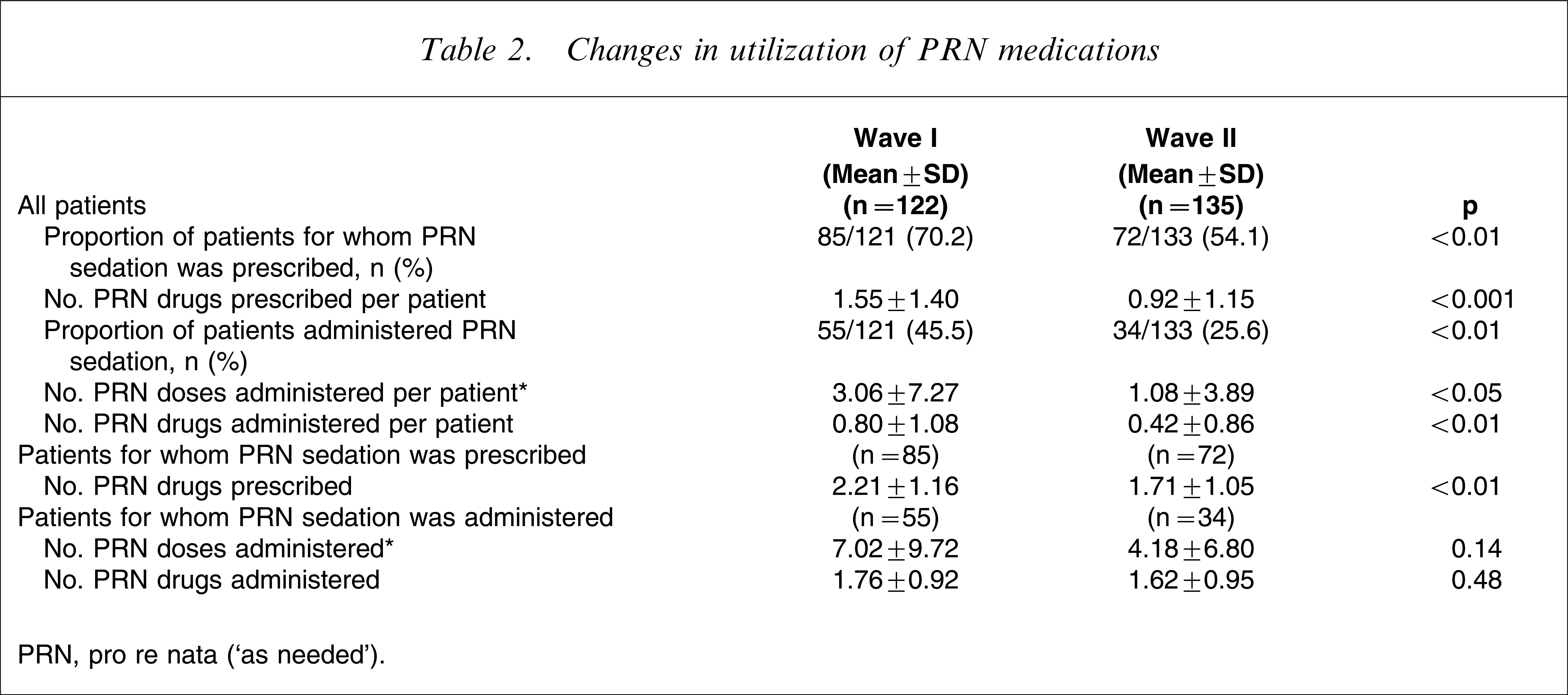
PRN, pro re nata (‘as needed’).
