
Abstract
Keywords
The problem
Despite the awareness that in addition to the biological determinants, psychological, social and cultural factors are also involved to varying degrees in the initiation, course and outcome of pathophysiological processes, insufficient attention is paid to their role in health and disease. The presence of physical and psychiatric comorbidity significantly enhances the complexity of assigning accurate diagnoses. Two domains of disorders may be at play, two genres of medications may be involved and doctors from two disciplines are engaged in deriving a diagnosis and constructing appropriate treatment recommendations. An example is the situation with ‘medically unexplained physical symptoms’, which presents an enormous dilemma for somatic physicians and psychiatrists alike.
The psychiatric taxonomy over the years has been insufficiently attentive to the way in which psychiatric diagnosis may be affected by the co-occurrence of physical illness. Physical symptoms may overlay psychiatric symptoms to the extent that the psychiatric algorithms do not apply. For example, DSM-IV [1] states that if symptoms such as insomnia, lack of energy, diminished libido and anorexia are considered secondary to a physical disease, they cannot be counted as vegetative symptoms for a diagnosis of depression. But clearly it is not an easy task for a clinician to know the origin of a symptom. Dysphoria in the patient with HIV/AIDS may emanate from the numerous medications prescribed, from the direct effect of the virus on the brain, from the patient's knowledge that he/she has contracted a potentially fatal disease, or from all three. Therefore, it remains a clinical judgement as to the aetiology of the symptoms, and treatment may have to begin before the true source of the dysphoria is known.
However, the ICD-10 [2], the most widely used of the diagnostic schemas, continues its practice of addressing only the traditional diagnostic classifications. Cooper elaborated upon these issues and the problems of its application in the medical setting at the primary care level and especially with psychosocial concerns [3]. The current glossary is not suitable for most medical practitioners. Both ICD-9 [4] and ICD-10 [2] have used a hierarchical structure. Clinical diagnostic entitieswith known biological aetiology are given pre-eminence. Functional psychoses, neuroses and poorly defined personality disorders are placed in a secondary position. Consequently, ICD-10 cannot be considered to be conceptualized as a triaxial diagnostic model: biological, psychological and social [2]. Nor does it encourage understanding of the interaction of these three sources of symptoms – the mechanisms that underlie the influence that one has upon the other – the biopsychosocial model.
There is another diagnostic issue that obtains and is not well served by the main taxonomies. The clinician's inability to secure a diagnosis may be resultant of the fact that psychological, social and/or cultural determinants are not sufficiently developed or apparent, especially in the primary care setting where physicians may see patients early in the course of their disorder, and the symptoms have not ‘matured’ enough to allow a specific diagnosis – the symptoms remain in a preclinical phase. To cope with this earlier, indeterminate phase of illness in primary care, two alternative taxonomies have been developed. The National Ambulatory Medical Care Survey emphasizes a modular classification of the patient's ‘reason for visit’ [5]. The International Classification of Health Problems in Primary Care (ICHPPC-2) [6] asserts that many patients will remain at the problem level of diagnosis rather than reach a systematized medical diagnosis. It is given that the ‘form fruste’ of a disease may not have emerged, that certain patients with problem level assessments will not go on to develop full-blown disorders, and that the primary care physician will need to accept the reason for the visit, or ‘problem level diagnosis’ as the best level of diagnosis that can be achieved for this patient at that time. In some circumstances, it is just not possible to make a reliable or valid traditional diagnosis, so the patient is left with a diagnosis of chest pain, nausea, diarrhoea and so on – but not an underlying illness diagnosis. It is important to note that as many as 50% of patients in primary care settings remain at the ‘reason for visit’ level of diagnosis [5].
Kleinman, using anthropological techniques, has attempted to describe illnesses in yet another way: The Patient's Explanatory Model [7]. This model considers culture and the context in which the illness occurs (e.g. ethnicity as a factor in the expression of pain). It attempts to take into account the patient's view of the cause of the illness and its pathophysiology, and of its expected course and the treatment that the patient anticipates may be administered, for example, given an antibiotic. This adds a dimension to the diagnosis from the patient's perspective, and may eventually help with compliance problems that may arise in cases where the patient feels that they are not understood, or that the wrong treatment is being used.
