
Abstract
Good collaboration between private psychiatrists and other elements of the mental health sector (including state-funded mental health services, general practitioners [GPs] and non-government organizations) [1], is in everybody's best interests. At present, it is limited by several barriers including differences in financial incentives, service cultures and treatment approaches, as well as communication difficulties, lack of clarity regarding roles and responsibilities and varying perceptions of others' expertise [2], [3]. There is increasing concern that this suboptimal collaboration can militate against positive outcomes for consumers and carers, although this has not been well studied empirically [4], [5].
In future, the role of psychiatrists may involve greater emphasis on consultation and shared care with GPs and others [6]. If this is so, collaboration will need to improve. Effective collaboration requires appropriate remuneration, commitment from clinicians (and managers), clear communication processes that respect consumer confidentiality, and an understanding on the part of each sector of the service context of the other sector [7]. There are published examples of initiatives that have successfully improved collaboration through strategies (e.g. colocation of public and private providers) [8], but they are rare.
The Public and Private Partnerships in Mental Health Project (Partnership Project) was funded by the Commonwealth Department of Health and Aged Care in 1999. It aimed to improve linkages between public sector mental health services and private psychiatrists and produce better outcomes for consumers aged 18 years or more. It was a joint initiative of two public sector organizations, St Vincent's Mental Health Service (SVMHS) and St George's Aged Psychiatry Service (SGAPS), and a private psychiatric hospital, The Melbourne Clinic (TMC). It was overseen by a steering committee which included representation from these organizations and consumers and carers from both sectors [9].
The Partnership Project was fully operational from September 2000 to August 2002. It served Melbourne's inner urban east, an area with a high coverage of private psychiatrists per capita, but very few shared care arrangements [10]. The Project had two major components: a Linkage Unit; and a series of trial item numbers which allowed private psychiatrists to be remunerated for activities other than direct patient care (expanded roles). Each is described in more detail later.
The Linkage Unit was designed to: (i) improve service delivery through collaborative arrangements for individual consumers; and (ii) promote systems-level and cultural change necessary for sustaining collaboration between the public and private sectors. It offered a twoway communication flow, enabling private psychiatrists to work with public sector services and providing information for SVMHS and SGAPS clinicians seeking a private psychiatrist for a particular consumer. It also facilitated linkages between mental health services (both public and private) and GPs and non-government organizations, and supported formal shared care arrangements between public sector clinicians and private psychiatrists and between public sector clinicians and GPs. It was responsible for raising awareness, supporting participating psychiatrists, and promoting cultural and structural change. It was also responsible for facilitating the expanded roles for private psychiatrists. Linkage Unit clinicians were located in inpatient units and community clinics at SVMHS and SGAPS, and regularly attended meetings at other facilities, including TMC. The Linkage Unit had a facilitating role, and did not directly coordinate care. This was to ensure that any improvements in collaboration could be sustained once the Partnership Project ceased. All referrals were directed through the existing duty/triage processes, according to agreed protocols. The Linkage Unit was staffed by the Project Manager (1.0 FTE) at SVMHS, a Linkage Unit psychiatrist (0.5 FTE) at SVMHS, Linkage Unit clinicians at SVMHS's Clarendon and Hawthorn Clinics (1.0 FTE each) and SVMHS's Inpatient Unit (0.5 FTE), and a Linkage Unit project officer at SGAPS (0.5 FTE).
Under the expanded roles component of the Partnership Project, private psychiatrists who satisfied specified requirements could bill the Project for their participation in the following activities, according to a schedule of item numbers that, like HIC item numbers, were based on duration and location of service [11], [12].
Supervision and training: Private psychiatrists provided supervision and training for staff from SVMHS and local non-government agencies, and ran cognitive behavioural therapy (CBT) workshops and clinical discussion groups (CDGs) for GPs. Case conferencing: Private psychiatrists took part in case conferences with others sharing the care of a given consumer, as well as the consumer him/herself and his/her carer(s). Secondary consultation: Private psychiatrists provided secondary consultations for GPs from two local Divisions of General Practice and for staff of SVMHS and SGAPS. These secondary consultations operated under different models (e.g. the psychiatrist seeing the consumer and then being available for contact from the GP or other mental health professional to assist in the consumer's ongoing care, and the psychiatrist interviewing a consumer with the GP or other mental health professional in his/her practice environment in order to provide training in interviewing techniques and skills in detection, diagnosis and treatment and then being available for subsequent provision of further advice).
