
Abstract
Surprisingly little attention has been paid to a key aspect of consultation–liaison psychiatry (CLP) – how to communicate with medical and other health professionals who request specialist assistance. We are concerned here with the written report, one of a series of tasks that comprises effective consultation. Determining the purpose of the consultation for instance (e.g. a complex diagnostic puzzle, an aggressive patient, a frustrated nursing team) is a prerequisite [1]. Furthermore, the report occurs in a framework that is influenced by other kinds of communication [2]; verbal exchanges, joint ward rounds and sharing at grand rounds. In short, the CLP consultation does not solely depend upon the written report but is enhanced by its form and content.
The written report must fulfil a range of functions if it is to be of use. CL psychiatrists need to communicate in a way that makes their findings and recommendations readily understandable [3], but at the same time they are commonly constrained by the principle of respect for privacy from recording intensely personal information which is then accessible to colleagues and students not directly involved in the patient's care.
A review of CLP literature reveals only one contribution, which is two decades old, that offers comprehensive guidelines [4]. Yet its lack of specificity to CLP regarding the recording of history and formulation details militates against its use. Some contributions to the subject [1, 5–8] do not address practical questions of what should be covered in a written report. Others focus on diverse aspects such as the task's complexity; referrers valuing different aspects [9]; ethical and medicolegal imperatives [1, 4, 8, 10–12]; the need for standardized approaches to facilitate research and audit; [7–11, 13, 14] and typical shortcomings of customary practice [15, 16]. Contributions such as these fail to provide guidelines on a comprehensive format.
Having scrutinized our own practices, conferred with CLP colleagues and evaluated the literature we conclude that exploring the written report aspect of CLP is overdue. To this end we have tackled the following questions: Is there an optimal form of the CLP written report? What is the rationale for this task? and What should a comprehensive report contain? Our purpose is to propose a schema that takes the functions of the report into account, so leading to effective collaboration between referrer and CLP clinician. We suggest psychiatric trainees use the schema during their CL term. We also recommend that it be preprinted in the same way as admission ‘packages’ in other areas of mental health service, and be incorporated in the section of the patient's file for that particular period of inpatient treatment.
Method
Our first step – to peruse textbooks on CLP [5, 17–20] – proved disappointing given the minimal attention paid to communication by these sources. We then reviewed the relevant literature using Medline and Psychlit. To complement these two steps we sought the views of our local CLP team that assembled on four occasions to explore the topic. Through this process we were able to map out a practically useful schema.
Results
Functions
The first step in developing our schema was to pinpoint the core functions of a CLP report. We summarized these as follows:
– to highlight relevant findings and their implications for outcome and treatment in a comprehensible form;
– to provide recommendations for treatment;
– to offer advice regarding follow up; to ensure continuity of care. Other functions are:
– to contribute to the education and training of those preparing or receiving a CLP report;
– to fulfil an archival role so as to inform future assessment and treatment;
and to satisfy the medico-legal expectations of a specialist consultation.
With these functions in mind we can turn to our schema (see Table 1). We shall elaborate on Table 1, providing the rationale for, and issues arising within, each section. Second, we shall illustrate the schema's application with our own clinical work (patients’ identities have been disguised).
Sections of the proposed consultation—liasion schema
Who is the patient?
The referrer's name, CL assessor's name, date of referral, and date/s of consultations are clearly cited at the beginning of this section. Then follows a ‘portrait’ of the referred patient, typically covering sex, age, ethnicity, religious affiliation, marital status, occupation, migrant status and pertinent life circumstances. Brief acknowledgement of any past psychiatric or medical illness is appropriate here, but shorn of detail. It is followed by a statement of the current illness.
Why you referred the patient to us at this particular time?
The task here is to crystallize the question(s) posed by the referrer. Given that these may be brief and cryptic, the assessor may extrapolate from other sources (e.g. information provided by the referrer over the phone or during a ward round). Other entries in the file are additional sources of information. A typical question is: ‘Is this patient depressed?’ However, on reading the entire request (in conjunction with clinical data ascertained in the above ways), it may emerge that the primary concern is suicidal risk or managing behaviour that is jeopardizing good nursing care. The temporal reference prompts the assessor to enquire about issues which may have a direct bearing on management (e.g. the patient may have refused assessment earlier, or discharge may be pending and psychological issues have been identified as effecting discharge planning).