When confronted with diagnostic ambiguity, the physician may be inclined to make unjustifiable psychiatric diagnoses such as malingering, hypochondriasis, somatization, depression, anxiety and so on. It is incumbent on the physician to be aware of tendencies to offer a psychological diagnosis as an expression of his/her frustration, and his/her belief system. The physician needs to be aware of ‘hidden disease’ – disease not yet observable, preclinical or beyond current techniques to detect. The physician also needs to be wary of using a premature physical diagnosis when faced with ambiguity, which he/she might do because of his/her belief system, fear of missing something or fear of upsetting the patient by failing to provide some diagnosis.
Triaxial and biopsychosocial models
The World Health Organization has promulgated studies to develop a triaxial diagnostic schema that includes tracts for psychological and social problems to accompany the biological or physiological tract [8]. In consonance with this approach, several investigators have developed measures for the identification of non-specific psychiatric dysfunction in the medical setting: the General Health Questionnaire [9], the Cornell Medical Index [10], the SCL-90R [11], the Problem Appraisal Scales [12] and the Present State Examination [13].
The DSM-III and its subsequent iterations were introduced as a multiaxial approach to the rendering of complex and multisystems diagnoses [14]. Axes I and II are psychological (state and trait disturbances), axis III is biological and axes IV and V are psychosocial (stressors and level of functioning). This strategy attempts to focus the clinician on attending to three conceptual levels of organization for a comprehensive diagnosis. It also attempts to enhance reliability by having preset algorithms for observable phenomena rather than permitting subjective impressions of poorly measurable thoughts and behaviours. It has an atheoretical conceptual framework. It was anticipated that the consideration of all three domains would enhance the clinician's understanding of possible relationships among these levels of organization: for example, congestive heart failure (axis III), delirium (axis I), impaired functioning (axis V) and a stressor – serious illness (axis IV). However, DSM-III did not emphasize a combinant or interactions explanation for the findings on these disparate axes. That is, it did not represent amodel of a biopsychosocial integrative statement of disease mechanism(s) that might have ensued from one dimension impacting upon another, as Engel elegantly opted for in his proposal of the model in his article in Science in 1977 [15]. However, the provision of the possibility to list ‘no diagnosis’ or ‘deferred diagnosis’ gives encouragement to the clinician to record a negative or uncertain position rather than latch on to a diagnosis that is likely to be wrong.
Another limitation of psychosocial diagnoses in the medical setting emanates from the fact that many of the issues are not necessarily traditional psychiatric diagnoses: non-compliance, bereavement and so on. DSM-IV managed this by adapting V Code classifications (from ICD-9-CM) for conditions not attributable to a mental disorder but nevertheless are a focus of treatment and intervention. They are used when no mental disorder per se has been found. Even though definitions are provided, the V Codes are neither reliable nor necessarily valid. No diagnosis is an acceptable alternative and should be encouraged rather than risking a misdiagnosis. The adjustment disorders category is another diagnostic group with questionable reliability and validity, but one of the most commonly used diagnoses in the medical setting [16]. A multinational study which included Monash Medical Centre (Melbourne, Australia) and Mount Sinai Medical Center (New York City, US) described the demographic attributes of this cohort and the characteristics of their medical comorbidity in disparate sites [16].
Limitations of DSM-IV in the medical setting
DSM-IV constitutes an important step in the evolution of psychiatric taxonomies in regard to making diagnoses more reliable, and questionably more valid. However, it poses major problems when applied in the medical setting and in patients with physical symptoms that are included in algorithms for psychiatric disorders. For instance, DSM-IV requires that if a symptom is judged to be secondary to a medical illness it should not be counted in the algorithm supporting the diagnosis of depression. But, not to count these vegetative symptoms may result in under- or misdiagnosis of a depressive disorder. The dilemma is that the clinician often neither knows the source/aetiology of these vegetative symptoms nor is it easily, or in some cases ever, discernable. This presents an enigma: count the vegetative symptoms and possibly overdiagnose depression in the medically ill; or do not count vegetative symptoms in the algorithm for depression and risk underdiagnosis. A third approach proposed by Endicott is to replace the vegetative symptoms with ideational or emotional symptoms, for example, ‘feeling blue’ [17].
