
Abstract
Until recently, modern medicine has focused on assessing patients through objective measures [1]. This is true of eating disorder studies. Increasingly, in medicine the focus is being redirected toward assessing the broader personal and social context of the person with the disease [1]. Quality of life (QOL) methodology has become an important adjuvant and alternative tool in clinical assessment [2]. QOL assessments are particularly useful in the management of individuals with psychiatric conditions and chronic medical conditions such as cancer, diabetes, epilepsy and chronic liver and renal disease [3] However, as claimed by Padierna, there is a distinct lack of relevant literature on health-related QOL research specific to eating disorders despite the disorders' being associated with significant physical, psychological and social dysfunction [4].
The World Health Organization (WHO) defines QOL as an ‘individual's perception of their position in life in the context of the culture and value system in which they live and in relation to their goals, expectations, standards and concerns’ [2]. Thus QOL is influenced by a broad range of associated domains, interlinking physical health with social and psychological functioning.
QOL assessments can be either generic or diseasespecific, subjective or objective [5]. Examples of the former include general health surveys such as the SF-12 or SF-36.1 [6]. For QOL assessments to be used for measurement of outcomes they must be accurate, reliable and valid. As stated by Skevington and Wright [7], ‘it is vital to the success of evidence-based medicine that the validity of outcome measures are established, otherwise measurement error can unwittingly lead to erroneous conclusions from clinical trials’. The aim of this study is to provide a valid tool to assess QOL in a field that traditionally has underutilized QOL data in the assessment and management of patients. In eating disorders, the concept of ‘wellness’ is both objective and subjective, and is determined through physical, psychological and behavioural criteria [8]. The specific aims of this study are: (i) to correlate the QOL ED scores with well-validated measures of psychological, physical, behavioural and eating disorder measures (concurrent validity); (ii) to examine changes in QOL ED scores across time (predictive validity), that is, between admission to and discharge from hospital and at hospital admission and 12 months later; and (iii) to ensure that the tool differentiates between eating disorder diagnoses and no diagnoses (discriminant validity).
Method
Patients
The patients were inpatients in a specialized eating disorder unit at the Northside Clinic, Sydney. Minimum age for admission to the clinic is 14 years. Most patients that failed outpatient or day patient treatment, were from country areas or from interstate. All patients included in the sample were female, ≤40 years and had been an inpatient for an average of 45 (range=22–92) days. Diagnosis wasmade by a specialist psychiatrist and a specialist psychologist on admission and by at least one at the 12-month follow-up.
Two groups of patients were studied. The first sample (n=241) consisted of 183 patients on admission, 109 of these patients also at discharge and 58 patients at the 12-month follow-up (collected earlier). Their mean age was 21.8, SD=7.8 years, and mean BMI (body mass index) 19.4, SD=4.3 kg/m2, and were diagnosed with anorexia nervosa (n=74), bulimia nervosa (n=33), eating disorder not specified (EDNOS) (n=80) and no diagnosis (n=54). The second sample consisted of 65 different patients both on admission and after 12 months. Their mean age was 19.3, SD=5.9 years, and mean BMI 17.7, SD=3.0 kg/m2, and were diagnosed on admission with anorexia nervosa (n=34), bulimia nervosa (n=10) and EDNOS (n=21). EDNOS included binge eating disorder.
Measurement tools
The measures used in this study include the Eating and Exercise Examination (EEE-C) QOL scores [9], Eating Disorder Inventory (EDI) [10], Eating and Attitudes Test (EAT) [11], Beck Depression Inventory (BDI) [12], State–Trait Anxiety Inventory (STAI) [13], Short-Form General Health Survey (SF-12) [5], Mental Summary Score (MSC) and Physical Summary Score (PSC). The EDI subscales examined were as follows: drive for thinness, bulimia, body dissatisfaction, ineffectiveness, perfectionism, interoceptive awareness; asceticism, impulse regulation and social insecurity.