Contribution of specific drugs to total available number of PRN doses
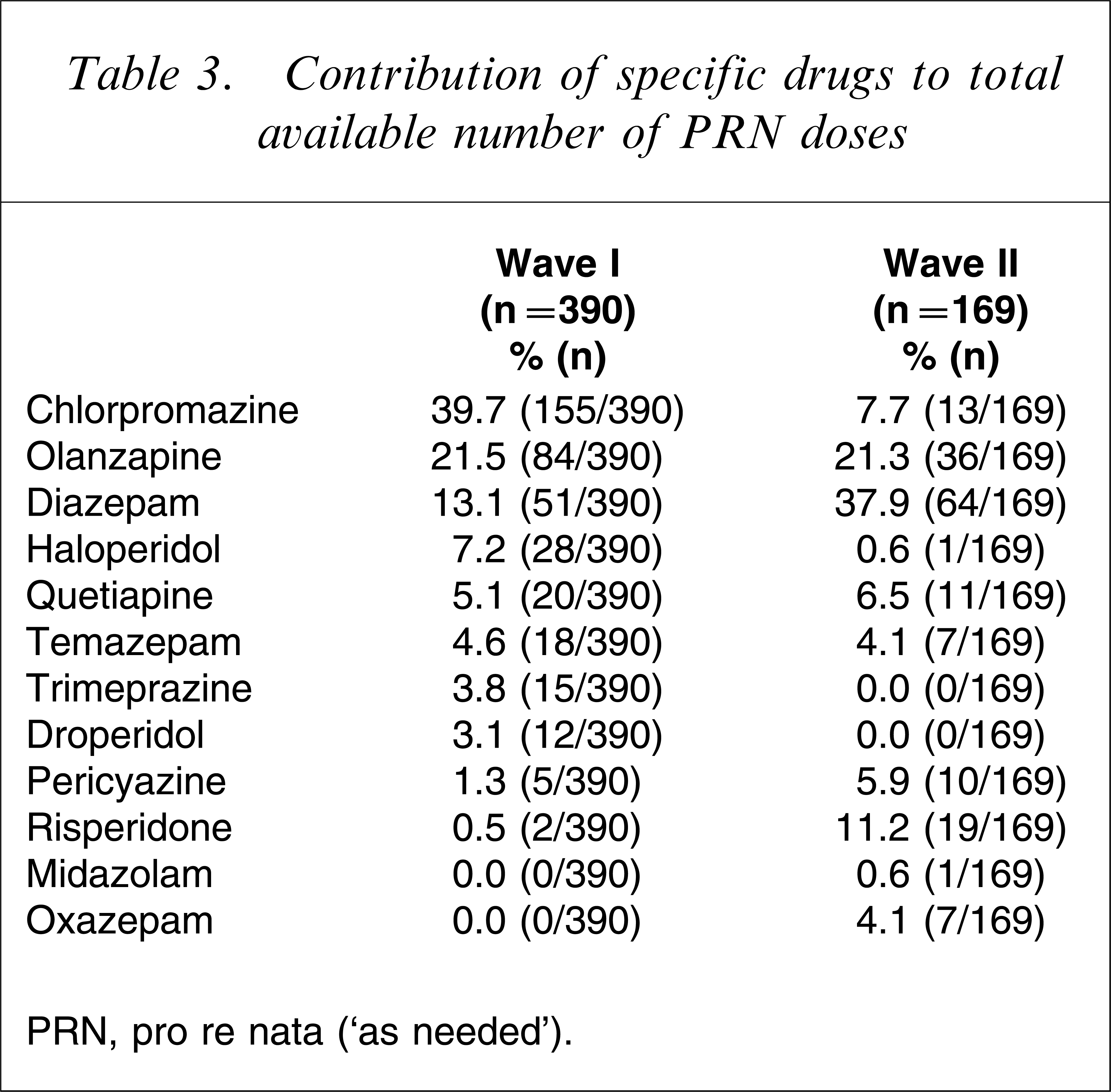
PRN, pro re nata (‘as needed’).
Examining the subset of patients prescribed PRN sedation during admission, there was a reduction in mean number of PRN drugs prescribed per patient (t = 2.85154, p < 0.01). Among those patients receiving PRN sedation, there was a reduction in the mean number of doses administered, but this was not statistically significant (t = 1.4883, p = 0.14). No difference was observed in the mean number of different drugs administered (t = 0.7287, p = 0.48; Table 2).