We describe the evaluation of both the Linkage Unit and the expanded roles for private psychiatrists, focusing on the impacts and outcomes of each.
Method
The use of triangulation, or ‘the combination of a number of methodologies in the study of the same phenomenon’ [13], [14], was considered essential in evaluating an initiative as complex as the Partnership Project, and quantitative and qualitative data from several sources were used. It should be noted that the evaluation process evolved with the Partnership Project, and some components described in an earlier methodology paper [15] were modified or excluded, and others added, for reasons of relevance and practicality. In particular, components that required direct access to information about consumers' service use and outcomes presented logistical difficulties because of the introduction of a new case register system during the course of the Project.
Data from the Linkage Unit
A purpose-designed database provided consumer-level information on episodes of collaborative care facilitated by the Linkage Unit. Descriptive analyses of these data were conducted, and they are presented as frequencies or percentages.
Data on the expanded roles for private psychiatrists
Billing data from the Partnership Project provided de-identified information on the uptake of the expanded roles by private psychiatrists during the 2 years of the Project. Again, descriptive analyses were conducted, presented as frequencies or percentages.
Health Insurance Commission (HIC) data
The above billing data were complemented by de-identified HIC data on the traditional fee-for-service activities of participating private psychiatrists in the year prior to the Partnership Project, and in the 2 years of the Project. Psychiatrists consented to the HIC releasing this information when they agreed to participate in the expanded roles. Information was available on the services rendered by these psychiatrists, as well as their associated costs in terms of benefits paid. The costs of the expanded roles to the Commonwealth Government as payer were considered by comparing the HIC costs in the baseline year prior to the Project with the combined HIC and Project billing costs in each of the two Project years. For the purposes of analysis, all costs were deflated to the baseline year for comparability, using health price deflators published by the Australian Institute of Health and Welfare [16]. Mean values were imputed for those psychiatrists who did not bill the HIC in a given year (two in each year).
Consultations with key stakeholders
Consultations were undertaken with key stakeholders, in order to examine experiences with the Linkage Unit and with the expanded roles for private psychiatrists from a range of perspectives. Semistructured interviews were conducted with 36 key informants (providing representation from: the steering committee; the Partnership Project management; the Linkage Unit; SVMHS, SGAPS and TMC management and staff; and participating private psychiatrists and GPs). The majority of key informants had been interviewed at the Project's commencement or during its implementation, and were therefore able to consider changes over time that could be attributed to the Project. Additional information was sought from a carers' forum, attended by over 40 carers of people in receipt of public sector mental health care, and from a meeting of five public and three private sector psychiatrists. The original evaluation design called for consumer/carer and provider focus groups, but these proved difficult to arrange, and the forum and the meeting were viewed as an acceptable substitute.
Most consultations were conducted by telephone or face-to-face, but a minority of stakeholders responded in written form. Information from each consultation was recorded as interviewer notes, and a written summary of each interview was prepared shortly after it had occurred. Broad themes were identified from stakeholder responses, and individual responses were classified according to these themes. Two of the authors, JL and BM, conducted the consultations. A third, JP, undertook the analysis, referring to JL and BM for points of clarity, where necessary. JL and BM then reviewed the analysis. The analysis was conducted by hand, with consultation text coded and sorted into themes.
Case studies
The Linkage Unit clinicians were asked to provide case studies that exemplified the work of the Linkage Unit, showing the range of its activities and demonstrating both achievements and difficulties. In total, 25 case studies were provided to illustrate the uniqueness and complexity of the work of the Linkage Unit, both in terms of level of consumers' need and numbers of providers involved in their care. The case studies are described in full in the Partnership Project's final evaluation report [17], but for reasons of brevity, only six are presented here. This subset was selected on the basis that they represented the common features of the complete set. The original evaluation design included an examination of routinely collected outcome data, but, as noted earlier, the introduction of a new case register system during the course of the Project created issues regarding data availability and quality. The case studies, while not a substitute for the originally planned outcome data, provide valuable information about the impacts of the Partnership Project for consumers.
