
Abstract
Background:
The success of integrated prevention initiatives for eating disorders and obesity is hampered by a lack of shared risk factor research. Bullying and sexual abuse are potentially potent shared risk factors for the spectrum of eating and weight disorders.
Methods:
A representative sample of N = 3005 South Australian males and females ≥15 years was interviewed about their height, weight, eating disorder symptoms, lifetime experiences of bullying and sexual abuse and mental and physical health-related quality of life.
Results:
Participants who were currently obese (25.2%) or underweight (2.7%) or who reported current eating disorder symptoms (32.7%) were between 10% and 27% more likely to have experienced bullying, and obese and eating disordered participants were also 47% and 56% more likely to have experienced sexual abuse, respectively. In regard to specific symptoms, a lifetime history of bullying was associated with increased risk of obesity, extreme dieting, purging and overvaluation of body weight and/or shape, whereas a lifetime history of sexual abuse was associated with increased risk of obesity, binge eating and extreme dieting and decreased risk of underweight. Lifetime histories of bullying and sexual abuse were associated with health-related quality of life impairment; however, lifetime bullying was associated with a greater adverse impact among participants with current eating disorder symptoms.
Conclusion:
Self-reported bullying and sexual abuse victimisation have shared associations with eating and weight spectrum problems. Differences in the symptoms associated with bullying versus sexual abuse are discussed, as well as the clinical and public health implications.
Eating disorders (EDs) are experienced by around 17% of adults (Hay et al., 2017) and are associated with significant personal and economic burden (Olesen et al., 2012). Isolating risk factors associated with EDs is crucial to improving our understanding of the aetiology of these disorders and to developing more effective intervention and prevention programmes (Sanchez-Carracedo et al., 2012). Recently, there has been a push to consider risk factors that might be shared across the full ‘spectrum of eating and weight disorders’, including obesity, underweight, forms of disordered eating and EDs (Sanchez-Carracedo et al., 2012). This has come from increased knowledge regarding the similarities (e.g. disturbances in eating and body image) and comorbidity between these conditions (Da Luz et al., 2017; Darby et al., 2009), particularly in the post–Diagnostic and Statistical Manual for Mental Disorders (5th ed.; DSM-5) era, with the formal acknowledgement of binge eating disorder (BED), an ED characterised in part by excessive consumption of food (American Psychiatric Association, 2013).
Integrated ED and obesity prevention initiatives have enjoyed limited success (with a few exceptions, e.g., Stice et al., 2008). One reason for this is the lack of research on shared risk factors. While dieting, media influence, body dissatisfaction and weight-related teasing have been suggested as potential shared risk factors for eating and weight-related problems (Haines and Neumark-Sztainer, 2006), such research has been hampered by the examination of risk factors for EDs and obesity in separate studies using different samples, designs, procedures and measurements.
To inform the improvement of prevention and early intervention programmes, it is essential to consider childhood adversity, a major psychiatric risk factor accounting for around 30% of all mental illness (Kessler et al., 2010), including EDs (Larsen et al., 2017), as well as obesity (Danese and Tan, 2014; Wegman and Stetler, 2009). Childhood adversity is not uncommon. The World Health Organization Mental Health Surveys reveal that one in three adults report a history of childhood adversity (Kessler et al., 2010) and another study indicated as many as 59.5% of Australian adults suffer similar adversity (Rosenman and Rodgers, 2004). Adversity encompasses a broad spectrum, including but not limited to bullying; physical and emotional neglect; physical, emotional and sexual abuse; and exposure to intimate partner violence, and there is evidence of sub-additive effects of multiple adversities (Kessler et al., 2010). It is thus critical to uncover how specific adversities contribute to the development of EDs and obesity to inform a targeted approach to prevention. In this study, we focus on bullying and sexual abuse as potential shared risk factors for the spectrum of eating and weight problems.
Around 40% of youth report having been bullied at least once in the past school term (Nansel et al., 2001) and 15% of Australian youth report regularly having been bullied in the past year (Thomas et al., 2017). The most commonly reported reasons among adolescents for bullying are appearance-related issues (Frisen et al., 2007). Thus, bullying is potentially a highly specific and potent risk factor for both EDs and obesity. Despite this, there is relatively little research to date that has investigated bullying as a risk factor for the onset of an ED and no major reviews are found. One multi-sample study by Hilbert et al. (2014) reported an increased risk for developing bulimia nervosa (BN) and BED among women and moderate effect sizes have also been found for the association with specific ED behaviours and body image problems with weight-related teasing specifically (Menzel et al., 2010). Obese children are also more likely to experience bullying (Puhl and Heuer, 2009), and one Australian study has reported that when overweight children experience bullying during adolescence they have greater increases in body mass index (BMI) by adulthood (Mamun et al., 2012), suggesting a bidirectional relationship.
Given the preponderance of EDs among females, sexual abuse may be a particularly relevant risk factor. By age 17, the lifetime prevalence of sexual abuse in the United States among females has been reported to be as high as 26.6%, and among males, 5.1%. Comparative estimates in an Australian telephone survey were 34% and 16%, respectively (Dunne et al., 2003). In a population-based study in the United States, male and female adults who reported childhood sexual abuse were at the highest risk, relative to participants reporting other childhood adversities, for later development of an ED (Afifi et al., 2017). This is supported by a meta-analysis of 10 studies finding a 2.7-fold increased risk for developing an ED among people with a history of sexual abuse (Chen et al., 2010). Childhood sexual abuse has also been linked with increased risk for adulthood obesity (Gustafson and Sarwer, 2004). Researchers have attempted to explain the relationship between sexual abuse and both EDs and obesity as possibly due to the use of disordered eating as a maladaptive coping mechanism (e.g. binge eating to self-soothe) or the shedding or gaining of excess weight as a ‘protective’ de-sexualising mechanism (Gustafson and Sarwer, 2004).
