
Abstract
Objectives:
The primary aim of this study was to investigate neuropsychological function in patients with earthquake-related posttraumatic stress disorder, compared with earthquake-exposed but resilient controls. We hypothesised that individuals with posttraumatic stress disorder would have poorer neuropsychological performance on tests of verbal and visuospatial learning and memory compared with the earthquake-exposed control group. The availability of groups of healthy patients from previous studies who had been tested on similar neuropsychological tasks prior to the earthquakes allowed a further non-exposed comparison.
Method:
In all, 28 individuals with posttraumatic stress disorder and 89 earthquake-exposed controls completed tests of verbal and visuospatial learning and memory and psychomotor speed. Further comparisons were made with non-exposed controls who had been tested before the earthquakes.
Results:
No significant difference in performance on tests of verbal or visuospatial memory was found between the earthquake-exposed groups (with and without posttraumatic stress disorder), but the posttraumatic stress disorder group was significantly slowed on tests of psychomotor speed. Supplementary comparison with historical, non-exposed control groups showed that both earthquake-exposed groups had poorer performance on a test of visuospatial learning.
Conclusion:
The key finding from this study is that there were no differences in verbal or visuospatial learning and memory in individuals with posttraumatic stress disorder compared with similarly earthquake-exposed controls. Compared with non-exposed controls, both earthquake-exposed groups had poorer performance on a test of visuospatial (but not verbal) learning and memory. This offers preliminary evidence suggesting that it is earthquake (trauma) exposure itself, rather than the presence of posttraumatic stress disorder that affects aspects of neuropsychological functioning. If replicated, this may have important implications for how information is communicated in a post-disaster context.
The experience of a natural disaster has been shown to result in increased mental health disorders particularly posttraumatic stress disorder (PTSD) in a small but significant minority of the population (Fergusson et al., 2014). There is also a robust literature reporting that most people exposed to such a trauma follow a resilient trajectory, with relatively short-lived distress which then settles (Bryant et al., 2014).
Memory in PTSD, particularly intrusive memories of traumatic experiences, has been the focus of considerable research (Brewin and Holmes, 2003; Dalgleish, 2004). However, although these re-experiencing symptoms are often seen as the hallmark of PTSD, clinically individuals often also report difficulty remembering emotionally neutral information. This is important to understand because it may pose a barrier to psychological treatment (Brewin, 2005). Previous findings have not been consistent, but two meta-analyses have reported memory deficits for emotionally neutral information in PTSD of small-to-moderate effect size, with effects being stronger for verbal than for visual memory (Brewin et al., 2007; Johnsen and Asbjornsen, 2008). The effect sizes are moderate when individuals with PTSD are compared with non-exposed controls and smaller when the comparison is with trauma-exposed controls.
The evidence for a smaller degree of memory impairment when individuals with PTSD are compared with exposed, but psychiatrically well individuals suggests that exposure to trauma may itself have a detrimental effect on neuropsychological performance. Indeed, the media often reports on these issues in the population describing them as, for example, ‘earthquake brain’ or ‘flood-brain’ (Crowe, 2011). This too is important to understand, particularly after a natural disaster where large numbers are exposed, because communication and psychoeducation are the cornerstones of recommended population-based interventions. There has therefore been increasing interest in examining the effects of trauma exposure on neuropsychological functioning in non-clinical individuals compared to non-exposed controls. Stein et al. (2002) showed that women exposed to intimate partner violence (with and without PTSD) had poorer neuropsychological performance regardless of PTSD status compared with healthy controls. However, Golier et al. (2005) comparing a small group of holocaust survivors with and without PTSD with non-exposed controls reported significantly poorer memory function in those with PTSD, while there was no difference between non-PTSD and non-exposed participants. Similarly, Chung et al. (2014) in a study of victims of domestic violence found no difference on a variety of neuropsychological tasks including tests of verbal memory between those exposed but without PTSD and healthy controls. Overall, results of these studies are heterogeneous, possibly due to the varying type and duration of trauma exposure.
Over 2010–2011, Canterbury, New Zealand, experienced four major earthquakes (moment magnitude scale MW > 6.0) and thousands of aftershocks, resulting in 185 deaths, thousands of injuries, major property and infrastructure damage throughout the city and loss of the majority of the central business district (Ardagh et al., 2012). This led to a large number of people being exposed to similar traumatic events and therefore created the opportunity to examine people with similar trauma exposure who either did or did not develop PTSD.
The primary aim of this study was to investigate neuropsychological function in individuals with PTSD compared with earthquake-exposed but resilient controls. We hypothesised that individuals with PTSD would perform less well on tests of memory than earthquake-exposed controls.
As a supplementary analysis, we also used data collected prior to the earthquake sequence from two groups of healthy individuals. Neuropsychological tasks which were common to non-exposed controls and the post-earthquake study were able to be compared. This created a comparison of individuals with PTSD, individuals exposed to similar trauma but who were resilient (the earthquake-exposed controls) and healthy controls not exposed to earthquakes and related traumas (the non-exposed controls). We specifically hypothesised that the earthquake-exposed controls would perform less well than the non-exposed controls.
Method
Participants
Earthquake-exposed PTSD group
This group were Canterbury residents with PTSD (n = 28) who had been referred for treatment to a Specialist Mental Health Service for members of the community with earthquake-related PTSD. These patients had a full clinical psychiatric assessment by an experienced clinician (F.A.C., H.C.C., J.J., V.V.W.M. or C.J.B.) confirming the diagnosis prior to beginning treatment. Participants were recruited between February 2013 and April 2015 (which was between 2 and 4 years after the most devastating February 2011 earthquake).