Results
Evaluation of the Linkage Unit: improving collaborative arrangements for individual consumers
A total of 224 episodes of collaborative care were facilitated by the Linkage Unit for 218 consumers (six consumers had two episodes, and the remainder had one). Table 1 summarizes the socio-demographic and clinical characteristics of these consumers. Fifty-three percent of these consumers were female. Forty-two percent were aged between 25 and 44. The majority (97%) spoke English as their primary language (i.e. the language they spoke at home, which may have impacted on their ability to communicate with providers). Only a minority (17%) had private health insurance. Half were in receipt of a pension or benefit. Almost one-third (30%) had a history of private psychiatric treatment. The primary diagnoses recorded for each episode were most commonly depressive disorders (44%) or psychotic disorders (39%).
Characteristics of consumers undergoing episodes of collaborative care facilitated by the Linkage Unit
Table 2 describes the 224 episodes in which there was some level of collaboration. The majority of these episodes of collaborative care (88%) involved internal referrals from staff at SVMHS or SGAPS, either directly through the Linkage Unit (e.g. where the case was referred at a team meeting or handover at the suggestion of the Linkage Unit clinician), or from elsewhere in these organizations, but a proportion (12%) were referred by private psychiatrists or GPs. At both SVMHS and SGAPS, these referrals involved collaborative care arrangements with a mix of inpatient and community staff. Most commonly, the anticipated nature of the collaboration involved care predominantly being provided in the private sector or medium- to longterm shared care. A range of collaborative care arrangements arose, varying in terms of whether they were new or had existed previously, and in terms of the roles of the participating providers.
Characteristics of episodes of collaborative care facilitated by the Linkage Unit
Role of the Linkage Unit in facilitating collaborative care arrangements
In total, the Linkage Unit was actively involved in facilitating 83 episodes of collaborative care, and was aware of but not involved in a further 120 collaborative episodes (the Linkage Unit's role in the remaining 11 was unclear). It is important to consider this involvement over time, as it relates to the intention of the Linkage Unit to facilitate collaboration in a manner that ensured sustainability beyond the life of the Partnership Project. Whereas the Linkage Unit was actively involved in facilitating 85% of all collaborative arrangements that were put in place in the first 6 months of the Project, this reduced to 52% and 17% in the second and third 6 months, respectively, and by the final 6 months it was only involved in facilitating 12%.
Experiences of providers with collaborative care arrangements
Providers who were consulted during the key informant interviews were generally positive about the Linkage Unit's role in brokering coordination of care. Participating GPs, for example, noted that the Linkage Unit led to improved communication with the public sector, and in particular with case managers. They also acknowledged that the Linkage Unit facilitated their access to private psychiatrists, but indicated that the system was still imperfect. For example, one GP stated: ‘I find that I can get an opinion from a private psychiatrist more easily. Through the Linkage Unit it is now far easier to organize that’ but countered this with the observation that ‘I still find it takes a long time to get an initial appointment for patients requiring ongoing psychiatric management [by a private psychiatrist].’ Access to public sector services was generally regarded as improved for private psychiatrists, although it was acknowledged that private psychiatrists still have difficulties when trying to get their patients admitted as inpatients to the public sector.
Outcomes and features of collaborative care for consumers
The selected case studies shown in Table 3 suggest that some of the collaborative arrangements were highly successful, with positive outcomes. Common features of collaborations that worked well included good multiway communication between all parties, sometimes involving innovative communication methods such as email, and clearly defined roles and responsibilities, including well-documented crisis plans. Joint attendance at assessment and treatment sessions by case managers, GPs and private psychiatrists were another hallmark of successful arrangements. Use of the formal protocols developed for transferring consumers from inpatient services at SVMHS and SGAPS to TMC or vice versa was also successful, enabling services to work smoothly together in the best interests of the consumer. When private psychiatrists were able to deviate significantly from their usual mode of practice (e.g. visiting consumers at home or providing secondary consultation), positive outcomes often ensued. Private hospital admissions were easier to arrange when the private psychiatrist was working from facilities with inpatient services, such as TMC.
Selected case studies of collaborative care arrangements
Some of the case studies demonstrated features that militated against good collaboration. For example, where communication was poor (e.g. if private psychiatrists did not respond to the case manager or public staff did not initiate contact with private sector), transfer of care was delayed or where the mode of service delivery was not feasible, progress was difficult.
The generally positive findings of the case studies were supported by the views of key informants, many of whom felt that the Linkage Unit had direct impacts for consumers and their families. One key informant reported that feedback from families who had been referred to the Linkage Unit had been ‘excellent’. Another noted that ‘the benefit to the family of shared care arrangements are quite substantial–the public system allows much greater involvement of carers and provides better information and support; the benefit of private psychiatrists taking on a client requiring more extensive psychotherapy is clear.’
