
Abstract
Tourette's syndrome (TS) is a chronic neuropsychiatric disorder with mean age of onset at 7.4 years and characterized by motor and phonic tics and related somatosensory urges. No longer considered a rare disorder, recent epidemiological studies based on direct observations have found the prevalence rate to be as high as 1–3% in a general high school population [1, 2]. Tourette's syndrome have reported an array of associated behavioural and emotional problems, including symptoms of attention deficit hyperactivity disorder (ADHD), some forms of obsessive–compulsive disorder (OCD), anxiety and mood disorders [3–5]. Some of these behavioural and mood problems were pervasive through adolescence and into adulthood considered it integral to TS. For many TS children, the associated behavioural and emotional problems are more disruptive and impairing than their tics [6].
Tourette's syndrome was first described by Georges Gilles de la Tourette in the 1880s, and has since been noted to commonly co-occur with psychiatric disorders, such as ADHD, OCD, anxiety disorders, depression, conduct and antisocial disorders, general adjustment problems and developmental and school learning disorders, prompting estimates that children with TS have a 5-to 20-fold increased risk for these disorders compared with non-affected peers [7]. Figure 1 summarizes their relationships.
Overlapping relationship of Tourette's syndrome (TS) to attention deficit hyperactivity disorder (ADHD), obsessive–compulsive disorder (OCD) and other disorders (including anxiety disorders, depression, conduct and antisocial disorders).
There was evidence to suggest that TS children with severe behavioural and emotional problems often suffered from comorbid psychiatric disorders, especially comorbid ADHD or OCD. A variety of behavioural and mood problems are know to associate with TS children with comorbid ADHD, and these problems are more pronounced in TS children with comorbid ADHD than in children with TS alone or in matched controls. For example, Shapiro and Shapiro found that male TS children aged 6–11 years with comorbid ADHD scored higher in the Child Behavior Checklist (CBCL) overall symptom subscales than normal control patients [8]. Sukhodolsky reported that comorbid ADHD was highly associated with disruptive behaviour and functional impairment in TS children [9]. Randolph et al. reported that TS children with ADHD had a higher rating of tic severity than the TS-only group [10]. Stephens and Sandor found that aggressive behaviour in TS children may be associated with comorbid ADHD or OCD [11]. Comorbid OCD is also found to be associated with increase in behavioural and emotional problems in TS [3, 12]. A higher proportion of tic-related OCD have intrusive, violent or aggressive thoughts and images and worries about symmetry and exactness [3]. Budman et al. found that OCD is closely associated with conduct disorder and ADHD and may represent part of a more general dysfunction of impulse control in TS [12].
We have observed in our clinical practice that the nonpsychiatric TS children without any comorbid disorders also suffered from behavioural and emotional problems. It would be interesting to know if the severity of tic symptoms was directly related to these behavioural and emotional problems in this group of TS children. Several clinical studies have reported significant association of severity of tic symptoms and behavioural disturbance [13, 14], but other studies have failed to establish this relationship [15, 16]. These inconsistent findings were probably related to age effects, insufficient control of medication status, imprecision in measurement of tic severity, and more importantly, failure to take into account comorbid conditions such as ADHD or OCD. The purpose of this study is to examine systematically the nature and severity of behavioural and mood problems in TS-only children and their relationship with the severity of tic symptoms. The primary goal is to determine whether severities of tic symptoms is an indicator of more complex and more severe behavioural and mood psychopathology in TS-only children.
Method
Patients
Patients were recruited at the Mental Health Institute of Central South University between 2000 and 2002. The TS group included 69 children (58 boys and 11 girls) between the ages of 8 and 16 years (mean=9.43, SD=2.4). Sixty-nine healthy middle to upper-middle class children (58 boys and 11 girls) between the ages of 8 and 16 years (mean=9.03, SD=1.32) were randomly selected from a local general school population. The two groups were matched in age, gender, IQ and educational background. Patients of the study group were all outpatients meeting the DSM-IV criteria (American Psychiatric Association, 1987) for TS. They had either not received any pharmaceutical treatment, or else were drug-free for at least 4 weeks before the study. The diagnosis was made on the basis of clinical observation and history provided by the parents and the patients themselves. Children who evidenced transient tics or chronic motor or vocal tics and comorbidities such as ADHD, OCD, anxiety disorders as well as bipolar and non-bipolar mood disorders were not included. All patients were free from gross neurological or other organic disorders. All healthy control patients were free from psychiatric disorders and gross neurological or other organic disorders.