Earthquake-exposed control group
This group were Canterbury residents who self-identified as resilient, that is, coping well, despite moderate to high exposure to earthquake-related events (such as physical injury or illness, death of a loved one, witnessing falling buildings, seeing bodies, property loss, income loss or problems with housing caused by earthquake-related events; n = 89). They were recruited in response to articles, opinion pieces and community notices in local newspapers and via word of mouth over the course of 13 months, from January 2013 to February 2014. These participants had a face-to-face assessment (by R.A.S., L.M.A.M. and A.L.) and completed diagnostic and self-report questionnaires to confirm that they had no earthquake-related psychiatric diagnoses and had not received any earthquake-related counselling.
Supplementary analysis – comparison with non-exposed control groups
Two healthy non-exposed control groups from historical studies were used: non-exposed control group 1 (n = 61) allowed comparison of verbal learning and memory using the Rey Auditory Verbal Learning Test (RAVLT; Porter et al., 2016); non-exposed control group 2 (n = 50) allowed comparison of visuospatial learning and memory (using the Groton Maze Learning Test (GMLT) and Timed Chase Test, CogState© (Douglas et al., 2011). These participants were all psychologically healthy individuals without a personal or family history of mental illness. They were recruited through advertisements in local newspapers and flyers in public places from the general population in Canterbury prior to the earthquakes between June 2007 and March 2009 and thus represent a non-exposed comparison group.
Neuropsychological assessment
The neuropsychological testing battery was designed to assess a range of neuropsychological functions, particularly in the memory domain given the importance of memory functions in etiological models of PTSD. Consideration was given to the severity of symptoms in the PTSD group when determining the length of the testing battery. Pencil-and-paper tasks were administered according to standardised instructions (Lezak et al., 2004) and computerised tasks according to corresponding manual protocols (E-Prime 2.0 software [Psychology Software Tools, Inc] and CogState [CogState Inc; www.cogstate.com]) on a PC laptop. Neuropsychological tasks were administered in a fixed sequence.
Verbal learning and memory
The RAVLT (Rey, 1964) assessed verbal learning and memory. The number of words remembered after a total of five trials, after a distractor list (post-interference) and after 20 minutes (delayed) was recorded as well as number of words from the distractor list.
Visuospatial learning and memory
The GMLT (CogState©) assessed visuospatial learning and memory (for detailed description of GMLT, see Snyder et al., 2008). On a computer screen, participants navigated through a 28-step hidden pathway, within a 10-by-10 grid of squares. The process was repeated for four successive learning trials (i.e. five learning trials in total) and one delayed trial after 20 minutes. On each trial, the number of errors was recorded.
In the comparison of non-exposed control study, only four learning trials were conducted for the GMLT. Thus, in the analysis comparing earthquake-exposed groups with non-trauma-exposed groups on the GMLT, only learning over the first four GMLT trials could be included.
Psychomotor speed
Psychomotor speed was assessed using the Timed Chase Test (which is a control task for the GMLT, involving participants chasing a moving tile around a grid of squares for 30 seconds) and the Digit Symbol Coding (Wechsler, 2008), which assessed participants’ ability to correctly draw symbols that corresponded with specific digits under time pressure (90 seconds).
Procedure
Assessments took place at a University Clinical Research Unit in Christchurch, New Zealand. Participants completed a diagnostic interview with the Mini-International Neuropsychiatric Interview (MINI; Sheehan et al., 1998) and self-report demographic measures. The earthquake-exposed groups (PTSD and earthquake-exposed controls) also completed other clinical measures. These included the PTSD checklist (PCL-S; Foa et al., 1993); Depression, Anxiety and Stress Scale (DASS; Lovibond and Lovibond, 1995); Connor–Davidson Resilience Scale (CDRS; Connor and Davidson, 2003); Social Adjustment Scale (Weissman and Bothwell, 1976); a Visual Analogue Scale (VAS) rating anxiety on the test day using a 10 cm scale (0 = no anxiety to 5 = severe anxiety); Trauma Exposure Severity Scale (TESS; Elal and Slade, 2005) and the Life Events Scale (LES; adapted from the Crisis in Family Systems (CRSYS; Shalowitz et al., 1998).
The PCL-S assesses current (past month) symptoms of PTSD in relation to an identified stressful experience. It consists of 17 items which correspond to Diagnostic and Statistical Manual of Mental Disorders (4th Edition; DSM-IV) symptoms and asks how often the person has been bothered by each symptom coded from 1 to 5 (1 = not at all, through to 5 = extremely). The total symptom severity score ranges from 17 to 85 with scores above 44 being in the clinical range (Blanchard et al., 1996).
The DASS-21 measures 21 symptoms over the past week; seven items each for depression, anxiety and stress rated from 0 to 3 (0 = did not apply to me to 3 = applied to me very much or most of the time; Ng et al., 2007). The DASS-21 scores (doubled to be comparable to the DASS-42) indicate overall severity of symptomatology and give subscale totals for depression, anxiety and stress. For the depression subscale, normal–mild has been defined as a score of 0–13 and moderate–extreme as 14–28. For the anxiety subscale, normal–mild has been defined as a score of 0–9 and moderate–extreme as 10–28. For the stress subscale, normal–mild has been defined as a score of 0–18 and moderate–extreme as 19–28 (Lovibond and Lovibond, 1995).
The CDRS assesses resilience over the past month. It consists of 25 items rated from 0 to 4 (0 = not true at all to 4 = true nearly all the time). The scores are summed and range from 0 to 100 with higher scores reflecting greater resilience.
The SAS assesses social functioning over the past 2 weeks. It consists of 45 items each rated from 1 to 5 with higher scores indicating greater impairment. The final score is derived by summing the scores and dividing by the number of items and ranges between 1 and 5.