Adults also experience bullying and many forms of abuse, including sexual assault, bullying in the workplace and other forms of aggression. As many as 20% and 7.5% of adults report that the majority of their cyber and traditional bullying experiences, respectively, occurred during adulthood (Kowalski et al., 2018). Despite this, few studies investigate adulthood adversity (e.g. none of the 10 studies in the Chen review on sexual abuse; Chen et al., 2010). Given previous evidence that the effect of childhood bullying as a risk factor for the development of ED symptoms may not last past late adolescence (Copeland et al., 2015), it may be important to consider adversities such as bullying and sexual abuse across the lifespan, including adversity that occurs in adulthood. Aside from adults, males in general are also often excluded from research investigating sexual abuse, bullying and EDs (Chen et al., 2010). Given recent findings that demonstrate that sexual abuse also increases the risk for EDs among men (Afifi et al., 2017), it will be important that future studies in this area continue to recruit samples that include both men and women.
While the literature on adversity and EDs to date has provided evidence that bullying and sexual abuse increase the risk for developing an ED, it is unknown whether these risk factors alter the course or severity of eating and weight problems relative to people with these problems who have not experienced sexual abuse or bullying. One useful index of severity that has been used in the ED field, as well as for physical and mental conditions more generally, is impairment in mental and physical health-related quality of life (Mitchison et al., 2015). Understanding whether a history of sexual abuse or bullying increases impairment is important for several reasons, including implications for prognosis and duration of treatment, which are important points for discussion with patients who present for treatment.
Aims
This study aimed to investigate the extent to which a lifetime self-reported history of bullying and/or sexual abuse was associated with current symptoms across the eating and weight disorder spectrum. Previous methodological limitations were addressed using a population-based sample of both men and women, investigating sexual abuse and bullying that occurred at any time across childhood or adulthood, and assessing the risk for developing a range of eating and weight-related symptoms. A second aim was to determine whether a history of bullying and/or sexual abuse is associated with greater health-related quality of life impairment among people with current eating and weight spectrum disorders. It was hypothesised that histories of bullying and/or sexual abuse would both be associated with increased likelihood of current ED symptoms, obesity and underweight, and that health-related quality of life would be poorer for sufferers of eating and weight spectrum problems who had a history of sexual abuse or bullying.
Methods
Sampling procedures
Data came from the Health Omnibus Survey, an annual household interview survey with a representative sample of ≥15-year olds from South Australia. Metropolitan and rural ‘collector’ districts were randomly selected (530/3939) based on a probability proportional to size sampling procedure, and 10 dwellings were systematically chosen within each district. The person to be interviewed within each dwelling was the person who was at least 15 years of age and had their birthday most recently. The samples were non-replacement, and up to six visits were made to conduct an interview with the designated participant. Interviews were conducted from September until December 2015. After excluding individuals who were terminally ill/mentally incapacitated (n = 104) or unable to speak English (n = 87), 3005 of 4226 eligible individuals accepted to be interviewed (participation rate: 71.1%). All participants provided verbal informed consent, and written parental consent was obtained for participants aged 15–17 years. Ethical approval was received from the Human Research Ethics Committee of the University of Adelaide (H0972010).
Measures
Demographic characteristics
Basic demographic information was collected including age, gender and educational attainment. Participants provided self-reported height and weight, later converted into BMI (kg/m2).
ED symptoms
Questions used to assess the presence of ED symptoms were based on the diagnostic questions in the ED Examination (EDE) (Fairburn and Cooper, 1993), the gold standard clinical assessment schedule for EDs. Overvaluation of body weight/shape (a core diagnostic and clinical feature of EDs; Fairburn et al., 2003) was measured by having participants rate the importance they placed on their weight and/or shape in determining their self-evaluation from 0 (‘no importance’) to 6 (‘supreme importance’). As in previous research, a score equal or higher than 5 was used to indicate the presence of overvaluation (Mitchison et al., 2013). ED behaviours were identified as present if they occurred regularly (i.e. at least weekly) over the previous 3 months. Objective binge eating was assessed by asking participants if they regularly ate ‘an unusually large amount of food’ with an accompanying sense of feeling ‘out of control’. Purging was assessed by asking participants whether they regularly used laxatives, diuretics and/or self-induced vomiting to control their weight or shape. Extreme dieting was assessed by asking participants whether they regularly were on a ‘very strict diet’ or ‘hardly eating anything at all’ to control their weight or shape. A question was used to assess the presence of avoidant–restrictive food intake disorder (ARFID) pathology, which was added as an ED in the latest revision of the DSM-5 (American Psychiatric Association, 2013). Participants indicated whether they significantly restricted their eating for ‘other’ reasons including food dislike or fear of swallowing (but not for weight loss, medical or cultural reasons) and to the extent that it had resulted in significant weight loss, nutritional deficiencies or functional impairment.
