
Abstract
Keywords
Disaster survivors may develop a wide range of psychological impairments and psychiatric diseases, including posttraumatic stress disorder (PTSD), major depression (MD), sleep disorder, anxiety and substance abuse [1–5]. The most common of the disaster-related psychiatric diagnoses MD and PTSD are strongly associated with each other [4,5]. Posttraumatic stress disorder can be triggered by profoundly traumatic events such as earthquake, and the adaptive dysfunction is strongly associated with the development of all other psychiatric disorders [3,6–9]. The reported prevalence range for post-earthquake psychiatric disorders varies widely (1.5– 74%) [3–5,9–12], with the female gender predominating [4,5,8,12].
A devastating earthquake registering 7.3 on the Richter scale struck Taiwan in the early morning of 21 September 1999. The Chi-Chi earthquake provided an unusual opportunity to study the impact of disaster on the development of psychiatric disorders in the Taiwanese population [5,8,9]. Tong-Chi, the second-largest village in Yu-Chi township, was selected for the population survey because it is near the earthquake epicentre and the typical house architecture is relatively simple. Therefore, even where structural damage was severe, residents usually managed to escape from buildings when the earthquake struck and, unlike other townships, there were relatively few deaths and injuries [13]. This scenario minimized the confounding effects of physical trauma and facilitated purely psychiatric investigation. The residents of Tong-Chi village were evaluated postearthquake using the Mini-International Neuropsychiatric Interview (MINI) for diagnosis of psychiatric disease, and the quality of life (QOL) of the victims was assessed with the Taiwanese version of the Medical Outcomes Study Short Form-36 (MOS SF-36) [4,5,8], which has been used in many different countries [14,15]. This survey investigated the prevalence of, gender differences in, and risk factors for, development of psychiatric disorders, with particular emphasis on the occurrence of PTSD and major depressive episode (MDE) in surviving residents of Tong-Chi village who had experienced the 1999 earthquake [4]. The relationships between the psychiatric diseases and QOL at 6 [4] and 21 months [5] post-earthquake were investigated separately, revealing a trend towards MDE and PTSD as risk factors for poor QOL. As there had been no further reports of the longterm effects of such a disaster with respect to incidence of psychiatric diseases and QOL in Taiwan, a follow-up investigation was conducted to enhance understanding of the long-term effects of disaster, in terms of these fundamental indicators, in earthquake survivors. In this study, we have attempted to evaluate the prevalence of psychiatric diseases, as well as QOL and its predictors, which had not been assessed by other research teams in Taiwan, 3 years after the earthquake.
Method
Subjects
The residents of Tong-Chi village were selected for evaluation as they were considered equally exposed to the effects of the Chi-Chi earthquake. Household registrations indicated that the village had 736 residents (357 men and 379 women) 16 years or older. Mean age for these residents was 51.3 ± 18.0 years (range: 16–98), with 53.0% over 50 years. Education level was primary school or below for the majority of the population (56.0%). Most were married (77.6%). No sex differences were demonstrated comparing basic information items. We later learned that the registered population of 736 included 159 residents who had left Tong-Chi village before the earthquake (manifested as vacant households). In this most recent study, there were 405 respondents in total (189 men and 216 women), giving an overall response rate of 55.0% of the total registered population. When the vacant households were taken into account, however, the adjusted response rate was 70.2% (405/577). The mean age of the respondents was 55.4 ± 16.7 years (range: 17– 87); most respondents were married (80%). No significant differences were demonstrated comparing the demographic information for respondents and non-respondents.
Instrument
The demographic questionnaire (Disaster Related Psychological Screening Test, Part I) [8] was designed by five psychiatrists and two public-health professionals to investigate salient risk factors, including post-earthquake financial problems, social network change or family loss and psychiatric impairment, as well as to determine background information such as age, sex and educational and marital status [8,16]. Several benefits of the Taiwanese version of the MINI are brevity, simplicity, clarity, increased sensitivity and specificity, and ease of administration [5,8,16,17]. This relatively short instrument was designed to provide just enough diagnostic information to make good clinical decisions while investigating 17 Axis I diagnoses. Priority was given to the identification of current disorders, with no attempt made to identify the diagnostic subtypes of psychotic disorders. The MOS SF-36 incorporates the item, health change in the past year, as well as two dimensions, physical component summary and mental component summary, for estimation of health-related functions along eight subscales: physical functioning, role limitations due to physical problems, bodily pain, general health, role limitations due to emotional problems, vitality, social functioning and mental health [5,16].