The TESS measures the number of earthquake-related stressors and the distress experienced in relation to these. Examples of items included were you or your loved ones injured? Did you see falling buildings? and Was your home damaged? It consists of 24 items, and participants are asked whether they had experienced the stressor (Yes/No), and if yes, how distressing this had been on a scale where 1 = not at all and 5 = extremely. The TESS Number of Exposures and Distress scores are summed.
The LES measures the number of contemporary life stressors and how difficult these were within the last 5 years and the last 6 months. Examples of items included Did your income increase or decrease? Did you have legal problems? and Did you marry or divorce? It consists of 63 items in 11 content domains (financial, legal, career, stability in relationships, safety in the home, safety in the community, medical issues pertaining to respondent, medical issues pertaining to others, housing problems, difficulty with authority and prejudice). Participants are asked whether they had experienced the life event (Yes/No), and if yes, how difficult his had been on a scale where 1 = not at all and 5 = extremely. The LES number of events and difficulty scores are summed.
Ethical approval
The study was approved by the National Health and Disability Ethics Committee URA/12/03/11 and written informed consent was given before participation in the studies.
Statistical analyses
Statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS) version 23 for Windows. Demographic and clinical data were summarised using standard descriptive statistics including means, standard errors (SEs), ranges, frequencies and percentages as appropriate. Comparison of demographic and clinical variables between the PTSD and earthquake-exposed controls used analysis of variance (ANOVA) and Chi-square tests. Analysis of neuropsychological test variables was conducted using analysis of covariance (ANCOVA) with group as the between-participant factor and age, gender, years of education, anxiety level on test day and depression (depression subscale score of the DASS) as covariates to adjust for baseline clinical features known to impact on neuropsychological functioning. Spearman’s rank-order correlations were performed to correlate PCL measures of symptoms (total and subscale) with scores on the neuropsychological tests for the PTSD and the earthquake-exposed groups. A two-tailed p value <0.05 was taken to indicate statistical significance.