The EEE-C was developed as an efficient, self-reported, computergenerated and computer-reported examination of eating and exercise behaviour, attitudes and feelings [9]. The QOL ED scores are computer administered, scored and reported and derived from 21 questions plus measured height and body weight. Each question is asked for the last 28 days or the last 3 months.
The QOL ED scores are as follows: body weight (BW), eating behaviour (EB), eating disorder (ED), psychological (PSY), acute medical (AMED) and daily living (DL). All of these values are scored on a scale of 0 to 4. There is a global QOL ED score, which is the total of all the six above-mentioned scores. This is scored on a scale of 0 to 24. The questions and scoring are available from the corresponding author upon request. Only data for the previous month are reported in this paper. All scores were derived from EEE-C question data from previous studies.
Procedure
Patients completed the EEE-C and questionnaires within the first week of inpatient treatment, before discharge or 12months later. The research was approved by the Human Ethics Committees, the Northside Clinic and the University of Sydney.
Analysis
Spearman's correlation (non-parametric) coefficient was used to examine concurrent validity of the global and individual QOL ED scores with the well-validated psychological, psychiatric, QOL and eating disordermeasures. Paired t-tests were used to compare the QOLED scores, between admission and discharge and at admission and 12months later. One-way anova with Bonferroni correction discriminated between QOL ED scores and eating disorder diagnoses. For all comparisons, the p-value for significance was 0.001.
Overall and domain internal consistency was measured using Cronbach's alpha.
Results
QOL ED correlations with eating disorder measures
The correlations of the QOL ED global and domain measures (for p < 0.001) and the established eating disorder measures are given in Table 1. The global score correlated the highest with the EAT and interoceptive awareness subscale of EDI.
Spearman's correlations coefficient (for p< 0.001) between QOL ED scores and established eating disorder measures (highest correlation highlighted) (n = 232)
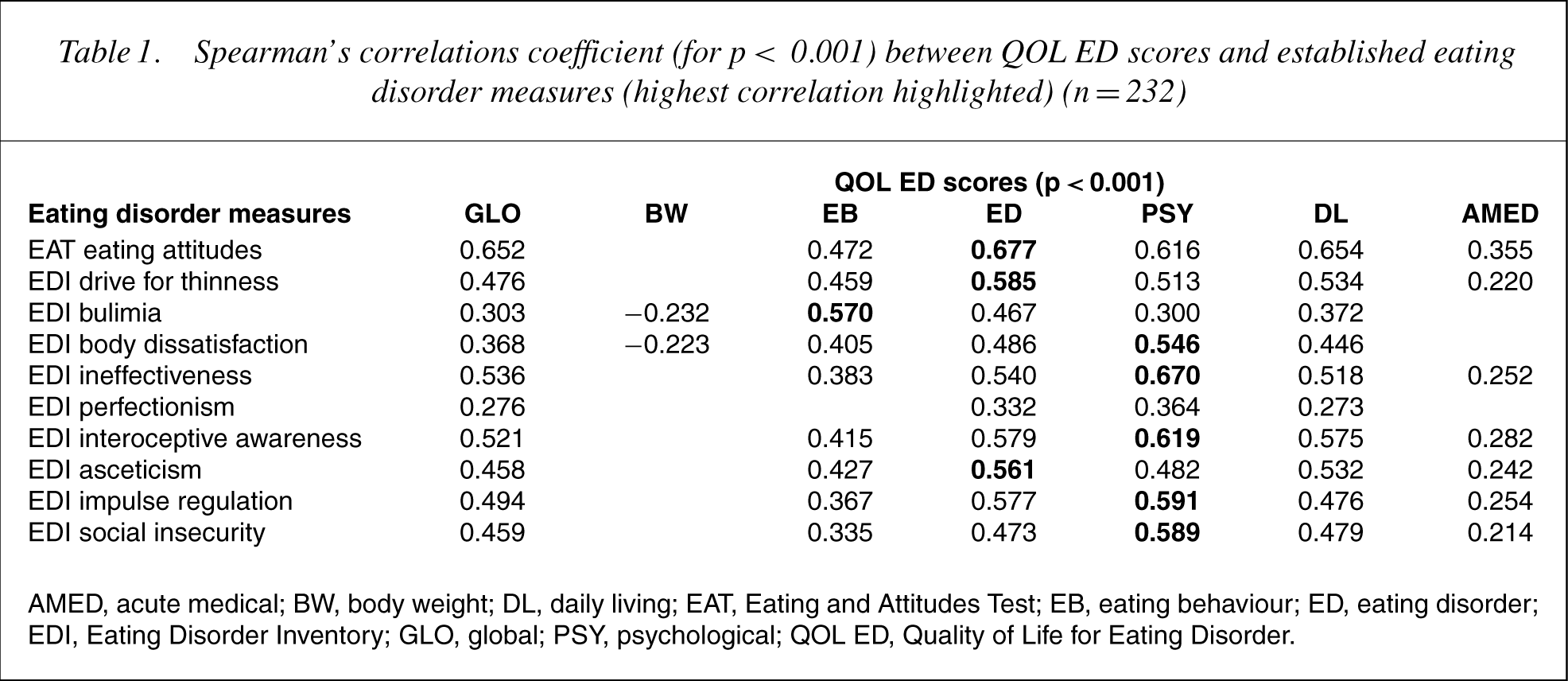
AMED, acute medical; BW, body weight; DL, daily living; EAT, Eating and Attitudes Test; EB, eating behaviour; ED, eating disorder; EDI, Eating Disorder Inventory; GLO, global; PSY, psychological; QOL ED, Quality of Life for Eating Disorder.
QOL correlations with psychological and physical measures