Assessment procedures
The diagnostic procedures included child and parent clinical interviews. A board-certified psychiatrist (SU Linyan) with 25 years of research and clinical experience treating TS children, diagnosed each case on the basis of a clinical interview with the parent and completed the Yale Global Tic Severity Scale (YGTSS) [17]. The severity of motor and phonic tics (separately) were rated along five discriminant dimensions on the YGTSS: number, frequency, intensity, complexity and interference. Patients' tic symptoms ranged from mild to severe. The parents were also asked to complete the CBCL [18].
Using the median total tic score as the dividing line, the TS children were divided into two groups: a less severe tic disorder group (LST; score≤23, n=34) and a more severe tic disorder group (MST; score<23, n=35). The subgroups did not differ significantly in age, special education, history of tics or compulsive motor habits.
Categorical data were analysed by chi-squared analysis, continuous data by analysis of variance or multinominal logistic regression and ordinal data by ordinal logistic regression. Associations between continuous variables were evaluated by Pearson correlations. Statistical significance was defined at 1% level, with trends reported at 5% level and all tests were two-tailed. Data are expressed as mean±SD unless otherwise stated.
Results
Comparison of behaviour problems between control and Tourette's syndrome group
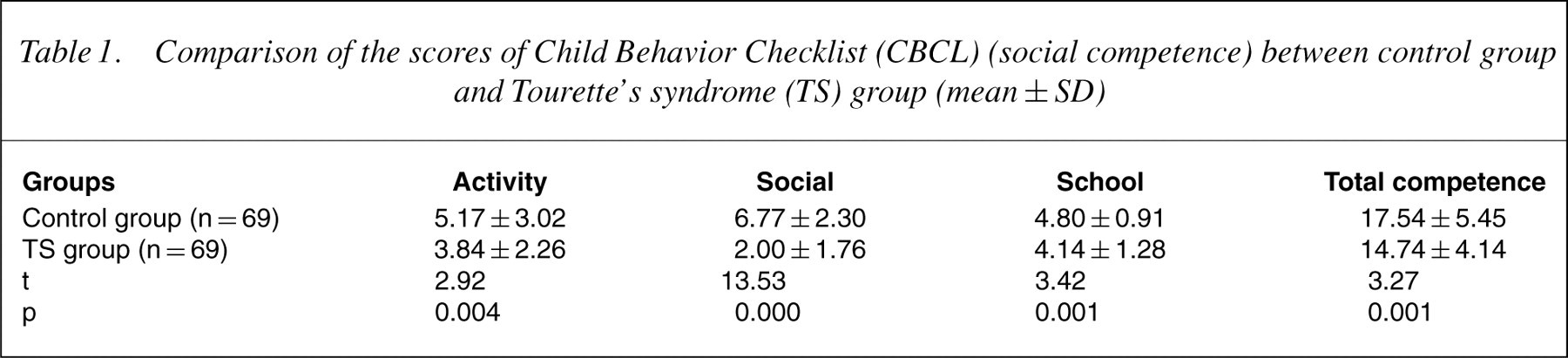
Tables 1 and 2 show the CBCL scores. The TS group had lower CBCL social competence subscale scores and total score than the control group, and had higher behavioural problems subscale scores and total score than the control group (p<0.01). We also found that 60.1% of TS children had attention problem scores higher than the clinical cut-off, 46.3% exceeded the cut-off on the anxious/depressed scale and 48.4% exceeded the cut-off on thought problem scale. But they did not meet DSM-IV criteria for ADHD, OCD and anxious/depressed disorders. Comparatively, only 5.8%, 4.3% and 4.3% of the control group had scores above the clinical cut-off on the attention problem, anxious/ depressed and thought problem scales, respectively, and none of them fulfilled DSM-IV criteria for ADHD, OCD or anxious/depressed disorders.