For supplementary analyses, the same comparisons were extended to include the non-exposed controls with similar comparisons using ANCOVA adjusting for age, gender and years of education. Clinical variables were not included as covariates as the non-exposed controls did not complete clinical questionnaires. There were some differences in the GMLT methodology with only four learning trials included in the non-exposed control groups (rather than five) which meant that only learning over the first four GMLT trials could be included in this comparison.
Results
Demographic and clinical measures
Table 1 shows that there were a similar proportion of males and females in the two earthquake-exposed groups and that the earthquake-exposed controls were significantly older and had more years of education than the PTSD group. As expected, the PTSD group had markedly increased rates of current PTSD, depression, other anxiety disorders and antidepressant use. Of the PTSD group, eight participants (32%) had had a diagnosis of PTSD prior to the earthquakes, seven of eight were in full remission at the time of the earthquakes and one participant in partial remission. None of the earthquake-exposed controls had a current or previous diagnosis of PTSD. The one individual with current depression and two with current panic disorder had had these disorders before the start of the earthquakes. Table 1 shows the expected clinical differences between the PTSD and earthquake-exposed controls as measured by symptoms of PTSD (PCL); depression, anxiety and stress (DASS); resilience (CDRS); general functioning (SAS) and ratings of anxiety on the test day. Of note, the self-report scores from the earthquake-exposed controls, who had self-identified as resilient and coping well, reflected this with DASS and PCL mean scores being well within in the normal range. The earthquake-exposed group were not a sub-clinical sample with, for example, the mean score from the PCL of 22 being close to minimum possible score of 17. The two groups experienced similar levels of distress from earthquake exposure (from the TESS) and from life events (from the LES).
Comparison of demographic and clinical variables between PTSD group, earthquake-exposed controls and non-exposed controls (in italics).
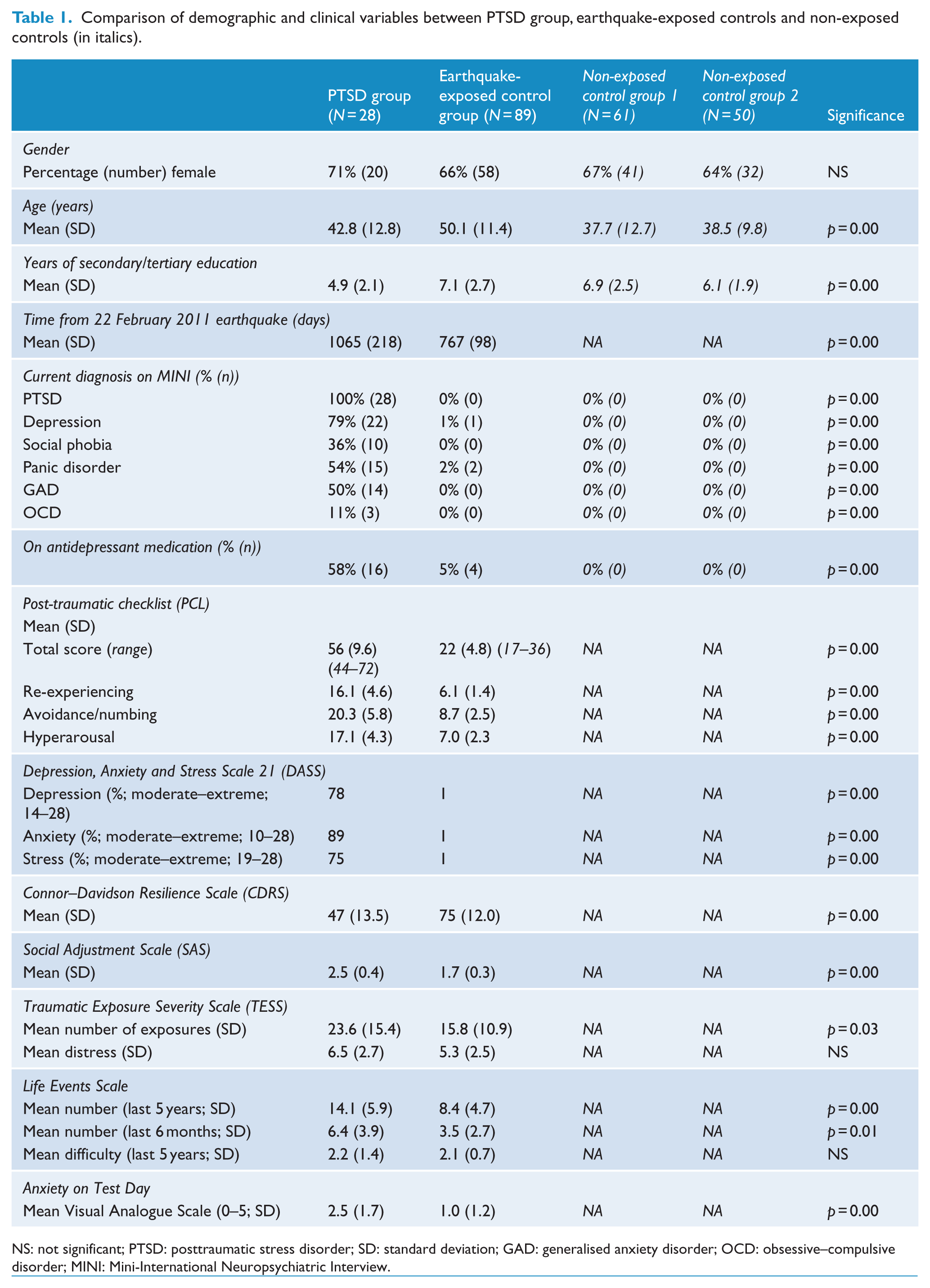
NS: not significant; PTSD: posttraumatic stress disorder; SD: standard deviation; GAD: generalised anxiety disorder; OCD: obsessive–compulsive disorder; MINI: Mini-International Neuropsychiatric Interview.
Testing days for the two groups occurred some considerable time after the most devastating February 2011 earthquake: mean of 755 (SD = 108) days for the earthquake-exposed controls and 1053 (SD = 201) days for the PTSD group. The difference between the two groups was due to PTSD patients being recruited as they were referred for treatment, whereas the earthquake-exposed controls were a research cohort recruited over a specific timeframe.
