
Abstract
Keywords
Between the health care we have and the health care we could have lies not just a gap, but a chasm.
(Institute of Medicine, 2001 [1])
In a document titled ‘Crossing the Quality Chasm: A New Health System for the 21st Century’, the Institute of Medicine challenged the American health care system to make fundamental changes [1]. As a result of this critique, many initiatives are now underway which aim to make health care safe, effective, patient-centred, timely, efficient and equitable. A central part of this process includes considerations about how services for general medical and psychiatric illness are purchased, administered and provided.
Compelling evidence suggests that patients with untreated or ineffectively treated mental health (including chemical dependence) problems, the majority of whom are seen in the general medical sector, have worse health outcomes, substantially higher total health care costs, and reduced productivity when compared to people with no such mental health problems. In this paper, we review the magnitude of this problem and provide specific suggestions about how to improve it at the health system level, the administrative level and the clinical level. We approach the task by answering six key questions: (i) How big is the problem? (ii) What are the costs and outcomes associated with independently managed mental health care? (iii) What should be the future goals in mental health? (iv)Can these goals be achieved with independent management of mental health? (v) Is changing the system worth the effort? (vi) What is the best way forward?
Separation of medical and mental health care is a worldwide practice leading to unacceptable clinical and economic outcomes in virtually all countries and cultures. The Australian system is no different. Boiled down to the core ingredients of any health system, that is, purchasers, administrators, providers and patients, budget silos are as great a distraction to the delivery of effective and economical care in Australia as they are in the US, Germany, Japan, Austria and many other countries (Fig. 1). This is true with regard to separate budgets for inpatient (e.g. state funded) and community-based outpatient (e.g. federally funded medicare) services, and also with regard to the separate management of physical and mental health care.
Structure of the health care system.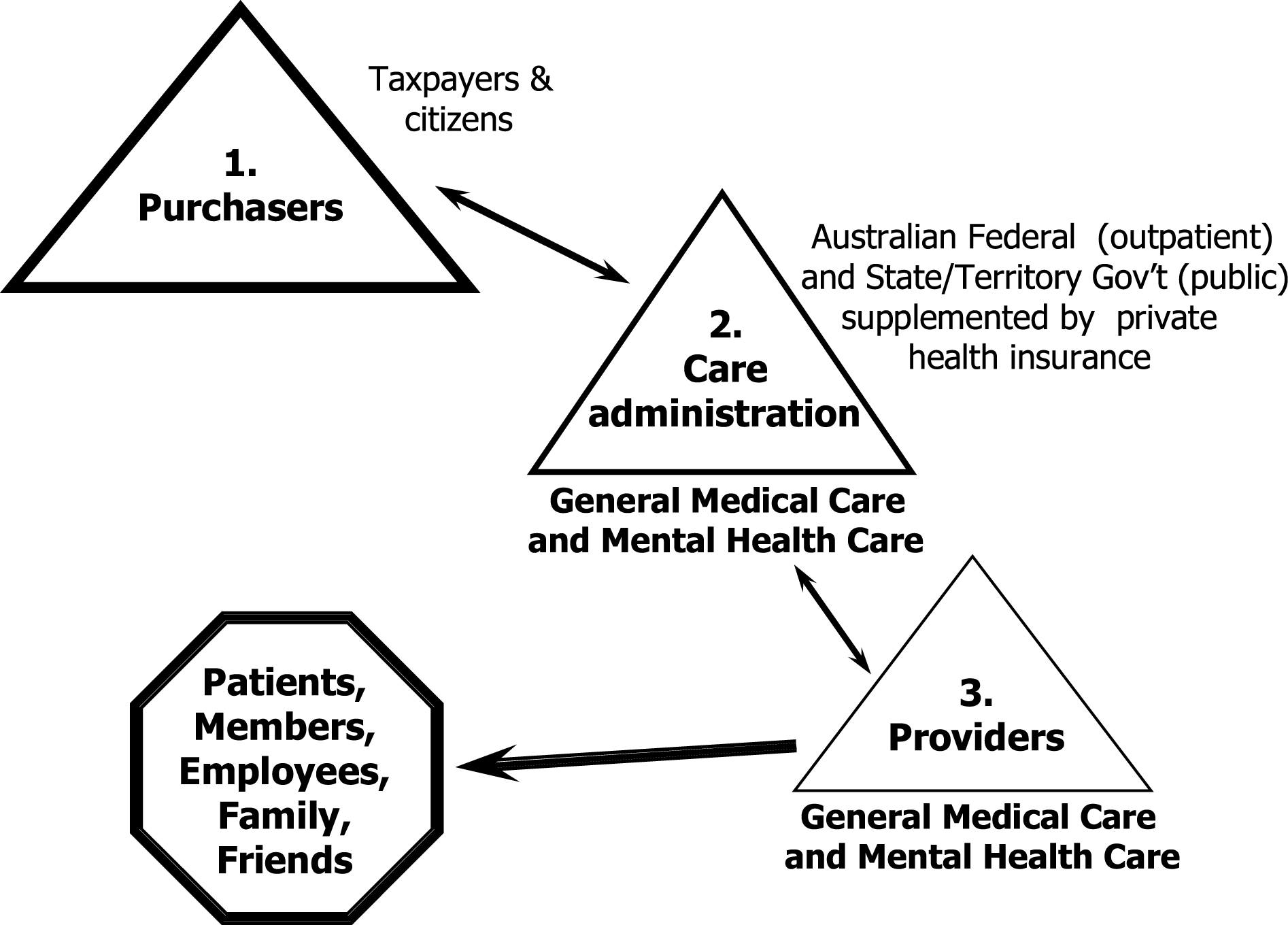
The suggestions for change described in this paper are based on two central internationally applicable premises:
that concurrent and coordinated care is more efficient, effective and economical than sequential and independently managed care; and that creating a health system that integrates medical and behavioural health care for complex, high cost patients with comorbid physical and psychiatric disturbances (3–5% of the total population) can lead to substantial cost savings by fostering better clinical outcomes, improving workplace productivity and allowing fixed budgets to extend services to a wider patient base.
Background
Through the years, medical and psychiatric illnesses have largely been treated in separate clinical settings. This was because the clinical presentations of the two appeared disparate and their treatment seemingly could be addressed independently. However, with advances in our understanding of the pathogenesis of mental illness and its manifestations, conditions that were once considered the domain of psychiatry, such as syphilis, epilepsy, rheumatic fever and hyperthyroidism, have switched treatment settings from mental health to medical.
We have now entered a new era in which, not only do we better understand the multiple aetiologies of psychiatric conditions, but we are also starting to recognize the substantial impact that mental illness has on how effectively, efficiently and economically medical illness is treated. For instance, the diagnosis and treatment of depression, a core psychiatric condition, is now seen more often in the general medical sector, under the direction of non-mental health professionals, than in the mental health sector [2–6]. Furthermore, it is consistently associated with increased medical service use [7–11], adversely impacts clinical outcomes of co-occurring medical conditions [8],[12–14], and is associated with increased mortality [15], [16]. The same can be said for anxiety, substance abuse, somatoform disorders, eating disorders, bipolar disorder, autism and schizophrenia.