However, stakeholders observed that public and private partnerships in care provision are still not the norm. At the carers' forum, only one carer reported that her relative was currently involved with both the public sector and a private psychiatrist; the majority said that they had some experience with private psychiatrists in the past but that these psychiatrists had ‘washed their hands of them’. Most participants felt that their relatives were being well catered for in the public sector; though some felt that access to the private sector would provide more ‘options for treatment.’
Evaluation of the Linkage Unit: promoting systems-level and cultural change
At a systems level, the Linkage Unit had major impacts. Linkage Unit personnel reported systemic changes that had occurred to facilitate better co-ordination of care, such as formalizing procedures for identifying and contacting private psychiatrists and GPs of public sector consumers. As an example, the inpatient unit at SVMHS now has a formal process whereby private providers are identified on admission and discharge checklists, and contacted. This has the support of senior medical and nursing staff in the inpatient unit.
Linkage Unit personnel also reported major changes in the level of consciousness about working with the private sector on the part of SVMHS and SGAPS providers. One key informant described this change as a ‘paradigm shift’, noting that private psychiatrists are now seen as an option at multiple points in working with a given consumer (e.g. at the point of triage, at discharge, and in ongoing shared care). Work with the Crisis Assessment and Treatment Service (CATS) at SVMHS and the Aged Psychiatry Assessment and Treatment Team (APATT) at SGAPS were cited as major successes, where a few successful interactions between team members and private psychiatrists altered the way in which they operate. Previously, they had a narrow focus on working with consumers in the short term; now they are inclined to involve private psychiatrists in ongoing care.
Evidence of cultural change was also reported elsewhere in the public sector. For example, one key informant reported anecdotally that at ward rounds and case discussions ‘… people are asking the questions about private psychiatrists… and whether they've been contacted. It's great feedback because it means that the ideas are swirling around.’ Another noted: ‘[There's]… more talk in clinical reviews and handovers like “this is a good GP that you might want to use” and “we know this psychiatrist who's happy to consider bulkbilling.” ‘As one of the Linkage Unit personnel put it: ‘It's… creating awareness… planting seeds in people's minds: and some of it might be in arid, dry, rocky soil and some of it might be in really lush, green … What's worked is that people have agreed to take on some of the roles.’ Another Linkage Unit respondent reiterated that ‘the Project has definitely contributed to raising awareness… so there is an expectation that private service provision is considered on a day-to-day basis for all patients', but cautioned that ‘the extent of practice change is unknown.’
Evaluating the expanded roles for private psychiatrists
Strategic efforts were made to recruit private psychiatrists to participate in supervision and training, case conferencing and secondary consultation. Recruitment activities included: personal visits by the Partnership Project psychiatrist; information sessions; recruitment letters; and the development and distribution of an information kit. As a result of these recruitment activities, 32 private psychiatrists consented to provide supervision and training, case conferencing and secondary consultation under the expanded roles. Four did not charge the Project for undertaking these activities. Twenty-eight billed the Project for a total of 555 h, with some billing for more than one type of activity. The total cost for these activities was $78 032.
Supervision and training were the most common, involving 16 psychiatrists and accounting for 432 h (78% of the total time) and $61 435 (79% of the total cost). The different supervision and training models reached a significant number of recipients. For example, 37 GPs took part in the CBT workshops, and 22 GPs participated in the CDGs.
Case conferencing and secondary consultation were less common among the private psychiatrists. Case conferencing activities involved eight psychiatrists and accounted for 38 h (7% of the total time) and $4925 (6% of the total costs). Eleven psychiatrists participated in secondary consultation, accounting for 85 h and $11 672 (15% of both the total time and costs).
Cost to the Commonwealth Government
Consideration was given to whether the costs of the expanded roles (specifically, direct payments to psychiatrists) were offset by reductions in HIC expenditure on professional services provided by participating psychiatrists.
Figure 1 shows the costs of direct payments to psychiatrists for participating in the expanded roles, combined with the benefits paid by the HIC to these psychiatrists for professional services between 1 September and 31 August in each of the 2 years of the Partnership Project.