Neuropsychological variables
Verbal learning and memory (RAVLT)
Repeated-measures ANCOVA showed no significant between-group effects (PTSD vs earthquake-exposed controls) on the RAVLT measures.
Visuospatial learning and memory (GMLT)
No between-group effect for GMLT total learning (total errors from trials 1–4) or for GMLT delay recall (total errors) was found although there was a non-significant trend for GMLT total learning (total errors from trials 1–4) to be poorer in the PTSD group. These results are shown in Table 2. Secondary exploratory analysis showed that when depression was removed as a covariate, a significant effect was seen on both measures, total errors from trials 1–4, F(1, 115) = 12.7, p = 0.001, and total error delay, F(1, 112) = 5.1, p = 0.03.
ANCOVA showing group effect of neuropsychological assessments in PTSD and earthquake-exposed controls.
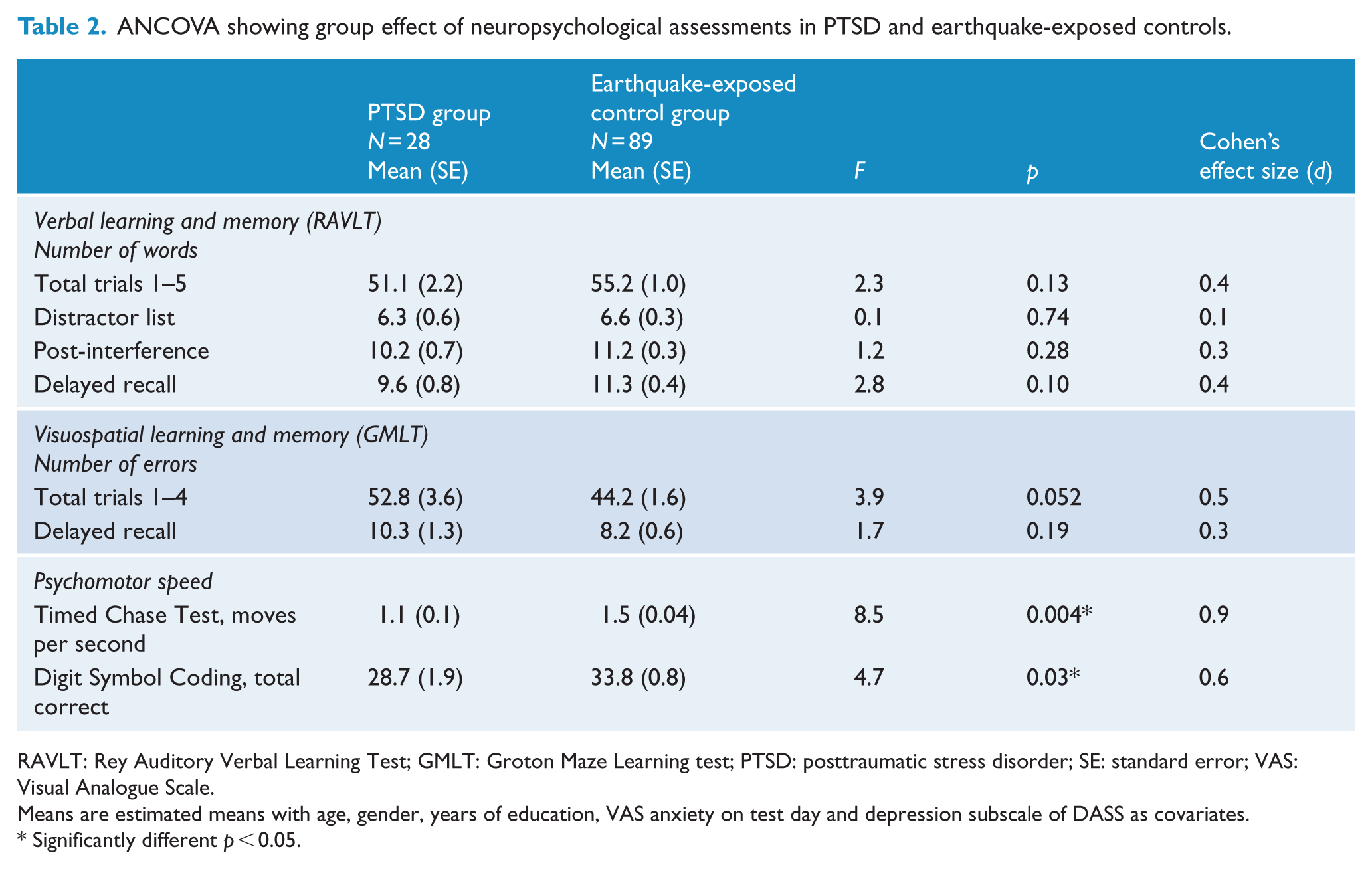
RAVLT: Rey Auditory Verbal Learning Test; GMLT: Groton Maze Learning test; PTSD: posttraumatic stress disorder; SE: standard error; VAS: Visual Analogue Scale.
Means are estimated means with age, gender, years of education, VAS anxiety on test day and depression subscale of DASS as covariates.
Significantly different p < 0.05.
Psychomotor speed
ANCOVA showed a significant group effect both for the Timed Chase Test, F(1, 115) = 9.9, p = 0.002, and Digit Symbol Coding, F(1, 115) = 11.2, p = 0.001. The PTSD group was significantly slower on both measures.
Correlation of PCL scores with neuropsychological functioning
No correlation was found for PCL (total and subscale) scores with performance on the RAVLT, GMLT or psychomotor speed tasks for either the PTSD or earthquake-exposed controls.
Comparison of PTSD group, earthquake-exposed controls and non-exposed control groups
Demographic and clinical variables for the non-exposed control groups are shown in Table 1 with the expected clinical differences. Analysis of performance on the neuropsychological measures (ANCOVA) comparing PTSD with earthquake-exposed and non-exposed control groups with age, gender and years of education as covariates is presented in Table 3. Clinical variables of depression and anxiety on the test day were not included as covariates in this analysis because the non-exposed control groups did not complete the clinical questionnaires.
ANCOVA showing group effects of neuropsychological assessments in PTSD, earthquake-exposed controls and the two non-exposed controls (in italics).
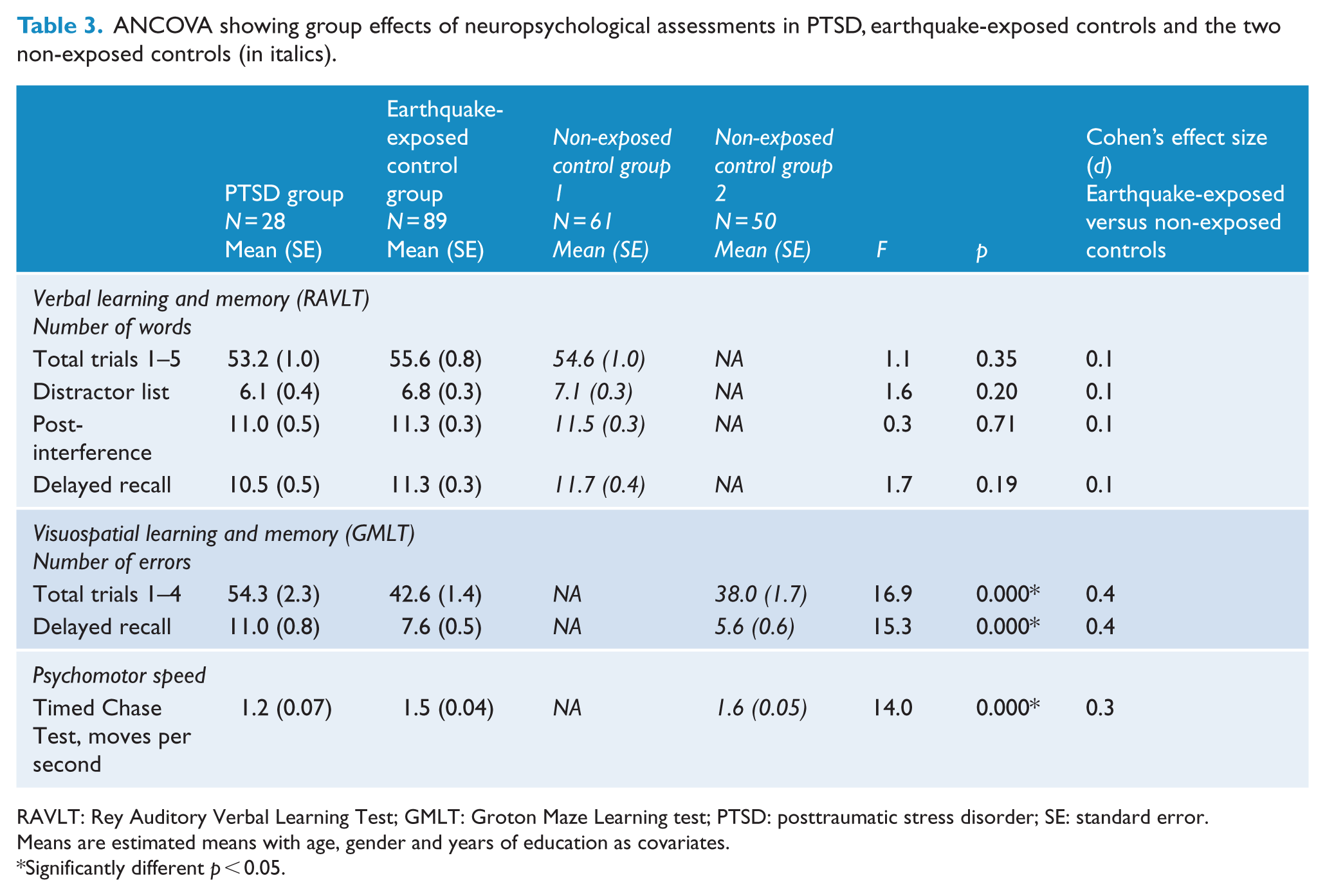
RAVLT: Rey Auditory Verbal Learning Test; GMLT: Groton Maze Learning test; PTSD: posttraumatic stress disorder; SE: standard error.