Koenig et al. compared schemas that were all-inclusive of symptoms regardless of their origin – physical or psychological – with those schemas that excluded questionable symptoms that could be attributed to medical illness, in hospitalized older adults [18]. They examined the prevalence, characteristics and course of symptoms according to six diagnostic schemes: inclusive, exclusive, exclusive–inclusive, exclusive–aetiological, substitutive and substitutive–aetiological. There was no difference with regard to predictive or convergent validity among the six schemas. ‘Although diagnostic strategy affects rates of major and minor depression offering a twofold difference between extremes, there is little reason to choose one diagnostic scheme over another in all cases’ [18]. None of these courses of ‘corrective action’ necessarily enhance validity, a major issue with the diagnosis of depression in the medically ill. Even persistent dysphoria and/or anhedonia (two of the primary symptoms in the diagnosis of a major depressive disorder) may be secondary to a medical illness.
There is a comparable problem with the diagnosis of anxiety, where the DSM-IV algorithm includes physical symptoms. Which symptoms emanate from physiological sources and which are of psychological origin? What would look to be at first glance an easy and reliable call of observable phenomena, in fact, relies on a judgement call of the specific origin or aetiology of these observable symptoms. The issue of aetiology of symptoms with psychiatric and medical comorbidity remains a chief stumbling block for the establishment of validity of psychiatric diagnoses in themedical setting. Reliability is enhanced by a phenomenological approach to diagnosis, but validity is sacrificed.
With regard to somatoform disorders – one of the most difficult and problematic of psychiatric diagnoses – there is considerable overlap in the criteria for the diverse diagnoses that the category includes. For instance, conversion reactions may be seen in psychogenic pain and somatization may be observed in hypochondriasis. Although in DSM-IV pain has been given its own category and several possible kinds, and psychogenic pain is not labelled a conversion reaction, the underlying mechanism involved in its formation is often conversion. A mechanism of origin statement would facilitate the validation of this diagnosis more than relying on phenomenological issues only.
McHugh and Slavey expand on how validity has been sacrificed for reliability in the American Psychiatric Association approach to diagnosis in their taxonomy DSM-IV [19], [20]. Although a description of observable phenomena may be the easier approach to reliability and communication issues, a dynamic understanding of the cause and meaning of the patient's symptom(s) is often a prerequisite for diagnostic accuracy. Specifically, the diagnosis of the somatoform disorders may hinge on a psychodynamic description that outlines past and present causal events in terms of conflicts and developmental issues as they relate to symptom formation. ‘The problem in dealing with the somatoform disorders from a purely symptomatic point of view in the medical setting is the failure to emphasize the connection between symptoms and personality diagnosis (the interrelationship between axes I and II), and the spectrum concept of disability, for example, fairly benign hypochondriasis as opposed to a malignant form [20]. The hypochondriacal patient, like the one with somatization disorder, uses conversion mechanisms extensively, and both may be convinced to varying degrees that they have a serious disease – the difference really being one of degree of personality dysfunction’ [20]. Grossman has also compared the DSM-III with the somatoform disorders [21].
DSM-IV for primary care physicians (DSM-IV®_-PC)
It was considered important to adapt the standard psychiatric taxonomy to the primary care setting. Since primary care physicians (PCP) are usually the first or at times the only physician to have contact with patients who have mental disorders, it is essential that they have access to a tool that would help them to identify and categorize mental disorders as they present in their unique medical setting. One goal was to have a taxonomy that was compatible and conversant with the management style of a PCP's practice.