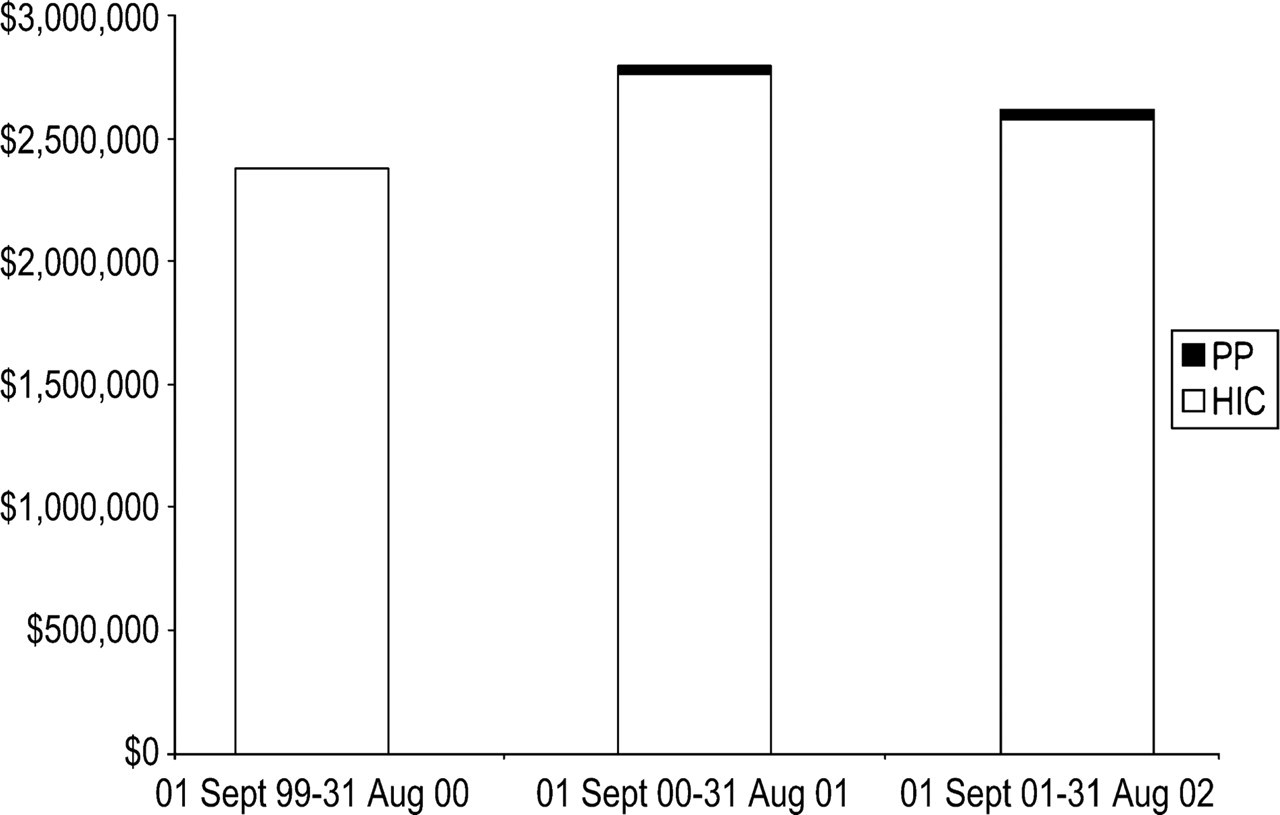
Health Insurance Commission and Partnership Project services billed by private psychiatrists, 1 September 1999–31 August 2002.
In the baseline year, the total Commonwealth Government expenditure on participating private psychiatrists was $2 377 318, solely comprising benefits from the HIC. In 2000/2001, the total was $2 795 675, comprising $32 492 (1%) in payments from the Partnership Project, and $2 763 183 in benefits from the HIC. In 2001/2002, the total was $2 616 996, accounted for by $42 613 (2%) in payments from the Project and $2 574 383 in benefits from the HIC. Commonwealth expenditure on private psychiatrists' participation in the expanded roles was not associated with a commensurate reduction in benefits paid by the HIC.
Experiences of participants
Most psychiatrists who provided supervision and training found the role extremely satisfying, appreciating the opportunity to do something different from their usual clinical work. They reported an increase in their own knowledge and skills, using descriptors such as ‘a wonderful experience of sharing ideas and working as a group’; ‘rewarding’; ‘challenging’; and ‘[providing]… something that was not attainable in the private sector.’ Many said they would undertake supervision and training with GPs and public sector mental health workers again, given the opportunity. They felt that the various models allowed them the flexibility to change their approach to cater for such eventualities as lower than expected numbers or differing levels of understanding regarding mental health when necessary.
