
Abstract
There has been considerable literature on possible relationships between people with psychotic illnesses and the criminal justice system [1]. Any such associations are complex. There are a myriad of individual, environmental and illness variables that may contribute. This paper sets out to delineate some of these factors by comparing a group of people with psychosis held in custody in a remand centre with a group of people with psychosis who have not offended and were residing in the community.
Fazel and Danesh [2] have recently published a systematic review of the prevalence of serious mental illnesses in remand centers and prisons. This review is comprehensive and likely to inform service planning in the future. They report the use of nine instruments for the diagnosis of psychotic illness and major depression in detainees and gaols. We are unaware that any of these have had their psychometric properties validated in the forensic populations reported.
Teplin [3] and Arboleda-Florez [4] have commented on the effect of divergent research methodologies and instruments reported in primary research in this area. They suggest that many of the heterogeneities in prevalences reported may be the result of differential sampling methods. Studies have used raters from various professional backgrounds with infrequent mentions of reliability or validity of data. These issues may be obscured in the process of meta-analysis.
A major Australian (Victorian) epidemiologically informed sample is the case linkage study byWallace et al.[5]. This study found a significant proportion (25%) of those convicted of serious crimes had had contact with Public Mental Health Services. Men with schizophrenia and substance abuse were more than eight times more likely to have been convicted of violence than those without substance abuse. Valuri et al. [6] in another (Western Australian) case linkage study reported that 23.1% of those people on the WA Mental Health Information System also appeared on the Offenders Data base. Individuals with a drug and alcohol-related diagnosis (48.5%) and 32.5% of people with schizophrenia had had contact with the criminal justice system.
In further Australian and New Zealand studies Glaser [7] described 50 consecutive admissions to the psychiatric division in a metropolitan goal. Seventy-two per cent suffered from schizophrenic, affective or organic mental illness, 56% had chronic physical disabilities and 84% had had previous in-patient treatment in either hospital or prison or both. This study does not give any information about the presence of serious mental illness outside the referral group. Herrmann et al. [8] reported on sentenced prisoners in Melbourne's three metropolitan prisons. They found 3% had a current diagnosis of psychotic disorder and 23% were diagnosed as having a current mood disorder. A life-time diagnosis of at least one mental disorder was made for 82% of the responders. Sixty-nine per cent received life-time diagnoses of dependence on or abuse of alcohol or other psychoactive substances. The National Study of Psychiatric Morbidity in New Zealand Prisons (1999) [9] surveyed all New Zealand prisoners. The life-time prevalence of alcohol abuse and dependence was 69% in women and 76% in men, cannabis use 43% in women and 55% in men and ‘other’ illicit drugs was 40%.
This present study is important as it is the first to use a screening instrument validated for the purpose. In addition, it provides a greater depth of information about sociodemographic, disease characteristics and service utilization of men with psychotic disorders.
Methodology
At the time of survey the relevant remand centre had 466 cells andwas the main remand and reception centre for males for the southern region of the state of Queensland, Australia. The patients were consecutive remanded individuals examined as they entered the centre during the trial period. Management and security considerations ensure that from time to time remandees and other prisoners may come from other areas but these are rarities. These data are discussed in more detail below.
The Screening Instrument for Psychosis (PS) was developed in the context of the Australian Mental Health Survey: Study of Low Prevalence Disorders [10]. The instrument is useful in determining whether a person should be referred to a mental health professional for diagnostic evaluation and possible treatment and/or diversion. White and Chant have reported on the psychometric properties of the PS in a forensic setting elsewhere [11].
All prisoners entering the Centre receive a health examination. The PS was entered into the routine assessment documentation. It was administered by general trained nurses who had been instructed in its use. These nurses obtained informed consent from prisoners to use the results for research purposes and for further contact by researchers. The screen results were available throughout the day making it possible for research assistants to approach people who had answered yes to any one of the seven questions for more detailed interview. Those prisoners who screened positive using the PS were all interviewed by trained research staff using the Diagnostic Interview for Psychosis (DIP). As in other studies of this type no prisoners refused interview.