Comparison of the scores of Child Behavior Checklist (CBCL) (social competence) between control group and Tourette's syndrome (TS) group (mean±SD)
Comparison of the scores of Child Behavior Checklist (CBCL) (behaviour) between Control group and Tourette?s syndrome (TS) group (mean±SD)

Relationship between behavioural problems and severity of tic symptoms
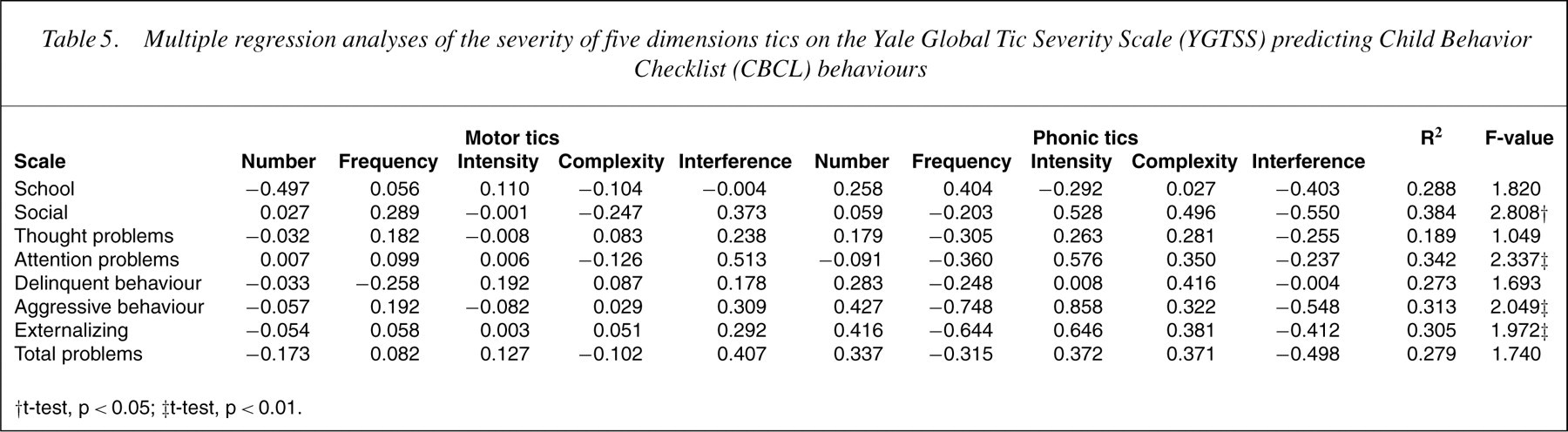
Table 3 shows children with MST had higher CBCL delinquent behaviour, thought problem, externalizing and total problem scores than those with LST (p<0.05). There was no difference between the two groups in CBCL social competence subscale scores and total score. Pearson correlations were then used to examine the relationship between the YGTSS current motor and phonic tic severity and the CBCL behaviour problems scores. The severity of tic symptoms was negatively correlated with school and total competence (r=−0.134 to 0.472, p<0.05) and positively correlated with severity of social problems, thought problems, attention problems, delinquent behaviour, aggressive behaviour, externalizing and total problems as assessed by CBCL (r=0.285–0.436, p<0.01) in Table 4. To examine whether behavioural problems in TS patients are primarily related to their tics, CBCL behavioural problems that were significantly related to YGTSS scores were further analysed by multiple linear regression. We found that YGTESS scores are predictive of social, attention, aggressive and externalizing problems (p<0.05). By R2 assessment, YGTESS scores were accountable for 38.4%, 34.2%, 31.3% and 30.5% of the social, attention, aggressive and externalizing problems, respectively, in Table 5.
Comparison of the scores of Child Behavior Checklist (CBCL) (behaviours) between less and more severe tic group (mean±SD)
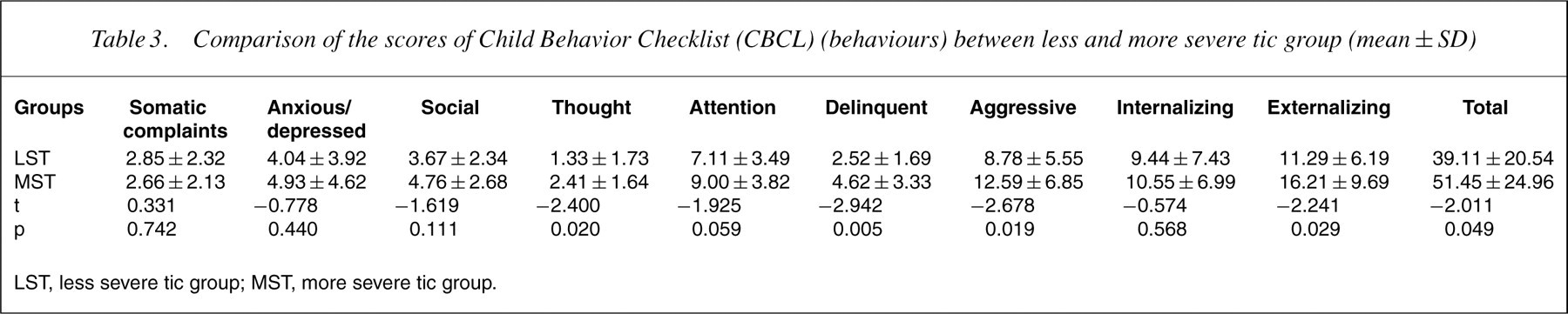
LST, less severe tic group; MST, more severe tic group.
