
Abstract
Studies conducted in various parts of the world indicate that postnatal depression (PND), predominantly major and minor unipolar depression, is the most common mental disorder associated with childbirth and is a significant health issue [1, 2]. Rates from well-designed cross-sectional and prospective studies typically range from 12% to 16% during the first 6 to 12 weeks postpartum [1–3]. They are usually somewhat lower when assessment is based on psychiatric diagnostic interviews than when screening instruments are used. Previous New Zealand studies using the Edinburgh Postnatal Depression Scale (EPDS) obtained estimates of 8% and 13% [4, 5].
Postnatal depression is an important health issue because of its adverse impacts on the wellbeing of mothers [1], spouses/partners [6], spouse/partner relationships [7, 8] and children [1]. Maternal depression has significant negative effects on early mother–infant interaction [9] and disturbs child cognitive, emotional and behavioural development [10–13]. Recent studies indicate that these disturbances to child development can be of long duration and appear to be most evident in boys and disadvantaged groups [14–16]. Women with PND also have an elevated risk for recurrent depression during subsequent pregnancies and at other times [17].
Although there are readily administered, validated tools to assess PND and effective treatments available, routine screening is not common and PND often persists undiagnosed and untreated [18, 19].
Factors consistently associated with the development of PND include prior history of depression, depression during pregnancy, marital/partner relationship problems, lack of support from partner or significant others, or both and recent stressful life events, including bereavement, housing problems and unemployment [1, 2, 20]. Many other risk factors have been identified less consistently.
Previous New Zealand studies [4, 5], consistent with the international literature, found that past psychiatric disorder, antenatal depression, poor partner relationships and single parenthood are significant risk factors. Maori ethnicity, age less than 20 years at the birth of first child, lower educational qualifications and low income were also associated with higher prevalence. A recent prospective Australian survey of urban and rural women obtained broadly similar results [21].
Most research, contrary to the findings of the New Zealand studies [4, 5], has found little or no relationship between PND and socioeconomic status measured variably as individual or household income, education level and occupational status [1–3]. Hagen [22] maintains that this failure to establish a link between socioeconomic status and depression is an artefact of study samples that are typically middle class and lacking in variability. This view is supported by the finding of high rates of depression in the few studies that have examined financially impoverished and disadvantaged communities in Western countries [23–25]. Furthermore, while broad indices of socioeconomic status are not usually found to be significant risk factors, other measures typically strongly associated with low socioeconomic status are. These factors include single motherhood, unemployment and receiving a pension/benefit [1, 2, 20, 21].
Ethnicity, cultural issues and migration have received some consideration in PND research. Abbott [26], Stern and Kruckman [27] and Miller [28] propose that PND is a culture-bound syndrome peculiar to Western societies and associated with a lack of rituals and supportive cultural practices surrounding childbirth. Others maintain that the medicalization of childbirth, including the expansion of obstetrics and high levels of technological intervention during the birth process, gives rise to postnatal distress and depression [29–31].
While most PND research has been undertaken in North America, Europe and Australia, studies have been conducted in non-Western countries too. There are also some comparative studies between countries. Reviewers of relevant international literature conclude that there is little support for the notion that PND is largely a product of Western societies [1,32–35]. Contrary to the culture-bound hypothesis, prevalence rates in non-Western cultures and developing countries are usually comparable to or higher than in Western countries. For example, Affonso et al. [35] obtained significantly higher rates of depressive symptoms in samples from Asian countries and Guyana than from Europe and Australia. However, there are some contradictory findings, including very low prevalence estimates from Japanese [36] and Malaysian [37] surveys. Although these estimates are low relative to the great majority of PND studies reported in the literature, similarly low rates have been obtained from surveys in Sweden [38] and the Netherlands [39].
A recent UK study found higher PND prevalence rates among Asians than Caucasians, leading the authors to propose that women from ethnic minorities may be at greater risk than those of the majority ethnic group [40]. Reference has been made to an Auckland study that found Maori ethnicity to be a risk factor [4]. However, comparative studies within multiethnic societies have generally found little difference between ethnic groups [1]. This said, there have been relatively few studies of this type and no country appears to have anything approaching a comprehensive epidemiological overview of the postnatal maternal mental health of its major ethnic groups.