Bullying (all participants) and sexual abuse (participants ≥18 years)
Lifetime bullying and sexual abuse were assessed with the following questions: ‘Have you ever been bullied at school or work’ and ‘In your lifetime, have you ever experienced any type of sexual abuse’. Response options for each question were ‘never’, ‘occasionally (1–3 times)’, ‘often (4–10 times)’, ‘frequently (>10 times)’ or refusal to answer. In this study, the response options of ‘occasionally’, ‘often’ and ‘frequently’ were merged to provide a dichotomous score for lifetime prevalence of bullying and sexual abuse. Participants who responded other than ‘never’ were also asked about their age when they were last bullied or abused and the duration of the most recent episode of bullying or abuse. Years since last episode were subtracted from participants’ current age to compute an ‘adulthood bullying/adulthood sexual abuse’ variable. Participants who responded other than ‘never’ to both bullying and sexual abuse questions were considered to have a lifetime history of both bullying and sexual abuse.
Health-related quality of life
The 12-item Medical Outcomes Study Short Form questionnaire (SF-12; Ware et al., 1996) was used to assess health-related quality of life. The SF-12 yields a physical health component summary score (PCS) and mental health component summary score (MCS). Items assess impairment in physical and mental health and the extent to which health status impairs important domains of functioning (e.g. occupational, social and other roles). The SF-12 is the most widely used measure of health-related quality of life (Sanderson and Andrews, 2002). Scores are transformed into T scores, with a mean value of 50 and standard deviation (SD) of 10, and higher scores indicate greater quality of life. The internal consistency estimate (Cronbach’s alphas) for the 12 items in this study was 0.87.
Identification of participants with eating and weight-related problems
Participants with ED symptoms were identified as those who endorsed at least one of the following symptoms: overvaluation of weight/shape, objective binge eating, extreme dieting, purging or avoidant–restrictive food intake. Obese participants were identified as those with a BMI ≥30 kg/m2. Underweight participants were identified as those with a BMI <18.5 kg/m2 (adjusted for age for participants <18 years).
Data analysis
Analyses were conducted using SPSS v.24. Data were weighted based on the correspondent sampling process and reweighted to the population distribution in the 2011 Australian Census. Covariates in all multivariate regressions and analyses of covariance (ANCOVAs) included age, gender, educational attainment and BMI (only in analyses of ED symptoms, not obesity or underweight). Insufficient numbers of participants reported ARFID symptoms to support analyses with ARFID as the dependent variable. Furthermore, insufficient numbers of participants were identified with a lifetime prevalence of sexual abuse and current underweight to support analyses with this group.
Chi-square analyses were used to determine the unadjusted lifetime prevalence of bullying and sexual abuse and assess differences between participants with and without current ED symptoms, obesity or underweight. Multivariate (adjusting for the covariates mentioned above) binary logistic regressions were employed to assess the effect of years since last bullying/sexual abuse episode, duration of last bullying/sexual abuse episode and adulthood bullying/sexual abuse on the likelihood to report current ED symptoms or to be obese or underweight. Additional multivariate binary logistic regressions were employed to assess whether lifetime bullying/sexual abuse/both increased the likelihood of participants reporting specific ED symptoms or being currently obese or underweight. Six multivariate analyses of covariance (MANCOVAs) were employed to test whether a history of bullying or sexual abuse had an additional adverse impact on the health-related quality of life (scores on the SF-12 PCS and MCS) of participants with current ED symptoms, obesity or underweight.
Results
Overall sample characteristics
Participants in the overall sample included 1527 (50.8%) females and 1478 males. Participants had an average BMI of 27.1 kg/m2 (SD = 6.0; range: 14.8–71.9 kg/m2) and an average age of 46.7 years (SD = 19.2; range: 15–100 years). Most participants had a trade qualification or tertiary certificate (39.1%) or no tertiary qualification (37.1%), with fewer than one in four having a university degree (23.8%). Within the total sample, 974 (32.7%) participants reported current ED symptoms, with 633 (21.1%) reporting overvaluation of weight/shape, 390 (13.0%) at least weekly objective binge eating, 163 (5.4%) at least weekly extreme dieting, 25 (0.8%) at least weekly purging and 12 (0.4%) ARFID-type food restriction. Regarding weight status, 694 (25.2%) were currently obese, and 74 (2.7%) were currently underweight.
Characteristics of bullying experiences
Table 1 presents the lifetime prevalence of bullying among people with current ED symptoms, obesity or underweight.
Self-reported lifetime prevalence of bullying and sexual abuse among participants with ED symptoms and high and low weight.
