
Abstract
Introduction
In the past decade, evidence has accumulated concerning impairment in quality of life associated with the eating disorders anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED) and variants of these disorders not meeting formal diagnostic criteria (Engel et al., 2009; Hay and Mond, 2005; Jenkins et al., 2011). Findings from this research have shown that individuals with these disorders who receive specialist treatment have high levels of impairment in certain aspects of quality of life, particularly those relating to psycho-social functioning (Crow and Peterson, 2003; Engel et al., 2009; Hay and Mond, 2005; Jenkins et al., 2011). Impairment in aspects of quality of life relating to physical health is more variable and, as would be expected, is most pronounced among patients who are very underweight (i.e. those with AN or variants of AN) or very overweight (i.e. those with BED or variants of BED) (Engel et al., 2009; Hay and Mond, 2005; Jenkins et al., 2011; Mond et al., 2004a; Wilfley et al., 2003).
Although this research is welcome, it is important to recognise that the poor quality of life observed among individuals with mental health problems who receive specialist treatment reflects, at least in part, the fact that impairment in role functioning is predictive of whether such treatment is received (Andrews, 2000). Uptake of mental health care among individuals with bulimic-type eating disorders, namely, BN, BED and variants of these disorders, may be particularly low and treatment-seeking for these disorders may be particularly closely tied to perceived impairment in quality of life (Fairburn et al., 1996; Mond et al., 2007a, 2009; Wilfley et al., 2001). Hence, and particularly for these more commonly occurring eating disorders, caution needs to be exercised when drawing conclusions about impairment in quality of life based on findings from clinical samples.
Data bearing on the quality of life of individuals with eating disorders recruited from general population samples are, however, limited (Hay and Mond, 2005; Jenkins et al., 2011). Hay (2003) found, in a general population sample of women and men, that participants who reported binge eating and/or extreme weight-control behaviour had lower scores on several subscales of the SF-36 and on the Mental — but not Physical — Component Summary scale, when compared with participants not reporting these behaviours. Mond et al. (2004a) found, in a general population sample of women, that individuals with bulimic-type eating disorders had high levels of impairment in mental health, as measured by the SF-12 Mental Component Summary scale, but minimal impairment in physical health, as measured by the SF-12 Physical Component Summary scale. Doll et al. (2005) found that college students with a (self-reported) history of disordered eating had lower scores on all but the physical functioning subscale of the SF-36, although differences were more pronounced for subscales tapping mental health. In the US National Comorbidity Replication Study (Hudson et al., 2007) most participants with bulimic-type eating disorders reported at least mild impairment in one or more domains of functioning, whereas severe impairment in role functioning was comparatively uncommon. There were no individuals currently meeting diagnostic criteria for AN in any of these studies, as is typically the case in general population studies (Mond et al., 2007a, 2009).
The goal of the present study was to add to this literature. Specifically, we compared quality of life between women with eating disorders — recruited from a large, general-population sample — and healthy women, using two different quality of life measures and considering both summary-score and item-level differences. Aside from hypothesising that impairment would be most pronounced for those items tapping mental health status, we were interested to know which specific aspects of mental health would be most affected and which specific aspects of physical health, if any, would be affected.
Methods
Study design and participants
Women with eating disorders were recruited as part of the Health and Well-Being of Female ACT Residents Study, a two-phase epidemiological study of disability, health-service utilisation and ‘mental health literacy’ associated with community cases of eating disorders (Mond et al., 2007a, 2008, 2009).
Recruitment of participants at the first phase of the study has been detailed in several previous publications (Mond et al., 2006a, 2006b, 2007b). In brief, self-report questionnaires were completed by 5255 female residents of the Australian Capital Territory (ACT) region aged 18 to 42 years (response rate of 57.1%). The ACT is a highly urbanised region that includes the city of Canberra (population of 314,000 in 2002). The questionnaire included measures of eating-disorder psychopathology, health-related quality of life, subjective quality of life, and demographic characteristics, namely, age, marital status, employment status, level of education, parity, first language, country of birth and (as a proxy for income) possession of private health insurance. Body mass index (BMI) (kg/m2) was calculated from self-reported height and weight (Mond et al., 2004b). The sample comprised approximately 10% of the total population of women aged 18 to 42 in the ACT and was representative of this population in terms of the demographic characteristics referred to above (Mond et al., 2006b).