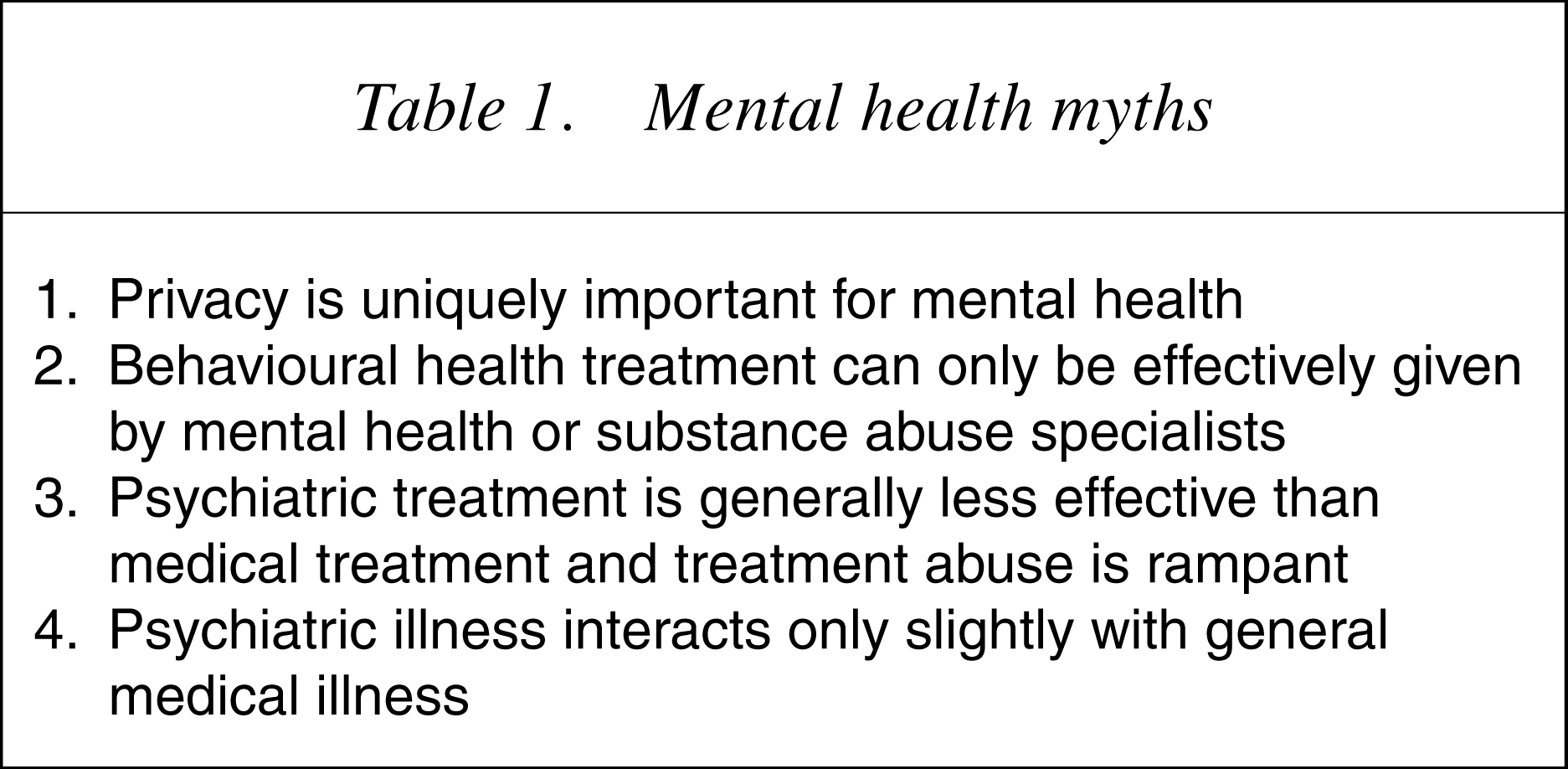
Despite this fact, purchase of care for mental illness (whether through taxes or private payments) occurs to a great extent independent of other medical illnesses, so much so that even when there is co-occurrence of physical and mental health problems and associated poor outcome, it is difficult to find ways to coordinate the medical and psychiatric services. Unfortunately, this continued separation is largely based on persistent myths about mental illness (Table 1). Integrated physical and mental health will only become a reality when informed populations come to recognize:
that privacy should be a core feature of all health care, not just mental health; that non-mental health professionals can also effectively administer mental health treatment, particularly when mental health support personnel are available; that treatment for the most common mental disorders, such as depression and anxiety, have evidence of efficacy comparable to, if not better than, that found for many other medical conditions; and that the co-occurrence of psychiatric illness with physical conditions is associated with a substantial decrement in clinical and economic outcomes in both the medical and psychiatric domains. Mental health myths
The care of the mentally ill continues to move across to other medical practitioners, particularly general practitioners and specialist physicians, as our knowledge of psychiatric illness improves and the clinical needs of patients outstrip the ability of mental health professionals to provide adequate service. For instance, patients with dementia receive treatment less frequently from mental health professionals and more frequently from neurologists and acute care physicians than in the past. Even patients with persistent mental disorders, such as autism, bipolar illness and eating disorders, increasingly receive care from non-mental health personnel as is manifest by the number of prescriptions for psychotropicmedications written by paediatricians and the like.
It is the supposition of this paper that we have now reached the stage of understanding about mental illness and its treatment that it is no longer possible or acceptable, either on clinical or economic grounds, to separate the diagnosis and treatment of mental health disorders from other medical disorders. The central message of this review is that mental illness (‘the psyche’) should be handled as just a part of other medical care. This requires structural reorganization of the way that health care is purchased, administered and provided, moving from an independently managed to an integrated model of general medical and psychiatric care.
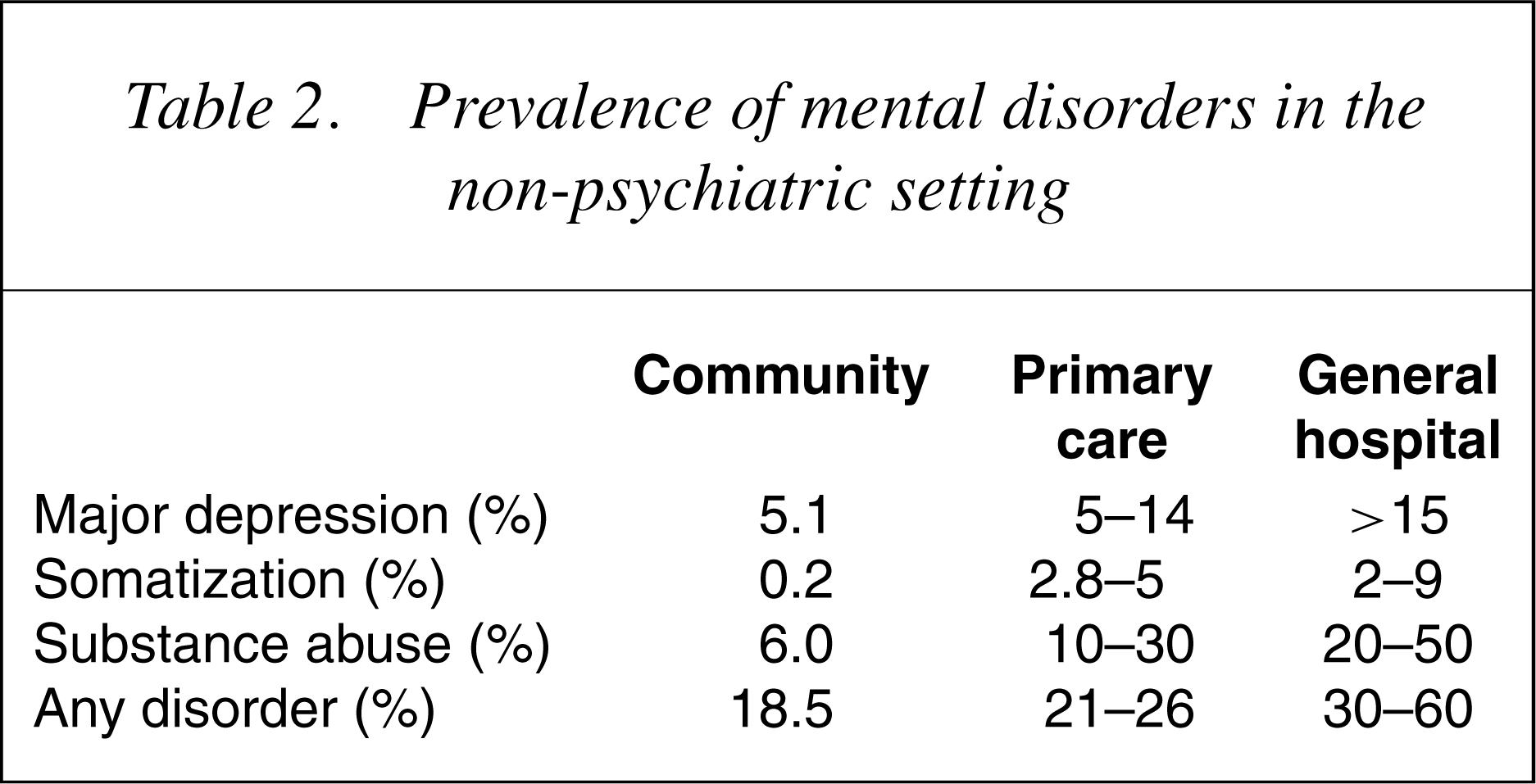
How big is the problem?
Prevalence of mental disorders in the non-psychiatric setting
What are the costs and outcomes associated with independently managed mental health care?
One of the central arguments for the separation of mental health services from the rest of medicine is that delegating that responsibility to thosewith expertise inmental health would result in better use of the limited health care resources available for patients with psychiatric illness. If this is the case, then we should see that patients with mental disorders are being properly treated with interventions likely to change outcomes, and that this is accomplished with the greatest value per dollar spent.