The assessment and comparative study of PND in ethnic minorities is a challenging undertaking for a variety of reasons. Although apparently not a culture-bound disorder confined to particular societies, the expression of postnatal depressive symptoms varies somewhat in different cultural contexts [32, 33]. This variation, combined with the related challenge of establishing equivalence when measures are translated into other languages, means caution is required when comparing prevalence across cultural groups.
Ethnic minorities also vary in ways other than ethnicity that impact on mental health status. For example, relative to members of majority ethnic populations, ethnic minorities are often of lower socioeconomic status and experience higher exposure to various mental health risk factors. They are also more likely to be migrants. There is a substantial body of research examining relationships between migration, acculturation and mental health, albeit that little of this research specifically addresses PND [41]. While migrants per se do not necessarily have elevated rates of mental disorder, including PND, some subgroups are at particularly high risk.
With respect to acculturation, it has been asserted that migrant and indigenous minorities that retain aspects of their original cultural identity while acquiring significant aspects of their adoptive culture generally experience a more positive adaptation than those who adopt alternative strategies [42, 43]. Other strategies include assimilation and relinquishing of identity and traditional cultural practices or rejecting new cultural practices and either living primarily in a subcultural enclave or becoming socially isolated. Relationships between acculturation and PND do not appear to have been explicitly examined to date.
While risk factors for PND are fairly similar across cultures [1, 2, 20], the meaning and significance of particular factors may vary. For example, Stuchbery et al. [44] found that low social support was associated with PND in Arab, European and Vietnamese mothers. While social support was implicated in the three groups, the source and type of support varied. These differences appear to arise from varying cultural expectations with regard to marital relationships and social support.
The Pacific population is a demographically young and rapidly growing population sector in New Zealand, particularly in Auckland [45]. At the time of the 2001 census, 231 801 Pacific people were resident in New Zealand, 6.5% of the total population. Relative to the general population, Pacific people experience lower socioeconomic status, poorer health and lower life expectancy [46]. A previous qualitative investigation involving interviews and discussion groups with 48 Pacific Island women and 13 health workers identified PND as a concern within Pacific communities that was important to family health and wellbeing [47]. The authors concluded that Pacific women are likely to be at a high risk for PND but suggested that risk factors identified in Western populations might not apply to them, and concluded that traditional family and cultural supports, affordable childcare and antenatal education are probably important protective factors.
The purpose of the present study was to assess the prevalence of and risk factors for PND symptoms in a cohort of Pacific mothers resident in Auckland, New Zealand.
Method
Data were collected as part of the Pacific Island Families (PIF): First Two Years of Life Study. The PIF Study is a prospective investigation of a cohort of 1398 infants born at Middlemore Hospital, South Auckland, during the year 2000 and their parents. This hospital was selected as the recruitment site for the cohort because it has the largest number of Pacific births in New Zealand and is representative of major Pacific ethnicities. All potential child participants were selected from live births at Middlemore Hospital, where the child had at least one parent who identified as being of Pacific Island ethnicity and was also a New Zealand permanent resident.
Approximately 6 weeks after the birth of their child, Pacific interviewers visited mothers in their homes. Once eligibility criteria were established and informed consent gained, mothers participated in 1-hour interviews concerning the health and development of the child and family functioning. This interview was conducted in the preferred language of the mother by a female interviewer fluent in that language. Usually, and always where requested, interviewers were of the same ethnicity as interviewees. All procedures and interview protocols had ethical approval from the National Ethics Committee. Detailed information about the cohort, procedures used, and interview protocols is presented elsewhere [48].
The EPDS was included in the 6-week assessment. The EPDS is a self-report instrument that focuses on cognitive and affective aspects of depression rather than somatic symptoms. In the present study, the instrument was administered as an interview. The scale does not provide a clinical diagnosis of depression, but a score above 12 is widely used to indicate the presence of probable depressive disorder. Although its reliability and validity has been established in a variety of populations and settings [1, 49, 50] and it has been used in previous New Zealand studies [4, 5], its use with Pacific Island mothers is limited [47]. For the present study, the EPDS was translated into relevant Pacific languages and back-translated into English by different investigators fluent in both a Pacific language and English.
Following the interviews, data were coded and double-entered into an electronic database (SPSS Data Entry Builder 2.0) that employed comprehensive data validation and checking rules.
Statistical analysis
Analyses were undertaken using the statistical software package SPSS for MSWindows (12.0.1) with the level of significance set at the 95% confidence interval. Univariate and multivariate logistic regression procedures were employed to assess relationships between predictor variables and probable depressive disorder.