What did we find?
Relevant clinical features, including notable negative findings (e.g. no suicidal ideation), are recorded here. The informant's verbatim comments are incorporated wherever possible, so enlivening the report and facilitating accuracy of material gained. Any discrepancies are spelled out (‘The nursing staff state… whereas the patient…’). If the patient was unaware of the consultation request this should be recorded along with his or her reaction. This may reflect dynamics with the referring unit that need addressing. Psychiatric findings are juxtaposed alongside pertinent clinical data (e.g. marked anxiety in the context of dramatic worsening of chronic obstructive airway disease).
The medical condition(s) for which the patient is being treated are pivotal to the report. This is straightforward when the condition is acute, short-term or secondary to the psychiatric state (e.g. selfinflicted injury). The link is more complex where the medical or surgical condition (e.g. multiple sclerosis, diabetes or epilepsy) either acutely or chronically predates or merges temporally with the psychiatric features. Repetition of medical details well known to the referrer is obviously superfluous but a brief summary of the physical illness, current symptoms, and past and current treatment helps to orientate all participating clinicians.
Summarizing the effects of the condition on the patient's life and their responses to the illness is salient, informing treatment decisions. This includes their mode and effectiveness of coping. Cognitive, emotional and behavioural dimensions apply. What the illness means to the patient and their understanding of its causes, prognosis and treatment are central cognitive elements. Fear, anger, guilt, shame, hopelessness, demoralization, helplessness and sadness are common emotional reactions. Behavioural patterns are many and varied, including dependency, fatalism, non-coperativeness, stoicism, motor retardation, attentionseeking and aggression directed to oneself or others.