Procedure
The psychiatric team conducted a 2-week psychiatric training program to instruct the six research assistants in the use of the Disaster Related Psychological Screening Test, and also arranged a 1-week training program to familiarize the psychiatrists with the Taiwanese version of the MINI. The details of this training program have been documented previously [5,16].
The research assistants then used the questionnaire to collect basic details and related risk-factor information, including demographic data, physical and economic status, familial injury and/or mortality and subjective assessments of memory function and social activity over the preceding month, from all residents aged 16 years or above. Analogous information for non-respondents was derived from local government records. The victims of the earthquake were visited at home 3 years after the earthquake occurrence by the research assistants, who also used the MOS SF-36 to assess respondent QOL. Approximately 2– 4 weeks later, the psychiatrists interviewed these same individuals using the MINI. To ensure measurement reliability, the psychiatrists and research assistants did not communicate with respect to the interview results during the study period. During every visit, the purpose of the research project was explained to the interviewee in detail. If the residents refused to participate at this point, only their demographic information was collected using the appropriate questionnaire. Informed consent forms were obtained from all respondents, together with approval from the local government authorities and the Department of Health, Taiwan.
Respondents were divided into three groups according to psychiatric diagnosis: posttraumatic stress disorder or major depression (PTSD/ MD), other psychiatric diseases (OPD) and mentally healthy (MH). The related risk factors and QOL for the three groups were then compared.
Data analysis
The chi-squared test was used for comparison of respondent demographic data for the three diagnostic groups. Subsequent to summation of the Likert-scale items in the MOS SF-36 survey, each scale was standardized so that response range was 0–100 (reflecting lowest to highest level of functioning, respectively). Analysis of variance was used to examine the score differences for each MOS SF-36 subscale for every diagnostic group, with the Scheffe method used for post-examination. A multiple regression model with forward stepwise analysis was also employed to study the significant main factors affecting the QOL subscale scores. All data were analysed using SPSS 10.0 statistical software (Chinese version, SPSS, Chicago, IL, USA).
Results
A total of 96 of the 405 respondents (23.7%) had at least one psychiatric diagnosis, and were assigned to the following groups: PTSD/MD (n = 40) [9.9%]; MD (n = 22) [5.4%]; PTSD (n = 14) [3.5%]; and PTSD & MD (n = 4) [1%] or OPD (n = 56) [13.8%]. The remaining 309 respondents (76.3%) were assigned to the MH group. There were no significant findings comparing sex, age, marital status and education level (Table 1). The prevalence of individual psychiatric diseases was investigated using the MINI (Table 2), with this study focusing on PTSD and MD, which are strongly associated with the occurrence of disaster. Comparing the mean subscale differences and standard deviations between the three groups (Table 3) revealed lower QOL for the PTSD/MDE group across all subscales; however, the OPD classification was not significantly associated with QOL, except in the physical functioning and mental health subscales. The multiple regression analysis provided predictions of the degree to which risk factors affected QOL subscale scores (Table 4). Negative correlations were demonstrated between age, physical illness, familial injury and/or death and social-activity decline in the physical functioning subscale (adjusted R2 = 0.37). Negative correlations were also demonstrated between age, physical illness, familial injury and/or death and diagnosis of PTSD or MD in the role limitation due to physical problems subscale (adjusted R2 = 0.27). Additionally, correlations between PTSD/MD group, age, female gender, physical illness and social-activity decline were negative, but positive between familial injury and/or death in the bodily pain subscale (adjusted R2 = 0.30). Negative correlations were demonstrated between age, female gender, physical illness, economic problems and PTSD/MD diagnosis in the general health perception subscale (adjusted R2 = 0.32). Further, negative correlations were demonstrated between age, female gender, physical illness, economic problems, memory decline and PTSD/MD diagnosis, but positive for current marital status in the vitality subscale (adjusted R2 = 0.26). Correlations were negative between physical illness, memory and social-activity decline and PTSD/MD diagnosis, but positive between current marital status in the social functioning subscale (adjusted R2 = 0.30). Negative correlations were demonstrated for the relationship between physical illness, economic problems and familial injury and/or death in the role limitation due to emotional problems subscale (adjusted R2 = 0.17). Finally, correlations were negative between female gender, physical illness, economic problems, memory and social-activity decline and diagnosis of PTSD/ MD, but positive between current marital status in the mental health subscale (adjusted R2 = 0.37).