Indications for PRN sedation
In wave I the most frequently documented indications were agitation (38.7% of patients) and aggression (14.5%). In wave II the most frequently documented indications of PRN sedation were agitation (29.6% of patients), insomnia (15.5%) or a combination of both (4.2%). Aggression was a documented indication for only 5.6% of patients prescribed PRN sedation in wave II.
In wave II, when the older medication forms were used, two-thirds of patients (66.7%, 14/21) did not have an indication for PRN sedation recorded. When the new form was used, only 15.4% (4/26) of patients had no indication recorded (χ2=12.92, p < 0.01).
Predictors of PRN sedation use
To assess whether changes in use of PRN sedation occurred independently of differences in other patient characteristics observed between waves, we conducted a logistic regression using administration of PRN sedation as the outcome variable. Predictor variables were time period, age, sex, diagnosis of internalizing disorder, use of mood stabilizers, and use of typical antipsychotics. Independent significant predictors of receiving PRN sedation were being in wave I (odds ratio (OR) = 2.72, 95% confidence interval (CI) = 1.54–4.82, p < 0.01), and older age (OR = 1.13, 95%CI = 1.01–1.26, p < 0.05). Gender, diagnosis of an internalizing disorder, use of mood stabilizers and use of typical antipsychotics were not significant predictors of PRN sedation use. When use of stimulants was also entered into the model, wave remained a significant predictor of use of PRN sedation (OR = 3.01, 95%CI = 1.67–5.42, p < 0.001), as did older age (OR = 1.17, 95%CI = 1.04–1.32, p < 0.01) and use of routine stimulant medication (OR = 2.41, 95%CI = 1.03–5.69, p < 0.05).
Discussion
The present findings indicate that within this specific child and adolescent psychiatric inpatient unit, utilization of PRN sedation decreased over time. We observed a reduction in the numbers of young people receiving PRN sedation, and an overall reduction in the number of PRN doses and number of drugs prescribed and administered. This is likely to reflect a change in both the prescribing practices of medical staff and administration practices of nursing staff. Although we observed a reduction in the proportion of young people receiving PRN sedation, no significant changes in number of doses or number of drugs administered were observed in the subset of patients who did receive PRN sedation. Changes in PRN sedation over time occurred independently of patient characteristics or use of routine medications.
It is likely that the observed reductions in rates of prescribing and administration of PRN sedation occurred secondary to a several factors. In February 2004 the unit introduced a behavioural management programme for aggressive behaviour. This programme, described elsewhere, emphasized prevention of aggression, and encouraged management using the least restrictive intervention possible [15]. Within this context PRN sedation was still permitted, but was used after other interventions had been ineffective. Although nursing activities have been reported to generate short-term reductions in use of PRN sedation [16], short-term evaluation of this programme yielded only non-significant reductions in use of PRN sedation. In fact, rates of PRN administration fell from 46% to 36% prior to implementation of the behavioural management project [15], suggesting that other factors are influencing changes in use of PRN sedation. For example, changes in medical or nursing staff may have influenced prescribing or administration of PRN sedation. Clinicians may differ in their attitudes and experience, and thus their utilization of particular interventions. Additionally, it is possible for individual clinicians to change their attitudes and practices over time. It would have been interesting to assess attitudes surrounding PRN sedation and alternative interventions as potential determinants of utilization. An alternative explanation is that informal reporting of high utilization rates following the original survey raised staff awareness of its widespread use, leading to changes in practice. This possibility highlights the importance of reviewing existing practice as a process for optimizing practice, although existing research on the capacity of practice feedback to generate change is limited [17–19].