Means are estimated means with age, gender and years of education as covariates.
Significantly different p < 0.05.
Verbal learning and memory (RAVLT)
Repeated-measures ANCOVA (PTSD, earthquake-exposed and non-exposed control groups) showed no significant effect of group for any of the RAVLT measures.
Visuospatial learning and memory (GMLT)
Repeated-measures ANCOVA (PTSD, earthquake-exposed, non-exposed control groups) showed a significant effect of group. Pairwise comparisons showed significant differences between the PTSD group and earthquake-exposed control group (p < 0.001) and between the PTSD group and the non-exposed control group (p < 0.001) for GMLT total learning (total errors from trials 1–4) and for GMLT delay recall (total errors). This is different from Table 2 because depression was not included as a covariate. Pairwise comparisons showed a significant difference between the earthquake-exposed and non-exposed controls for GMLT delay recall (total errors; p = 0.014) and a trend towards a significant difference for GMLT total learning (total errors from trials 1–4; p = 0.051). These results are shown in Figures 1 and 2.
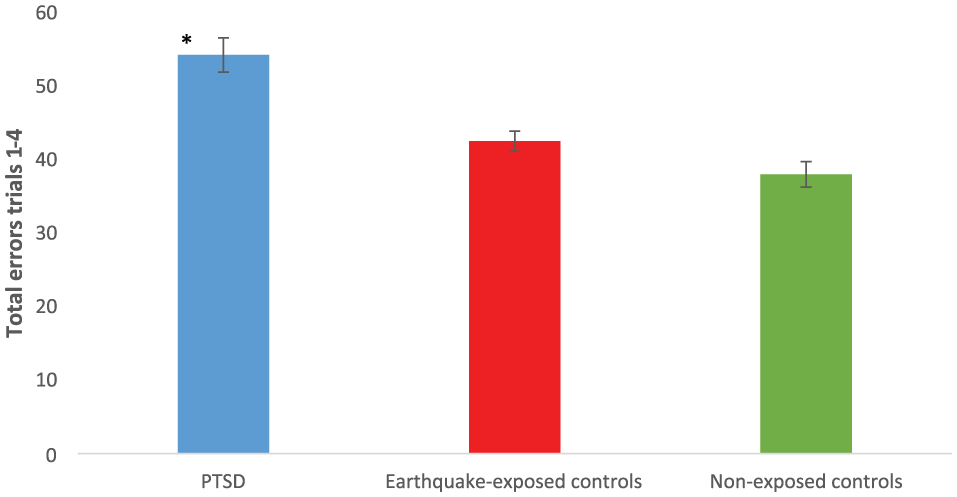
Mean (SEM) of total errors from trials 1–4 from GMLT in PTSD, earthquake-exposed and non-exposed controls. These results did not include depression as a covariate.
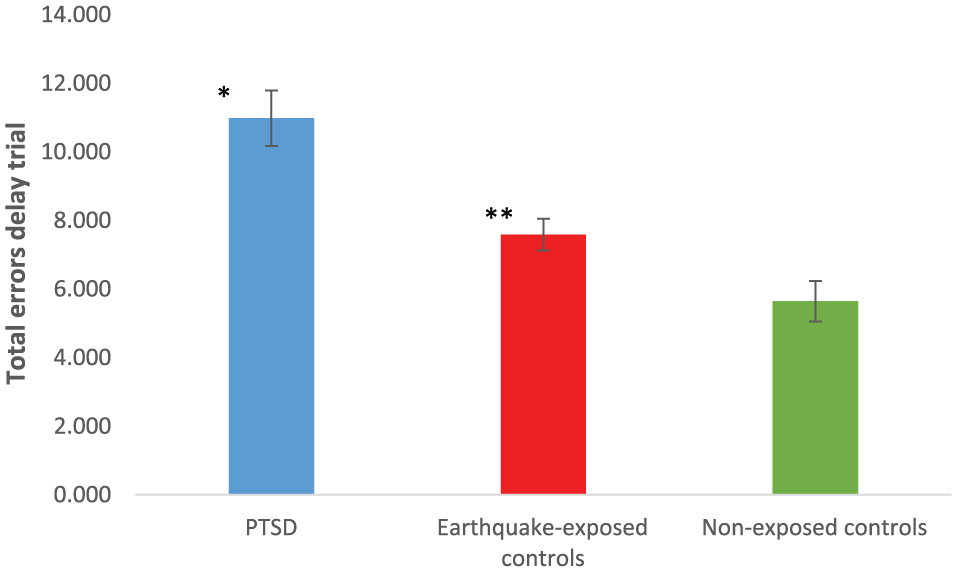
Mean (SEM) of total errors delay from GMLT in PTSD, earthquake-exposed controls and non-exposed controls. These results did not include depression as a covariate.