Demographic data for psychiatric diseases in respondents from Tong-Chi village (n = 405)
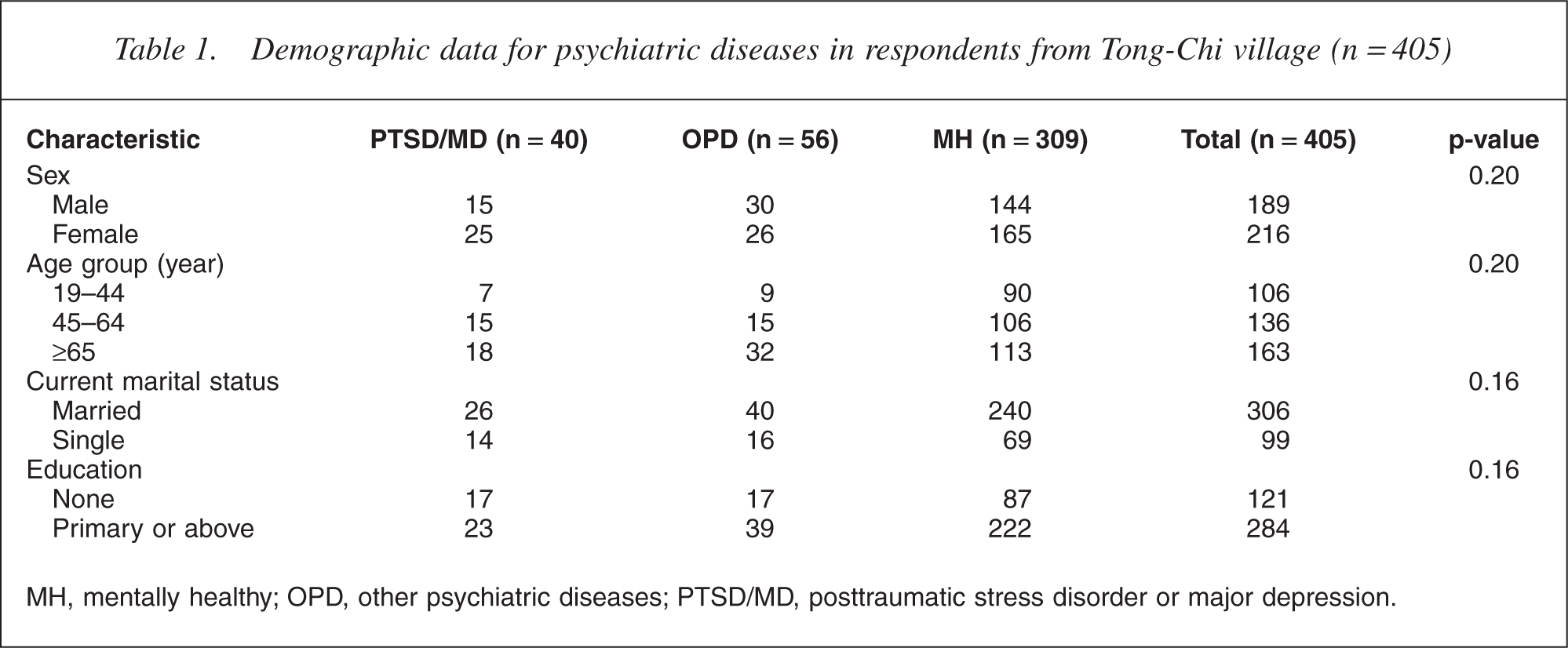
MH, mentally healthy; OPD, other psychiatric diseases; PTSD/MD, posttraumatic stress disorder or major depression.