Results
Response rate
Ninety-six percent (N=1590) of potentially eligible mothers of Pacific infants who had been born between 15 March and 17 December 2000 gave consent to be visited in their homes when the infant was 6 weeks old. Of the 1477 mothers contacted and who met the eligibility criteria, 1376 (93.2%) agreed to participate in the PIF Study. A more conservative recruitment rate of 87.1% would include mothers who consented to contact and were (a) confirmed eligible or (b) of indeterminable eligibility due to inability to trace. Of the 1368 biological mothers, 1363 (99.6%) completed all questions of the EPDS and were included in the analyses reported.
Sociodemographic characteristics
Just under one-half (47.4%) of the 1360 mothers self-identified their major ethnic group as Samoan, 20.9% as Tongan, 16.7% as Cook Islands Maori, 4.3% as Niuean, 3.4% as Other Pacific (includes mothers identifying equally with two or more Pacific groups, equally with Pacific and non-Pacific groups, or with Pacific groups other than Samoan, Tongan, Cook Island Maori or Niuean), and 7.3% as non-Pacific. The mean (SD) age of the mothers was 27.8 (6.1) years, 80.5% were married or in de facto partnerships, 33.1% were New Zealand– born and 27.5% had post-school qualifications. Just over one-quarter (27.7%) of the mothers were primipara.
EDPS reliability and prevalence