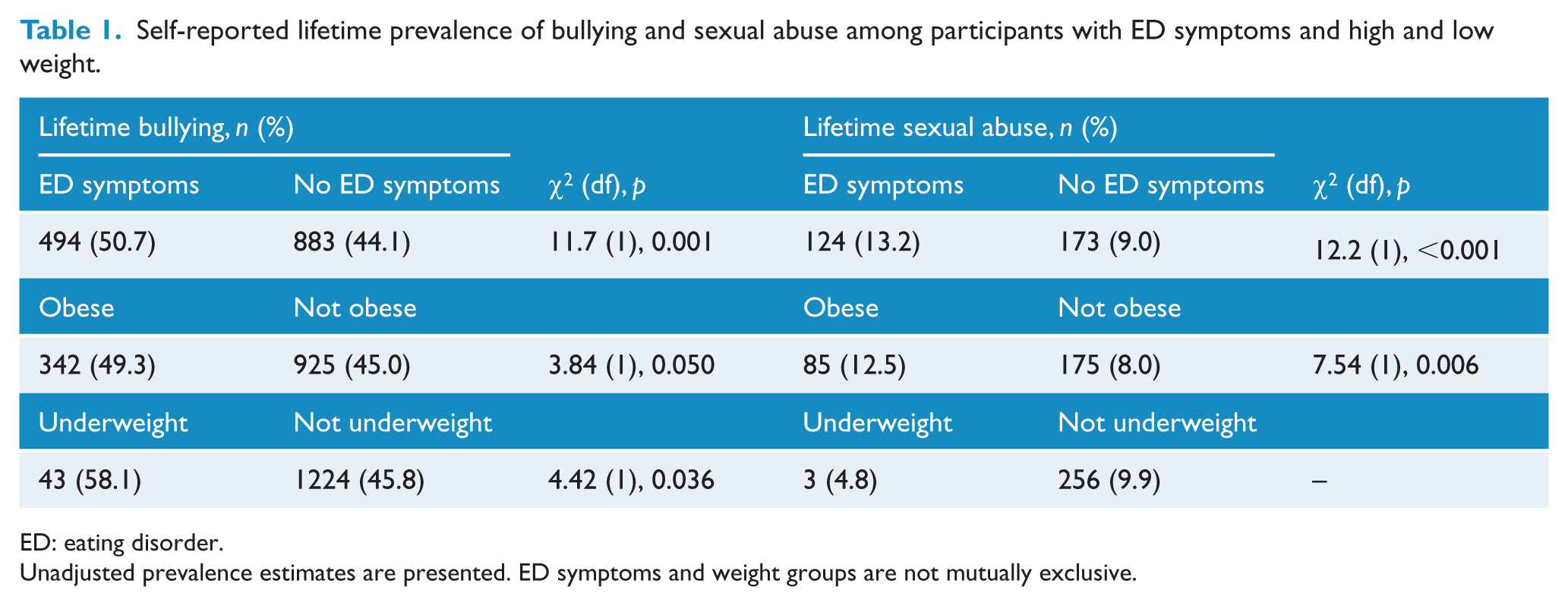
ED: eating disorder.
Unadjusted prevalence estimates are presented. ED symptoms and weight groups are not mutually exclusive.
Participants with ED symptoms
Roughly half of the participants with current ED symptoms reported being bullied in their lifetime and were 15% more likely to have been bullied than participants without ED symptoms. Five (1.0%) participants could not remember the last age they were bullied. For the remaining participants, the median age of the most recent bullying episode was 24.2 years (SD = 14.7; range: 5–72 years). The median number of years since the last bullying episode was 9.3 (SD = 17.2; range: 0–75 years ago). The median duration of the last bullying episode was 6 months (SD = 2.9 years; range: 1 day to 55 years). Adulthood bullying was reported by 37.0% of participants with ED symptoms. Years since bullying (p = 0.260), duration of last episode (p = 0.446) and adulthood bullying (p = 0.361) were not associated with the likelihood to endorse current ED symptoms.
Participants with weight problems
Roughly half of the obese and over half of the underweight participants reported being bullied in their lifetime, and both groups had an increased likelihood of having been bullied compared to other participants. Information on the age last bullied was not available from four (1.0%) obese participants. For the remaining participants, the median age of the most recent bullying episode was 15.0 years for obese (SD = 14.7; range: 5–72 years) and 14.1 years for underweight (SD = 8.3; range: 8–60 years) participants. The median number of years since the last bullying episode was 22.0 (SD = 18.9; range: 0–77 years ago) for obese participants but 5.1 years (SD = 12.0; range: 0–64 years ago) for underweight participants. The median duration of the last bullying episode was 5.5 months (SD = 3.9 years; range: 1 day to 55 years) for obese participants and 5.5 months (SD = 1.1 years; range: 1 day to 4 years) for underweight participants. Adulthood bullying was reported by 34.4% of obese and 24.5% of underweight participants. Years since bullying (p = 0.187; p = 0.769), duration of last episode (p = 0.957; p = 0.339) and adulthood bullying (p = 0.350; p = 0.108) were not associated with the likelihood to be currently obese or underweight, respectively.
Characteristics of sexual abuse experiences
Table 1 also presents the lifetime prevalence of sexual abuse among participants with current ED symptoms, obese participants and underweight participants.
Participants with ED symptoms
Participants with ED symptoms were 47% more likely to report a history of sexual abuse. Three (0.4%) participants did not state the last age they were abused. Of the remaining participants, the median age of the last sexual abuse episode was 14.0 years (SD = 8.8; range: 3–52 years). The median number of years since the last sexual abuse episode was 28.0 years (SD = 16.9; range: 0–69 years). The median duration of the last episode of sexual abuse was 2 days (SD = 3.4 years; range: 1 day to 20 years). Of those who reported a history of sexual abuse, 37.5% had experienced sexual abuse in adulthood. Years since sexual abuse (p = 0.068), duration of sexual abuse (p = 0.278) and adulthood sexual abuse (p = 0.756) were not significantly associated with the likelihood of endorsing current ED symptoms.
Obese and underweight participants
Obese participants were also more likely to have a lifetime history of sexual abuse. This was not the case for underweight participants, with too few underweight participants having a history of sexual abuse to support further analyses. Two obese participants could not remember the age they were when they were last sexually abused (0.3%). Of the remaining obese participants, the median age of the last sexual abuse episode was 14.0 years (SD = 9.0; range: 3–56 years). The median number of years since the last sexual abuse episode was 36.0 years ago (SD = 17.7; range: 1–70 years). The median duration of the last episode of sexual abuse was 1.8 months (SD = 4.2 years; range: 1 day to 20 years). Years since sexual abuse (p = 0.239), duration of the last episode of sexual abuse (p = 0.078) and adulthood sexual abuse (p = 0.06) were not associated with the likelihood to be currently obese.