Prevalence of psychiatric diseases from MINI in Tong-Chi village 3 years after earthquake (n = 405)
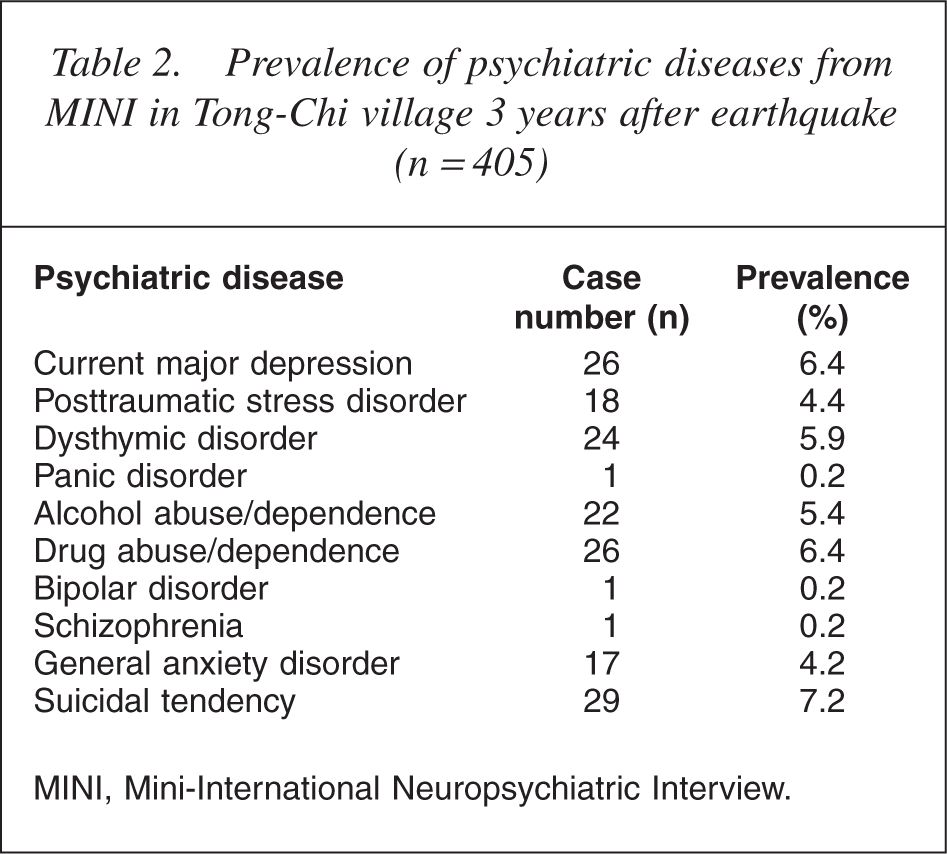
MINI, Mini-International Neuropsychiatric Interview.
Comparison of quality of life score stratified by diagnostic group 3 years after earthquake (n = 405)
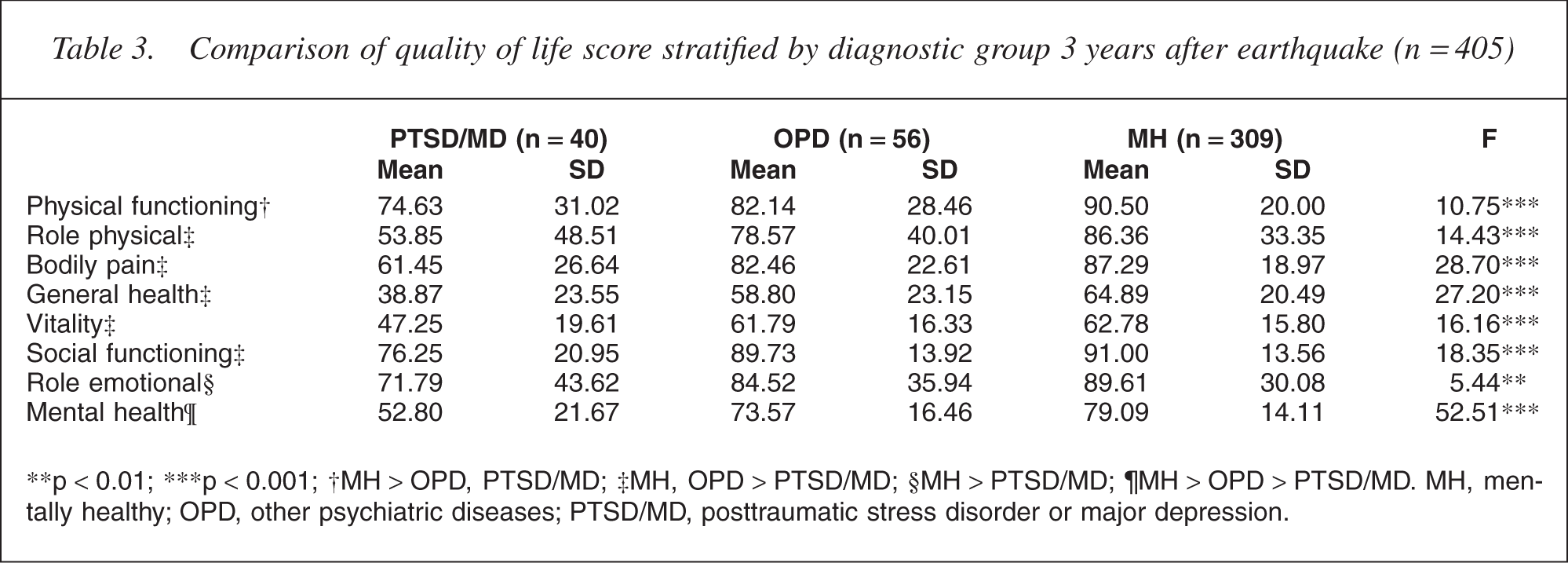
∗∗p <0.01; ∗∗∗p <0.001; †MH <OPD, PTSD/MD; ‡MH, OPD <PTSD/MD; §MH <PTSD/MD; ¶MH <OPD < PTSD/MD. MH, mentally healthy; OPD, other psychiatric diseases; PTSD/MD, posttraumatic stress disorder or major depression.
Multiple regression for prediction of MOS SF-36 subscale score for respondents 3 years after earthquake
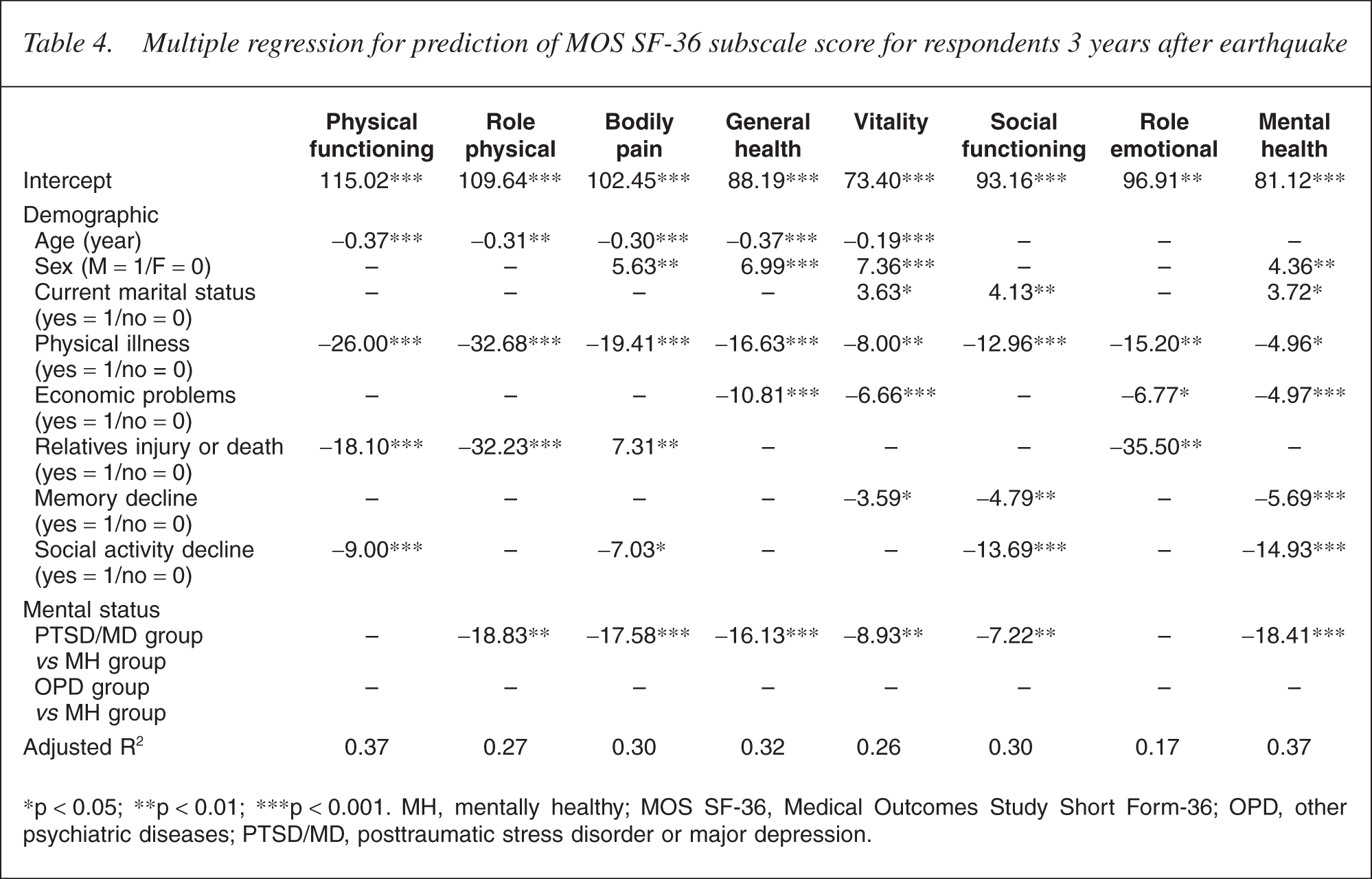
∗p <0.05; ∗∗p <0.01; ∗∗∗p < 0.001. MH, mentally healthy; MOS SF-36, Medical Outcomes Study Short Form-36; OPD, other psychiatric diseases; PTSD/MD, posttraumatic stress disorder or major depression.
Discussion
Many papers exploring post-earthquake PTSD have been published in the last 5 years [7–20]; however, the reported prevalence of this dysfunction was assessed from 3 to 20 months after the seismic disturbance, and long-term follow-up results were lacking. One of these reports investigated the incidence of PTSD and MDE 20 months after the 1999 earthquake in Turkey, with estimated rates of 39% and 18%, respectively, demonstrated for non-treatment-seeking earthquake survivors [19]. A retrospective study showed that lifetime selfreported exposure to natural disasters was 22%, and that the interval