Results were compared with respondents who had a confirmed diagnosis of psychosis within in the Queensland arm of the Low Prevalence Study of the National Survey of Mental Health and Wellbeing. This provided an administratively convenient community comparison group. It meant that the same relevant mental health acts and criminal codes were applicable to both groups. This removed a possible systematic error that may have arisen if other groups derived from the above study had been used. The census in Queensland included Ipswich, Logan City, and part of the City of Brisbane. The catchment area covered a diverse range of localities including part of the densely populated inner city, urban, periurban and rural districts. All people who reported as having committed an offence within the previous 12 months and those currently in an inpatient unit were removed from the comparison set. The census identified 283 people in the community sample. After adjustment for the exclusion characteristics there were 102 people left.
Results
Six hundred and twenty-seven men entered the centre during the trial period. Six hundred and twenty-one remand prisoners were screened. Six men were not. Four remandees were returned from court to the watchhouse and were transferred directly to hospital and two others were transferred out of the remand centre before interviewers could contact them. Of the 621 screened, 65 answered yes to at least one question in the DP and were interviewed by the research assistant. Sixty-one complete sets of responses were obtained.
Prevalence
Following interview using by the DIP, 61 of the total potential sample of 627 remandees were identified as having a psychotic disorder. This gives a 1-month point prevalence of 9.5% for psychosis.
The observed remand and community rates within an item exceeds 80% (at a nominal 5% significance level) for almost all items whose actual significance level in case/control comparisons is below 1%, and exceeds 60% for items whose actual significance level is below 2%. Therefore, as can be seen by inspection of Table 1, the sample sizes at hand were sufficient to reliably detect rate differences of around 20% or more. Conversely, however, our sample sizes have power of approximately 20% for the detection of rate differences of approximately 10%, and thus it is possible that rate differences that have not achieved an actual significance level of 5%or lessmay still be associated with a genuine case/control effect, but we do not have enough data to identify it.
Summary of results of remand centre surveyed
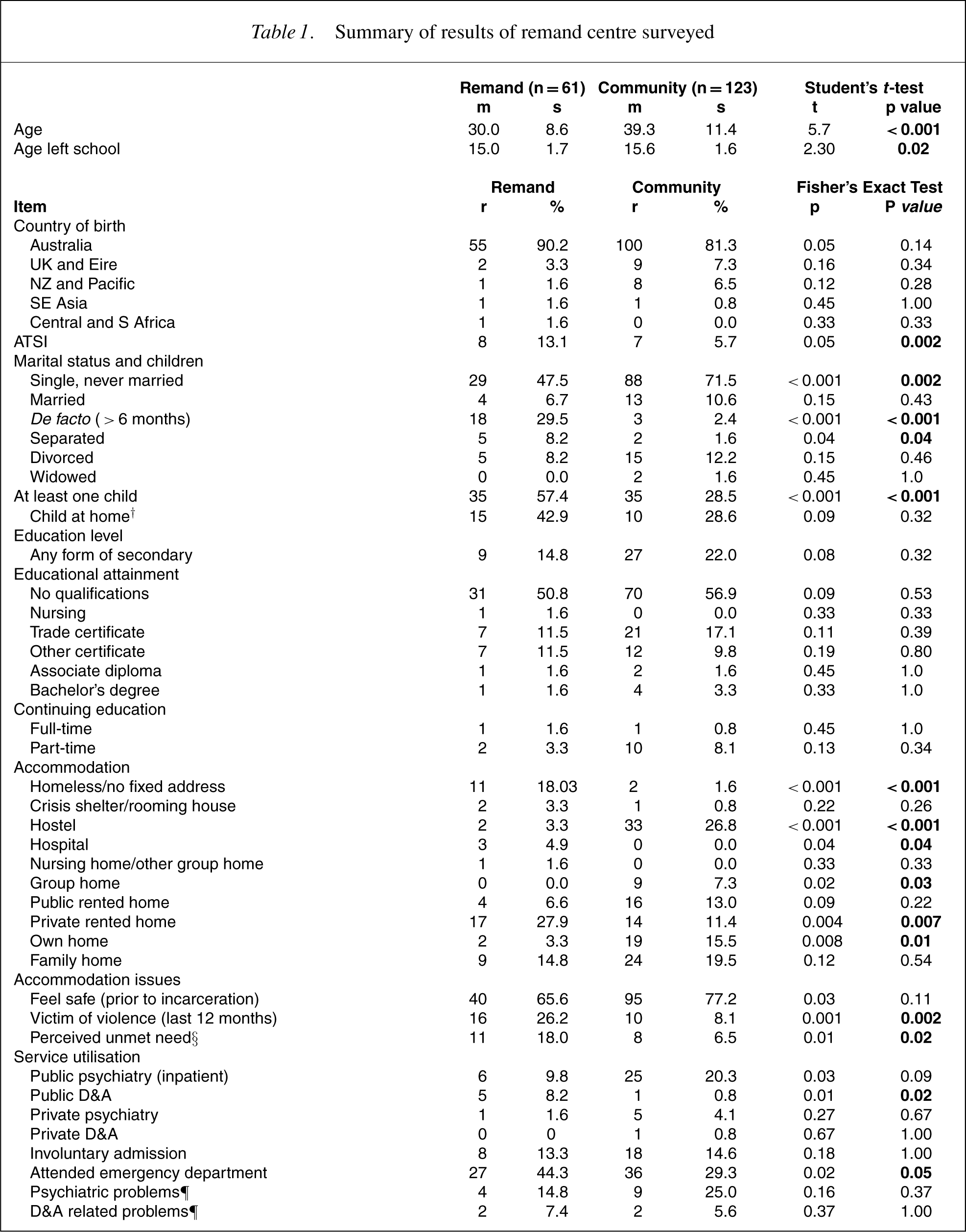