Coefficient of correlation (r) between the severity of five dimensions tics on the Yale Global Tic Severity Scale (YGTSS) and the scores of Child Behavior Checklist (CBCL)
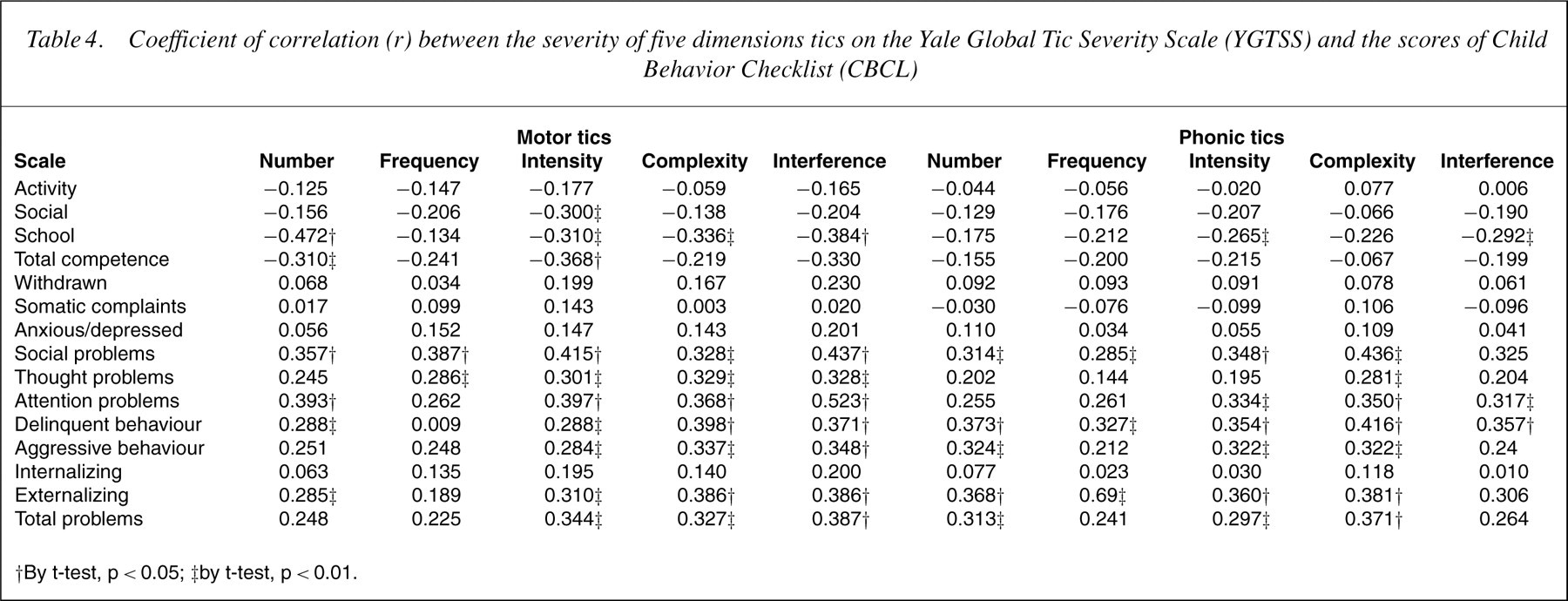
†By t-test, p < 0.05; ‡by t-test, p < 0.01.
Multiple regression analyses of the severity of five dimensions tics on the Yale Global Tic Severity Scale (YGTSS) predicting Child Behavior Checklist (CBCL) behaviours
†t-test, p < 0.05; ‡t-test, p < 0.01.