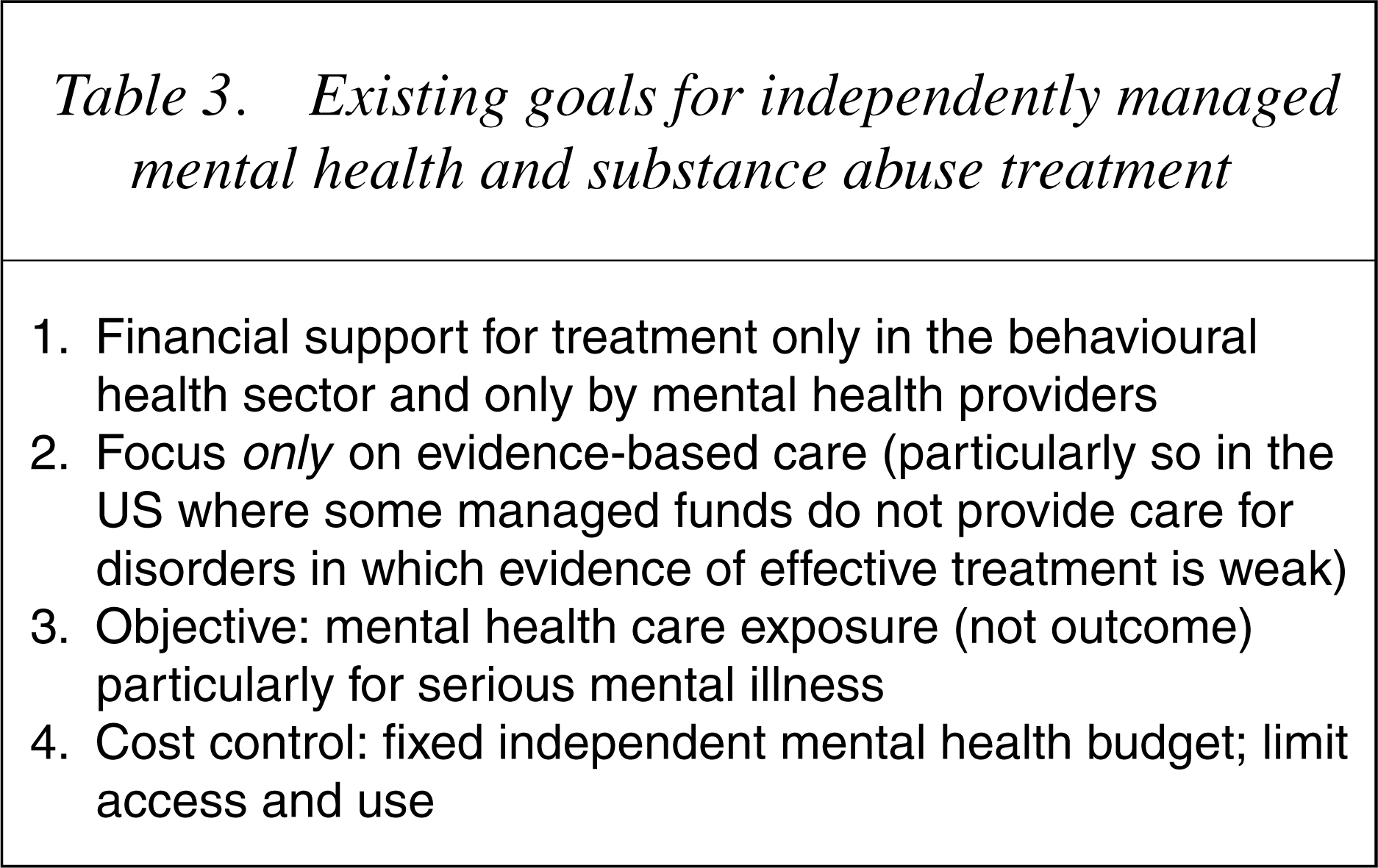
Recent studies, however, suggest that independently managed mental health administration, which is driven by focused goals within the behavioural health framework (Table 3), achieve limited success when viewed in the context of total health care for a population.
For instance, Narrow et al. [25] report that 71% of patients with mental illness receive no mental health care (26]. Of the 29% that receive treatment, two-thirds do so within the general medical sector, often with little input from mental health professionals and also with limited clinical success [6], [27], [28]. The figures are similar in Australia [29]. Studies by Kessler et al. [27], on a US population, suggest that only 42% of those who have depression receive minimally adequate treatment. Applying this figure to other mental health conditions, a generous estimate considering the efforts made in education about the diagnosis and treatment of depression, only 12% of the population would have been exposed to outcome changing care. This finding alone raises questions about the legitimacy of the argument that management of mental health care by those with mental health experience has brought value to patients with mental illness.
Treatment of mental illness in the US (annually, 18.5% of population, 52 million Americans) have clinically significant mental illness) [25].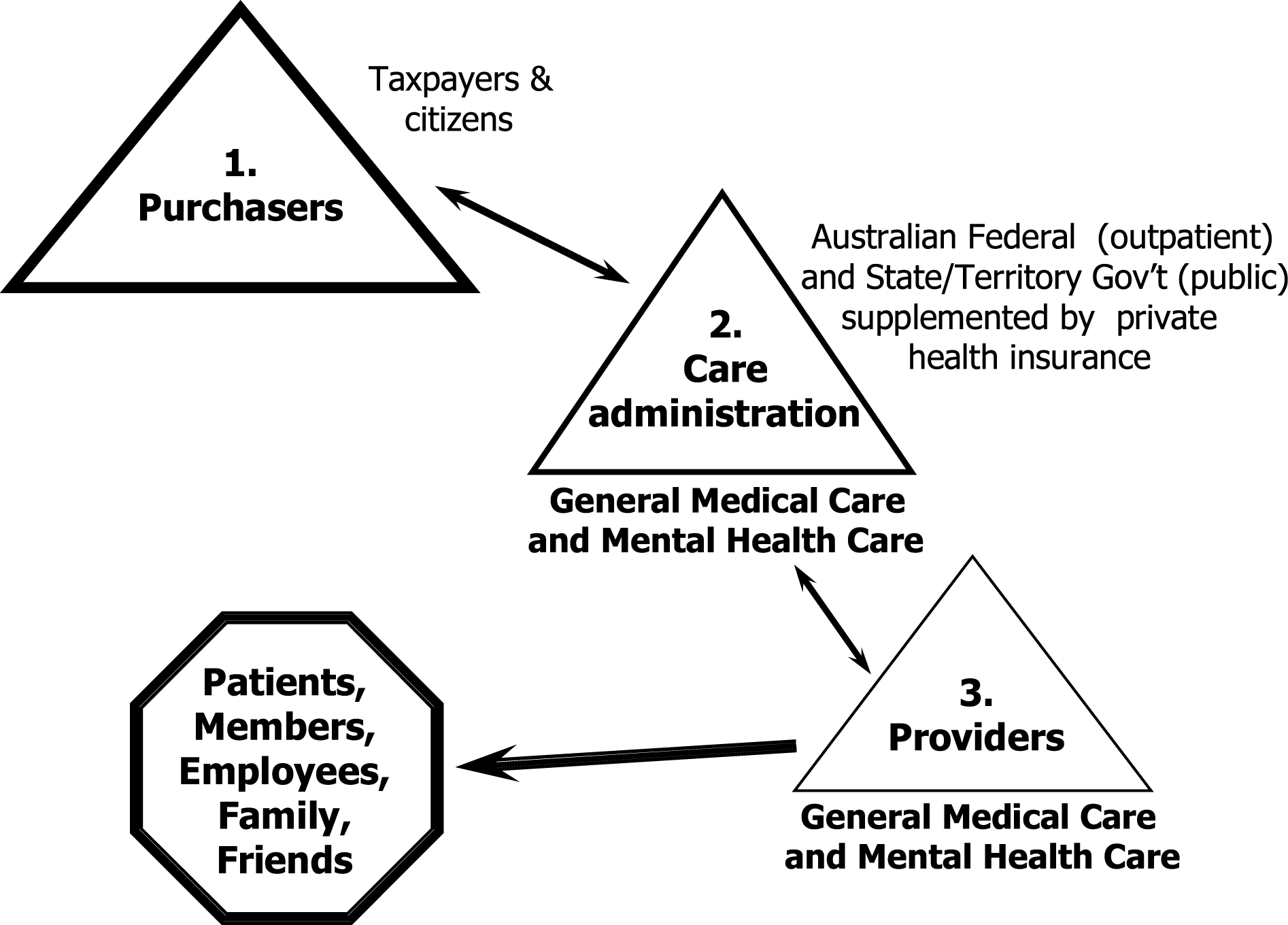
Existing goals for independently managed mental health and substance abuse treatment
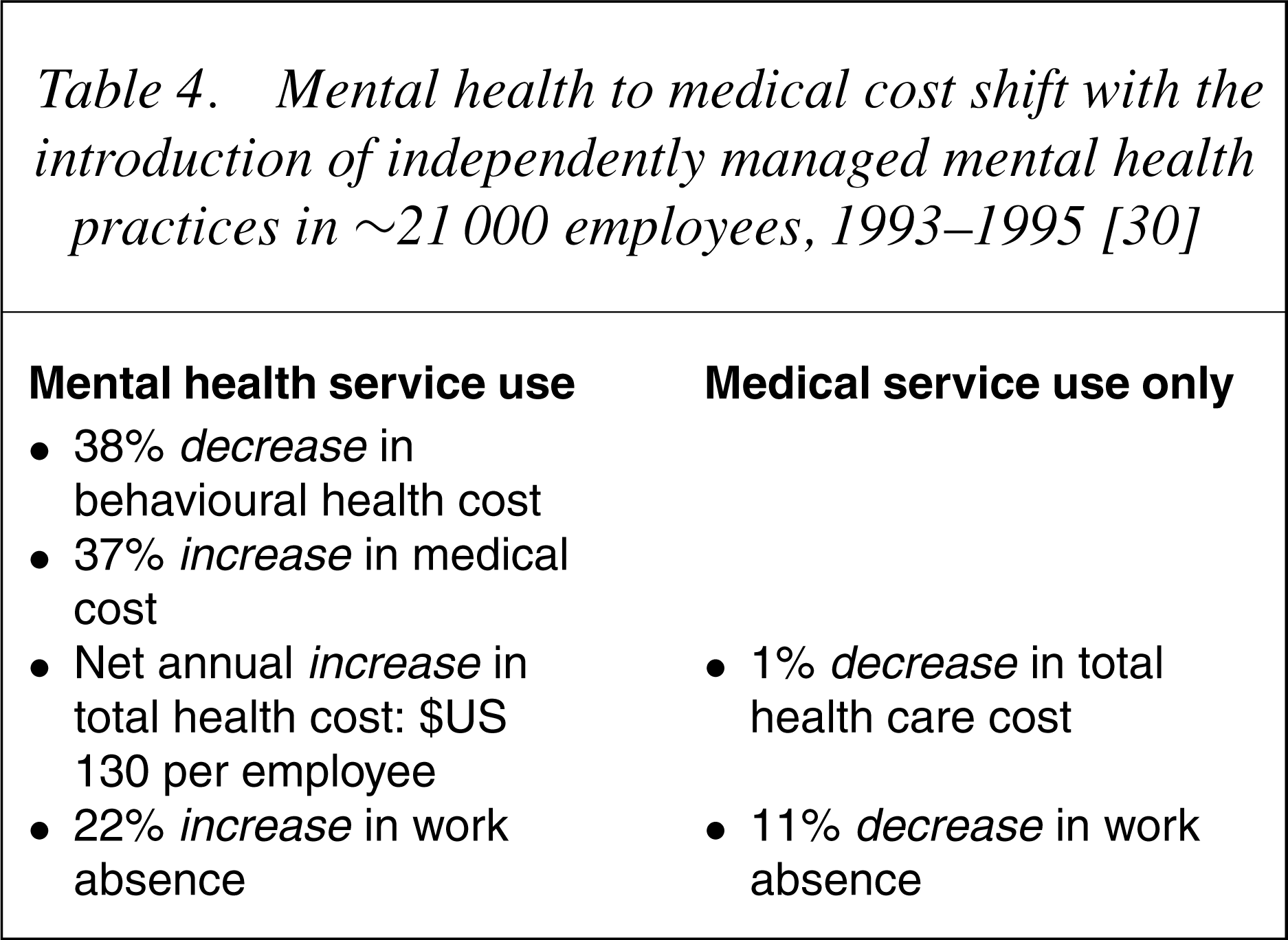
Mental health to medical cost shift with the introduction of independently managed mental health practices in ∼21 000 employees, 1993–1995 [30]
The focus of exactly where the majority of health care spending occurs in people with mental health problems has been difficult to unravel because independent administrative and claims processing systems for medical and mental health services are stored in non-communicating databases. A recent report on a cohort of 250 000 enrolees of a major health plan in the US now substantiates that total service use in those managed using independent medical and behavioural health practices is double for those with behavioural health service use [32]. Perhaps