Lifetime bullying/sexual abuse and current eating and weight-related problems
The results of the multivariate logistic regressions for the effects of lifetime bullying and sexual abuse on current ED symptoms (binge eating, extreme dieting, purging, overvaluation of weight/shape) and weight problems (underweight, obesity) are presented as odds ratios (ORs) in Table 2. Each regression was adjusted for possible confounding effects of age, gender and education, and the regressions for ED symptoms also adjusted for BMI. As can be seen, lifetime bullying and sexual abuse were each separately associated with increased likelihood to be currently engaging in extreme forms of dieting and to be obese. Lifetime bullying was additionally associated with an increased likelihood to purge and overvalue weight/shape. Lifetime sexual abuse was additionally associated with a decreased likelihood to be currently underweight and an increased likelihood to binge eat. Finally, having experienced both bullying and sexual abuse was associated with an increased likelihood for all ED behaviours (binge eating, extreme dieting, purging) but not overvaluation of weight/shape nor obesity or underweight.
Risk for eating disorder symptoms, obesity and underweight associated with lifetime bullying and sexual abuse.
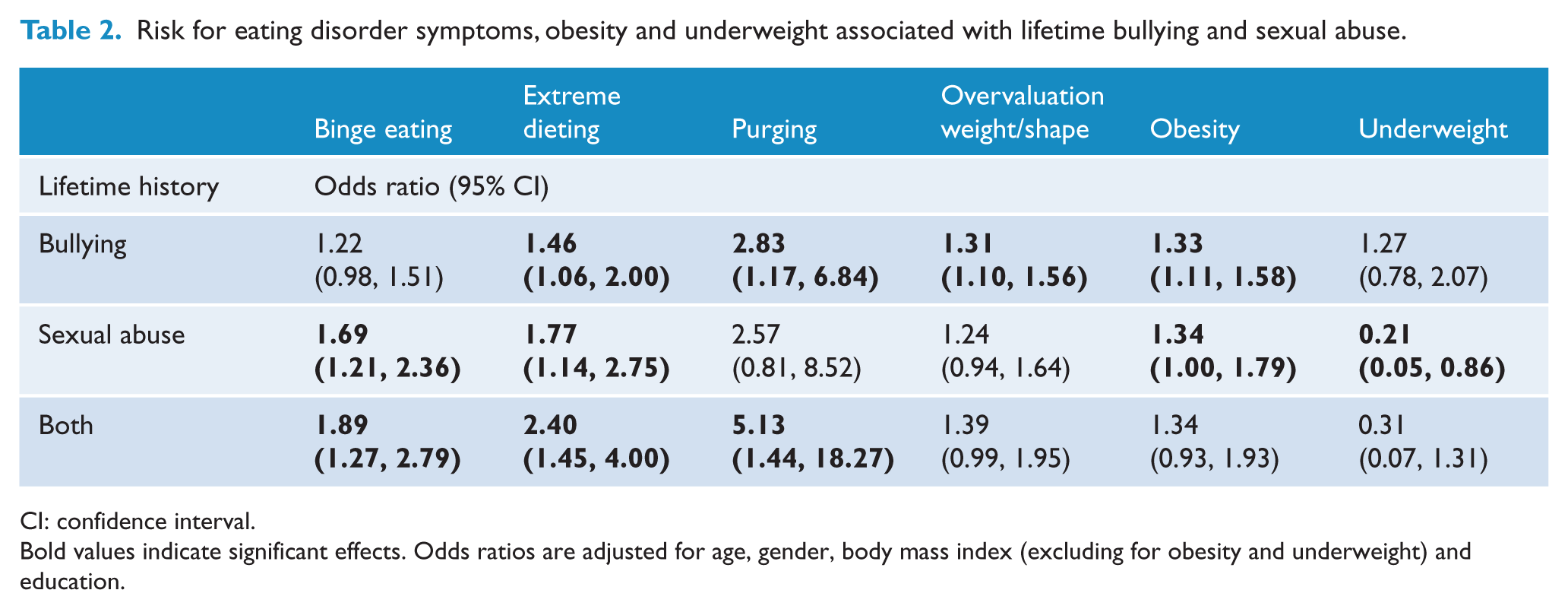
CI: confidence interval.
Bold values indicate significant effects. Odds ratios are adjusted for age, gender, body mass index (excluding for obesity and underweight) and education.
Health-related quality of life impairment associated with lifetime bullying/sexual abuse prevalence in participants with eating and weight-related problems
The results of the MANCOVAs that assessed the effects of bullying and sexual abuse, separately, and their interaction with ED symptoms and weight problems on health-related quality of life are presented below. In the overall sample, MCS and PCS were lower among those with a lifetime history of bullying or sexual abuse. Furthermore, ED symptoms were associated with lower MCS, and obesity was associated with lower PCS. No differences in MCS and PCS were observed in underweight participants (data available from the authors on request).
Participants with ED symptoms
Table 3 presents the means and SDs of scores on the MCS and PCS within participants with current ED symptoms, obesity or underweight. A significant interaction between ED symptoms and lifetime bullying on MCS (but not PCS, p = 0.224) was observed, F(3, 924) = 4.33, p = 0.037, partial η2 = 0.002. While there was an adverse effect of a lifetime history of bullying on mental health-related quality of life among all participants relative to participants without a history of bullying, this effect was greater among participants with current ED symptoms (see Figure 1). No significant interactions were found between ED symptoms and a lifetime history of sexual abuse on MCS (p = 0.130) or PCS (p = 0.405).
Physical (PCS) and mental (MCS) health-related quality of life impairment associated with lifetime bullying and sexual abuse in participants with eating and weight-related problems.