Mental state findings are noted, with emphasis on features that point to immediate risk assessment and to likely psychiatric diagnoses. The level of detail depends on the particulars of the case. For instance, a complete cognitive examination is essential when an underlying dementia is suspected, and a comprehensive appraisal of affect in the case of a reported mood change, and a thorough assessment of thought content and form in a possibly psychotic patient. A methodical description of insight and judgement complements earlier observations regarding responses to illness. Given that a CLP consultation is rarely initiated by patients, their attitudes to potential psychiatric interventions are of particular relevance.
Who are the patient's family and other supports?
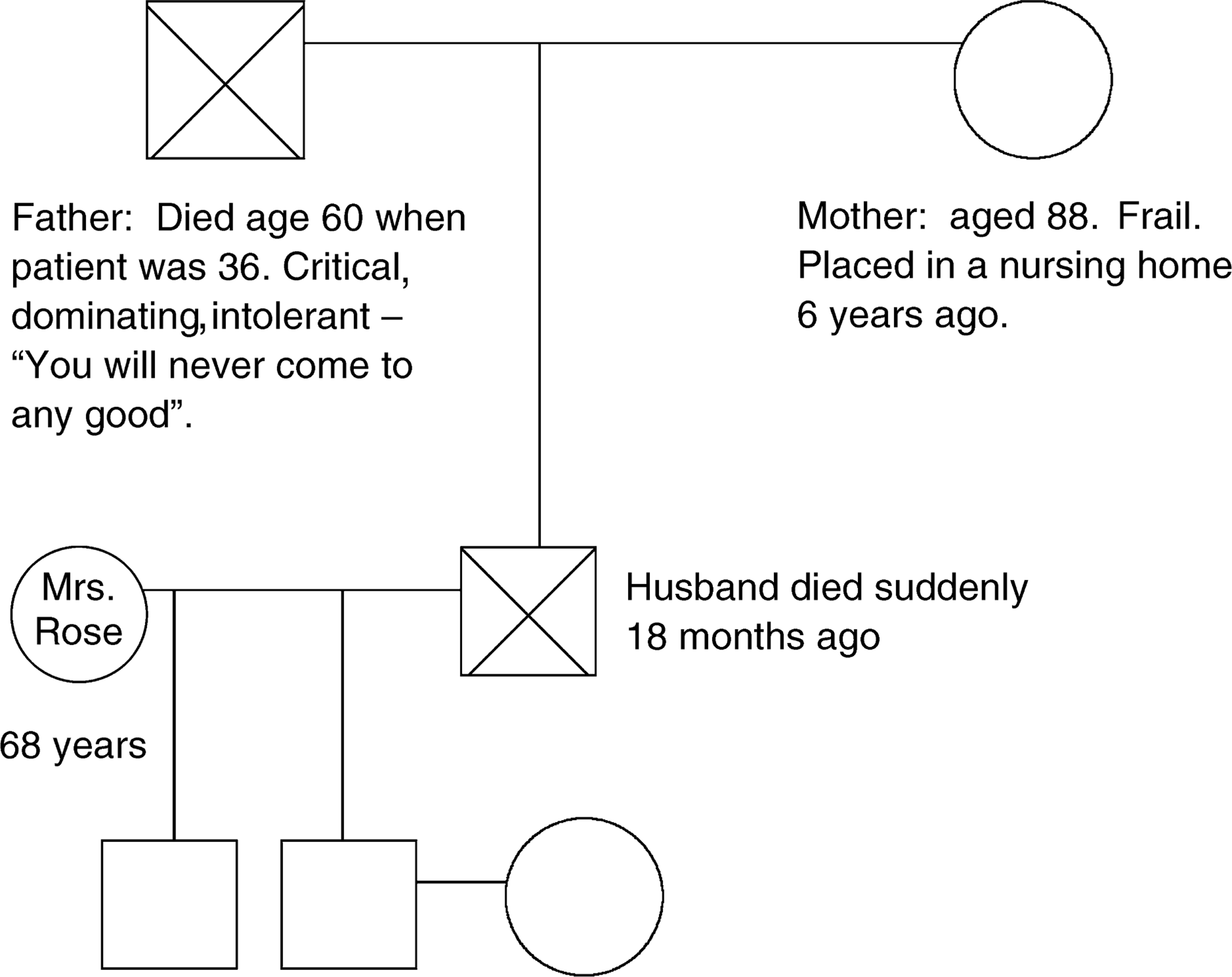
This section is virtually always applicable in one measure or another. An annotated genogram is invaluable (see Fig. 1 & Fig. 2); moreover it conveys substantial clinical data. The family structure is graphically presented using conventional symbols. An account of family functioning is highlighted by brief annotations on the genogram itself. Any relevant family medical and/or psychiatric history is a critical ingredient in contributing to an understanding of the patient's clinical features – not only the ‘facts’ but also perception and fantasies. Apart from immediate relatives the extended family and significant other figures (e.g. close friends, godparents) are incorporated into the genogram as well as the nature of the relationships between them. The patient's sense of these people's attitudes towards him, their knowledge about his current difficulties, and what they might think caused it and could help it, may shed light on the patient's own attitudes and his broader social identity. A specific note regarding the availability of support from family and beyond, and its quality, is part of the inquiry.