more important than this finding, which has also been reported in other studies [10], [33], [34], is that over 80% of the costs associated with the care of these patients is for medical claims and prescription medications for physical disorders (35] who showed that patients with psychosis, depression, anxiety and chemical dependence all had total annual health care costs 2.3–2.6 times that of those without. Mental health and chemical dependence services accounted for less than 13% of total health care costs with the exception of psychotic patients in whom 33% of expenditures were for mental health, not physical health, services.
Health care expenditure for 250 000 patients with and without mental health service use [31].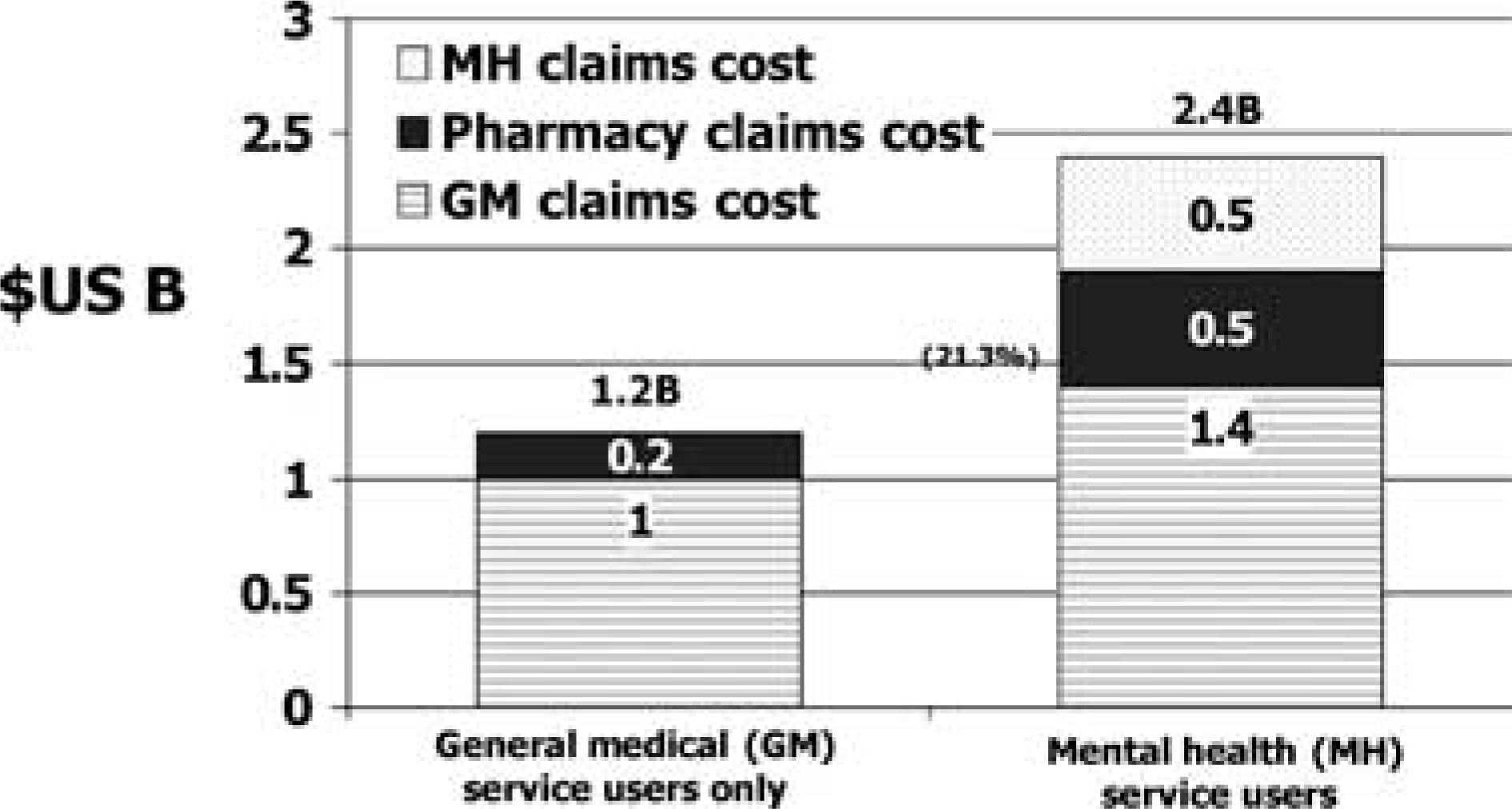
If the majority of health care costs in mental health patients are for medical services and related medications, it suggests that there is an interaction of medical and psychiatric illness that is not being addressed adequately in health systems which handle medical and mental health independently. This finding becomes even more important when one considers that a reduction in mental health service use is associated with a return to nearly baseline levels of total annual health care spending [32], even in patients with complex illness and comorbidity.
Ironically, most countries continue to maintain health systems in which medical and mental health practitioners not only do not talk with each other, but are discouraged from doing so by the funding systems in which they work. For instance, in Australia, despite a National Mental Health Plan that encourages general medical and mental health service coordination, there is no mechanism for insuring that mental health professionals with the skills to work at the interface of medicine and psychiatry have funding to support their work [36]. They are caught between tight medical and mental health budgets, neither of which claim ownership for supporting clinical work in the area of psychiatric consultation. Similar examples are easily identified by practitioners in many other countries, including the US, Austria, Germany and the Netherlands.
What should be our future goals in addressing mental health issues?