The correlations of the QOL ED global and domain measures (for p < 0.001) and the established psychological and physical measures are given in Table 2. The global score correlated highest with BDI, STAI and the mental assessment QOL score (SF-12).
Spearman's correlations coefficient (for p< 0.001) between QOL ED scores and established psychological, physical and behavioural measures (highest correlation highlighted) (n = 232)
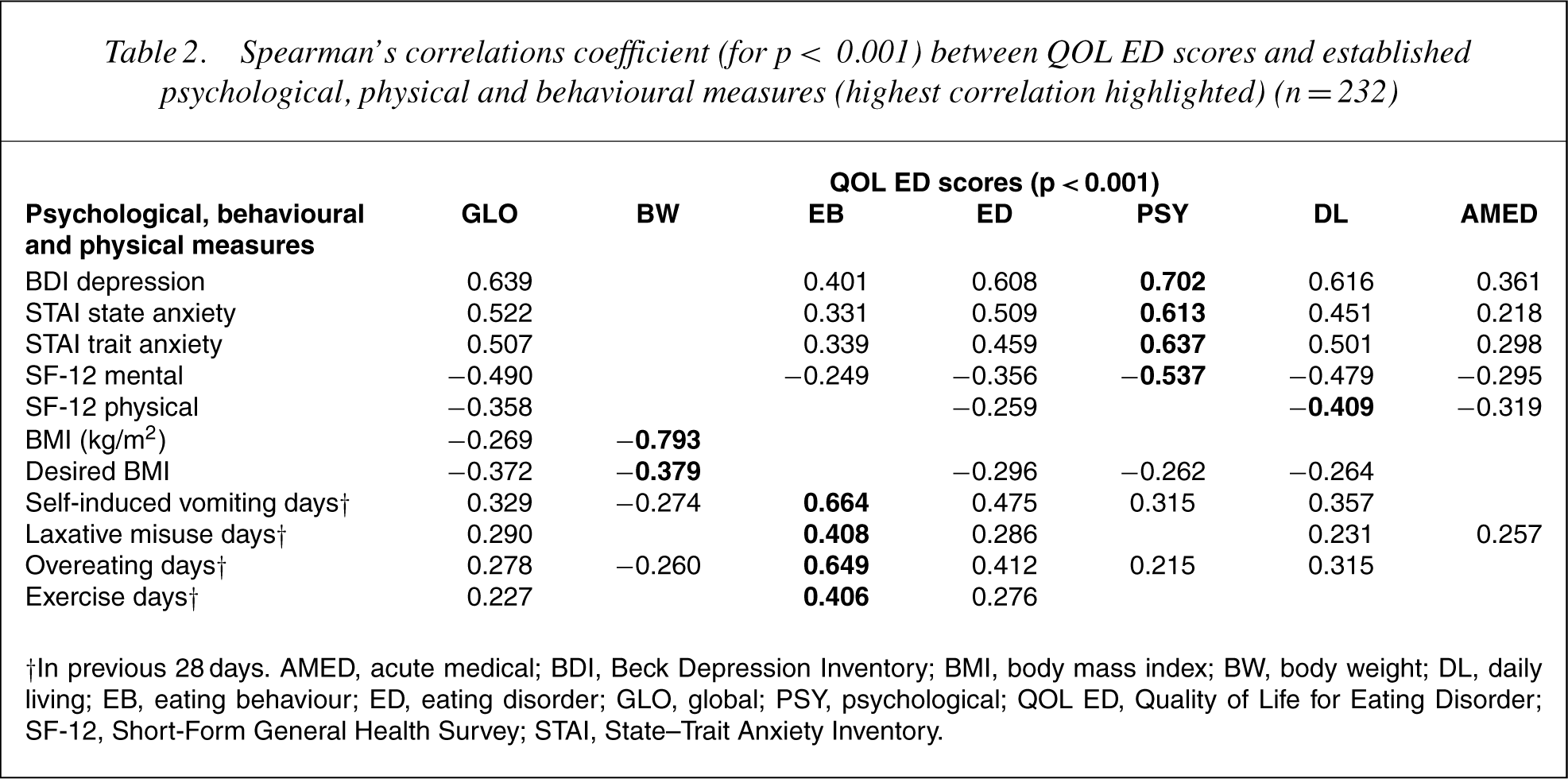
†In previous 28 days. AMED, acute medical; BDI, Beck Depression Inventory; BMI, body mass index; BW, body weight; DL, daily living; EB, eating behaviour; ED, eating disorder; GLO, global; PSY, psychological; QOL ED, Quality of Life for Eating Disorder; SF-12, Short-Form General Health Survey; STAI, State–Trait Anxiety Inventory.
Internal consistency
The instrument showed high internal consistency when each question was tested (Cronbach's alpha=0.93). The internal reliability of each domain score was good: EB (Cronbach's alpha=0.58), ED (Cronbach's alpha=0.84), PSY (Cronbach's alpha=0.89), DL (Cronbach's alpha=0.88).
QOL ED admission and discharge
Table 3 shows that the QOL ED scores are all statistically significantly improved between admission and discharge. The reference scores for a community group of 264 female students aged 14 to 28 years are also listed.