†Among persons with at least one child.
§For the police (last 12 months).
¶Among persons attending an emergency department.
Age
When compared to the Brisbane community sample of people with psychotic disorders (mean age 37.2 years, SD 10.15) prisoner sufferers (27.74 years, SD 7.32) are younger (t=5.66, p=0.0001).
Ethnic origin
The majority of the remandees, 55 (90.16%), was born in Australia. Others were born in the UK and Ireland (3.28%), New Zealand and the Pacific Islands (1.64%), South-East Asia (1.64%) and Central and Southern Africa (1.64%). Despite the overrepresentation of Aboriginal and Torres Strait Islanders in Australian correctional settings there was no significant difference in the number of people of Aboriginal and Torres Strait Islander heritage (8; 13.11%) and those in the community sample (4; 3.91%). These percentages are not significant because of the small sample size. They are no more likely to be of Indigenous descent (χ2 =0.08).
Marital Status and Children
There was no significant difference between the two groups in relation to marital status. In the remand group 29 men (47.54%) were described as single and never married; 4 (6.56%) were married; 18 (29.51%) were de facto (greater than 6 months); 5 (8.20%) were separated and 5 (8.20%) were divorced The remand population was more likely to have children (p=0.01]) see Table 1. Of those people who had children 15 (24.59%) of them had children living at home. Seven (20.59%) described themselves as being the main carer for these children in the past 12 months. Of those, seven were rated as having no dysfunction in parenting ability, two as obvious dysfunction and none as severe dysfunction.
Education
The mean age of leaving school was 14.55 years (ST 1.69). Only 9 (14.75%) had had any form of secondary school education. In terms of educational attainment 31 (50.82%) had left school with no qualifications. One person had a nursing qualification, 7 (11.48%) had a trade certificate, 7 (11.48%) had another form of certificate, 1 (1.64%) had an associate diploma and 1 (1.64%) had a bachelor's degree. One person (1.64%) described themselves as having been enrolled in informal studies in the past 12 months on a full-time basis and 2 (3.28%) on a part-time basis. There was no significant differences from the Queensland section of the Low Prevalence Disorder Servey.
Accommodation
The very high levels of homelessness found in the remand group compared to the community group probably relates to a complex representation where lack of shelter and dishabilition, or lack of social skills in the community are often merged into the concept of homelessness.