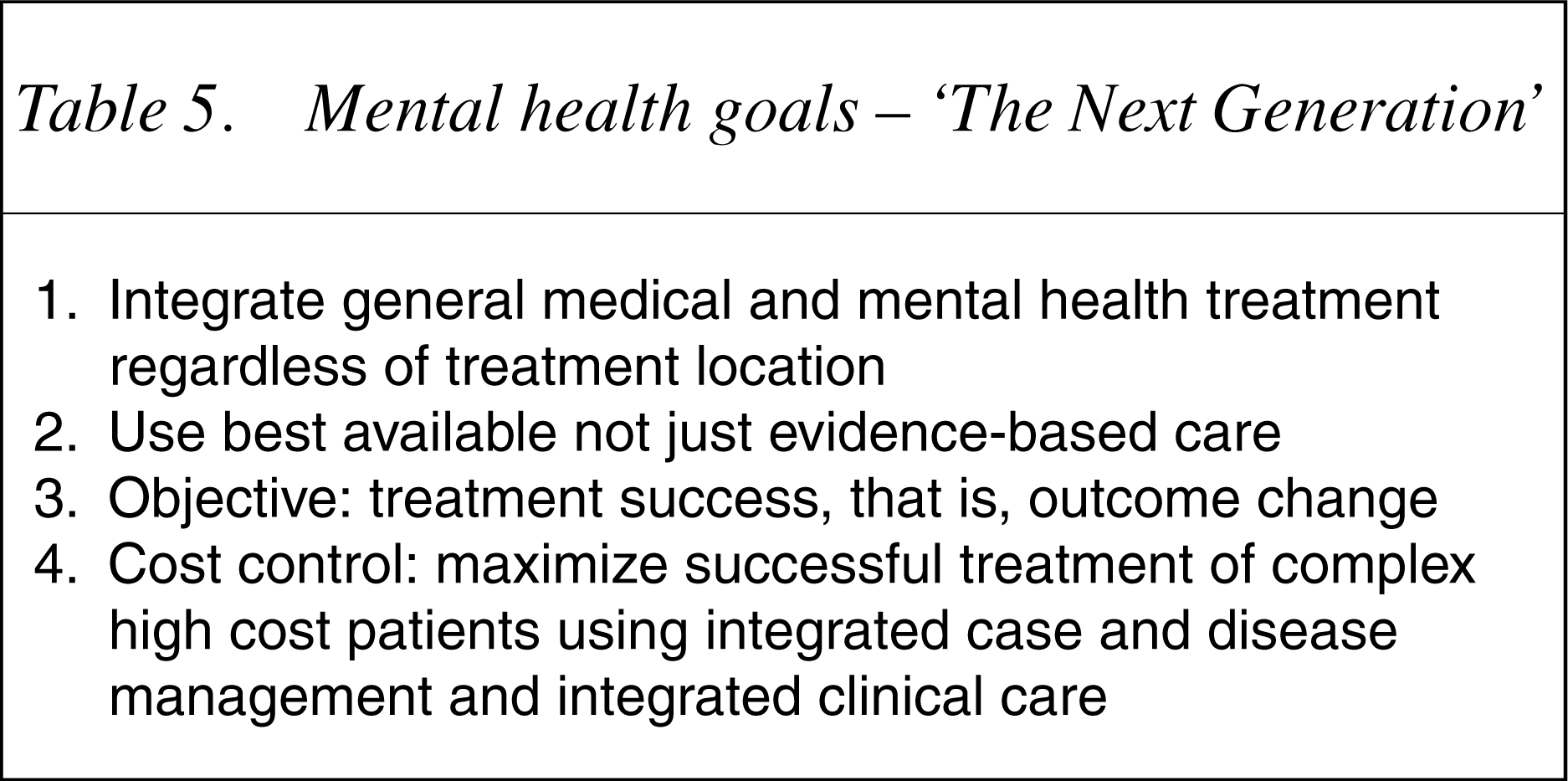
So far in this review, we have seen that a substantial number of patients have concurrent general medical and psychiatric illness, yet most health systems worldwide continue to support services in each of these areas of medical practice as if they had little connection. In those clinical situations in which the manifestations of aberrant behaviours have obviously been found to be associated with underlying medical conditions, care has been transferred from the mental health sector to the medical, for example, epilepsy. This transition is currently taking place with dementia in many locations throughout the world. The question arises, ‘Is there sufficient evidence that the remainder of psychiatric illnesses are sufficiently distinct and non-interactivewith other medical conditions to maintain their separation from the rest of medicine?’
Mental health goals – ‘The Next Generation’
Can these goals be achieved with independent management of mental health?
Few understand the impact that independent general medical and behavioural health business practices have on the delivery of integrated services. At the heart of the issue is the fact that there are two competing financial bottom lines keen to transfer accountability for the payment of services to the other stakeholder, that is, mental health to physical health or physical health to mental health. This is exactly what is happening in Australia with regard to support for consultation–liaison psychiatry. Both the general medical and psychiatric sectors recognize the value that mental health services would bring to complex, high cost patients with comorbid illness as is manifest by the emphasis on this area in the First National Mental Health Plan promulgated in 1993 [37]. However, neither the medical, mental health, nor a combination of the two sectors, have been willing to relinquish a sufficient part of their budget to support even a rudimentary integrated approach to patient care, that is, the coordination of the mental health and medical health workforces that could lead to improved clinical outcomes, better worker productivity and lower health care costs.
The situation is even more dramatic in the US where an entire managed behavioural health system has been built-up since the introduction of separate general medical and mental health diagnostic-related groups – the trigger in the US for independently managed behavioural health. The US system is so entrenched in administrative processes that segregate mental health that correcting the problem turns out to be a massive undertaking.
Areas requiring change for medical and mental health integration
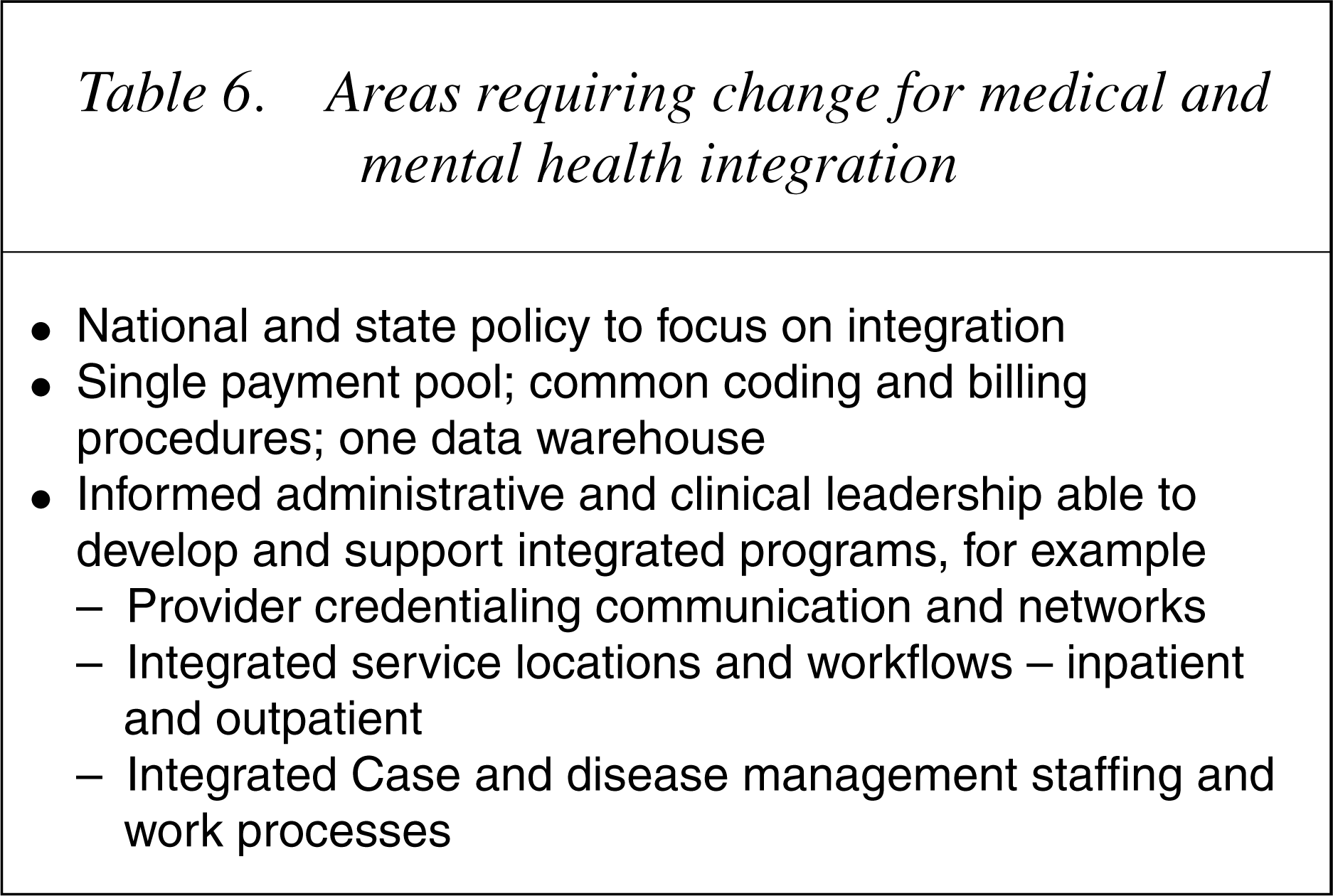
Interestingly, the solution to integration is relatively simple; mental health needs to be handled as an integral part of other medical services. One can argue that obstetric care is inherently different from pathology, paediatrics from radiology and internal medicine from anaesthesia, yet they are a part of the same administrative and funding system. Psychiatry, likewise, is clearly different than other branches of medicine but is the only one handled independently. This can easily change. There is no reason that any health system, regardless of its administrative configuration, cannot be simplified to include mental health and chemical dependence as core components of the health benefits available to their populations.