The reliability coefficient (Chronbach's α) of the EPDS for all women in the study was 0.86. Corresponding values for the individual ethnic groups were as follows: Samoan, 0.87; Tongan, 0.77; Cook Island Maori, 0.82; Niuean, 0.83; Other Pacific, 0.84; non–Pacific Island, 0.85.
The mean (SD) EPDS score was 6.84 (5.42) and the number of mothers with probable depression (EDPS score 13 or higher) was 224 (16.4%).
Risk factors for PND
Of 30 variables examined by univariate logistic regression procedures for associations with probable depression, 18 reached significance. Results for these 18 significant variables are presented in Table 1. For the categories within each variable the numbers and percentages of mothers exhibiting probable depressive disorder, along with the associated odds ratios, are shown. Variables (maternal unless stated) examined but failing to reach significance were age, education, whether born in New Zealand, length of time lived in New Zealand, parity, whether attended antenatal classes, childcare activities score (modified CCAS scale [51]), partner's childcare activities score (modified CCAS scale), delivery method of infant; gender of infant, birth weight of infant, whether mother had regular childcare arrangements.
Numbers (row percentages) and univariate odds ratios of probable depression (EPDS > 12) by selected variables
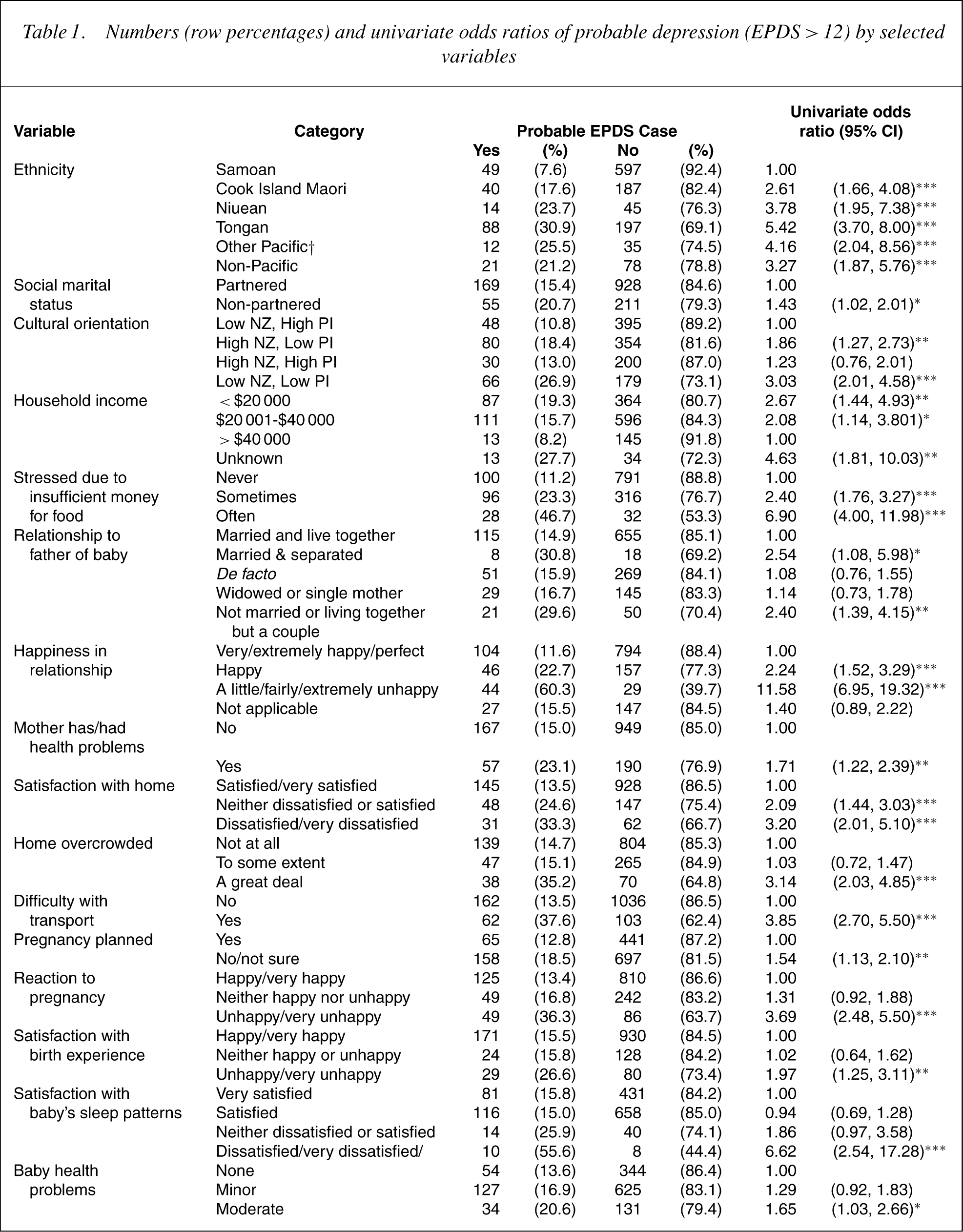
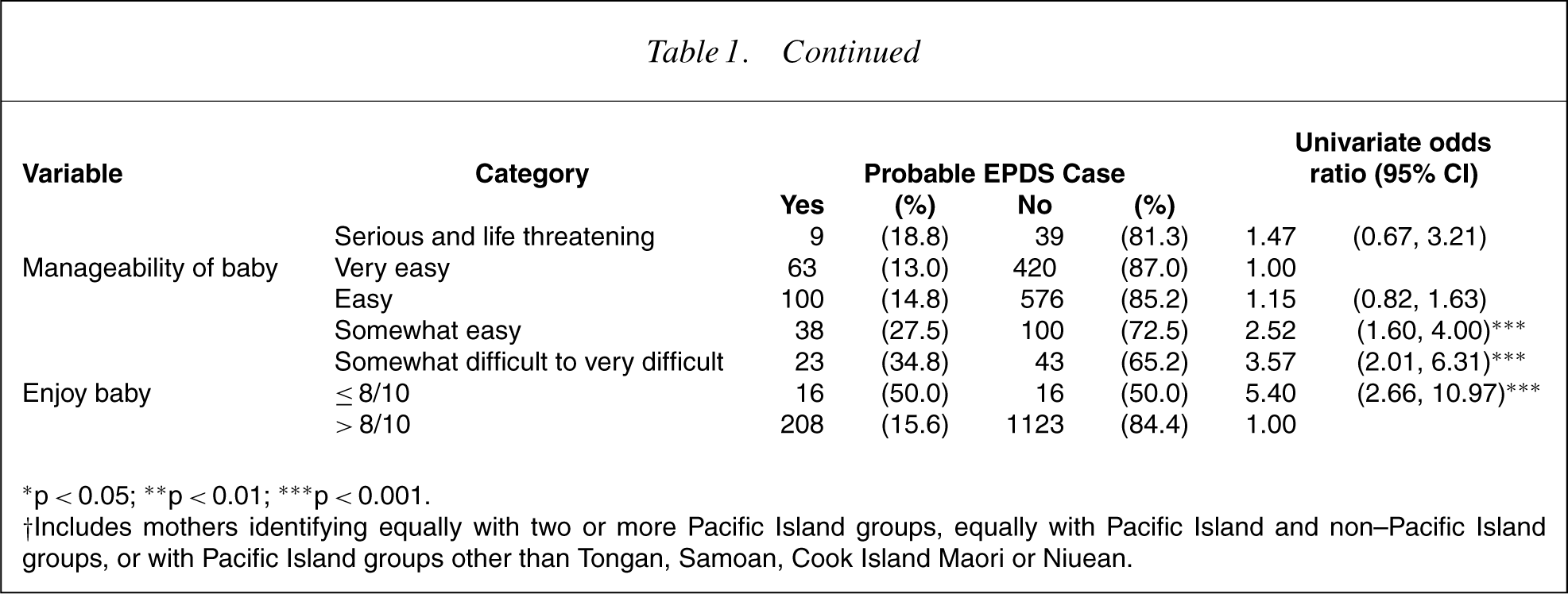
∗ p < 0.05; ∗∗ p < 0.01; ∗∗∗ p < 0.001.