DSM-IV®_-PC has been engineered to be compatible with DSM-IV-TR [22] and ICD-9-CM [4]. Its unique features include listing the commonly seen psychological and mental conditions in order of their occurrence in the PCP setting. It attempts to begin with symptom conditions and migrates to diagnoses using an algorithmic format to assist the PCP in reaching their diagnostic formulation. It takes into account the perspective that the PCP often deals with problems that do not necessarily go on to reach a diagnosis per se, but still require attention and treatment. In this sense, it is like ICHPPC-2 [6], a problem-oriented taxonomy, but in addition guides the PCP to accurate psychiatric diagnoses using algorithms and practical information to enhance diagnostic decisionmaking. This psychiatric diagnostic and teaching tool for mental symptoms and disorders in the primary care setting has been strongly influenced by the practitioners for whom its use was intended. It was formulated and reviewed by many primary care specialty groups, for example, American Academy of Family Physicians, American Academy of Pediatrics, Society of General Internal Medicine, Society of Teachers of Family Practice and others. However, many of the questions and limitations regarding validity and reliability, comprehensiveness and dimensions of diagnoses described for the DSM-IV-TR [22] above also pertain to the DSM-IV®_-PC [23].
McHugh and Slavney's perspective approach to diagnosis
McHugh and Slavney have articulated with great precision a manifesto for altering our approach to psychiatric diagnosis, and for the need of a more comprehensive taxonomy for our field in the second edition of Perspectives of Psychiatry [19]. Much of what follows comes from a summary of McHugh and Slavney's writings as reported in the Psychiatric Research Report published by the American Psychiatric Association Division of Research (summer 2001) [20].
The authors summarize three epochs of diagnostic conceptualizations in US psychiatry [19]. Psychobiology (1910–1940), founded by Adolf Meyer who coined the term, emphasized psychiatry as the study of life at the psychosocial level rather than focusing on biological psychiatry. It required a complete history and a full mental status examination. Psychoanalysis (1940–1970) deemphasized biological contributions and diagnosis. The Empirical epoch (1970–2000) saw the development of DSM-III, DSM-IIIR and DSM-IV as atheoretical conceptual frameworks based on appearance as already described, sacrificing validity for reliability and omitting other salient dimensions. McHugh and Slavney continue, ‘interestingly enough, medicine as a discipline abandoned appearance driven diagnoses (fever, anaemia etc.) many years ago and moved its taxonomy ahead by taking to account mechanism wherever it could. This evolution aided validity and specificity which in turn enhanced accurate and more appropriate treatment approaches’ [20].
McHugh and Slavney suggest that psychiatric diagnoses must reside on their distinct and essential nature and on the patient's overall psychological life. They have formulated four perspectives of psychiatry and established a conceptual framework looking at each perspective from several points of view.
It is the sum of these four perspectives that renders an understanding of the patient and a comprehensive diagnosis that permits sufficient awareness to have treatment take place on several contextual levels simultaneously. Thus, diagnosis encompasses more than a symptom profile, more than an algorithm, and more than what is registered on a scale. It encompasses multiple aspects of a patient's mental life, their culture and their own perspective of what their symptoms mean [7]. McHugh and Slavney conclude that the next generation of psychiatric taxonomies and their diagnoses must include at least some features from these four dimensions and not just be based on the atheoretical appearance of symptoms [19]. McHugh believes that the creation of DSM-V should await a different theoretical and conceptual framework for its construction; to recapitulate the format of DSMIV and DSM-IV-TR will not move the field forward in the important area of diagnosis [McHugh PR: personal communication].
Need to see psychiatric disorders in a new light: depression as a systemic illness – of brain, mind and body – with systemic consequences
Depression has until now in this discussion been presented as a psychiatric diagnosis with vegetative, ideational and mood-disturbance symptoms. However, in the twenty-first century, depression, especially major depressive disorder, is being conceptualized as a systemic disorder with major somatic components including appetite, energy, libido, and sleep disturbance and ideational signs including helplessness, hopelessness, guilt and suicidal thinking, in addition to a changed activity of the hypothalamic pituitary axis and the consequent effects on the cardiovascular system and on systemic disorders. We have evidence now that depressive symptoms are associated with increased risk for the development of increased morbidity and mortality with coronary heart disease and stroke [24–27], and with poor glycaemic control in type 1 or 2 diabetes [28].