Service utilisation
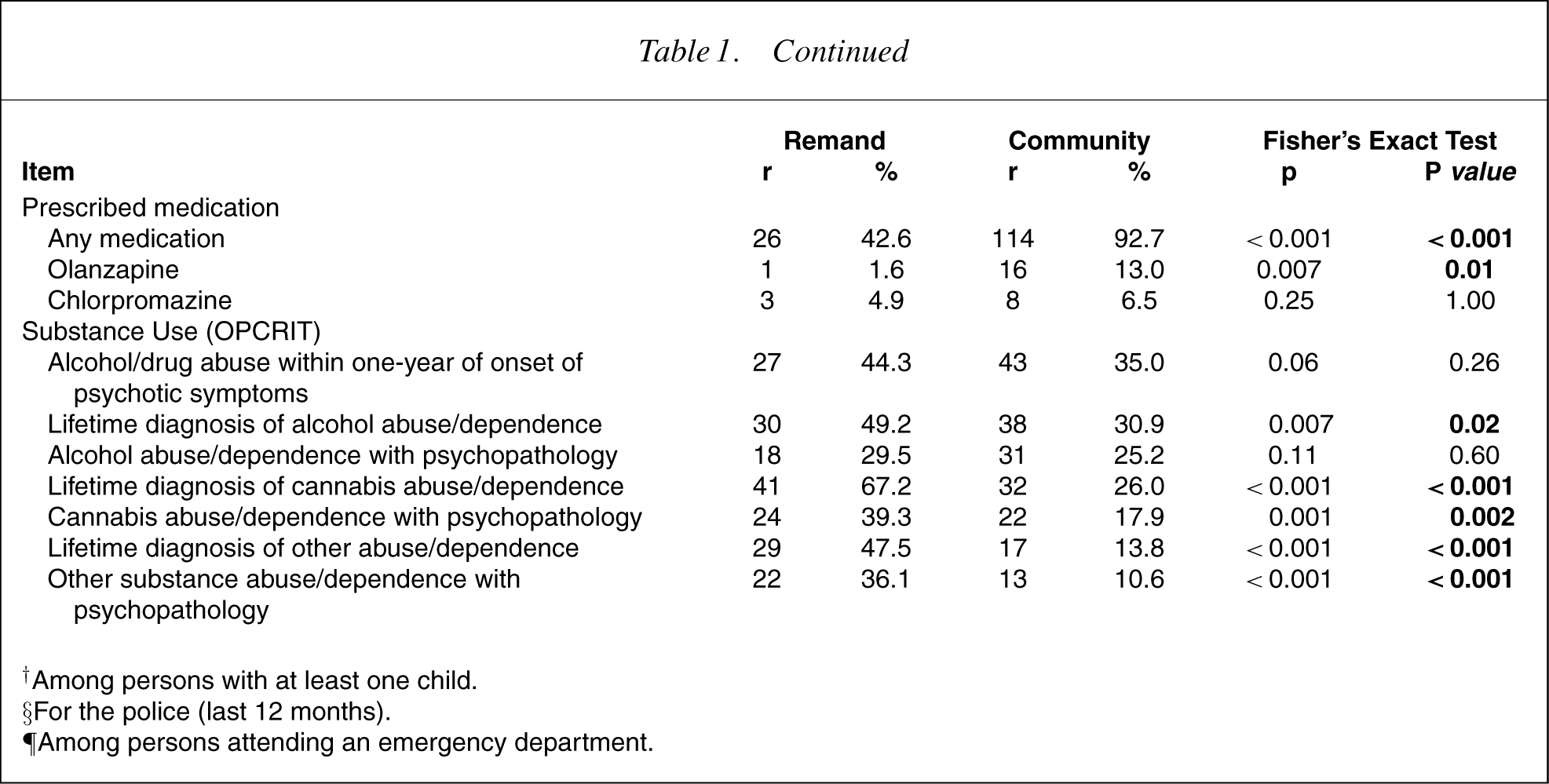
Eighteen (30%) of the remandees had been an inpatient of a public psychiatry hospital in the previous 12 months. In addition four had been in a public drug and alcohol hospital, one in a private psychiatry hospital, and three in a private drug and alcohol hospital. Eight people had been admitted involuntarily at least once. Only five people had had contact with a case manager from a mental health service. Twenty-one people attended an emergency department in the previous 12 months; four attended the emergency department for psychiatric problems and two for a drug and alcohol-related problem. The rest were for physical problems. Twenty-six remandees stated that they had taken a prescribed medication in the past month. One had had olanzapine, 3 took chlorpromazine, 20 took a benzodiazepine and the other 3 remandees ‘didn't know’.