Discussion
Tourette's syndrome childrenmanifest a broad range of neuropsychiatric disturbances. For many children with tic disorder, the associated emotional and behavioural problems are more disruptive than their tics, leading to impairments in social, occupational, or other important areas of functioning [19, 20]. By comparing 69 TS-only children with 69 control children, we found that TSonly children had significantly higher CBCL scores on somatic complaints, anxious/depressed, social, thought, attention, delinquent, aggressive, internalizing, externalizing and total problem scales than control patients, and significantly lower scores on social competence (activity, social, school and total competence). These findings are consistent with those from earlier reports [21]. With their tic symptoms often drawing attentions from parents, teachers and other school children, TS childrenwere often ridiculed and rebuked both in the family and at school. Initially, TS children may be rebuked in the family because parents may think that tics were a habit disturbance and failed to understand that it is an illness. In school, when teachers failed to understand the disease, symptoms such as vocalization, action and coprolalomania may be regarded as intentional violation of school discipline and the children may be criticized in class. Other school children may ridicule their tic symptoms and they may feel lonely and bullied. Also, TS children could concentrate less well in class because they had to spend a lot of effort just to control their tics, which may lead to underperformance in school. Truancy and absenteeism became a problem in some TS children, while others chose to fight back. All of these were reasons behind their behaviour and mood problems and their impairment in social and study functions.
We also found that more severely affected TS children (MST) had significantly higher scores on thought, externalizing (delinquent, aggressive) and total problems than less affected TS children (LST), also consistent with earlier reports [21, 22]. In contrast to previous studies, we did not find MST to be associated with greater internalizing and depression problems than LST.
The thought problems assessed in CBCL included disruptive and obsessive–compulsive symptoms (cannot get one'smind off certain thoughts (question 9) and repeating certain acts over and over (question 66)). These are the most prevalent manifestations among the MST. In clinical practice, we found that some TS children were obsessed with trying to stop themotor and phonic tics, while others had obsessions and compulsions not related to tic symptoms. One had repetitive eye blinking and guttural throat clearing, and kept sharpening his pencil while writing. We found that 48.4% the TS children were above clinical cut-off (T score<70) on thought problems. This strongly suggested that there is a relationship between the severity of TS and obsessive–compulsive symptoms, consistent with earlier reports [23–25]. Current neuroanatomical and neurobiological studies provided ample evidence to indicate the involvement of specific cortico-striatothalamo- cortical (CSTC) circuits in the expression of TS [3]. Neuroimaging studies also supported the hypothesis that basal ganglia and related portions of CSTC circuitry are important in the pathophysiology of OCD [3]. Our study could not proof CSTC circuitry hypothesis but provided indirect supporting evidence.
The more severely affected TS children scored higher than LST on the externalizing problems (aggression, hyperactivity and conduct problems) subscales of CBCL. This suggests that impulsive behaviours are related to the severity of tic symptoms. These behaviours mainly consisted of agitation, low-anger threshold, fruanly and lying. In some cases, TS children shouted at, or even acted violently, to their parents for trifles, but quickly calmed down and showed regret in a few minutes. Externalizing problems were the main reason for medical consultation in some children, while other children already had a history of aggressive behaviours and being overly active before developing tics. These findings are generally consistent with earlier reports that TS was associated with impulsity [3, 25]. Positron emission tomography and single photon emission computed tomography studies showed either increased or decreased activities in the frontal regions [3], the known inhibitory control centre of the brain. The impairment of this control centre results in impulsive behaviours [26]. These findings also support our hypothesis.
Pearson correlations showed that the severity of tic symptoms was negatively correlated with school and total competence and positive correlated with social problems, thought problems, attention problems, delinquent behaviour, aggressive behaviour, externalizing and total problems. This suggests that school and social functioning were impaired, and some of the behaviour problems were increased in association with increasing severity of tic symptoms, and multiple regression analyses confirmed these observations.
The relationship between TS and behavioural problems is currently not well understood. Some investigators believe behavioural problems that frequently co-occur with TS are an integral part of it, while others think that they are secondary to comorbidities of TS, especially ADHD and OCD. There was evidence to support both arguments. The study showed that some of the co-occurring behavioural problems (attention problems, obsessive–compulsive symptoms and externalizing problems) are positively related to the severity of tic symptoms in TS children with no comorbidities, especially ADHD and OCD. However, these explained only 30% of the problems at best by R2 analysis. To better understand the nature of behavioural problems in TS, we may need to study its different comorbid conditions in greater detail.
This work was supported by Nation Natural Science Foundation of China (30300118).