Is changing the system worth the effort?
There are two compelling arguments about why a change is worth the effort. First, data indicate that independent general medical and mental health care management is associated with a low percentage of mental health and chemical dependence patients being treated, largely because most people with psychiatric illness do not enter the mental health sector. An even lower percentage receives minimally effective care. Furthermore, the majority of people being treated are treated in general medical settings, so that there is, in effect, a cost shift of health care spending for behavioural health problems from mental to physical health. In short, health systems which segregate general medical and mental health management have a poor track record for providing basic mental health services and holding down the total cost of care for those with mental illness. There is, therefore, a very good chance that almost any reasoned change will result in better care and lower cost.
The second argument relates to accumulating data on the value that the coordination of general medical and mental health care could bring to the health care system. In recent years, one of the most important findings relating to the economics of health care is that the majority of health care costs are the result of service use by a minority of patients (38]. This presents an opportunity to reduce health care cost by improving the way that health care services are provided to a relatively small portion of the population.
Complex patients use the majority of clinical services [32].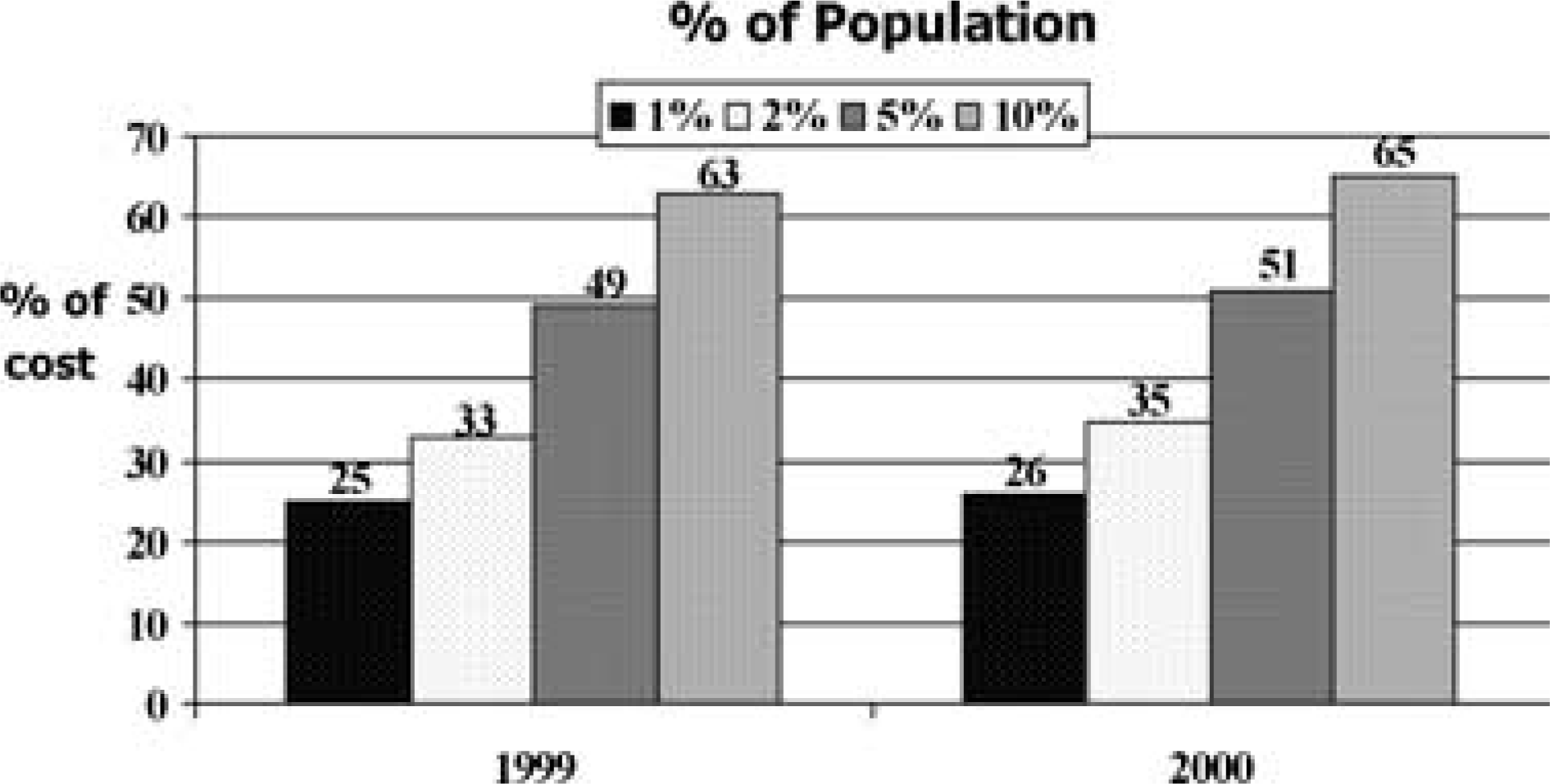
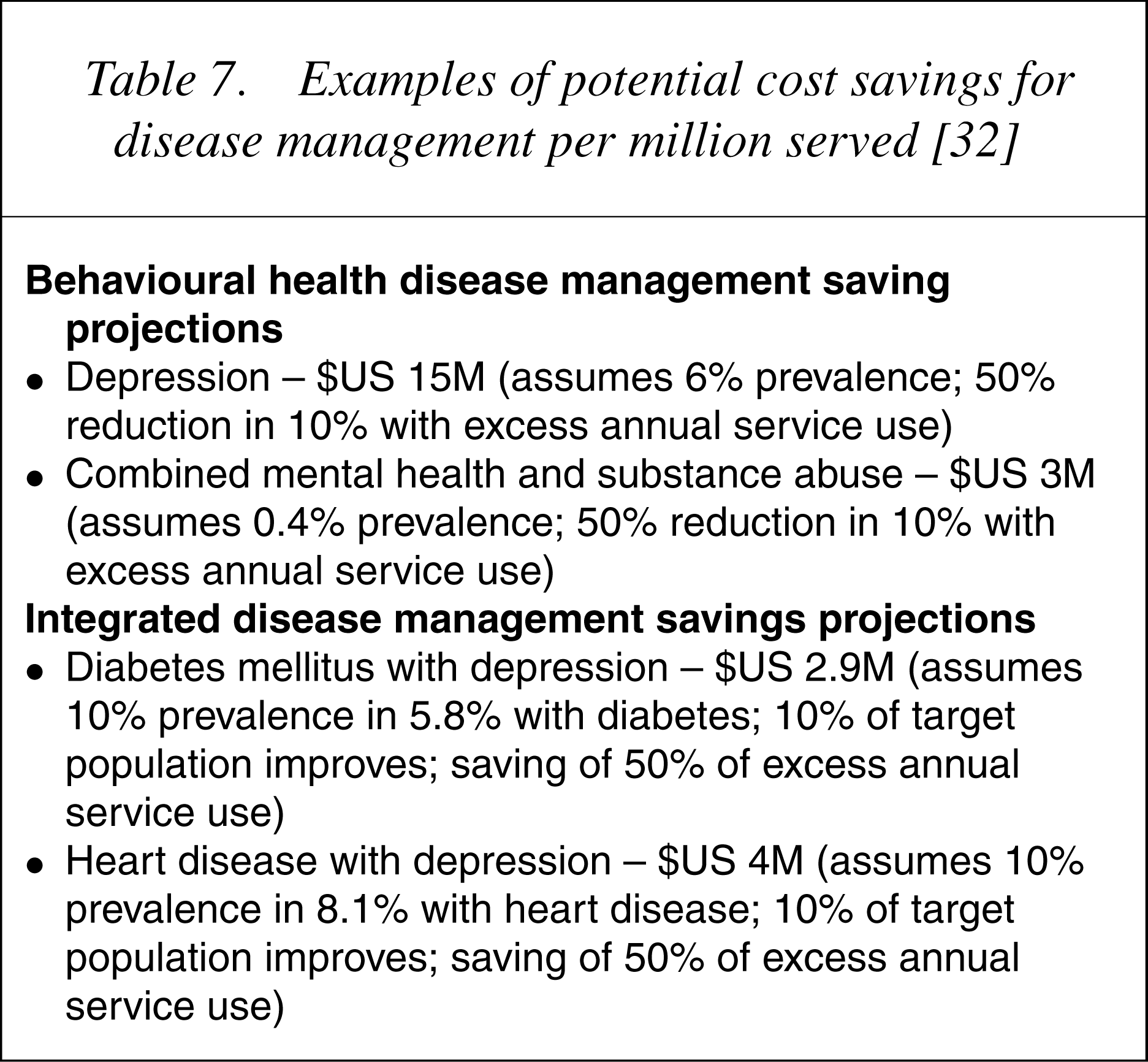
Since we are now able to prospectively identify high cost patients through predictive modelling and health risk assessments, it is possible to introduce cost saving techniques, such as disease and case management, designed to reduce service use by improving clinical outcomes in these patients. Disease management techniques augment clinician treatment and prevent high cost by assisting patients to better manage chronic illnesses through education about their health condition, better use of community resources, treatment adherence procedures and early identification of disease progression.
