
Abstract
Depression is the leading cause of disability [1,2], and is second only to hypertension as the most common chronic condition seen in general practice [3]. Professional helpseeking is an important aspect of treatment, with GPs providing more than three-quarters of mental health services in the Australian community [4]. Although there is strong evidence supporting pharmacological and psychosocial treatments for depression [5], studies using community samples suggest that the lay public is often unaware of the benefits associated with these forms of treatment [6].
In addition to seeking professional help, individuals employ a diverse range of self-help and complementary help-seeking strategies to cope with symptoms of anxiety and depression. This includes relaxation therapy, taking vitamins and engaging in regular exercise [7]. Although two-thirds of patients visiting a conventional mental health provider report the concurrent use of complementary therapies [8], fewer than 40% disclose this to their doctor [9]. Thus it is important to acknowledge and understand the range of measures that individuals use to cope with depression, both to maximize their benefit and understand the process by which patients deal with their disorder [10].
To date, much of the research in this area has been carried out in community samples [11]. This paper focused on the coping strategies used by those who had a diagnosis of depression and who were attending a specialized mood disorders unit for further assistance with managing their illness. We specifically sought to examine what strategies patients used in an effort to alleviate their symptoms, and further, to investigate the helpfulness of each of these strategies. Sociodemographic and illness-related differences were examined with reference to each of these research questions.
Material and methods
Sample
A sample of 239 consecutive attendees was referred by general practitioners and psychiatrists for diagnostic and management advice for a depressive disorder to the tertiary referral Mood Disorders Unit (MDU) at a Sydney teaching hospital. The study group consisted of 176 outpatients (74 male, 102 female) aged 16–82 years (M=42.9, SD=14.4 years) who fitted the diagnostic criteria for a primary DSMIV depressive disorder and had complete data for the questions relevant to the current study. Written informed consent was obtained from all participants.
Clinical assessment and measures
Data were collected (from July 2001 to February 2004) from questionnaires completed by the patients prior to the consultation, and from patient interviews conducted by research assistants and consultant psychiatrists. The patients underwent a comprehensive assessment detailed elsewhere [12]. The structured interview assessed DSM-IV lifetime diagnoses of depressive episodes and anxiety disorders using the computerised Composite InternationalDiagnostic Interview(CIDI), version 2.1 [13]. More complex clinical features of the current depressive episode, including DSM-IV assignment of melancholia or non-melancholia, were measured by the administration of the 21-item Hamilton Rating Scale [14] and the 18-item CORE instrument [15].
Patients completed self-rating scales in a series of questionnaires developed by the MDU. These questionnaires assessed sociodemographic information, current and past psychiatric history, and coping strategies employed by the patient during times of depression. Participants indicated what strategies they had used from a list of 21 items and were also given the option to specify any other methods they had used if these were not included in the original list. Patients rated whether such strategies were helpful on a dichotomous scale (helpful/not helpful). The items included in this questionnaire had been modelled from previous studies [7] and modified to suit the current sample.
Statistical analyses
Multiple logistic regression analyses were carried out to determine if the predictor variables of gender, age, lifetime history of anxiety, the presence of melancholic depression and repeated episodes of major depression were associated with (i) the use of specific actions to alleviate depression and (ii) the perceived helpfulness of these actions.
Results
Of the 176 who participated in the study, all had a diagnosis of DSM-IV major depression, 74% of the sample (n=131) had experienced a least one previous episode prior to attending to MDU, and 73% (n=129) had at least one DSM-IV anxiety disorder in their lifetime. Thirty per cent of the sample (n=53) had clinical features qualifying for a diagnosis of melancholic depression, whereas the remainder were diagnosed with non-melancholic depressive subtype (n=123).
Strategies used to assist with depression
The strategies used to assist with depression are ranked in order of reported frequency (Table 1). As expected in a sample referred to the MDU by GPs or psychiatrists, the use of antidepressants was very high (98%). Other frequently cited strategies used for coping with depression included talking to family (84%), reading about the problem (82%) and learning relaxation (64%). Although most of these strategies were common in both sexes, women were more than twice as likely to have visited a naturopath.
Predictors of employing actions to cope with depression: odds ratios (with 95% CIs) using multiple logistic regression analyses

p< 0.05; ∗∗ p< 0.01; ∗∗ p<0.001; bold font represents significant values.