Participants who met the screening criteria for an eating disorder, namely, a high level of weight or shape concerns in conjunction with the regular occurrence of any eating-disorder behaviour over the previous four weeks (Mond et al., 2004b), were approached to participate in the second phase of the study, involving a face-to-face interview. The interview assessment included administration of the diagnostic items of the Eating Disorder Examination (EDE) (Fairburn and Cooper, 2003), a semi-structured, investigator-based interview that may be used to assign operational diagnoses for the DSM diagnoses of AN, BN, BED and Eating Disorder Not Otherwise Specified (EDNOS) and that is widely regarded as the interview assessment of choice in the field (Mitchell and Peterson, 2005). Interviews were completed with 324 individuals, which represented a response rate of 76.6% at the second phase. Individuals interviewed were more likely to be married than those not interviewed (38.2% versus 29.8%; χ2= 9.58, p < 0.05). There were no other differences between these groups.
One hundred and fifty-nine participants (48.8% of the interviewed sample) were classified as eating-disorder cases based on the interview assessment, with diagnoses of: BN: n = 30; BED: n = 20; and EDNOS: n = 109. Participants with EDNOS were primarily variants of BN or BED, for example, individuals who reported regular episodes of subjective over-eating, extreme concerns about weight or shape and extreme weight control behaviours, but not objective over-eating (binge eating) episodes (Mond et al., 2010a). Only four participants (2.5%) with eating disorders were currently underweight (BMI < 18.5), none of whom met the criteria for AN. Less than half (40.3%) of women with eating disorders had ever received advice or treatment from a health professional for an eating problem, typically a primary care practitioner (Mond et al., 2007a).
The recruitment of healthy women has also been described previously (Mond et al., 2004a, 2004b). In brief, as part of pilot work for the Health and Well-Being Study, self-report questionnaires were completed by 232 female ACT residents aged 18 to 45 selected, at random, from the Electoral Roll (response rate = 63.8%). The questionnaire included the same measures of eating-disorder symptoms and quality of life subsequently employed in the larger study, as outlined below. For convenience, we refer to individuals in the pilot study sample as ‘healthy women’, although the term ‘general population sample’ is, strictly speaking, more accurate. The sample was representative of young adult women in the region in terms of socio-demographic characteristics (Mond et al., 2004b).
When compared with healthy women, women with eating disorders were younger (mean = 28.9 years, SD = 5.6 versus mean = 33.6, SD = 9.0; t = 5.59, p < 0.01), had higher BMIs (mean = 27.2, SD = 7.1 versus mean = 24.6, SD = 5.6; t = -3.85, p < 0.01), were less likely to be married or living as married (53.8% versus 65.8%; χ2 = 5.59, p < 0.05), less likely to have one or more children (40.9% versus 57.0%; χ2 = 9.72, p < 0.01), and more likely to have been born in Australia (90.6% versus 82.7%; χ2 = 4.83, p < 0.05). (Whereas 26.9% of women with eating disorders met the accepted criterion for obesity (BMI ≥ 30), 15.3% of healthy women were obese (χ2 = 7.22, p < 0.01). The prevalence of severe obesity (BMI ≥ 40) was low in both groups (healthy women: 2.3%; eating disorders: 5.5%; χ2 = 2.53, p = 0.11).
Where appropriate, data for a clinical sample of women with eating disorders receiving specialist treatment (n = 118) are given for descriptive purposes, namely to give an indication of the ‘clinical significance’ of the impairment in quality of life observed among community eating-disorder cases. The clinical sample, which was recruited coincident with the community sample, comprised consecutive referrals to the ACT Eating Disorders Day Program with diagnoses of AN (n = 35), BN (n = 43) and EDNOS (n = 40) (Mond et al., 2005).
Study measures
Eating Disorder Examination Questionnaire
The Eating Disorder Examination Questionnaire (EDE-Q) (Fairburn and Beglin, 1994) is a 36-item self-report measure of eating disorder symptoms derived from the EDE interview. The EDE-Q focuses on the past 28 days and is scored using a 7-point, forced-choice, rating scheme. Subscale scores — relating to dietary restraint and concerns about eating, weight and shape — and a global score, are derived from 22 items addressing attitudinal aspects of eating-disorder psychopathology (Mond et al., 2006). Scores on these scales range from 0 to 6, with higher scores indicating higher symptom levels. In the present study, the EDE-Q subscales provided a continuous measure of eating-disorder symptoms. High levels of agreement have been demonstrated between self-report-(EDE-Q) and interview-(EDE) derived subscale scores in various study populations (Mond et al., 2004b; Berg et al., 2011). Remaining items of the EDE-Q assess the occurrence and frequency of eating-disorder behaviours. These items were not considered in the present study since eating-disorder behaviours were assessed at the (EDE) interview.