Examples of potential cost savings for disease management per million served [32]
Whereas disease management is more preventative in nature, case management falls at the intensive end of the care enhancement spectrum. It is designed to help patients who have spun out of control. Those who benefit from case management constitute the 5% of patients already using 50% of health care resources. Case management techniques are similar to disease management. However, the services are much more involved, requiring better trained clinical staff and a higher level of patient– casemanager interaction, than diseasemanagement. Case managers' primary responsibility is to assist treating clinicians at the site of care maximize improvement for the patient. Cost savings is a direct result of decreased service use in patients with improved clinical outcomes.
Although case and disease management are vehicles to maximize improvement in patients with the highest utilization of care, they are only as good as the clinical system in which they are instituted. Introduction of case and disease management practices brings value, however, when they are instituted in an integrated treatment environment, they can yield much greater clinical and economic results.
What is the best way forward?
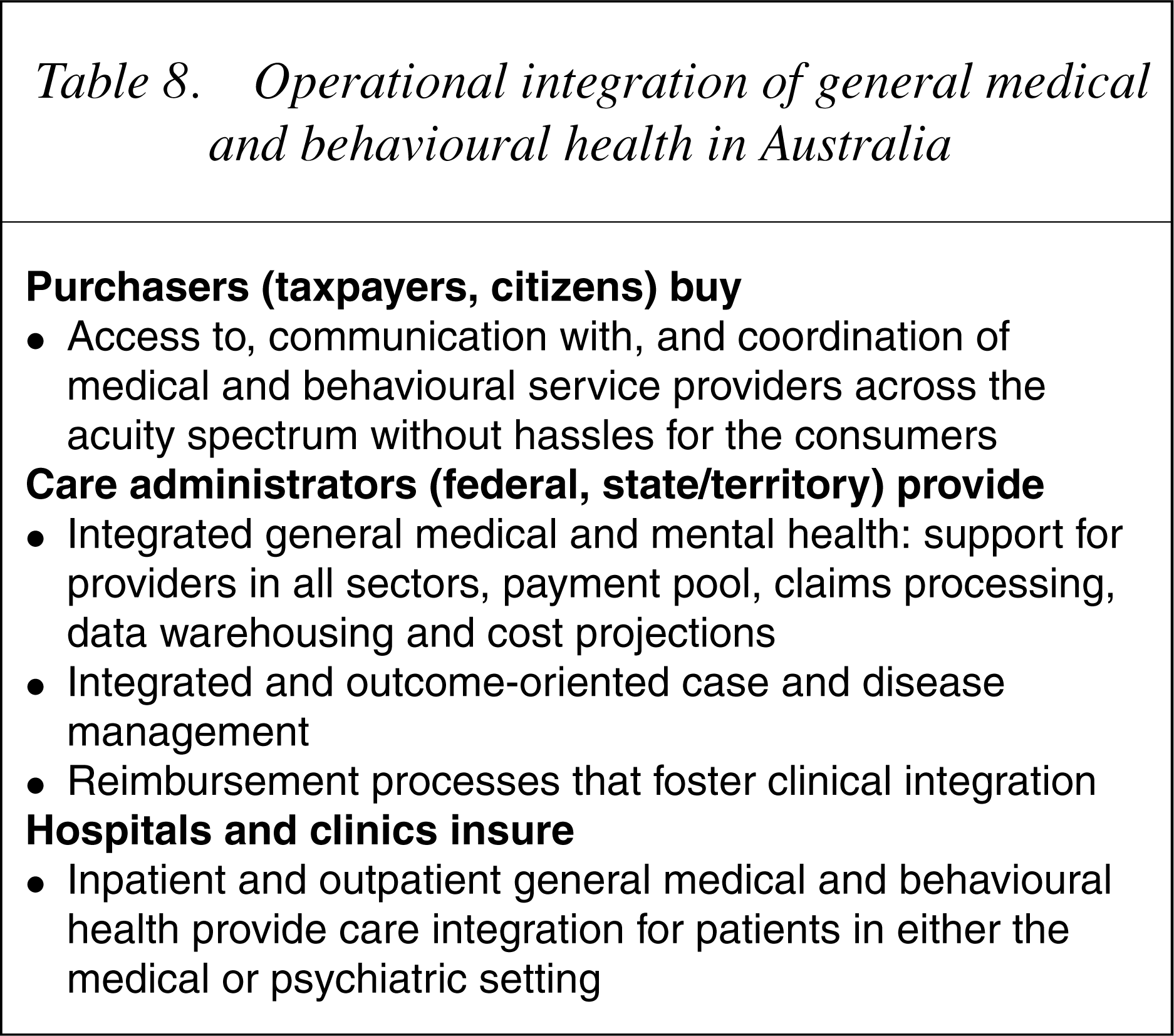
The first and most important step in this process is to ensure that the major stakeholders and decision-makers know that the poor clinical and economic outcomes associated with the independently managed system described above cannot be corrected without integrating medical and mental health personnel communication and work processes, in part through a common and seamless funding system and in part through a unified organizational structure. A good example of an attempt to coordinate general medical and mental health services without these core components being present was seen in the ‘mainstreaming’ aspect of the First Mental Health Plan of Australia [37]. An integral component of this plan was to emphasize and encourage mental health treatment in the general medical setting. Although the plan led to closer proximity of mental health and physical health service delivery and encouraged participation in mental health care by non-mental health professionals, it did little to support the coordination of medical and mental health and actually reduced the budget for mental health specialists practising within the medical sector [36]. Only with a single budget, and when professionals interested in outcomes for both medical and psychiatric illness regardless of clinical setting, accept accountability for the whole patient, will the integrated care occur.
Operational integration of general medical and behavioural health in Australia
Core components of integrated outpatient care
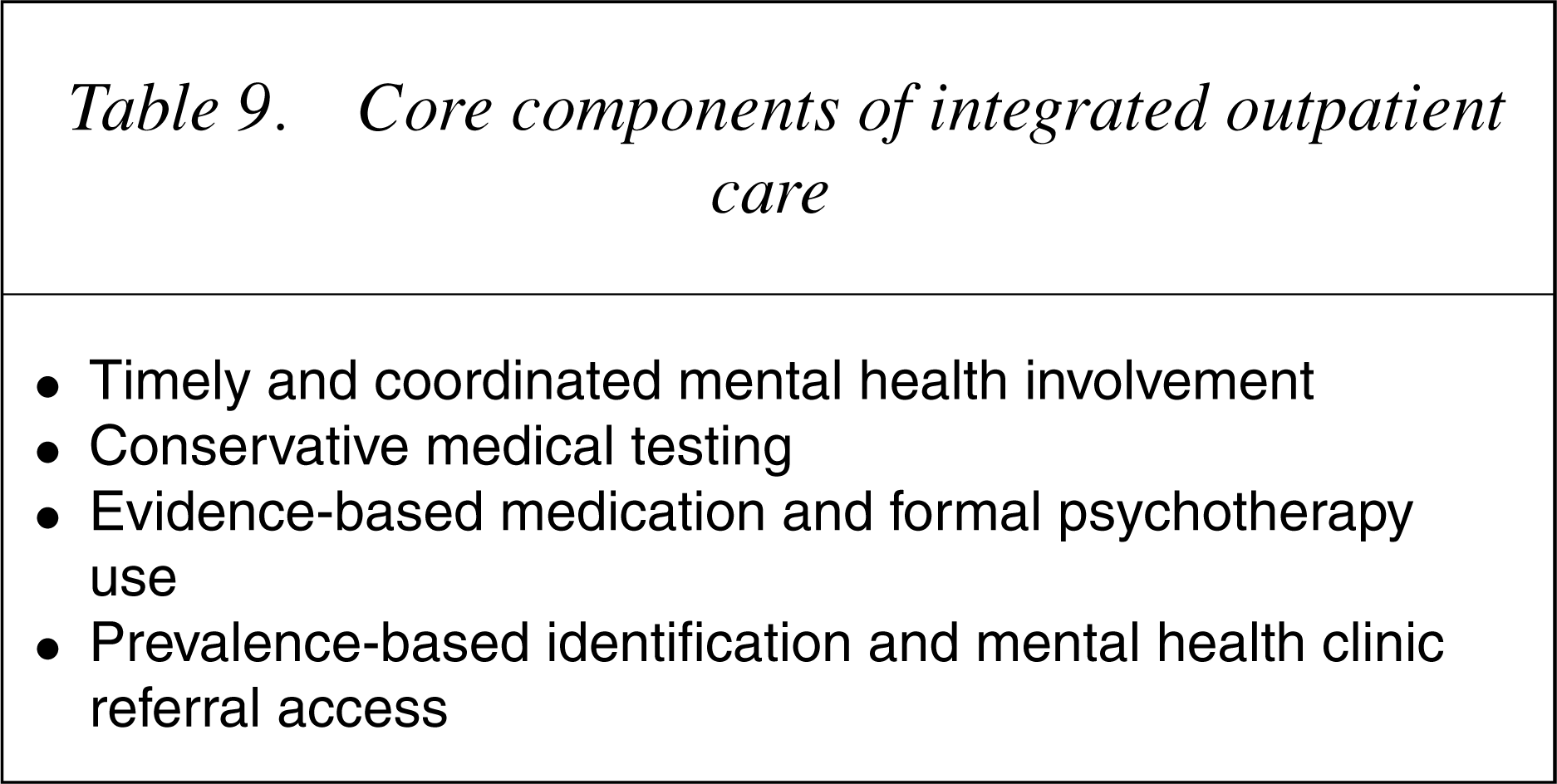
Timeliness usually requires the involvement of amental health team, composed of various mental health and substance use professionals, assisting non-behavioural health clinicians. These teams should be led by consultation– liaison psychiatrists who have the expertise to maximize care in these often complicated and high cost patients. Since there are too few psychiatrists to serve the large number of under-served or un-served patients at present, clinicians from non-behavioural health specialties will still need to assume clinical responsibility for following through on many of their patients' mental health needs, often under the supervision and/or with the assistance of their mental health colleagues.