Comparison of QOL ED scores at admission and discharge from hospital (n = 109)
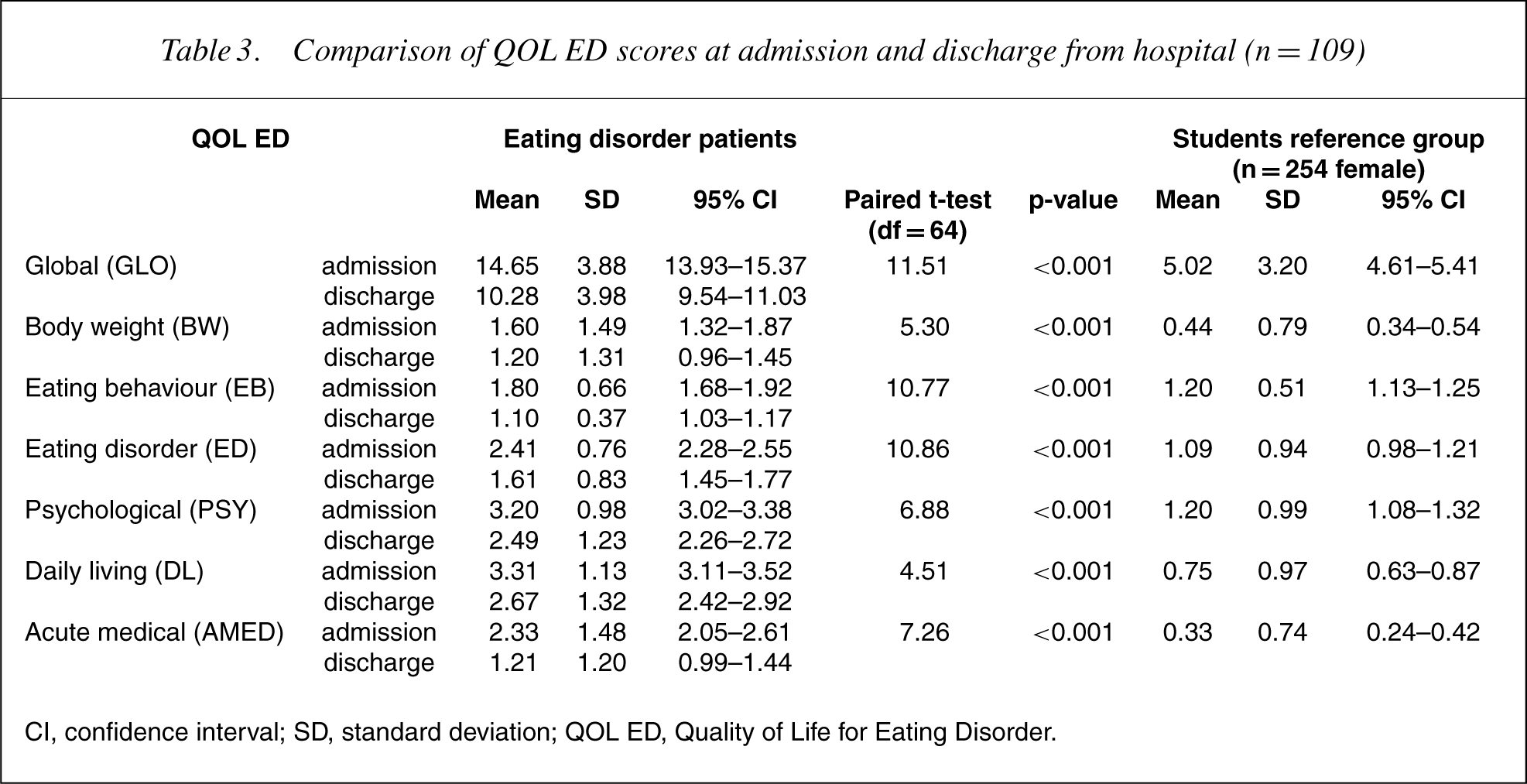
CI, confidence interval; SD, standard deviation; QOL ED, Quality of Life for Eating Disorder.
QOL ED changes admission and 12 months
Table 4 shows that the QOL ED scores are all statistically significantly improved between admission and at the 12-month follow-up.