Medical Outcomes Study (12-item) Short-Form disability scale
Health-related quality of life was assessed with the Medical Outcomes Study (12-item) Short-Form disability scale (SF-12). Items of the SF-12 are summarized into two weighted scales (Physical Component Summary scale, PCS; and Mental Component Summary scale, MCS), designed to assess physical and mental health impairment. Each scale is scored to have a mean of 50 and standard deviation of 10 (in the US population), with lower scores indicating higher levels of impairment. The SF-12 has very good psychometric properties, including demonstrated validity in the Australian population (Sanderson and Andrews, 2002; Ware et al., 1996). PCS items include “Does your health now limit you in moderate activities, such as moving a table, vacuuming or playing golf?” and “During the past four weeks, were you limited in the kind or work or other activities undertaken as a result of your physical health?”. MCS items include “During the past four weeks have you accomplished less than you would like as a result of any emotional problems?” and “During the past four weeks how much of the time have you felt calm and peaceful”? A score of 30 or less on the MCS has been taken to indicate severe impairment in mental health (Sanderson and Andrews, 2002).
World Health Organization Brief Quality of Life Assessment Scale
Subjective quality of life was assessed using the World Health Organization Brief Quality of Life Assessment Scale (WHOQOL-BREF), a 26-item measure yielding scores on four domains relating to the individual’s subjective evaluation of physical health, environmental health, psychological functioning and social relationships (Skevington et al., 2004; WHOQOL Group, 1998). Items are scored on a five-point, Likert-type scale, with scores of ‘1’ and ‘5’ indicating, respectively, extreme dissatisfaction and extreme satisfaction. Only items comprising the Psychological Functioning (QOL-P) and Social Relationships (QOL-S) domains were included in the present study because perceived physical health was considered to be adequately assessed by the SF-12 and items tapping environmental health were not considered relevant for the ACT population. Items of the QOL-P include “To what extent do you feel your life to be meaningful?” and “How satisfied are you with yourself?”, whereas items of the QOL-S include “How satisfied are you with your personal relationships?” and “How satisfied are you with the support you get from your friends?”. One of the (six) items comprising the QOL-P, which specifically addresses body dissatisfaction, was excluded when calculating summary scores.
Statistical analysis
Independent samples t-tests were used to compare scores on summary measures of quality of life, namely, the SF-12 PCS and MCS and WHOQOL-BREF QOL-P and QOL-S, between healthy women and (community cases of) women with eating disorders. For the item-level analysis, dichotomous variables were created for each of the 21 items comprising the four summary scale QOL measures such that, for each item, the two responses indicating poorest quality of life (e.g. ‘very dissatisfied’, ‘extremely dissatisfied’) were coded ‘1’ (‘quality of life poor’), whereas the remaining responses were coded ‘0’ (‘quality of life not poor’). Chi-square (χ2) tests were then used to examine differences between groups in the proportion of participants reporting poor quality of life, for each item, whereas multiple logistic regression analysis was used to examine the likelihood of poor quality of life for individuals with eating disorders when compared with healthy individuals, controlling for between-group differences in age, BMI and demographic characteristics.
Results
Comparison of women with eating disorders and healthy women on summary measures of eating-disorder psychopathology and quality of life is shown in Table 1. As can be seen, women with eating disorders had large decrements in scores on the SF-12 MCS and QOL-P, whereas a more modest (but still highly significant) difference between groups was observed on the QOL-S. Women with eating disorders also tended to have lower scores on the SF-12 PCS than healthy women (p = 0.07).
Mean (SD) scores on measures of eating-disorder psychopathology and quality of life among community cases of women with eating disorders and healthy women.