Not onlywill primary and specialty medical care physicians accept increased responsibility for mental health care, they must also learn new ways to approach physical health test ordering and medication prescribing for those with mental health problems. The majority of excess cost in patients with comorbid illness is for medical services and medications [32]. It is now possible to alter this elevated service provision through training [39], [40]. In some patients, it will be necessary to use ‘re-attribution’ to reduce somatic preoccupation and cut down unnecessary medical service use. In others, with medical illnesses such as diabetes, it is important to ensure that patients adhere to care recommendations, that is, follow their diet, show up for appointments, take their medications etc., since their mental illness may make them less reliable in doing this for themselves. This is an area in which the value of case and disease managers comes into play, but, again, it needs to be a coordinated and collaborative effort by general medical and mental health professionals.
Finally, since the greatest value comes to patients who have complex, high cost illness, it is important to use proactive high risk case-finding. Primary and specialty care physicians are notoriously poor in identifying people with mental illness [41]. Since there are patients who use the greatest number of health care resources, it is important to actively identify them and attempt to alter their clinical course.
Core components of integrated inpatient care
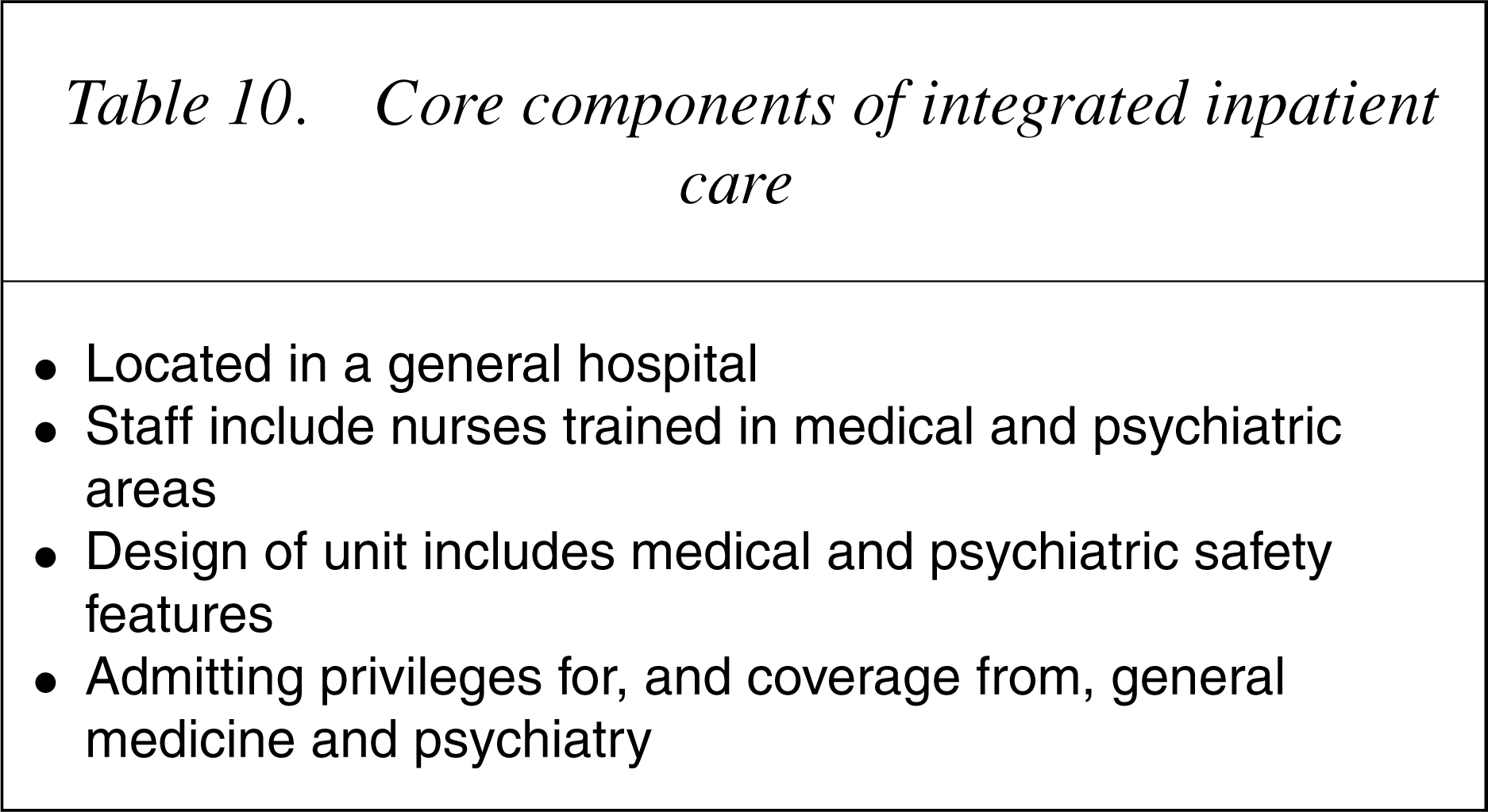
Finally, it should be stated that there has been a reluctance for psychiatry to endorse a move to become integrated with the rest of medicine for fear of losing what small support it receives for the services it provides. Evidence from the American system belies the sagacity of this argument. Between 1988 and 1998, a time when independent managed behavioural health was in its growth phase, the HayGroup [44] documented a fivefold decrease in the value of mental health care provision in comparison to general medical care (54.7% decrease in spending for behavioural health compared to an 11.5% decrease for physical health). Although it is possible that resources devoted to mental health care could be eroded in an integrated system, it would almost require wholesale abandonment of mental health care by the medical health system, an unlikely scenario in these days of scarce mental health service availability.
Conclusions
Independent general medical and mental health administration is associated with access to mental health and substance abuse treatment in less than one-third, and to minimally adequate treatment in one-tenth of all people with mental illness.
Mental health treatment in an independently managed health system shifts health care expenditures from the mental health to the medical sector and predicts a high total cost of care for mental health patients, primarily as a result of general medical service use and pharmacy. Future health system goals designed to rectify these negative clinical and economic effects should centre on system changes which foster the coordination of, and joint accountability for, general medical and mental health services. Competing general medical and mental health payment pools, as presently exist in the American and Australian systems, prevent the effective, efficient and economic integration of general medical and behavioural health services. Health systems cannot afford to continue to squander health care resources by ignoring the excess service use associated with segregated mental health and general medical administration. Changing to an integrated general medical and mental health system actually simplifies administrative and operational processes while leading to more effective and efficient clinical care and better health care resource use.
Footnotes
Acknowledgements
The authors acknowledge the contributions of Yasuhiro Kishi, MD (Japan), Frits Huyse, MD (the Netherlands), Kurt Kroenke, MD (US), Per Fink, MD (Denmark), Graeme Smith, MD (Australia), Chul Lee, MD (Korea), Albert Diefenbacher, MD (Germany) and Wolfgang Söllner, MD (Germany and Austria) who provided advice to the authors about the integration of general medical and mental health care, particularly as it relates to international practices within medicine in each of their countries.