†Includes mothers identifying equally with two or more Pacific Island groups, equally with Pacific Island and non–Pacific Island groups, or with Pacific Island groups other than Tongan, Samoan, Cook Island Maori or Niuean.
Because many of the independent variables examined in the univariate analyses are associated with one another, a stepwise multiple logistic regression analysis was undertaken to enable the estimation of odds ratios at each level of a predictor variable when adjusted for other variables in the model. In this analysis 5 of the 30 variables examined in the univariate logistic regressions were initially forced into a multivariate model as control variables, namely mother's age, education, ethnicity, social marital status and household income. The remaining variables were then assessed for inclusion, with p to enter set at 0.15 and p to remove at 0.20. Eleven variables reached significance in the multivariate model and these variables along with their adjusted odds ratios and associated confidence intervals are shown in Table 2. While 10 of these variables had exhibited significant associations with probable depression in the univariate analyses, maternal parity also attained significance when the effects of other variables (being stressed owing to insufficient money to buy food in particular) were controlled for in the multivariate model. Variables included in the final model but not reaching significance were age, education and social marital status, three of the five variables forced into the model as control variables.
Adjusted odds ratios of probable depression (EPDS>12) for variables attaining significance in a multiple logistic regression (N = 1285)†
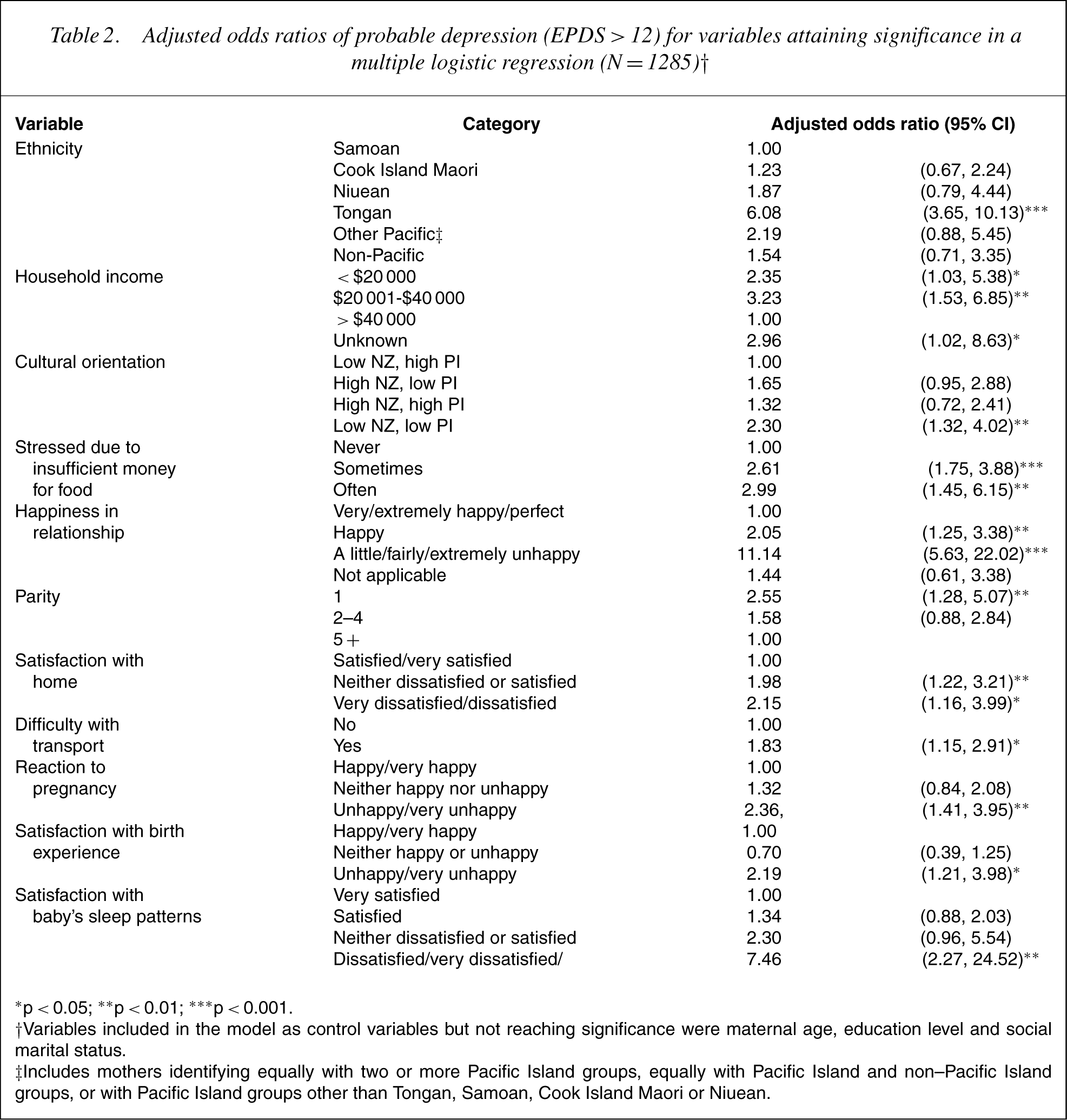
∗ p < 0.05; ∗∗ p < 0.01; ∗∗∗ p < 0.001.
†Variables included in the model as control variables but not reaching significance were maternal age, education level and social marital status.
‡Includes mothers identifying equally with two or more Pacific Island groups, equally with Pacific Island and non–Pacific Island groups, or with Pacific Island groups other than Tongan, Samoan, Cook Island Maori or Niuean.