Some key informants commented on broader impacts, noting that the supervision and training had improved ‘mutual professional respect’ and led to new referrals and shared care arrangements between private psychiatrists and both the public sector and GPs. Many psychiatrists made comments such as: ‘My working relationship with GPs has been improved… I'm back in touch with them and getting important feedback about their current working situation’; ‘A number of people I see privately now come from the staff I supervised… they know me as a person to refer… clients to.’ General practitioners too, reported that they had a better knowledge of referral sources as a result of participating in supervision and training sessions, and were more likely to use these referral sources. However, not everyone was positive about improving relationships. Some felt they already had strong existing relationships; others felt that although communication had improved, it was too early to judge whether this would have flow-on effects in terms of referrals and shared care; still others felt that increasing referrals was not a sensible goal for supervision and training activities, because it would just add to their already busy workload.
The psychiatrists offered some criticisms, however. One psychiatrist commented that when the role involved conducting assessments alongside a GP, he was concerned that the GP viewed this purely as a way of securing an assessment from a psychiatrist, rather than as a learning experience. Another observed that some referrals came from the public sector that were not appropriate: ‘for example, referrals requesting ongoing care came to me despite the fact that this was not what I was providing through the Project.’ A common theme was that where communication was good, secondary consultation worked; where it was poor, secondary consultation was suboptimal.
Discussion
The Partnership Project was a major undertaking that promoted collaboration between public sector providers of mental health care, private psychiatrists and GPs. Through its Linkage Unit, it achieved a substantial shift in service culture, making systemic changes that have the potential to be sustained beyond the life of the Project. It made a difference to how many public sector clinicians at SVMHS and SGAPS approach their work, offering them the chance to think about collaboration and referral to the private sector. It also had significant impacts for some private psychiatrists, in terms of increasing their comfort with and understanding of the public sector, and provided opportunities for many GPs to further their knowledge and skills in managing consumers with mental health problems. It created a smoother referral process, with improvements in the referral pathway in both directions.
Shared care arrangements were facilitated for 218 consumers. These consumers were relatively evenly split with regard to sex, and were most commonly young, unmarried, English-speaking and diagnosed with an affective disorder or a psychotic disorder. Despite the fact that only a minority had private health insurance and half were on a pension or benefit, negotiations for collaborative arrangements involving the private sector were achieved.
Although it is encouraging that the Linkage Unit facilitated these shared care arrangements, it is fair to say that the positive cultural and systems changes have not yet led to changes in practice across the board. Shared care arrangements are still not the norm. Although some consumers and carers were reported to have experienced greater satisfaction with the care facilitated by the Linkage Unit, this has yet to be generalized. While the improvements in satisfaction were not limited to particular groups of consumers, some with particularly complex needs did not experience the full benefits of improved collaboration.
The flow-on effects of major cultural and systems change would be expected to take time, however, and there is evidence that many of these changes will continue and be strengthened beyond the life of the Project. Although the Linkage Unit ceased functioning formally at the end of the Project, several steps have been taken to ensure that its roles will be continued. With regard to maintaining changes in service delivery to improve collaborative arrangements for individual consumers, the key functions of the Linkage Unit will be continued in a revised intake duty and triage service, and the activities of an existing General Practitioner Shared Care Committee will be expanded. The fact that the practices of some clinicians have begun to change (e.g. options for private psychiatric care are now considered more routinely) augurs well for continued systems-level and cultural change, particularly in the context of the formal policies and protocols developed through the Partnership Project. The likelihood of the former roles of the Linkage Unit being maintained is enhanced by the fact that SVMHS and SGAPS have become organizationally aligned in the same program, under one management within St Vincent's Health, and by the fact that the majority of Linkage Unit staff will continue to be employed within the service. The services is also taking steps to ensure that another nominated senior clinician within each clinical team at SVMHS and SGAPS will have continuing responsibility for promoting public–private links.