Psychomotor speed
Repeated-measures ANCOVA showed a significant effect of group on psychomotor speed from the Timed Chase Test. Pairwise comparisons showed significant differences between the PTSD group and the earthquake-exposed control group (p = 0.00) and between the PTSD group and the non-exposed control group (p = 0.00), but no significant difference between the earthquake-exposed and non-exposed control groups (p = 0.081).
Discussion
The primary aim of this study was to investigate neuropsychological function in individuals with PTSD compared with earthquake-exposed but resilient controls. We hypothesised that individuals with earthquake-related PTSD would perform significantly less well than healthy earthquake-exposed participants on tasks of both verbal and visuospatial learning and memory. Counter to our hypothesis, we found no such differences in performance although there was a non-significant trend for the PTSD group to perform less well on a task of visuospatial memory.
As expected, the PTSD group had significant PTSD (as evidenced by the MINI diagnostic interview and the self-report scores from the PCL), depression and other mental health disorders. The earthquake-exposed control group, who had self-identified as coping well, also had diagnostic and self-report scores reflecting their resilient state. Interestingly neither of the groups had specifically greater increased ratings of hyperarousal symptoms from the PCL despite exposure to ongoing aftershocks and other stressors as a result of the earthquakes.
The finding from this study was of no significant difference in performance on tasks of verbal or visuospatial memory between the PTSD and trauma-exposed controls although there was a non-significant trend for the PTSD group to perform less well on the GMLT total learning task. Similar findings have been reported previously by a study of interpersonal violence (Stein et al., 2002), but results have not been consistent. There have also been reports that there may be different impacts for different types of trauma exposure. For example, memory impairments have not been reported when individuals with PTSD secondary to sexual abuse are compared with similarly exposed controls without PTSD (Johnsen and Asbjornsen, 2008). Interestingly, the meta-analyses described above, which report memory deficits of small-to-moderate effect size did not include any studies where the PTSD had resulted from exposure to natural disasters (Brewin et al., 2007; Johnsen and Asbjornsen, 2008). As far as we are aware, there has been only one previous report of neuropsychological functioning after a natural disaster. This included 56 people, with and without PTSD, 4 years after an earthquake in Turkey, and reported impaired performance in the PTSD group on a test of immediate verbal recall (Eren-Kocak et al., 2009).
In our study, when current depression score was not included as a covariate in the analysis, there were significant differences in visuospatial learning and memory with the PTSD group performing less well than the earthquake-exposed controls. This suggests that differences may relate to symptoms of depression or to a history of depression. We note that there was a significantly higher percentage of the PTSD group with a history of depression than in the exposed control group; however, we opted to control for current symptoms rather than history of depression since this was a more sensitive analysis. Some previous studies have, in fact, suggested that the differences in neuropsychological functioning reported in PTSD may reflect high comorbidity with depression (Barrett et al., 1996; Johnsen et al., 2008). Although this has not been a universal finding, the results from our study provide some support for this in that the differences in visuospatial memory performance between the PTSD and earthquake-exposed control groups were explained by measures of depression.
The PTSD group also performed significantly more slowly than the earthquake-exposed control group on tests of psychomotor speed even when adjusting for depression symptoms. Although the differences are not at the level of those seen in psychomotor retardation, it suggests that those with PTSD may be processing information more slowly. It is possible that this reflected a trade-off between speed and accuracy with increased processing time required to maintain performance. Previous studies have reported inconsistent findings with regard to psychomotor speed (van Wingen et al., 2012).
It has been suggested that impairment of memory for emotionally neutral tasks may be explained by abnormalities in neurotransmitters responsible for symptoms of arousal (Vasterling et al., 1998). However, our findings do not support this with no correlation between PCL total or subscale hyperarousal scores and neuropsychological measures in either the PTSD or earthquake-exposed controls. This is similar to other studies which also reported that arousal symptoms did not correlate with neuropsychological measures in both PTSD and trauma-exposed controls (Flaks et al., 2014).
As described above, there has been increasing interest in examining the persisting brain effects of trauma exposure. Further comparison (in the supplementary analysis) with non-exposed control groups allowed examination of the impacts of exposure to earthquakes on neuropsychological functioning. We hypothesised that the earthquake-exposed controls would perform less well than the non-exposed controls in light of widespread reports in the media of ‘earthquake brain’ in the general population (Crowe, 2011). Our findings were consistent with this on tests of visuospatial (significant difference from the GMLT errors on delay task and approaching significance on GMLT errors from trials 1–4) but not verbal learning. Although the differences were only of the order of 0.5 of a standard deviation, and in a relatively specific area of functioning, their persistence over time suggests that functioning was impacted in those exposed to the earthquakes. It may be that the physical experiences in an earthquake of violent and repeated physical shaking and the ongoing post-earthquake environment with exposure to multiple aftershocks (over 10,000 in a 2-year period) may have particular or specific visuospatial impacts. It is also of note that because of extensive damage from the earthquakes, there were frequent road closures and the loss of landmark buildings throughout the city. A common experience reported widely in the media was that people found it very difficult to find their way around which may reflect the findings reported in this study combined with the demands of the post-earthquake environment and all these physical changes. Interestingly, it has also been suggested that cognitive biases in the processing of emotional information are associated more with performance on tasks of visual working memory than verbal tests (Dalgleish et al., 2003) and that non-verbal memory measures may serve as a proxy for emotional learning and processing (Wingo et al., 2010).