Although ethnicity remained a significant risk factor in the multivariate analysis, the odds ratios for the different groups changed appreciably when the effects of other variables were taken into account. This is illustrated in Figure 1.
Univariate and adjusted odds ratios of probable depression (EDPS < 12) by ethnicity.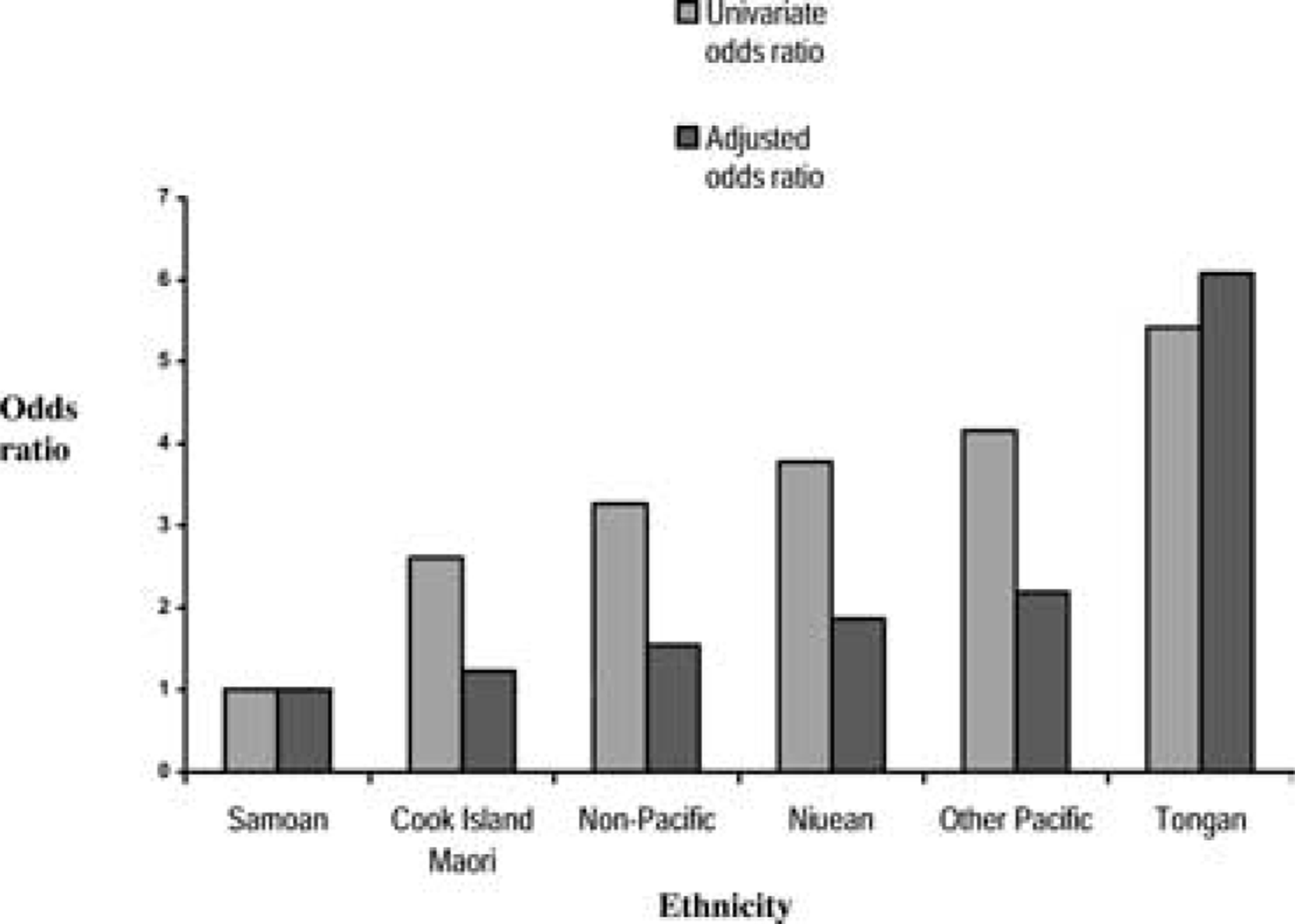
Discussion
This is the first study to assess the prevalence of postpartum depressive symptoms in a large cohort of Pacific women. The probable PND estimate of 16.4% is at the high end of the range typical of surveys conducted internationally and somewhat higher than rates from earlier Auckland (8%) and Christchurch (13%) studies [4, 5]. In the Auckland study, Maoris had elevated prevalence, in large part due to lower education and income levels, younger age at the time of first birth, and higher rates of sole parenthood—all identified as risk factors in that study [4]. Although the overall estimate of 16.4% is not particularly atypical, it is important to note the substantial differences between the different Pacific Island ethnic groups as well as some other subgroups at very high risk.
The Auckland survey of Webster et al. [4] included some Pacific Island women but reported that language difficulties compromised assessment of depression. Lealaiauloto and Bridgman [47] also mentioned assessment problems and questioned the cultural appropriateness of the EPDS. They suggested that the screen fails to detect some aspects of postpartum distress in Pacific Island mothers and that it might generate conservative prevalence estimates. In the present study, Pacific interviewers did not report administration problems, and the internal consistency of the EPDS was high overall as well as for specific ethnic groups. None of the individual items appeared to be problematic. While this suggests the EPDS is valid in the present context, further investigation of its formal psychometric properties, including predictive and construct validity, is warranted.