An annotated genogram of the patient, William Smith. An annotated genogram of the patient, Jill Rose.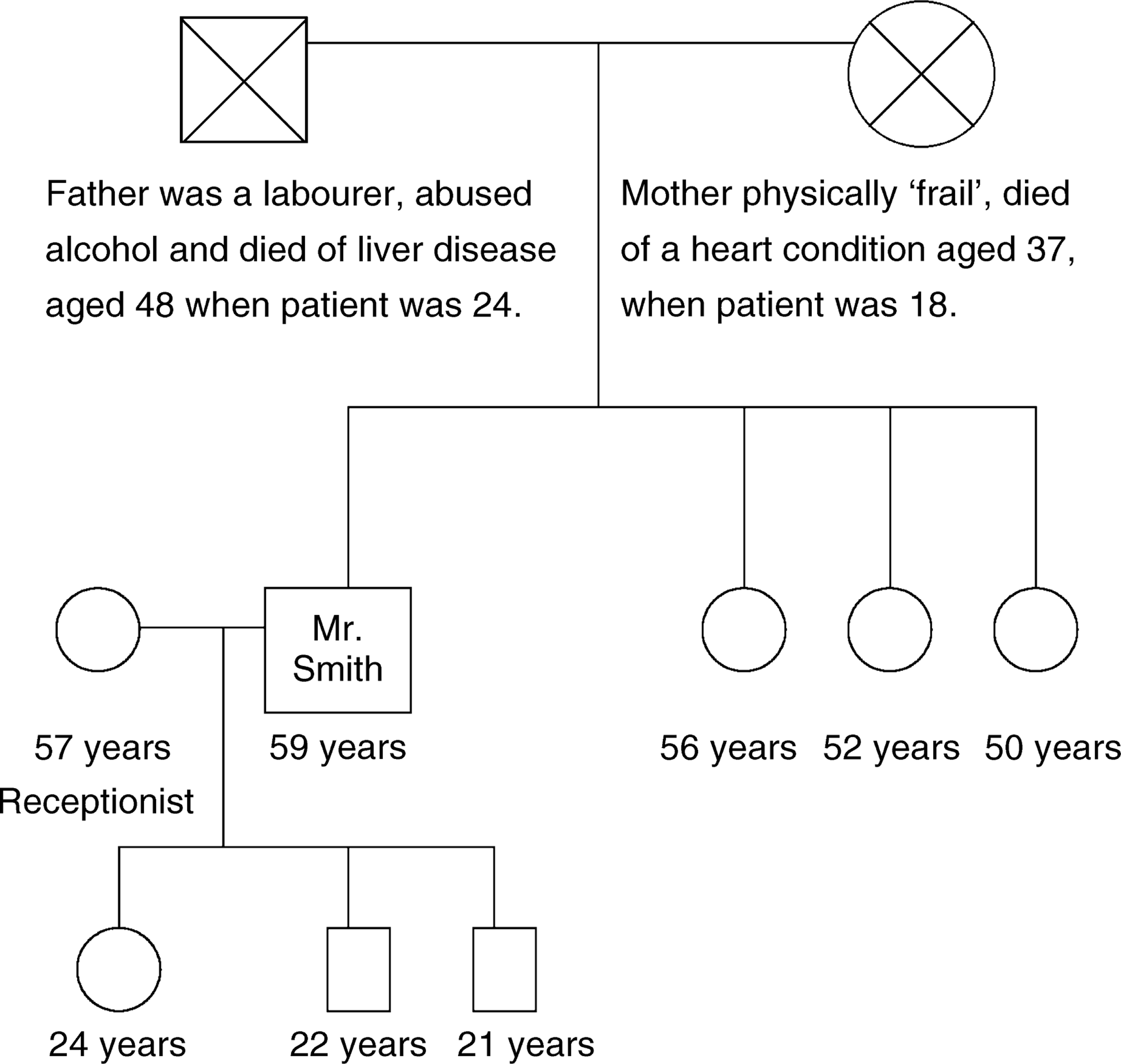
How do we understand these findings?
The task here is to make sense of the clinical findings covered in the preceding sections. This question is conveniently dealt with by applying a biopsychosocial approach, that is generally used by psychiatrists in their clinical work. This entails consideration of any predisposing biological factors, particularly family history of psychiatric disorder and any disease process and/or medical treatments that might be affecting the current picture. The psychological domain covers a wide canvas, including developmental trauma, premorbid personality (e.g. dependent, obsessional, avoidant), early family environment and adverse life events. The socio-cultural dimension is similarly broad, involving aspects like education, poverty, racism, sexism, migration, divorce, homelessness, quality of support, cultural identity and values.
More proximate contributions in these three domains are also highlighted. Poor seizure control in complex partial epilepsy or increased dose of steroids are biological examples. Responses to illness exemplify the psychological with somatization, abnormal illness behaviour and the sick role being particularly relevant. Illustrations of recent social factors are refugee status and marital separation.
Psychiatric diagnosis often informs less than the attempt to make sense of the clinical picture. When clear-cut (e.g. bipolar disorder, chronic schizophrenia, delirium, Alzheimer's disease, somatoform disorder) the diagnosis is explicitly documented (identifying if a specific classificatory schema is applied, e.g. DSM-IV). A differential diagnosis is offered when the case is more ambiguous.