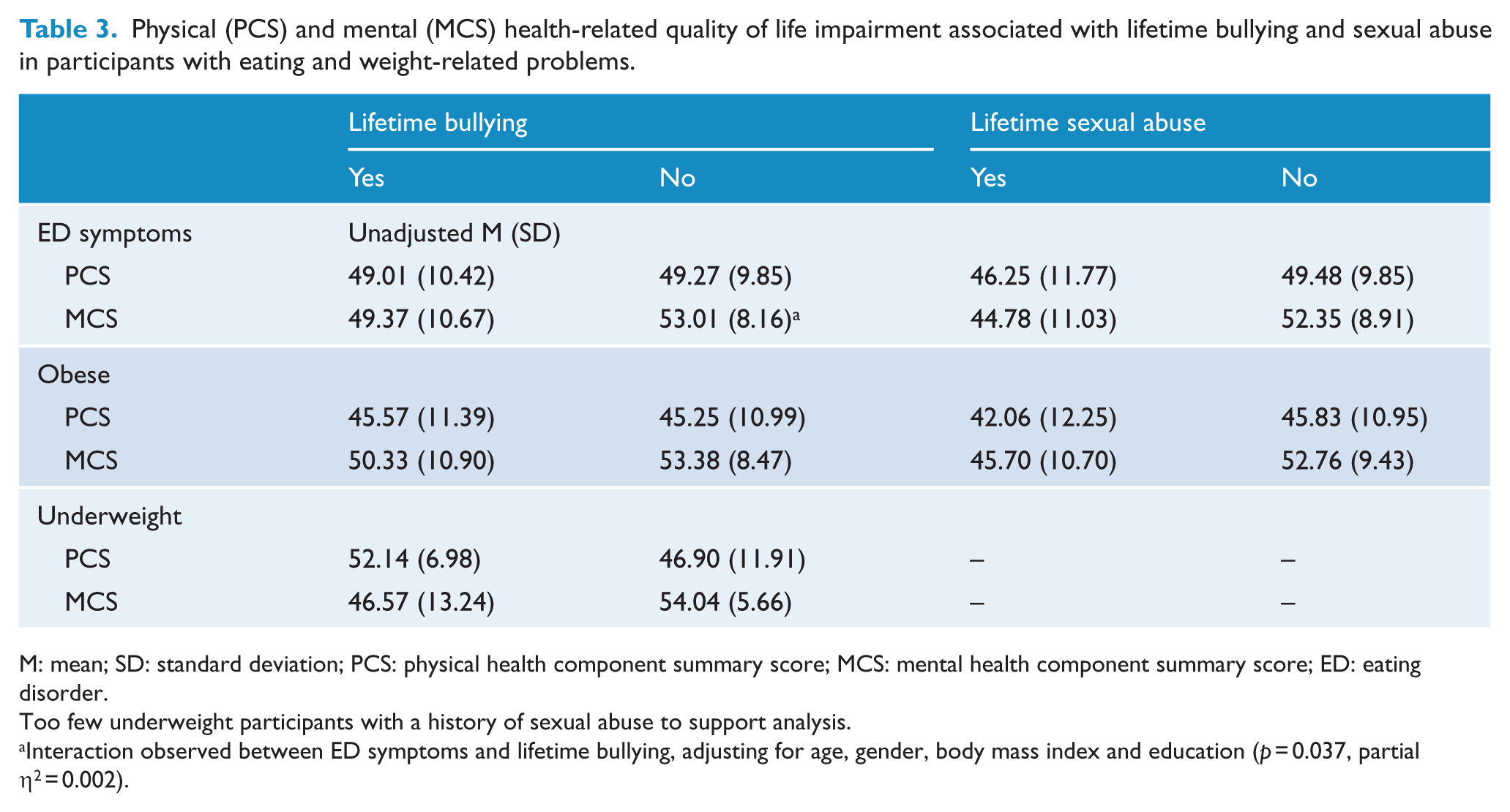
M: mean; SD: standard deviation; PCS: physical health component summary score; MCS: mental health component summary score; ED: eating disorder.
Too few underweight participants with a history of sexual abuse to support analysis.
Interaction observed between ED symptoms and lifetime bullying, adjusting for age, gender, body mass index and education (p = 0.037, partial η2 = 0.002).
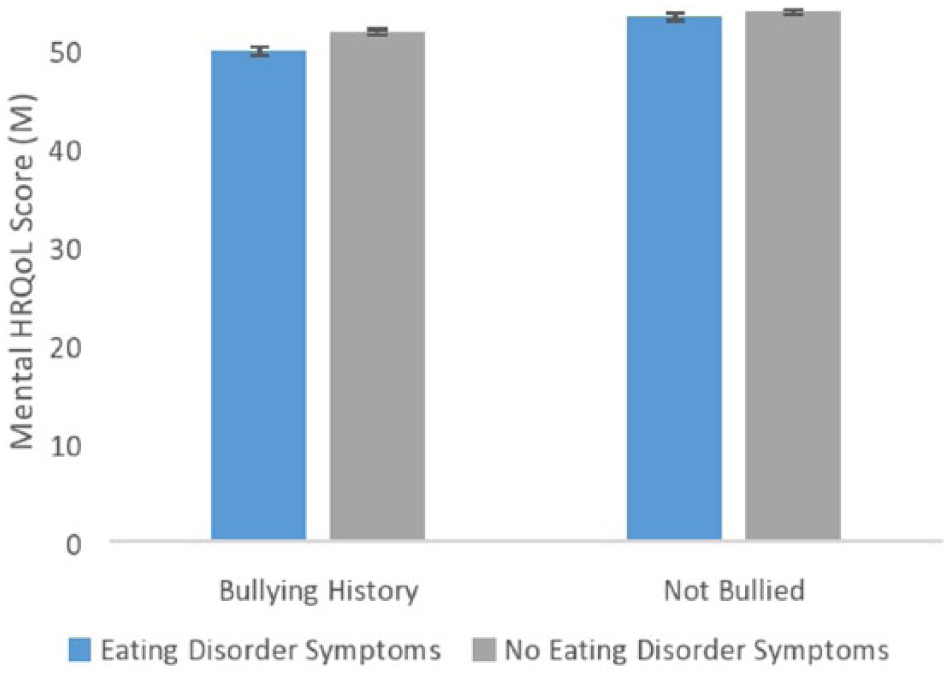
Mental health-related quality of life (HRQoL) scores among participants with and without current eating disorder symptoms and a history of bullying. An interaction was observed between bullying and eating disorder symptoms (p = 0.037, partial η2 = 0.002), indicating that while there was an overall adverse effect of lifetime bullying on mental HRQoL, this was greater among people with current eating disorder symptoms. Means and standard errors are adjusted for age, gender, body mass index and education.