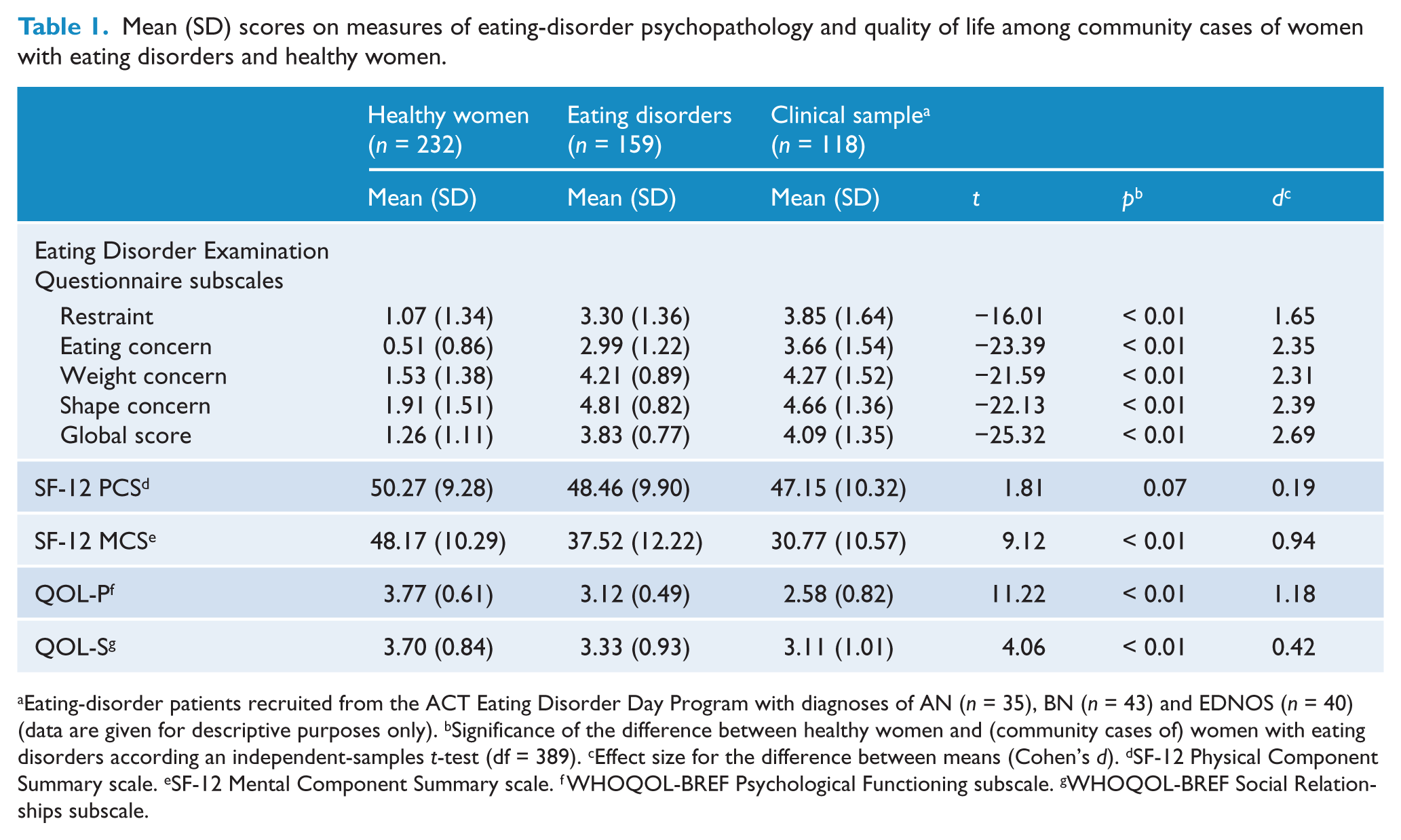
Eating-disorder patients recruited from the ACT Eating Disorder Day Program with diagnoses of AN (n = 35), BN (n = 43) and EDNOS (n = 40) (data are given for descriptive purposes only). bSignificance of the difference between healthy women and (community cases of) women with eating disorders according an independent-samples t-test (df = 389). cEffect size for the difference between means (Cohen’s d). dSF-12 Physical Component Summary scale. eSF-12 Mental Component Summary scale. fWHOQOL-BREF Psychological Functioning subscale. gWHOQOL-BREF Social Relationships subscale.
These findings were unchanged when between-group differences in age, BMI and demographic characteristics were statistically controlled. Whereas 9.4% of healthy women reported severe impairment in mental health (SF-12 MCS ≤ 30), 28.9% of women with eating disorders reported severe impairment in mental health (χ = 24.26, p < 0.01; adjusted odds ratio = 4.56, 95% CI: 2.23, 9.34).