What do we recommend regarding management?
Recommendations for treatment should be congruent with, and informed by, the preceding sections. Format is crucial inasmuch as the referrer needs to have the points explicitly and clearly presented. A statement about the nature and degree of any risk of harm to self and/ or other, and how to address this, is necessarily the first issue to highlight. A need for involuntary status and implications for treatment of a medical illness are stipulated. The need to mount further enquiries (e.g. collaborative history from the GP, family member or night nursing staff) or to conduct special tests (e.g. neuropsychological, neuroimaging) are clearly specified alongside any role the CLP team might play in this. Treatment recommendations may cover psychotropic and other medications, and psychological interventions such as crisis counselling, couple therapy, brief dynamic therapy and family therapy. Systemic approaches may incorporate one or more staff meetings to promote understanding of their interactions with the patient (e.g. hostile countertransferance to a regressed patient) and, if appropriate, the family.
What further clinical developments have ensued?
These section permits documentation of clinical developments which have taken place during the patient's admission. Examples are: response to an intervention; change in the medical condition; acquisition of new data which sheds light on the original assessment; possible factors to account for any deterioration in the mental state; review of treatments such as medications and/or the need for a dedicated psychiatric nurse.
What do we recommend regarding psychosocial follow up?
Discharge recommendations and psychiatric follow up need to be recorded precisely to accomplish continuity of care and to prevent a patient slipping out of the service loop. A vague suggestion that ‘the patient would benefit from supportive therapy and monitoring of medication’ amplifies the risk of a dislocated follow up.
Illustrating our schema
We now illustrate the use the schema with two typical but different patients.
First example
Who is the patient?
Name of the patient: William Smith
Name of referrer: Dr John Stevens, Coronary Care Unit
Date referred: 7/2/00; Date first seen: 8/2/00
CLP Registrar: Dr Mark Slaven; Consultant: Dr Stephen Brown
William Smith, a 59-year-old separated truck driver receiving sickness benefits, lives with his two sons in a regional town. He is currently being treated in the Coronary Care Unit for unstable angina, and is scheduled to have an angioplasty within a few days.
Why you referred the patient to us at this particular time?
Mr Smith is tearful and expresses a wish to die or to put it in his own words: ‘It's too much – I can't go on’. You have asked us to assess his mental state as an urgent matter prior to the angioplasty.
What did we find?
Mr Smith gives a 10-year history of multiple medical problems, including poorly controlled angina, renal colic and a work-related foot injury. He also has a history of alcohol abuse but has abstained for the past 5 years. He has not been examined by a psychiatrist even though he describes having felt ‘down more days than not’ over the past decade.
The most recent episode of lowered mood began 6 months ago when his angina and renal colic worsened markedly. Following angiography he was advised that he did not require cardiac surgery, but would need to lose weight and give up the only activities that gave him pleasure – chopping wood and gardening. The renal colic, occurring daily, was not controlled by a maximal dose of oral analgesic and non-steroidal medications. Over the last three months he had sought Pethidine injections daily from various GPs as well as the local hospital, before being referred to St Vincent's Hospital for lithotripsy. During the flight to Melbourne, he had chest pain and became convinced he was about to die.
He now feels furious towards the doctor who advised him that he did not require surgery. He had wished he was dead the previous day but now felt encouraged, since ‘something is to be done’. An inquiry about depressive, anxiety and psychotic features proved negative. In particular, no disturbance of sleep or other biological functions was elicited.
On mental state examination he was an obviously distressed man, expressing intermittent anguish from his right loin pain. His affect, however, was only mildly lowered. He spoke angrily about being let down by various people – doctors, his wife, sisters and sons. His life would be worth living if he could be free of pain. His attention was diminished when in pain but there was no other evidence of cognitive dysfunction. He did not see himself as ‘emotionally ill’: ‘Everything would be okay’ if his physical problems were ‘properly treated’.
– Current family functioning: uncommunicative, infrequent contact between Mr Smith and siblings (Fig. 1).
– Psychiatric family history: Mother chronically anxious. Father alcohol dependent.