Only a small number of studies compare traumatised individuals without PTSD and healthy controls. One study reported similar findings to this study with women exposed to intimate partner violence (with and without PTSD), regardless of PTSD status having poorer performance on tasks of sustained auditory attention, working memory and response inhibition compared with non-exposed controls (Stein et al., 2002). However, two other studies of holocaust survivors and victims of domestic violence found no difference on a variety of neuropsychological tasks including tests of verbal memory between those exposed, but who did not have PTSD, and healthy controls (Chung et al., 2014). Lack of consistency in this research may be explained by the fact that these studies were heterogeneous in type, degree and duration of exposure, that is, including the holocaust (Golier et al., 2005) and exposure to domestic (Stein et al., 2002) or urban violence (Flaks et al., 2014).
Neuroimaging studies have been more consistent suggesting significant differences in brain functioning after exposure to trauma even in the absence of clinical symptoms of PTSD (Patel et al., 2012; Stark et al., 2015). Li et al. (2017) reported that earthquake-exposed individuals without PTSD compared with non-exposed controls had greater grey matter density in prefrontal–limbic brain systems, while soldiers exposed to combat who did not develop PTSD (and those never deployed) showed persistent reduction in functional connectivity between the midbrain and prefrontal cortex (van Wingen et al., 2012). It is possible that the visuospatial findings from our study in both earthquake-exposed groups (with or without PTSD) reflect similar changes to prefrontal–limbic brain regions or circuits.
Findings of this study also invite comment about the concept of resilience. Resilience has been defined in various ways (Wingo et al., 2010). For example, positive affect despite chronic exposure to stressful life events, the absence of PTSD following exposure to a potentially traumatic event and a high score on the CDRS. In this study, we asked people in the earthquake-exposed but resilient control group to self-identify as resilient which included aspects of all the above definitions. Their scores on the measures used supported this with higher scores on self-rated resilience and lower scores on all measures of clinical dysfunction despite experiencing equivalent stress to the PTSD group (from the TESS and LES). Although there has been evidence suggesting that higher intellectual capacity may moderate the risk of developing PTSD after trauma exposure (Gilbertson et al., 2006; Koenen et al., 2007; Parslow and Jorm, 2007; Vasterling et al., 2002), this study was not able to address this. The trauma-exposed but resilient controls did have higher education than the PTSD group, but it may be that more educated people volunteer to participate in studies of neuropsychological functioning.
This study has the following limitations. There was a difference in the time of testing between the two earthquake-exposed groups. However, both were more than 2 years from the beginning of the earthquake sequence, and it is unlikely that this would influence results. There were also some limitations associated with the groups; individuals in the PTSD group although presenting clinically with PTSD as the primary diagnosis had considerable comorbidity which limits what can be inferred as being related to a diagnosis of PTSD and in comparison with the PTSD group, the earthquake-exposed controls all self-identified as resilient and were older and more educated (and this in particular may have affected the findings). This was, however, adjusted for statistically. There were some limitations related to the assessment of exposure to other traumas in the two groups. Although we assessed exposure to life events over the preceding 6 months and 5 years (using the LES), we did not assess exposure to childhood trauma. It is therefore possible that the findings could be impacted by childhood trauma. A final issue is that of limited statistical power related to the size of the PTSD group. This may have resulted in type II errors in the comparison between the PTSD and control groups.
There are also some limitations associated specifically with the use of historical samples as the non-earthquake-exposed comparison groups. The decision to do this was based on recent reports describing symptoms and brain changes as a result of exposure to trauma per se which meant that comparison with a non-exposed control group would provide important information. It would not have been possible to access a non-earthquake-exposed group without going outside the region, due to the widespread impact of the disaster. Issues associated with the use of this additional comparison included some differences in the GMLT methodology with only four learning trials included in the non-exposed control groups (rather than five) which meant that only learning over the first four GMLT trials could be included in the comparison. It is possible that the earthquake-exposed groups had more learning and therefore a likely higher score on delayed recall because they were exposed to five trials. This limits the validity of the delayed recall comparison. However, this would have been expected to produce improved rather than poorer performance on this task, and therefore, the result is still of interest despite the limitation.
In conclusion, the key finding from this study was that no differences were found in verbal or visuospatial memory in individuals with PTSD compared with similarly earthquake-exposed controls. In comparison with non-exposed controls, both earthquake-exposed groups had poorer performance on tests of visuospatial, but not verbal memory. This offers preliminary evidence suggesting that it is earthquake (trauma) exposure itself, rather than the presence of PTSD that affects neuropsychological functioning. If replicated, the findings may have important implications for how information is communicated in a post-disaster context. Authorities would need to be aware of the impacts of exposure to earthquakes on peoples’ ability to process particularly visuospatial information, which may be particularly challenging in an environment where there is so much physical change. It would also be helpful for future studies to examine whether these deficits resolve over time as the stressors associated with living in a post-disaster environment improve.
Footnotes
Acknowledgements
The authors thank Wendy Mayes for administration of FER tasks and Andrea Bartram for data management.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was funded through grants to the first author (C.J.B.) from the University of Otago Research Committee.