from the last event to study enrolment averaged 13 years [20]. Another investigation of Chi-Chi earthquake survivors revealed a prevalence rate for PTSD of 10.3% 10 months after the catastrophe [21]. These studies demonstrate that PTSD and MD may persist for at least 2 years if disaster survivors do not receive any treatment. In our previous investigation [4,5], the prevalence of MDE was 9.5% at 6 months and 8.2% at 21 months post-earthquake, respectively, with PTSD rates of 7.9% and 10.0%. There are two possible explanations for the increased PTSD rates 21 months postearthquake. First, the MH residents were more likely to migrate to urban areas in search of greater economic and educational convenience during this time. Second, PTSD symptoms in the responders may have been subclinical at 6 months post-tremor, with delayed onset only diagnosed at 21 months. This may account for the modest increase in PTSD prevalence in the second year. Our PTSD/MD incidence appears markedly lower than analogous-reported rates [5,8,16], but with the results mildly reduced relative to those studies conducted immediately post earthquake [9,12,16]. In the current study, the prevalence rates for MD and PTSD were 6.4% and 4.4%, respectively, 3 years after the Chi-Chi earthquake. Further, our 3-year MD prevalence was higher than analogous determinations in past Taiwanese reports that did not assess earthquake survivors, but with analogous rates of 0.97% and 5.6% demonstrated for a rural village population [22] and a sample of geriatric people, respectively [23]. Although there are no post-earthquake PTSD prevalence data for Taiwan before the 1999 earthquake, it appears reasonable to assume a low rate, as determined from the PTSD diagnostic criteria. The results of this investigation are similar to the findings of other reports, showing a positive correlation between earthquake occurrence and the relative prevalence of mental disorders. After the disaster, our research teams provided the villagers with ongoing medical and psychological treatment for about 18 months and established a good relationship with the local community. This professional rapport facilitated efficacious investigation in Tong-Chi village. Our 3-year prevalence rates for PTSD and MD were lower, perhaps owing to the fact that the earthquake survivors benefited from the availability of treatment [18–21]. Six months after the earthquake, 25 of the responders were diagnosed with MD, 18 with PTSD and 17 with MD combined with PTSD after doorto- door visitation. Twenty-one of the responders received antidepressants and/or psychotherapy for 18 months after the earthquake. Of the residents with PTSD or MD, 35% (21/60) received treatment, with a subsequent remission rate of approximately 50% [24]. This gradual reduction in MD over the more extended period suggests that survivors of cataclysmic events who suffer from mental disorders gradually improve after treatment or because of natural remission [4,5].