A number of the risk factors identified are consistent with those of previous research. As in past studies that included significant numbers of participants of low socioeconomic status, a number of indices of privation, including low household income, stress due to insufficient money for food, transport difficulties and dissatisfaction with home, predicted PND symptoms. Overcrowding was an additional factor in the univariate analyses but failed to reach significance in multivariate analyses. These and related stressors have been associated with a wide variety of mental and physical health problems additional to PND [52].
The strongest risk factor was dissatisfaction with partner or spouse relationship. In both univariate and multivariate analyses, mothers indicating unhappiness were many times more likely to experience depressive symptoms than those who were happy or were not in a relationship. Mothers who were single or had separated from the baby's father were also at somewhat higher risk than those who were living with the father, although this relationship was not sustained in the multivariate analyses. Contrary to expectation, although relationship satisfaction was important, childcare support from partners and access to other regular childcare arrangements was not associated with probable PND. Neither was attendance at antenatal classes.
A number of factors related to pregnancy, birth, and the baby's health and behaviour also predicted probable PND. Those holding up in the multivariate analyses included mother's satisfaction with learning of her pregnancy, her birth experience and the baby's sleep patterns. These and similar factors have been identified in previous investigations. These studies have been less consistent with respect to parity and obstetric intervention. Degree of obstetric intervention or the delivery method was not associated with PND in the present study. Firsttime motherhood was identified as a risk factor in the multiple logistic regression when controlling for with a variety of other risk factors.