Conclusions
A large group of seriously mentally ill people are held in custody in Queensland. They are marginalized, impoverished, and find it difficult to engage the health and social support systems. These findings are consistent with other prevalence surveys of similar populations overseas and suggest that the local Remand and Reception Centre is the largest acute mental health institution in the state.
The low number of indigenous Australians in the survey may be unexpected given their over-representation in the custodial system. However, Goulash et al. [12] have previously suggested that the screening instrument may not be a culturally sensitive method of identifying indigenous people with psychotic disorders.
The offender group had greater levels of substance abuse and or dependence. Brink et al. [13] in their group of prisoners concluded that compared with other prisoners on remand, prisoners on remand with substance misuse problems reportedmore childhood adversity, conduct disorder, self-harm, past psychiatric treatment and current mood disorder, and had fewer qualifications, were more likely to be unemployed and have more housing difficulties. Half of both groups were single, having never been married. This may speak to the considerable social disadvantages that face all individuals with major mental disorder. Patients with schizophrenia have been reported as more frequently being victims of crime and exploitation [14]. This was confirmed in this study. Impaired judgement disorganisation, frontal deficits, poor social supports, clustered social adversity (i.e. homelessness and unemployment) and physical ill health may contribute to this. Whatever the nature of the relationship, a large proportion of both groups, almost nine out of ten of the offenders and almost seven out of ten of the nonoffenderswere unemployed. Waghorn et al. have recently reported on persons with psychotic disorders in a representative Australian community sample of whom 75.2% were found to be non-participants in the labour market. Furthermore, the employment status of Australians with psychosis seems to be consistently associated with age, educational attainment, partner status, diagnostic category and course of illness. Premorbid work adjustment predicted aspects of employment status, whereas participation in public psychiatric rehabilitation, several symptom measures, and gender did not [15].
The original concept of “criminalisation of the mentally ill” suggested that mentally ill people may access health care and social support services with the criminal justice system. Nuttbrock et at. [16] have pointed out that the notion of convergences between mental disorder and criminal behaviour is non-trivial in nature and is inadequately explained in terms of social policy or demographic variables alone. The conceptual cartography of the complex nature and degree of this convergence is incomplete and requires further study. An extension of this hypothesis is that there has been a ‘transinstitutionalization’ from mental health care into custodial care as a result of the move to community care of the seriously mentally ill [17]. Further informationmaybe extrapolated from the prevalence studies of remandees and prisoners over the last century. Despite their separation geographically, temporarlly and the disparate diagnostic and research methodologies, there is broad evidence that there has always been a large number of seriously mentally ill people contained in custodial institutions. There appears to be little evidence for the position that ‘jails have become a repository for the seriously mentally ill’ proposed by Teplin [18].
Herrman et al. [19] found that 41% of their sample of homeless men in Melbourne received a lifetime diagnosis of psychotic disorder and 24% a current diagnosis. They highlight the historical precedent in the campaign for asylums in the 19th century when many mentally ill people were housed in jails. Zapf et al. [20] found a significant relationship was between homelessness and severe mental disorder in a group of men on remand. There were no significant differences found between the homeless and the non-homeless on the types of crimes for which they were incarcerated or in contact with health care services within the past year. Sullivan et al. [21] showed that homeless persons share childhood histories of economic and social disadvantage. Those mentally ill people who become homeless after becoming ill have an especially high prevalence of alcohol dependence. They concluded that mental illness may play a role in initiating homelessness for some, but is unlikely in and of itself to be a sufficient risk factor for homelessness. Zitrin et al.[22] report that psychotic thinking among homeless persons may be a significant factor in reducing access to and maintenance of government entitlements. They argue that in the context of an increasingly restrictive and bureaucratic welfare system, providing assistance to homeless people who have severe psychopathology presents new challenges to service providers.
Homelessness is a historically specific phenomenon that also affects people who are not mentally ill. It should not be used to justify the removal of the mentally ill from community settings on a long-term basis. Those mentally ill people on remand present a group of persons with a complex array of problems. The simplistic “prison, hospital or community treatment” debate should consider the development of flexible preventative, management and accommodation services for people with severe mental disorder [8].