This section will focus on the relationship between major depressive disorder and the cardiovascular system. Major depressive disorder is reported in 8% of patients and depressive disorder of any type in 15–36% of inpatients in general hospitals [29]. It is estimated that 15–23% of postmyocardial infarction patients experience major depression [30]. Depression and its associated symptoms are independent risk factors for the development of coronary heart disease and/or death after an index myocardial infarction. Frasure-Smith reports depression to be a significant predictor of mortality (p<0.001) 6 months following a myocardial infarction [31]. Multivariate analysis showed that depression was a significant predictor of mortality after accounting for other important risk variables: the effects of left-ventricular dysfunction, previous myocardial infarction and premature ventricular contractions.
The risk potential from depression occurring simultaneously with coronary heart disease is equivalent to that of diminished left-ventricular function and the past history of having had a myocardial infarction [30]. It was also reported that a new onset depression was at greater risk than chronic or recurrent depression. Several additional findings have been reported [30]. Depression is a risk factor in postmyocardial infarction patients for ventricular arrhythmias and sudden cardiac death. Elevated Beck Depression Inventory scores were a more powerful predictor of mortality for those patients with greater than 10 premature ventricular contractions and for those with diminished heart rate variability – a well-known risk factor for mortality.
Biological alterations in depression postulated to be related to outcome in coronary heart disease include: (i) sympathoadrenal hyperactivity; (ii) diminished heart rate variability; (iii) ventricular instability; (iv) myocardial ischaemia secondary to mental stress; (v) alterations in platelet receptors and/or reactivity; (vi) increased corticotrophin-releasing factor; (vii) increased release of corticotrophin (adrenocorticotropic hormone); and (viii) increased B-endorphin [30]. 30].