Ethnicity and acculturation variables constitute another and final major grouping of risk factors. Perhaps the most significant finding of the study was the large variation in probable PND prevalence estimates between Pacific Island ethnic groups, ranging from 7.6% for Samoans to 30.9% for Tongans. The former is among the lowest estimates internationally, the latter among the highest. While there is cultural variation between the Pacific Island groups included in the study, there are many similarities in their background, acculturation and social situation in New Zealand. For these and other reasons differences of this magnitude were not anticipated.
At the outset it was expected that prevalence differences between ethnic groups, if present, would be largely explained by differential exposure to other risk factors. This was the case for most groups, with odds ratios reducing and converging when the effects of other risk factors were taken into account in multivariate analyses. However, for Tongans, the odds ratio increased and the gap widened between this and all other groups. This means that factors associated with being Tongan, other than those identified in this study, account for the Tongan's very high prevalence of PND symptoms. It cannot be concluded from the present analyses what they are. It is important that further consideration is given to the identification of factors associated with being Tongan that place them at such high risk for probable PND. Of equal importance is increasing understanding of why Samoans have low rates when exposed to adverse circumstances, including multiple known risk factors. Identification of protective factors could be of considerable value in developing prevention programmes for Pacific Island and other high-risk groups.
It is possible that Tongans resident in New Zealand and perhaps elsewhere, including Tonga, have higher rates of depressive disorders generally, not just postpartum. Research bearing on this is lacking. A national general adult population psychiatric epidemiological study is currently in the field in New Zealand. It includes oversampling of Pacific Island people and should help clarify this matter. In this regard, it would have been helpful to include assessment of past history of depressive episodes in the present study. This was not considered at the 6-week postpartum assessment but will be included in a subsequent measurement cycle, which will enable this issue to be revisited and also considered in relation to the persistence of depressive symptoms beyond the postpartum period.
Non–New Zealand birth and years of residence were not found to be associated with probable PND. This raises the possibility that PND rates in Pacific Island nations may be similar to what they are in New Zealand. Although often used as indicators of acculturation, the preceding indices are a crude proxy for complex and dynamic processes. Aspects of acculturation were assessed more directly by a measure of cultural orientation. On the basis of theory and previous international research [41–43], it was hypothesised that mothers who adopted an integration adaptation strategy (i.e. high NZ, high PI) would have the lowest prevalence of depressive symptoms and those who adopted a marginalization strategy (low NZ, low PI) would have the highest prevalence. Those using other strategies, namely assimilation (high NZ, low PI) or separation (low NZ, high PI), were considered likely to fall between the former groups.
Consistent with expectations marginalizers who did not participate significantly in either Pacific Island or the majority culture had elevated prevalence, which remained when the effects of other risk factors were taken into account. Although integrationalists were at low risk, so too were those who adopted a separation strategy, valuing and engaging significantly with Pacific Island cultural norms. In comparison to women pursuing either of these ‘adaptive’ strategies, assimilationists who favoured dominant cultural practices were at somewhat higher risk. These findings suggest that retention of elements of traditional Pacific identity and culture serve a protective role with respect to postpartum psychological disorder. Further research is required to assess this, to determine which particular values and behaviours are implicated and whether or not they differ across Pacific ethnic groups.
Given that the present study is confined to cross-sectional data, it cannot be ascertained whether risk factors have a causal relationship with depressive symptoms. Some factors, particularly those involving mothers' satisfaction ratings of various experiences and relationships, could well be a consequence of depressive symptoms, rather than a cause. Alternatively, they may share a common underlying cause. However, a number of the correlates of probable depression have emerged in previous prospective studies, suggesting that they are causally implicated. Although further research is required, the risk factors identified in this study provide a guide to identifying women who have a high probability of being depressed. They point to potential intervention points for social policy and prevention programming and may also have relevance to treatment planning and the ongoing wellbeing of mothers and families.
Footnotes
Acknowledgements
The Pacific Island Families Study is supported by grants awarded by the Foundation for Science, Research and Technology, the Health Research Council of New Zealand and the Maurice and Phyllis Paykel Trust. We note, with appreciation, the contribution of families participating in the study and other members of the PIF research team.