Age, history of MD or anxiety and depression subtype also predicted the actions patients took to cope with depression. An increase in agewas associated with a decrease in communication with friends, taking less time off work, and being less likely to use alcohol to cope. Drinking was twice as common among those with recurrent episodes of depression. In terms of depression subtypes, those with melancholic depression had higher rates of hospitalisation and non-melancholics smoked more to assist in reducing their symptoms. Patients with a history of anxiety disorders were more likely to have consulted a GP or psychologist, have a massage or use alcohol to alleviate their depression compared to those without a history of anxiety disorders.
Strategies perceived as helpful for depression
The three most helpful activities (reported in Table 2) were seeing a psychiatrist (67%), taking antidepressants (63%) and consulting a psychologist (60%). Women were more likely to report actions relating to professional help-seeking as helpful, including being admitted to hospital, consulting a psychiatrist and receiving counselling. Younger people were more likely to report counselling and learning relaxation techniques as helpful. Thosewith a diagnosis of melancholic depression reported drinking alcohol as more helpful. Due to the small number of patients completing the item ‘special diet’, this was not analysed in a logistic regression.
Predictors of the helpfulness of actions to cope with depression: odds ratios (with 95% CIs) using multiple logistic regression analyses
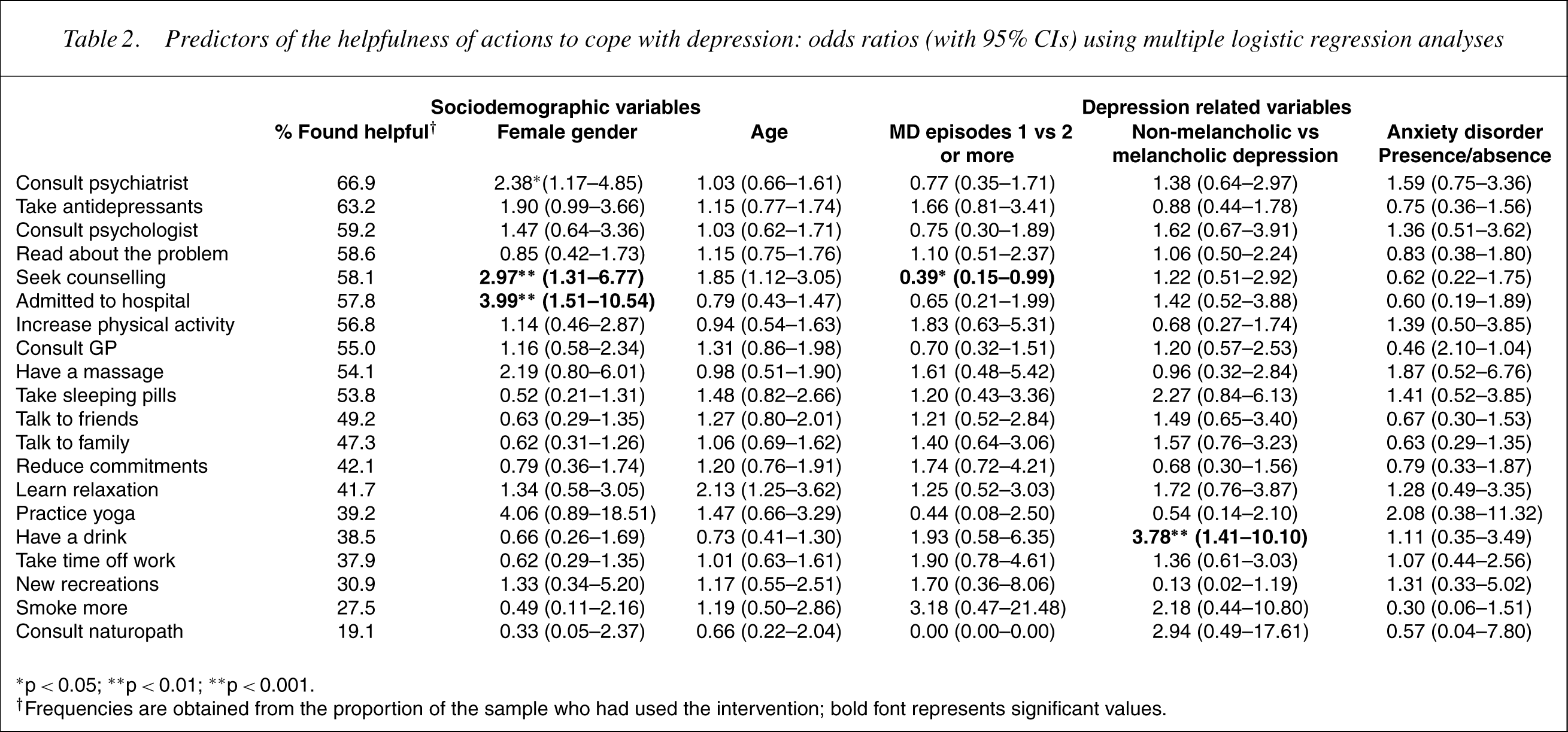
∗ p< 0.05; ∗∗ p< 0.01; ∗∗ p< 0.001.