Obese and underweight participants
No significant interactions were found between obesity status and a lifetime history of bullying or sexual abuse on MCS (p = 0.456; p = 0.628) or PCS (p = 0.643; p = 0.074), respectively. No significant interactions were found between underweight status and a lifetime history of bullying on MCS (p = 0.102) or PCS (p = 0.105).
Discussion
Risk factor research for EDs and obesity has tended to investigate these conditions separately, with different samples and methodologies, and in women, which has undermined recent efforts to uncover shared risk factors for eating and weight-related problems (Haines and Neumark-Sztainer, 2006). The primary aim of this study was to examine the extent to which lifetime prevalence of bullying, sexual abuse and their combination were associated with an increased likelihood to report current eating and weight-related problems, including specific ED symptoms, obesity or underweight. We found that participants who had reported previous experiences of bullying or sexual abuse were at increased risk for current ED symptoms and obesity, but that the pattern of risk differed depending on the adversity experienced. We also found that having experienced either bullying or sexual abuse, but particularly sexual abuse, added to the health impairment experienced by all participants. However, the effect on mental health impairment was uniquely greater among participants with ED symptoms who had experienced bullying, whereas all participants who had experienced sexual abuse, regardless of whether they also had current ED symptoms, had low mental health-related quality of life.
Evidence from numerous ED and obesity studies suggest that weight-related teasing may be a shared risk factor (Haines and Neumark-Sztainer, 2006). In this study, we found evidence in the same sample confirming that self-reported lifetime bullying was associated with an increased risk for both ED symptoms and obesity. Furthermore, our findings extend those from previous studies on ‘weight-related teasing’ (see review, Menzel et al., 2010), to demonstrate that general peer victimisation (including physical, verbal and relational bullying) and bullying that is not necessarily weight-targeted are associated with an increased likelihood for EDs and obesity. As far as we are aware, no study has examined sexual abuse as a shared risk factor for obesity and EDs, nor has sexual abuse typically been included in the discourse regarding shared risk factors for eating and weight-related problems (Haines and Neumark-Sztainer, 2006). We thus present here unique findings that provide evidence for the shared nature of self-reported histories of both bullying and sexual abuse as risk factors across eating and weight disorders.
The majority of research on both ED symptoms and sexual abuse has been conducted with female samples, owing to their higher prevalence among women. This study is thus fairly unique in its inclusion of males. In post hoc analysis, gender was not found to be a source of heterogeneity for the association between sexual abuse and any of the investigated ED symptoms (p value for interaction: >0.05 in all cases, data not shown), suggesting that the identified relationships are similar in men and women. However, the association between bullying and binge eating was modified by gender (p value for interaction = 0.001), with a history of bullying associated with greater odds for binge eating in women (OR = 1.94; 95% confidence interval [CI] = 1.37, 2.75), but not men (OR = 0.80; 95% CI = 0.52, 1.24). More research is required to investigate why males are less likely to develop binge eating in the context of a history of bullying, particularly given that no gender differences were observed in the relationship between bullying and other ED symptoms.
Differences emerged in the specific ED symptoms that were associated with bullying versus sexual abuse, highlighting the need to examine specific types of adversity separately. While bullying led to the development of maladaptive goal-directed behaviour (i.e. extreme dieting and purging in the pursuit for thinness) for participants in this study, sexual abuse led to the development of binge eating, which may represent a form of emotional avoidance (Fairburn et al., 2003). A possible explanation for differences in these apparent coping mechanisms comes from studies that have demonstrated the relatively popular and powerful personalities of people who bully, whom others may aspire to emulate or otherwise gain popularity with (Espelage and Holt, 2001). Thus, children (and potentially adults) may attempt to ‘escape’ peer victimisation through the use of extreme weight loss methods and conformation to popular ideals. On the other hand, escape from sexual abuse may be perceived to be relatively more difficult and thus may be more likely to lead to self-soothing coping and inoculating strategies, such as binge eating. For instance, several studies have drawn a link between misuse of substances as a maladaptive coping mechanism in sexual abuse/assault victims (Ullman et al., 2014). Less research has assessed the link with binge eating, which may represent an alternative and more readily available ‘substance’ for emotional avoidance. The finding that participants in our study had experienced their last episode of bullying or abuse two decades ago indicates that once developed, such maladaptive coping strategies are likely to be maintained without intervention.