The success of the expanded roles for private psychiatrists offered through the Partnership Project was inconsistent. The supervision and training activities were readily embraced by private psychiatrists, who found these roles extremely satisfying and appreciated the opportunity to engage in work outside provision of direct clinical care. The supervision and training was also highly beneficial to recipients, a finding that is supported by specific evaluations of the CBT workshops and CDGs, reported elsewhere [18], [19]. In the evaluation of the CBT workshops, all GP participants indicated that they had developed an understanding of the principles of CBT and the conditions that are most appropriate for the application of CBT [19]. Similarly, in the CDGs evaluation, the majority of GP participants reported that their learning objectives had been met, that they had a greater understanding of mental health issues after the CDGs, and that their interest in the area had expanded [18].
By contrast, the uptake of case conferencing and secondary consultation was weaker than anticipated. It should be noted that some private psychiatrists undertook these activities without billing for them, viewing them as part of their normal role. Partnership Project personnel observed that there was less interest in these activities, in spite of them being part of the ‘natural association’ between private psychiatrists and other providers (particularly GPs), and being a potentially influential means of tackling the barriers to collaboration between the public sector and private psychiatrists. Suggestions to rectify this include better promotion of case conferencing and secondary consultation, a better match between areas of expertise and needs, and financial incentives for other parties, such as GPs, to participate. Where case conferencing and secondary consultation opportunities were taken up, the experiences of private psychiatrists were generally very positive. Examples of case conferencing and secondary consultation working well should be further explored.
The relatively low uptake of case conferencing is of particular relevance, given certain recent developments in relation to the Commonwealth Medicare Benefits Schedule (CMBS). In 2000, a series of new item numbers were added to the CMBS, which allowed for case conferences between physicians (including psychiatrists) and at least three other multidisciplinary providers, in recognition that improved co-ordination in community settings leads to improved consumer impacts/outcomes through a more flexible, efficient and responsive match between consumers' needs and services [20]. In 2002, the total number of case conference participants was revised to three (one psychiatrist and two others). An evaluation of the new case conferencing item numbers for private psychiatrists has been commissioned [Pirkis J and Burgess P. (2002) An evaluation of the introduction of Case Conferences for Consultant Psychiatrists and new Item Numbers on the Medicare Benefits Schedule, National Health and Medical Research Council Strategic Research Development Committee, Grant No. 219210], and the current findings suggest that it will be important for the evaluation to focus, at least initially, on their uptake.
From the perspective of the Commonwealth Government as payer, the fees billed by psychiatrists for their expanded roles were relatively minimal, accounting for 1–2% of their HIC payments. It would perhaps have been desirable if the expanded roles had been cost neutral (i.e. that their cost was offset by a reduction in HIC benefits paid for direct clinical care). The overall cost was greater in the two years of the Partnership Project than it was in the baseline year, although without more sophisticated trend analysis it is not clear whether HIC costs would have risen anyway. As a group, the private psychiatrists who participated in the Partnership Project were not typical as they were comparatively ‘low billers’ of the HIC, with many only working part-time in private practice (often complementing this with work in the public sector). This made it difficult to describe a ‘typical’ billing year for these psychiatrists and allowed for a lesser but still shared role across services. One psychiatrist who participated was returning to private practice after a long absence, and others were close to starting practice after newly qualifying as specialists. It is likely that the expanded roles did not lead to a reduction in fee-for-service sessions with consumers, as many of the activities (particularly those related to supervision and training) occurred outside the usual practice hours. Nonetheless, the Linkage Unit's achievements suggest that more flexible payment models for private psychiatrists are worth exploring in the face of the artificial divisions created by the different funding arrangements currently in place for the public and private sectors.
The Partnership Project represented an innovative approach to problems of lack of collaboration between the public mental health sector, private psychiatrists and GPs, and achieved major systems-level and cultural change. It led to changed practice and satisfaction for some patients and carers. This did not take place across the board, and collaborative arrangements are still not the norm. However, the Project has demonstrated a means to achieve them. Its achievements have the potential to be sustained at a ‘grassroots’ level. Moreover, the model can be transferred to other contexts, where it could make inroads in improving collaboration between public and private mental health sectors.
Footnotes
Acknowledgements
We thank the Commonwealth Department of Health and Aged Care, and the Victorian Department of Human Services for their support and Beth Bailey, Lyn Chaplin, Wayne Chamley, Margaret Goding, Christine McDougall, Rhonda Goodwin, Edmond Chiu, Elizabeth Sommerville, Bernie Dowling, Kim Simon, Olga Yastrubestskaya. Thanks also to Tony Pinzone for data management and analysis.