QOL ED admission and after 12 months (n = 65)
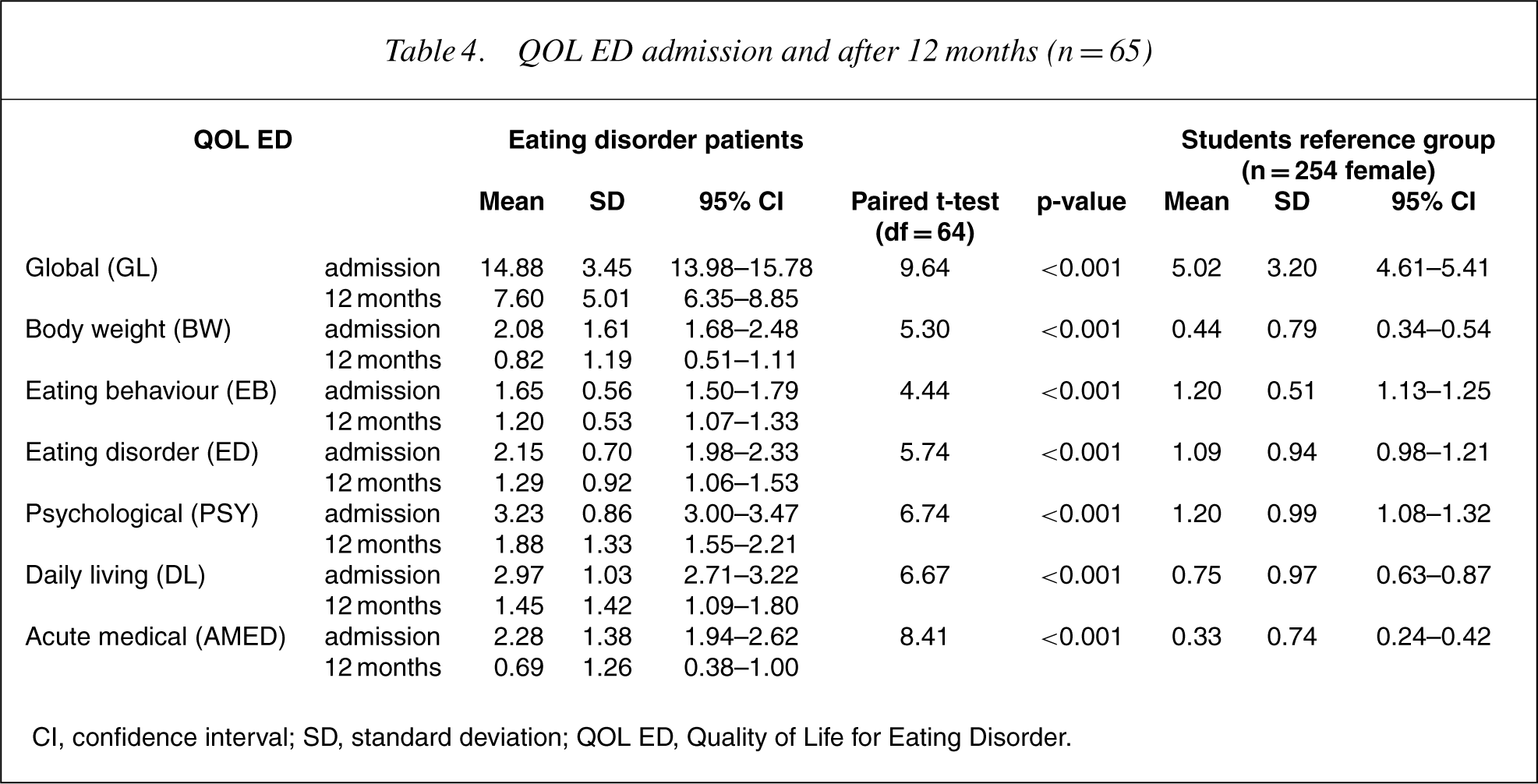
CI, confidence interval; SD, standard deviation; QOL ED, Quality of Life for Eating Disorder.
QOL ED and clinical diagnoses
Themean values for the QOL ED scores for each diagnosis are shown in Table 5. All QOL ED scores for the diagnoses of anorexia nervosa, bulimia nervosa and EDNOS were significantly greater than those for no diagnosis (p < 0.001). Anorexia nervosa and bulimia nervosa were significantly different for QOL ED scores of body weight, eating behaviour and eating disorder (p < 0.001). The scores for anorexia nervosa and EDNOS were significantly different for QOL global, body weight and acute medical (p < 0.001). Bulimia nervosa and EDNOS were significantly different for all QOL ED scores except psychological (p < 0.001). There were no significant differences between the three eating disorder groups for psychological scores and daily living scores.