The QOL subscale scores were decreased for the PTSD/MD group relative to the MH analogue. The QOL scores for the OPD and MH groups were comparable, but with the exception of the physical functioning and mental health subscales, with statistically significant differences not demonstrated. Further, although mean scores for all QOL subscales were higher for the OPD group, decreased QOL scores were more significant for the PTSD/MD group only for the role limitation due to physical problems and mental health subscales. This may indicate that, 3 years after the earthquake, statistical power was not adequate to reveal significance because the prevalence of PTSD and MD had decreased. However, despite the demonstrated lack of significance, it appears reasonable to conclude that, for survivors diagnosed with PTSD or MD, long-term treatment and rehabilitation programs should be emphasized to improve their QOL.
From multiple regressions for prediction of MOS SF-36 subscale scores, prominent risk factors were age, female gender, physical illness, economic problems, familial injury and/or death, subjective assessment of memory and social-activity decline, and diagnosis of PTSD or MD. For elderly subjects, a significant negative correlation was demonstrated for the physical function, role limitation due to physical problems, bodily pain, general health and vitality QOL subscales, revealing that ageing was associated with physical but not mental deterioration. Economic problems and self-reported memory decline were predictors of decreasing scores on several QOL subscales, especially in the mental dimension, which agrees with our general understanding. We may conclude therefore that the persistence of long-term economic problems is one of many important factors affecting QOL. The factor of social-activity decline was associated with both the physical and mental dimensions. Familial economic loss was also a significant risk factor reflected in several QOL subscales, but not body pain and social function. The PTSD/MD classification was significantly associated with decreased scores on many QOL subscales; however, this effect did not extend to physical functioning and role limitation due to physical problems. As might be expected, the associations between the PTSD and MD diagnoses and the QOL subscales were less significant 3 years post-earthquake in comparison to 6 months post-catastrophe [4]. Further, the influence of PTSD/MD diagnosis on QOL decreased gradually reflecting the psychological alleviation of earthquake impact over time. In long-term follow-up of earthquake victims emphasis should be placed on the treatment of MD and PTSD.
On the other hand, we found the aged scored lower on the QOL subscales, especially in the physical dimension. Female gender tended to have lower QOL scores on the bodily pain, general health, vitality and mental health subscales. Scores appeared higher comparing the married survivors to others in the mental dimension. Further, survivors with physical illnesses scored lower on all QOL subscales, reflecting the generality of effect across both physical and mental dimensions. The diagnosis of PTSD/MD had a comparable effect on almost all of the QOL subscales, except physical function and role limitation due to emotional problems. This confirms the general proposition that physical and mental health are interrelated, as indicated in the reports of other authors [25]. Therefore, mental and physical function should be emphasized contemporaneously in any intervention for, or study of, the victims of major catastrophe.
There were a number of limitations to our study. First, given the profound ethical considerations implicit in intervention for natural disaster, psychiatric diseases were treated immediately an accurate diagnosis was delivered, so there was no control group for comparison. Second, the emigration of residents in the 3 years after the earthquake owing to economic and social factors introduced some bias affecting our study results. Third, longitudinal variations in economic and political factors may have also introduced confounding factors. In addition, a lack of trauma exposure prior to the earthquake may be a cumulative or vulnerable factor influencing proportion of psychiatric dysfunction in the respondent population.
Conclusion
Compared with the previous investigations of the 1999 Chi-Chi earthquake, our study shows that, relative to the general population [5,16], a higher percentage of the survivors developed various psychiatric disorders, with the increased prevalence persisting but gradually declining at 3 years after the event. However, this inter-study difference does appear to decrease. The risk factors that affected QOL in our survivor population were age, female gender, physical illness, economic problems, subjective assessment of memory and social-activity decline and diagnosis of PTSD or MD.
Footnotes
Acknowledgements
The study was supported by grants from the National Science Council, Taiwan (No. ROC NSC 90-2625-Z-280-001 and ROC NSC-90-2625-Z-010-001).