In Table 2, it can be seen that, in simple (bivariate) analysis, having an eating disorder was associated with poorer quality of life for all nine of the items comprising the WHOQOL-BREF Psychological Functioning and Social Relationships subscales and for nine of the 12 items comprising the SF-12. Also, in Table 2, it is apparent that these findings were unchanged when the analysis was repeated using logistic regression analysis to control for between-group differences in age, body weight and demographic characteristics, with the exception that differences between groups on the WHOQOL-BREF items addressing satisfaction with personal relationships and social support and the SF-12 item addressing impairment in social activities no longer reached statistical significance at the 0.05 level.
Proportions of healthy women and women with eating disorders reporting poor quality of life on specific items of the SF-12 Physical and Mental Component Summary scales and WHOQOL-BREF Psychological Functioning and Social Relationships subscales.
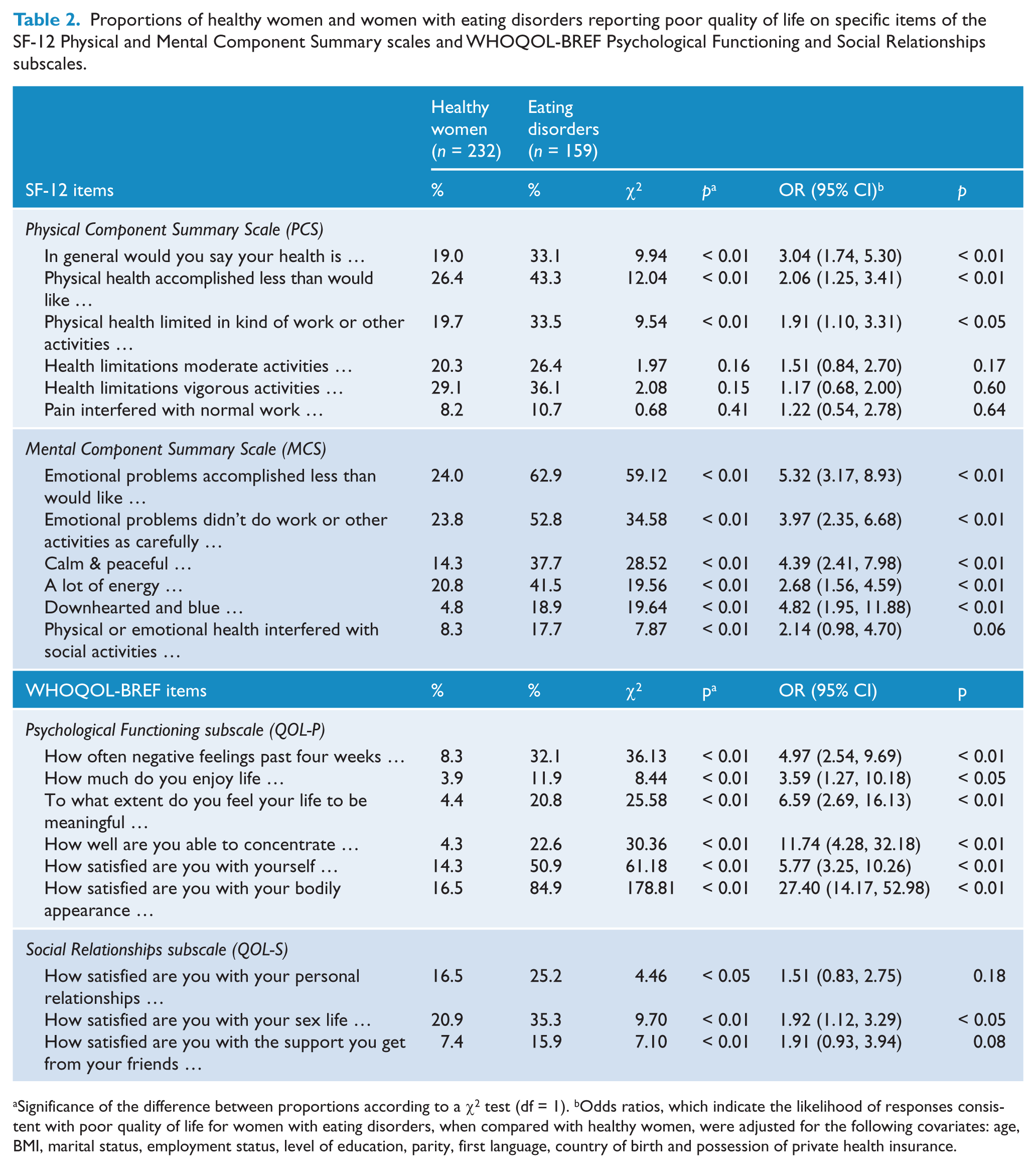
Significance of the difference between proportions according to a χ2 test (df = 1). bOdds ratios, which indicate the likelihood of responses consistent with poor quality of life for women with eating disorders, when compared with healthy women, were adjusted for the following covariates: age, BMI, marital status, employment status, level of education, parity, first language, country of birth and possession of private health insurance.