Hypothetical schema of pathophysiologic alterations associated with depression that likely contribute to increased vulnerability to cardiovascular disease (CVD). Autonomic nervous system innervation of the heart via parasympathetic vagus (X) and sympathetic (postganglionic efferents from cervical and upper thoracic paravertebral gangila) nerves is shown. CRF indicates corticotropin-releasing factor; ACTH, corticotropin; TNF-α, tumor necrosis factor α, IL-1, interleukin 1; IL-6, Interleukin-6: HRV heart rate variability; and HPA, hypothalamic-pituitary-adrenocortical axis.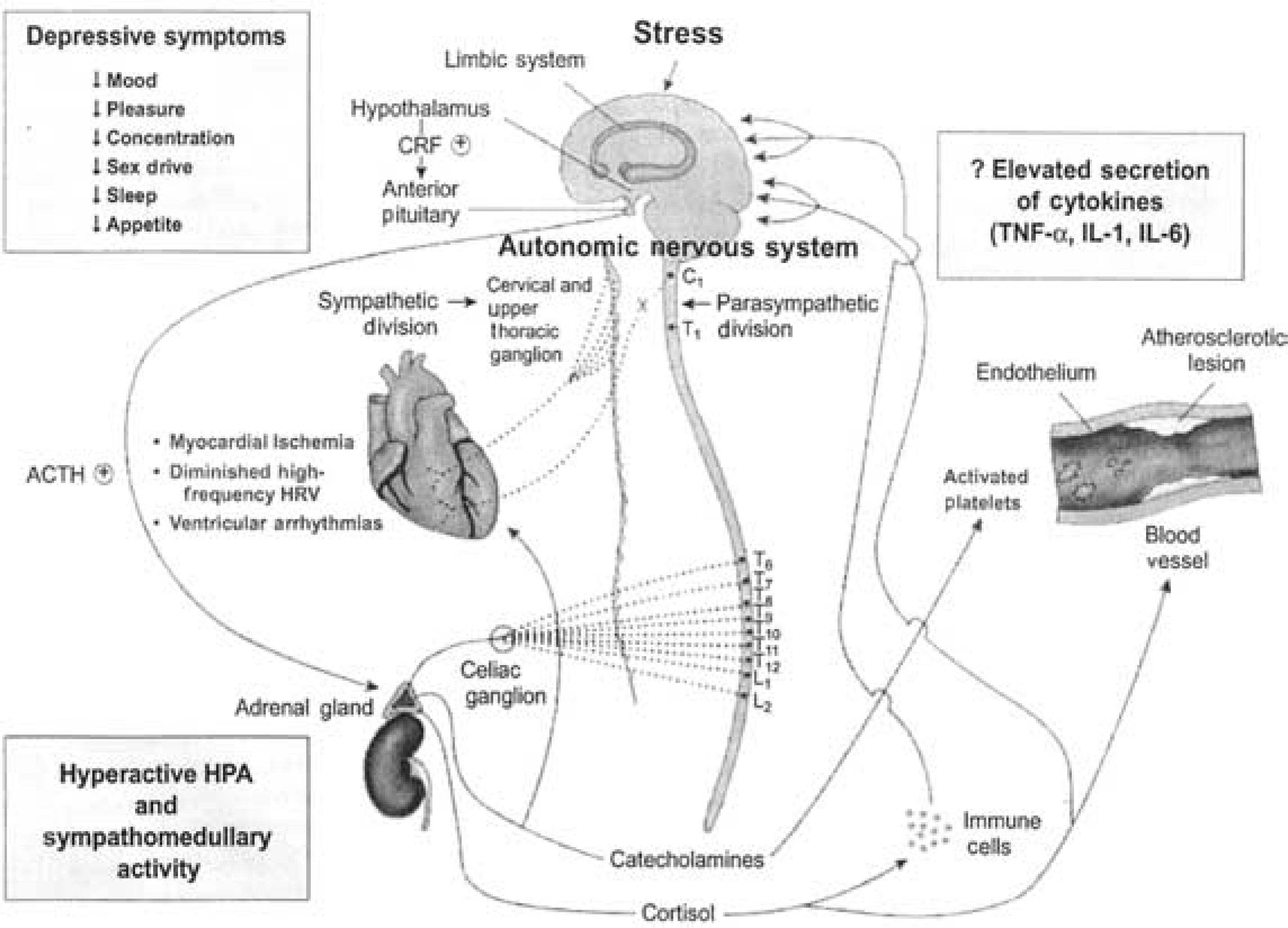
Depression is a common finding after cerebral vascular accident (CVA) with Robinson reporting that frontal, non-dominant CVAs aremore commonly associated with depression [32]. Cerebral vascular accidents present an additional confound in diagnostic accuracy where consciousness is interfered with and/or the clinician has to deal with aphasia, as happens in other disorders affecting brain function. Cerebral vascular accidents were 2.3 times more frequent in elderly who were also depressed [32]. These findings are relevant to the thesis that depression should be considered a systemic disease, not just a mental illness. The relationship between depression and CVA may operate through similar mechanisms to those proposed for myocardial infarction, for example, platelet activation [30]. Robinson has expressed the view that all patients who have had a CVA be placed on an antidepressant, as a prophylactic to minimize the complications and additive risk that depression provides, regardless of the evidence for the presence of a depressive disorder [Robinson RG: personal communication].
Pain and depression are also intertwined clinically and therapeutically, and recent evidence about their neural basis and pathways gives some support to the hypothesis that depression is a systemic illness [33–35].