– Support: ‘None’. Sons live with him but provide ‘limited’ support (e.g. drive him to hospital). Daughter lives at a distance and is not close to him, following a longstanding feud over her ‘lifestyle’. No close friendships.
How do we understand these findings?
Mr Smith has a history of vulnerability both genetic and environmental in its source. In addition to his father's alcohol abuse and mother's chronic anxiety, he describes both physical abuse and emotional neglect by the father, and a mother wholly impotent to intervene. He developed a view of himself as undeserving – ‘I need to suffer so that others are spared’. Nonetheless he harboured intense resentment. He lost his main support when his marriage broke up 10 years ago, probably due to his excessive dependency. He has coped emotionally since by remaining physically active but less adaptively by relying on alcohol and seeking frequent support from doctors for physical complaints. Uncoordinated drug management for pain appears to have reinforced Mr Smith's difficulties in asking for help appropriately as well as contributing to his vulnerability to depression.
In diagnostic terms (DSM-IV) we could apply the categories of dysthmia opiate dependence with physiological dependence and chronic pain disorder associated with psychological factors and medical conditions (angina and renal colic).
What do we recommend regarding management?
Mr Smith's expression of wanting to be dead reflects intense frustration rather than morbid suicidal intent.
His tendency to keep emotional difficulties to himself may interfere with pain management; staff need to inquire specifically about the pain.
The CCU should liaise with the urologists and GP to clarify the approach to relieving the renal colic, particularly if the planned lithotripsy is to be postponed.
Antidepressants are not recommended since the disturbed mood is only slight.
CLP team to monitor clinical course and response to treatment.
What further clinical developments have ensued?
8/2/00: Mr Smith appears less hostile although he is anxious about the angioplasty tomorrow. The way the nurses have asked him about the pain has reassured him that they believe it is real. This has made it easier for him to take the analgesia they offer. Discussion with CCU nurses about teaching Mr Smith relaxation exercises to modulate his secondary anxiety.
9/2/00: Mr Smith felt pleased the angioplasty had gone well, but he continues to be bothered by abdominal pain.
11/2/00: Mr Smith is angry that the urologists have reviewed his Xrays and concluded that lithotripsy is not indicated. They recommend a review by his local urologist. He has difficulty coping with their uncertainty about the cause of the pain. ‘I can't keep fighting. All I want is the pain to go’. He is receiving Proladone suppositories and Panadeine Forte. We suggest a review by the Drug and Alcohol Consultant with a view to starting long-acting oral narcotics.
What do we recommend regarding psychosocial follow up?
Coordinated pain management between GP, local hospital and urologist.
Discussion with GP indicated a local pain program with an emphasis on building coping strategies and mutual support of sufferers.
GP to work with Mr Smith on building interests within the limits caused by the pain. We have discussed the usefulness of a joint meeting with him and his sons.
Second Example
Who is the patient?
Name of Patient: Jill Rose
Name of referrer: Dr Mark Rogers, General Medical Unit A
Date referred: 22/8/00; Date first seen: 23/8/00
CL Registrar: Dr Charles Andrews; Consultant: Dr Stephen Brown
Jill Rose is a 68-year-old widow, mother of two children, who lives alone in her own house and receives an aged pension. She has a past history of a postnatal depressive episode (aged 25), a congenital foot deformity, atrial fibrillation and hypertension. She was admitted to the Medical Unit after taking an overdose of Imipramine. The genogram for this patient is shown in Fig. 2.
Why you referred the patient to us at this particular time?
You have requested psychiatric evaluation and advice regarding appropriate treatment and follow up.
What did we find?
Mrs Rose describes having lost her will to live since her husband's death from chronic liver disease 18 months ago. Over the last three months her feelings of sadness have increased substantially, so much so that she has cried incessantly. Although she had longed for death continuously since becoming bereaved she began to consider suicide more recently. She has spent most days confined to a chair waiting for the time to pass; she has stopped attending her church social group. She has lost her appetite, and has difficulty sleeping, often waking around 2.30 am. Her daughter-in-law has reported that Mrs Rose has become ‘wrapped up’ in herself and stopped their regular telephone conversations. Three days ago, on the anniversary of Mr Rose's birthday, she took 25 Imipramine tablets in the hope of dying. She had been on 50 mg nocte for the last year (prescribed by the GP), and on Perindopril for hypertension. Her daughter-in-law found her unexpectedly, noted she was drowsy, and summoned an ambulance. In the Emergency Care Centre she was given charcoal, and her cardiac state was monitored for 12 h.