In both bivariate and multivariable analysis, differences between groups were most pronounced for items addressing perceived impairment in or dissatisfaction with emotional well-being and psycho-social functioning. However, statistically significant differences between groups on three of the SF-12 items addressing physical health impairment, namely, “general health”, “physical health accomplishments” and “physical health limitations”, were observed in bivariate analysis and each of these differences remained significant after controlling for potential covariates.
Discussion
Summary of main findings
We examined impairment in quality of life among community cases of women with eating disorders. When compared with healthy women, women with eating disorders had marked impairment in aspects of quality of life relating to mental health functioning, as measured by the SF-12 Mental Component Summary scale and WHOQOL-BREF Psychological Functioning subscale, and this was the case in both bivariate and multivariable analysis. Impairment in social relationships, as measured by the WHOQOL-BREF Social Relationships subscale, and in physical health, as measured by the SF-12 Physical Component Summary scale, was less pronounced and due, at least in part, to between-group differences in age, body weight and demographic characteristics. Nevertheless, significant impairment in certain aspects of physical health was apparent after controlling for these variables.
Study implications
The finding that women with eating disorders, as a group, reported substantial impairment in aspects of quality of life relating to emotional well-being is consistent with findings from previous studies and reflects, at least in part, the fact that BN, BED and variants of these disorders are associated with high levels of comorbidity with anxiety and affective disorders (Jenkins et al., 2011; Mond et al., 2009). In the present study, close to one third (29.8%) of women with eating disorders reported severe impairment in mental health, the latter defined as a score of 30 or less on the SF-12 MCS, compared with 9.4% of healthy women.
However, the present findings also suggest that there is considerable variation in the extent to which the behaviours characteristic of bulimic-type eating disorders are associated with mental health impairment and that, in the general population, a substantial proportion of women with these disorders may experience only mild to moderate impairment in certain aspects of quality of life. Thus, only 10.2% of participants with eating disorders rated their quality of life as poor or very poor, only 11.9% reported that they enjoyed life a little or not at all and only 20.8% reported that their life was a little or not at all meaningful. Less than one-third (29.8%) of women with eating disorders reported severe mental health impairment, defined as a score of ≤ 30 on the SF-12 MCS.
In interpreting these findings, it is important to note that eating disorders, unlike most other psychiatric conditions, have strongly ego-syntonic features, such as the sense of achievement and pride afforded by rigid control of dietary intake and/or the regular use of extreme weight-control behaviours (Gale et al., 2006; Vitousek et al., 1998). Whereas the treatment challenges posed by these features are well-known to clinicians, their implications for the assessment of quality of life have not generally been considered (Mond et al., 2005). For example, evidence suggests that perceived impairment in psycho-social functioning among some individuals with AN, particularly those in the early, restricting phase of the disorder, may be minimal (Mond et al., 2005).
Whether, and to what extent, similar processes might operate among community cases of individuals with bulimic-type eating disorders is unclear, although it is apparent that certain bulimic behaviours are viewed as acceptable and even desirable among a subgroup of women in the community and that perceptions of this kind are associated with actual eating disorder symptoms (Mond and Arrighi, 2001; Mond et al., 2010b). Hence, it is reasonable to suggest that ego-syntonic aspects of eating-disordered behaviour may have the effect of reducing perceived impairment in quality of life among at least some individuals with BN and variants of BN.