QOL ED for eating disorder diagnoses; anorexia nervosa (n = 71), bulimia nervosa (n = 55), EDNOS (n = 80) and no diagnosis (n = 35)
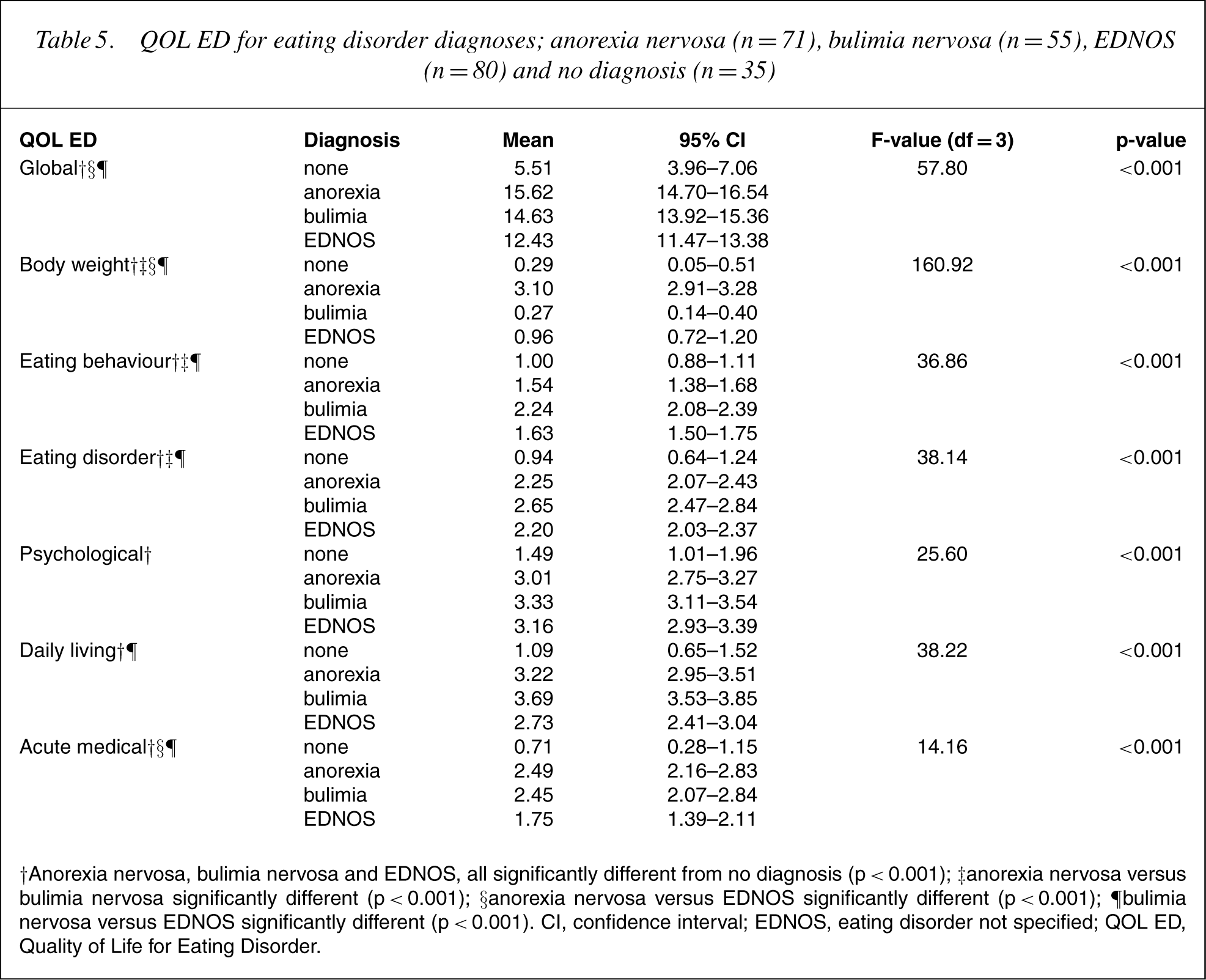
†Anorexia nervosa, bulimia nervosa and EDNOS, all significantly different from no diagnosis (p < 0.001); ‡anorexia nervosa versus bulimia nervosa significantly different (p < 0.001); §anorexia nervosa versus EDNOS significantly different (p < 0.001); ¶bulimia nervosa versus EDNOS significantly different (p < 0.001). CI, confidence interval; EDNOS, eating disorder not specified; QOL ED, Quality of Life for Eating Disorder.