On examination, Mrs Rose was a woman looking much older than her age. She was dressed in a nightie, sat next to her bed and exhibited obvious psychomotor retardation. Her soft speech showed little spontaneity. Her mood was lowered and she cried several times during the interview, especially when reminiscing about her husband. She did however, show intermittent reactivity. She wished she had succeeded in her suicidal act but also felt ashamed about trying to take her life. She has no plans to try again. No delusions or hallucinations were found. She was unsure about what could help her, but expressed interest in getting help. She was able to reflect that she felt a little better after talking. Cognitively, she was orientated, but exhibited diminished attention and delayed recall on verbal memory testing.
Who are the patient's family and other supports?
– Current family functioning. Son and daughter-in-law support the patient but are frustrated at her ambivalence about seeking professional help.
– Psychiatric family history: Mother suffered from depression in midlife, latter history of strokes and Vascular dementia.
– Supports: Close friends through church from whom she has withdrawn.
How do we understand these findings?
Mrs Rose presents a complicated grief reaction that now manifests as clinical depression with prominent psychomotor features. She is predisposed to this in that she has had previous episodes and her mother suffered similarly. Throughout her childhood she was labelled by her father as ‘flawed’ by virtue of a foot deformity which resulted in a marked limp as a child. He was ashamed of her. Her sense of being unwanted was compounded by being teased at school and by her mother leaving the family when Mrs Rose was 15. An unplanned pregnancy (which she subsequently lost), led to her getting married at 18. Although her husband, like her father, was dominating and bullied her, she was fiercely loyal despite her son's advice to act more assertively. Her husband died unexpectedly after admission to hospital for treatment of gallstones. She still feels guilty for encouraging him to have the treatment and not being with him at the time of his death. Adjustment to assuming responsibility for decision-making has been difficult. She has always had few friends and has isolated herself from them since her husband's death.
What do we recommend regarding management?
Mrs Rose is not currently suicidal and appreciates the need for professional help. Nevertheless, her abiding sense of feeling unworthy makes her a suicidal risk in the medium term. Although her son and daughter-in-law are supportive, they are unable to live with her. We will contact the local psychogeriatric team and recommend their involvement while she is in a psychiatric inpatient setting and plan subsequent community follow-up.
Her psychomotor retardation needs monitoring specifically with regard to drinking and eating and mobilizing sufficiently.
Reintroduction of Imipramine is not recommended given the overdose and past history of atrial fibrillation. A selective serotonin reuptake inhibitor (SSRI) is recommended instead (e.g. Sertraline 50 mg mane). In addition, an opportunity to discuss and explore the loss of her husband, that is, grief therapy is indicated.
We will review later today.
What further clinical developments have ensued?
Despite continued retardation, the patient has eaten and drunk adequately with nursing encouragement.
What do we recommend regarding psychosocial follow up?
The psychogeriatric team has arranged a bed for her and transfer is possible tomorrow. I have discussed this with Mrs Rose. While initially distressed, she later was relieved and accepted the plan. I have informed the family who were very pleased at the prospect of Mrs Rose receiving further help and support.
Feedback from the GP indicates only patchy knowledge about Mrs Rose. He appreciated information about the potential lethality of tricyclic antidepressants in overdose, the recommended therapeutic doses, and the need to review their efficacy.
Discussion
We have sought to map out a comprehensive CLP schema while acknowledging that different aspects need highlighting for different patients and clinical situations. However, the six core functions of the report govern its overall format and the potential content of each of its eight sections. Our approach also embodies a set of issues that ideally require attention in every case, ensuring that no relevant matters are neglected.