† Frequencies are obtained from the proportion of the sample who had used the intervention; bold font represents significant values.
Discussion
The rates of use of complementary interventions reported in this study are relatively high in comparison to earlier reports taken from the general population [16]. This is interesting given that virtually all participants had been prescribed an antidepressant and were attending the MDU, implying high acceptance of standard professional treatments. Practitioners should, therefore, recognise that their patients are likely to have tried at least one form of complementary therapy, even if this is not disclosed during treatment [17].
Differences relating to sociodemographic and illnessrelated characteristics were frequently recorded. In particular, younger patientsmore frequently talked to friends and took time off work, and ‘had a drink’ to cope with their depression. A history of anxiety disorder was a major determinant of the types of strategies used, both in terms of clinical actions (consulting aGP or psychologist) and complementary actions (such as having a massage). Those with anxiety disorders and with repeated depressive episodes used alcohol to cope with their depression, while patients with non-melancholic depression were more likely to smoke than their melancholic counterparts. These results highlight the need for clinicians to enquire about substance use and, furthermore, encourage individuals with a depression and/or smoking history not to recommence the habit when depressed as it is likely to exacerbate their problems and impair their ability to overcome depression [18,19].
Being female was the most significant predictor of perceived benefits of particular interventions. Females found consulting a psychiatrist or counsellor and being admitted to hospital to be more helpful than males. A previous study using a similar sample of 98 men and 172 women from the MDUreported that whereas men andwomen had very similar experiences of depression (when examined for duration, depression type and severity prior to treatment), their repertoires for dealing with depression significantly differed [12]. These findings support previous literature indicating that gender is a major determinant of professional help-seeking rather than actual depressive experience [7,20,21].
Few differences were recorded for the helpfulness of interventions between groups based on the number of previous episodes, on the type of depression experience, or whether patients had experienced an anxiety disorder. Complementary medicines were just as frequently used and found to be as helpful as the clinical interventions. These results may be due to the changing profile of complementary medicine, with activities such as yoga now being used more commonly in the general community. Increasing physical activity was also popular, with over half the patients indicating they had tried this to reduce their depression. Although there were no differences in exercise usage or perceived helpfulness between those with melancholic and non-melancholic depression, it is plausible that the mechanisms of how exercise helps may differ. Those with melancholic depression may find that it gives relief from lethargy, whereas those with nonmelancholic depression may find that it assists in reducing emotional dysregulation. While the positive effects of exercise on depression have been shown in a number of reviews [22], the quality of the studies does not allow researchers to conclude whether the benefits are direct or indirect (e.g. through increasing social interactions) [23].
Although the majority of patients had talked to family and friends about their depression, less than half had found it helpful. This is in contrast to receiving information through reading, a strategy thatwas used and found to be helpful to patients regardless of gender, age or depression experience. Reading about themental illness is likely to encourage patients to consider more treatment options [6] and providing information has been linked to an increase in help-seeking behaviour [6,24,25]. Although we are mindful of the need to consider the characteristics of the depressive episode [26], education may be of particular value for those with non-melancholic depression and with significant anxiety. These results also highlight the importance of making information available to those whomthe depressed person is likely to turn, as individuals with good social support are more likely to seek professional help for mental problems [27], which further point toward the importance of a supportive informed social network.
Although this paper is limited in that these results are highly specific to those seeking specialist care, there are several important ‘take home’ messages from this paper. Professional intervention remains a fundamental part of treating depression, yet self-help and complementary therapies are used and perceived to be just as helpful as orthodox treatments by many patients. Although this paper is not intended to provide recommendations of treatment, it should be beneficial among professionals for appreciating the use and helpfulness of a range of coping strategies. This should potentially complement and enhance patients’ prescribed treatment regime, as well as assist their significant others in providing helpful advice and encouragement as well as more general social support.
Footnotes
Acknowledgements
The work is supported by NHMRC Program Grant 222708 and by an Infrastructure Grant from the Centre for Mental Health, NSW Department of Health.