The finding that women with eating disorders had lower subjective satisfaction with their social relationships than healthy women is consistent with findings from early studies of BN patients (Crow & Peterson, 2003; Schmidt et al., 1995). If, as the present findings suggest, bulimic behaviours are associated with impairment in social relationships at the population level, then at least two interpretations of this association might be given. First, engagement in these behaviours, which are typically associated with shame and secrecy, may be conducive to the avoidance of social situations. Second, impairment in social functioning among individuals with eating disorders may reflect the influence of an underlying vulnerability, a disturbance of personality for example, from which disordered eating initially developed (Keel et al., 2000). The latter hypothesis is consistent with findings from outcome studies of BN patients in which impairment in interpersonal relationships has been observed even after the remission of eating disorder psychopathology (Keel et al., 2000).
Also of note is that the impairment in each of the three aspects of social relationships assessed — satisfaction with personal relationships, support from friends, and one’s sex life — that was apparent in bivariate analysis was less pronounced after controlling for between-group differences in demographic characteristics. Given that the main demographic difference between participants with eating disorders and healthy women was that women with eating disorders were less likely to be married, one interpretation of these findings is that marriage may lessen the impact of disordered eating on social adjustment. Alternatively, bulimic behaviours and/or associated personality disturbance may be conducive to both social impairment and lower likelihood of marriage.
In the present study, impairment in overall levels of physical health, as measured by the SF-12 PCS, was minimal among individuals with eating disorders. Although women with eating disorders were heavier than healthy women, the prevalence of obesity among women with eating disorders was still low when compared with clinical samples of individuals with BED (Wilfley et al., 2003) and the prevalence of severe obesity was low in both groups. Further, and as might also be expected the prevalence of purging behaviours among women with eating disorders in the present study was low when compared with that observed in clinical samples of individuals with BN (Mond et al., 2006a). Nevertheless, impairment in certain aspects of physical health was apparent among women with eating disorders, even after controlling for between-group differences in body weight. Thus, when compared with healthy women, women with eating disorders were three times as likely to report that their health was poor or very poor and twice as likely to report impairment in everyday activities due to physical health limitations.
It is possible that stress associated with negative body image is conductive to perceived impairment in physical health (Muennig et al., 2008). Alternatively, or in addition, personality characteristics associated with eating disorders, such as low self-esteem, depressive mood and perfectionism, may be conducive to an unduly negative appraisal of physical health (Cassin and von Ranson, 2005). Similarly, the markedly elevated levels of perceived limitations in everyday accomplishments and perceived impairment in the ability to concentrate observed among women with eating disorders in the present study may reflect, in part, the perfectionism and achievement orientation that often feature in these disorders. The inclusion of a comparison group of women with psychiatric disorders other than eating disorders would be needed to elucidate the nature of these influences.
Study limitations and other methodological considerations
Several limitations of the present study need to be considered when interpreting these findings. First, the present findings apply only to individuals with bulimic-type eating disorders. The lack of participants with AN-type disorders likely reflects both the low base rates of eating disorders characterized by low body weight and the fact that individuals with these disorders may be over-represented among non-respondents in general population surveys (Mond et al., 2004c).
Second, the generalisability of the present findings is constrained by the choice of study population, namely, younger women from an urbanised and relatively affluent region of Australia. Replication of the findings in younger and older women and in men and women from more diverse backgrounds would therefore be of interest.
Third, we used only generic measures of quality of life. In recent years, several so-called eating-disorders-specific quality of life measures have been developed (Engel et al., 2009; Jenkins et al., 2011). The advantage of these measures, which assess the extent to which quality of life is affected by specific conditions or symptoms, is that they are likely to be more sensitive to change (Engel et al., 2009). A problem with disease-specific measures is that they require a judgement on the part of the participant as to the role of specific symptoms in accounting for impairment in different aspects of functioning. Given the high levels of comorbidity between eating disorders and symptoms of anxiety and depression, the validity of such judgements is debatable (Mond et al., 2004a).
Finally, since this was a cross-sectional study, the usual caveats concerning the direction of the observed associations apply. Whereas eating-disordered behaviour may be conducive to poor quality of life, poor quality of life, for example, associated with depression, may be conducive to disordered eating (Patton et al., 2008). Notable strengths of the present study were the recruitment of participants from a general population sample, interview assessment of eating-disorder psychopathology and the inclusion of two different quality of life measures.
Footnotes
Funding
The Health and Well-Being of Female ACT Residents Study was funded by The Canberra Hospital Private Practice Fund, ACT Health and Community Care and ACT Mental Health.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.