Future considerations
Future psychiatric diagnostic taxonomies need to have several amendments to make them relevant even at our current level of knowledge. First, they must find some way to deal with medical comorbidity and the contribution that medical symptoms and illness make to the symptom picture that the clinician observes. There is a need for scales and measures that could account for the contribution of medical illness. The Beck Depression Scale is heavily cognitively laden while the Hamilton Depression Scale has many vegetative signs and symptoms questions. Second, the next generation of taxonomies must include at least some features from the four dimensions that McHugh and Slavney have outlined, and not just the atheoretical appearance of symptoms [19]. Psychiatry needs to learn from medicine that the superficial counting of symptoms may enhance reliability but it does not enhance validity. Diagnosing an illness requires more than merely a symptomatic understanding. Third, upcoming taxonomies need to take into account gender, age, race and ethnicity. Fourth, assessment instruments need to consider an array of biopsychosocial variables to achieve greater reliability and validity of the diagnostic impression. Clarke et al. have developed the Monash Instrument for Liaison Psychiatry [36]. This is probably the most comprehensive measure currently available to assess the patient in the medical setting for psychiatric morbidity. It is replete with biopsychosocial variables, which permits the rater to make a diagnosis according to the main taxonomies, and allows for the creation of new ones as well. Finally, the future of diagnosis in psychosomatic medicine and patients with psychiatric and medical comorbidity will require that we have: (i) molecular targets; (ii) better animal models; (iii) new molecular libraries; (iv) new diagnostic systems that would include pathophysiological genotypes; and (v) neurobiological phenotypes [37].
The diagnostic algorithms for children, youth and adolescents may differ from those for adults. For instance, anhedonia is a key symptom in youth and adolescent depression. Geriatric medicine and paediatric physicians are very aware that their patients need a different type of assessment and different doses of medication compared with midlife adults. These algorithms need to be amended as new knowledge shows differences in these cohorts. There will eventually be biological and genetic markers that will assist both diagnosis and knowledge of recovery from illness. For example, A1C haemoglobin accurately indicates if a patient has diabetes, the degree of severity and the improvement if any from treatment.
Goldberg in his seminal studies to elucidate the variance between the diagnostic capability of PCP to detect or not detect psychosocial or psychiatric disorders found that the ability to detect was closely related to the doctor's ‘interest and concern’ (40%) and ‘conservatism’ (18%) rather than to his/her psychiatric focus (5%) or length of the medical interview (3%) [9]. Doctors who took longer to interview did no better than those that hurried, and ‘none of the many forms of non-verbal behaviour measured in the doctor were predictive of his ability to detect psychiatric morbidity’. Goldberg developed a scale – The General Health Questionnaire – to assess the presence of ‘caseness’ in a patient, that is, the presence of psychosocial or psychiatric problems. This scale did not offer a diagnosis per se, but it did alert the physician to further pursue questioning to elucidate difficulties in the psychosocial domain.
‘Alerts’ that would draw the physician's attention for the need for more comprehensive psychosocial assessment would be a most important contribution to achieving the appropriate diagnosis. ‘Medically unexplained symptoms’ often by default are classified as psychiatric. Rather they may be subclinical; presyndromal – early stages of an unfolding illness, or in contrast, in the recovery phase of an illness that is responding. In such cases, it would be much better to use the categories ‘no diagnosis’ or ‘deferred diagnosis’ than automatically use a psychiatric label. It is important to note that the editors of the DSM-IV felt it incumbent to have a form of that diagnostic manual shaped for primary care clinicians to facilitate their accuracy in making psychiatric diagnosis [1]. It remains a question as to the effectiveness of this strategy to enhance diagnostic accuracy.
Strain et al. [38] have developed a computerized database system – the Microcares Software Program – which emphasizes alerts to: (i) caseness before the physician's initial encounter; (ii) diagnostic specificity; (iii) drug and physical status interactions; (iv) drug–drug interactions; (v) compliance; and (vi) patient outcome. This enables the physician in the medical setting to be alerted to problems throughout the history, physical, diagnostic, treatment and outcome phases of psychological interventions with the medically ill.
Huyse et al., working with the European Consultation Liaison Work Group, have developed two measures that will alert physicians to medical patients who will need complex care: the COMPRI and the INTERMED[39], [40]. These assessment instruments produce a statement of the likelihood of need for complexity of care at admission to the general hospital, and give a forewarning of its nature.