Our finding of a long-lasting adverse effect of a history of bullying is at odds with a prospective study that found bullying to be a significant risk factor for the later onset of ED symptoms during adolescence but not after age 19 (Copeland et al., 2015). A possible explanation is that the risk for ED symptoms in participants who are in their mid-20s, the upper age of the former longitudinal study, is already high (Mitchison et al., 2014) and thus additive effects of bullying may not be observed during this critical time of increased weight/shape salience. However, it is possible that bullying may exert a lasting effect, such that while people may be equally likely to have ED problems during young adulthood, this ‘risky period’ may be extended for participants with a history of bullying.
Interestingly, the hypothesised additive effects of a combined prevalence of bullying and sexual abuse were only realised for ED behaviours in this study. It is surprising that there was no significant association between obesity and a combined reported history of sexual abuse and bullying, given that each of these adversities were associated with obesity when considered separately. The increased use of extreme weight control behaviours among participants who had experienced both bullying and sexual abuse may explain this finding. On the other hand, the risk for binge eating was also higher, which is usually, but not always, associated with weight gain. Finally, the lower number of participants reporting both bullying and sexual abuse may have reduced the power to detect this effect. Thus, further research into the multiplicative effect of multiple adversities on ED symptoms and weight status is required to explain these findings.
Physical appearance is the most common reason for bullying among adolescents (Frisen et al., 2007), and experiencing this type of peer victimisation may threaten body self-esteem and increase the drive to pursue thinness. Our study suggests that bullying may play a particularly important role in the development of EDs. We found that bullying was associated with an increased risk for core cognitive (i.e. overvaluation of weight/shape) and behavioural (i.e. dieting and purging) ED symptoms and was also associated with greater deficits in mental health functioning in participants with ED symptoms. The literature examining the link between bullying and EDs to date has been limited by a lack of prospective analyses, exclusion of males and an overreliance on crude measures of bullying, often also confined to the assessment of weight-related teasing. Future research addressing these limitations would be welcome and should lead to initiatives to address bullying in public health interventions for weight and EDs. Furthermore, given the increasing concern regarding cyberbullying and youth mental health, it will also be important to investigate the relationship between bullying and EDs/obesity in a social media context, which is highly laden with personal and idealised images of bodies (Fardouly et al., 2015; Perloff, 2014).
This study has several strengths and limitations. Notable strengths include the large population-based sample, use of interviews, inclusion of males and females and a large age range, the measurement of multiple adversities and the measurement of problems across the eating and weight spectrum. Limitations include the retrospective recall of bullying and sexual abuse and leaving the definition of bullying and sexual abuse to the participant. Due to individual variation in personal definitions of adversities such as bullying and sexual abuse, it is preferable to provide participants with a standard definition prior to asking questions about prevalence. Another limitation is the self-report of height and weight, which, due to the sensitivity about weight among individuals with EDs and high and low weight, may have contributed to missing and/or skewed data. Anthropometric measures are superior, although often infeasible in such large-scale population studies. Finally, other psychiatric comorbidity was not assessed, which precluded analyses that would further determine the independent relationship between victimisation and disordered eating across the weight spectrum.
Several implications may be drawn for public health and clinical practice. It will be important to ensure that services and care providers involved with children, adolescents and adults with a history of bullying or sexual abuse are aware of the increased risk for body image problems and maladaptive eating and weight loss behaviours. This will facilitate monitoring of symptoms and timely referral to appropriate services where needed. Also, given the poorer mental health of individuals with ED symptoms who suffer these adversities, it is important that clinicians treating EDs assess for, and factor into treatment decisions and prognostic calculations, the presence of a history of bullying and abuse. While increased risk following experiences of sexual abuse and bullying may not be specific to EDs (Chen et al., 2010; Striegel-Moore et al., 2002), treatment-seeking and access to support services specialising in EDs may be lower compared to services for anxiety, mood and trauma (Hart et al., 2011; Swanson et al., 2011). Finally, our findings provide support for the implementation of universal prevention programmes that target bullying, in both school and work contexts, as a vehicle to reducing risk for the later development of EDs across the weight spectrum. Most participants reported adversities that were confined to their childhood. Thus, introducing effective prevention strategies during childhood during the time that these adversities occur, to either reduce the likelihood of these adversities or increase resiliency against the deleterious after-effects of these adversities, is an important piece to the solution. Work has begun in this area and promising results have been found in the reduction in weight and shape concerns, weight-related teasing and average BMI (Wilksch et al., 2015). On the other hand, given that a significant proportion of participants reported adulthood bullying, adulthood resiliency and anti-bullying programmes, particularly in the workplace, may also be very useful at reducing disordered eating and weight gain.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.H. receives/has received sessional fees and lecture fees from the Australian Medical Council, Therapeutic Guidelines publication and New South Wales Institute of Psychiatry; royalties/honoraria from Hogrefe and Huber, McGraw Hill Education, Blackwell Scientific Publications, BioMed Central and PLOS Medicine; and she has received research grants from the NHMRC and ARC. She is Deputy Chair of the National Eating Disorders Collaboration Steering Committee in Australia (2012–) and Member of the ICD-11 Working Group for Eating Disorders (2012–) and was Chair Clinical Practice Guidelines Project Working Group (Eating Disorders) of RANZCP (2012–2015). She has prepared a report under contract for Shire Pharmaceuticals in regard to BED (July 2017). All views in this paper are her own. S.T. is the Chair of the Shire Australasian BED Advisory Committee. He has received both research grants and travel grants from Shire and has received consultancy fees for both commissioned reports and speaking engagements. He is also in receipt of royalties from McGraw Hill for contribution to text books.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Macquarie University Research Fellowship (DM).