Discussion
QOL assessments emphasize the patient, not the disease [1], and therefore must be self-reported by the patient. They have the ability to unearth issues that are important to the patient, thus facilitating optimal treatment and outcomes and enhanced patient–health professional interaction [14]. As far as is known, this is the first QOL measure specific to eating disorders. The global and domain measures apply to all eating disorders: anorexia nervosa, bulimia nervosa and EDNOS (including BED). The QOL ED provides self-reported measures of behaviour, eating disorder feelings, psychological feelings, perceived affect on study/work, social life and relationships and acute medical status. Body weight is measured and also included, as extreme weights can reflect poor physical and mental health that is denied or not recognized by the very emaciated or morbidly obese person. It can be used to assess the previous 28 days in short-term assessments or the previous 3months if preferred in longer-term studies.
The QOL ED measures correlate highly with established measures of eating disorder behaviour and attitudes, with validated psychological measures and mental and physical QOL measures (SF-12). The best traditional measures are the EAT and the BDI. The Speilberger STAI and the interoceptive awareness subscale score of the EDI were also excellent. Inspection of the maximal QOL ED scores for each domain correlated appropriately with the established measures, for example, QOL eating disorder with EDI drive for thinness, QOL eating behaviour with EDI bulimia and QOL psychological with EDI ineffectiveness.
More important, the data have shown that this measure is reliable and sensitive to change over time and can therefore be useful in the longitudinal assessment and management of patients with eating disorders. It showed highly significant changes over the short term (during hospital inpatient treatment) and over a longer time (12 months) in global and all domains. The comparative sizes and directions of the changes were appropriate. The changes during inpatient treatment were smaller (global) and predominately had to do with eating behaviour and eating disorder feelings. The changes over 12months were greater (global) and predominantly had to do with eating disorder feelings and psychological feelings. The acute medical scores indicated that not all 155 patients had short-term physical medical problems and not all medical problems were resolved during hospital admission. The daily living score, that is, the effects of their eating and exercise problems on their study/work, social life and relationships with friends and family appear to reflect the global scores. This is exactly what a good QOL instrument should indicate: the amount of distress perceived by the person at a given time, and not as assessed by the clinician on the basis of objective measures.
QOL ED scores for the different diagnoses show that: (i) an eating disorder diagnosis is clearly differentiated from a no eating disorder diagnosis (recovered) for global and all domain scores; and (ii) there are differences between the scores for the eating disorder diagnoses both dependent on and independent of the behaviours and body weight used in making a diagnosis, that is, overeating for bulimia nervosa. The differences and lack of differences between the diagnoses and QOL scores may help our understanding of patient's perceptions of their eating disorders, for example, defect of daily living and psychological distress is no different between all eating disorder diagnoses.
The criticism of this instrument is that it has not been trialled as a stand-alone pen-and-paper questionnaire at this time; it has always been administered, scored and reported by computer. Population norms are given for 264 female students aged 14 to 28 years in this paper; norms for a wider age range of women and for men is needed. The measure needs to be examined with obese men and women.
In summary, this QOL ED is a quick 21-question selfreport instrument that covers the domains of behaviour, eating disorder feelings, psychological feelings, effects on daily life, effects on acute medical status and body weight and has a global score. It can be used clinically and in research to monitor progress in both the short and the long term, be used to discuss progress with the patient, is able to highlight the aspects of a person's disorder requiring more attention, and can be used to talk with the patients about their areas of distress and to clarify any misconceptions patients may have about their understanding of their eating disorder or theirmedical status. In other words, this instrument fulfils the potential uses for a QOL assessment in the clinical and research setting [1]. This research suggests that some eating disorder patients can recover within 12 months of inpatient treatment and that most of them show improvement.