We also observed a shift in the types of drugs used for PRN sedation, in particular a shift from chlorpromazine to diazepam as the most commonly used drug. This may be explained by the increasing concerns about extrapyramidal side-effects and emerging clinical recommendations suggesting that benzodiazepines may be more appropriate than antipsychotics to manage acute distress [4, 13, 20, 21]. It may also reflect, however, a change in the predominant indications for PRN sedation. Agitation was the most commonly recorded indication in both waves for PRN sedation. In wave II, insomnia had replaced aggression as the second most common indication for PRN sedation. In the second wave a reduction in use of PRN sedation for aggression may have led to a relative increase in the proportion of doses used for anxiety and insomnia, which may be more appropriately treated with benzodiazepines rather than antipsychotics [22]. A limitation of the present study is that indications for PRN sedation were poorly documented, as has been reported elsewhere [11, 12], but the present findings suggest that recording of indications may be improved by changing drug documentation charts. One challenge for improving practice relates to the common use of ambiguous terms such as ‘agitation’, which may be interpreted differently by different clinicians [14]. It would be interesting for future research to examine factors predicting selection of a particular drug by clinicians.
The present study had a number of limitations. Although we observed a significant reduction in utilization of PRN sedation, it remains uncertain whether this reflects a persisting trend. We were also unable to examine attitudes of clinical staff involved in prescribing and administering PRN sedation. It is likely that staff attitudes and experiences are important determinants of utilization of interventions such as PRN sedation. Monitoring utilization over longer time periods, using a greater number of time points and assessing the role of potential influencing factors such as staff attitudes would enhance the capacity of future research to inform our understanding of these issues. Other study limitations include the reliance on a single site and use of retrospective data collection. Although we attempted to control for the influence of changing patient characteristics, it is possible that subtle differences in clinical presentations of patients that we were not able to measure contributed to reductions in use of PRN sedation. In spite of these limitations, to the best of our knowledge this is the first report documenting reductions over time in utilization of PRN medication in a child and adolescent unit.
Although young people may consider PRN sedation to be an acceptable intervention [23], there are a number of reasons why use of PRN sedation in children should be reduced. A key goal in management of aggressive children is to assist the child in acquiring skills required to regulate emotional states and control externalizing behaviour. Medication is unlikely to contribute to these goals [24]. PRN medication may contribute to risk of adverse effects or drug interactions [25, 26]. There is also a paucity of clinical data available to support its use in children and adolescents; widespread use of an intervention with minimal supporting evidence may exacerbate parental anxiety about use of psychotropic medications.
It is important to note that regular use of PRN sedation may reflect the need for more effective management of an underlying problem [11]. It logically follows that reducing patient distress by optimizing individualized and milieu-based interventions should reduce the demand for PRN sedation, rather than only use of PRN sedation per se. Achieving a reduction in patient distress is likely to involve multifaceted interventions that incorporate a range of therapeutic alternatives, both behavioural and pharmacological. Nursing interventions are often used in conjunction with PRN sedation [27]. Further research is required to understand the role of such non-drug interventions for common PRN indications such as anxiety and insomnia.
Additionally, the role of pharmacological alternatives to PRN sedation, and in particular the comparative role of PRN sedation and routine medications, is not well-established. It is unclear whether PRN medications provide an alternative to routine medications, or are best used as an adjunct intervention. In general, regular use of psychotropic medications is supported by greater evidence than use on a PRN basis. One study, however, reported that children and adolescents not receiving PRN sedation were more likely to receive polypharmacy [28]. In the present study, reductions in use of PRN sedation were not accompanied by any major increases in use of routine medications, and the small increases observed were not found to influence use of PRN sedation.
In summary, the present findings indicate that high levels of PRN sedation are not inevitable in a child and adolescent psychiatric inpatient unit. Nonetheless, a proportion of children may still require PRN sedation. Future prospective research is required to identify factors that influence changing utilization of PRN sedation, interventions that reduce use of PRN sedation, and to evaluate the safety and effectiveness of PRN sedation in this patient population.
Footnotes
Acknowledgements
The first author is supported by a Research Fellowship, provided by the National Health and Medical Research Council, Australia.