In addition we have suggested how to incorporate cogent aspects of a conventional psychiatric history into a CLP report. We need to recognize that the format applied in a normal psychiatric setting is not appropriate in a CLP one. Flagging the eight sections in ‘user friendly’ terms is part of this exercise, namely presenting a document to non-psychiatric colleagues but not at the expense of what the CL psychiatrist intends to convey. The relevance of customary categories of the psychiatric written record like ‘Developmental and personal history’ and ‘Formulation’ may be less obvious to referrers compared to more familiar constructs like ‘Diagnosis’. Placing this information into the section ‘How do we understand these findings?’ makes its relevance much clearer. The same argument relates to ‘Past History’ which we incorporate into the section ‘What did we find?’.
Guthrie and Reed [17] have considered the question of what to cover in a CL report but adopt the procedure of adding a series of questions to the conventional psychiatric history. They suggest, for example, that pertinent subjects like ‘evidence of abnormal illness behaviour’ and ‘physical disease and the patient's reaction to it’ constitute additional material. We regard this strategy of an ‘addendum’ as less effective for communication since it is presented in an unintegrated fashion. As Small and Fawzy [15] and Berlin and Sluzki [16] have stressed, the family context of the patient is often underemphasized in the CLP report even though it may have a profound bearing on course and outcome. We certainly agree. Hence, the distinct section we give to it and, in particular, incorporation of a detailed genogram. Indeed, we see the ‘tree’ as a sine qua-non-of a helpful CLP report.
Apart from the advantage of conveying directly how we make sense of patients and their clinical features, with explicit recommendations for treatment, familiarity with this approach and dimensions under each of the eight questions is bound to have a continuing educative impact. Trainees would be more able to appreciate how their CLP consultant-teachers obtain and distil relevant data, while medical, nursing and allied health colleagues would be effectively exposed to the psychiatric approach to their medical patients.
Our recommended format also satisfies archival and medico-legal requirements, desired features of all medical records. Entries need to take into account appropriate legislation (e.g. guardianship and mental health) and specify explicitly which staff members assume various responsibilities. The related ethical question of respect for confidentiality remains a thorny one given the need to record clinical material that elucidates the nature of the case but which is often intensely personal. This dilemma however, applies to all hospital records with a balance struck between what treating staff need to know in order to be helpful and inserting private details which are not apposite at the time of consultation. This quandary is clearly of significance but outside our brief.
Now we turn to the CLP form itself. In Table 1, we presented the eight sections and their prompts to ensure coverage of the initial assessment and a section for subsequent entries. The prompts may be superfluous for the seasoned assessor but help to remind the novice of the type of inquiry to pursue under each question. This is advantageous in the setting of frequent changes of psychiatric and medical staff.
We proposed the ‘stand-alone’ format (which as illustrated would usually comprise 3–4 pages) since it facilitates easier identification, particularly in the bulky file of a complex case. This format will also allow for copies to be easily forwarded to participants in follow-up care (e.g. GP, private psychiatrist or community mental health clinic). It is anticipated the record will be mostly hand written although the template could be easily placed on computer networks to allow individuals to type directly if this was quicker.
Little is empirically known about what features of the written consultation are associated with clinical effectiveness. Seward et al. [21] postulated that their observed high concordance rate between psychotropic recommendations in the CLP written report and consultees prescribing, may have related to the specificity of the recommendations, a feature which we have emphasized. It is known that different consultees value different aspects of a CLP service in general [7] and the information within a CLP report may be used differently depending if the author is a trainee versus a psychiatrist [21]. Standardization of the CL record as proposed will facilitate auditing, quality assurance and further research. An important question is whether this schema would lead to more effective outcomes – a report that is more readable, understandable and linked to recommendations that are acted upon. Therefore, we propose that if it finds favour it should be evaluated. Qualitative enquiry could explore the consultees opinion's of the schema, while other measures might be concordance rates with recommendations. A trial of the schema would need to be heralded by an introduction and rationale to our referring colleagues, for its use.
Conclusion
The written report is fundamental to the CLP consultation. While it should always be tailored to the specific clinical situation, using a consistent set of pertinent categories is advantageous. These categories are derived ideally from the intrinsic functions of the CLP report. We have proposed a readily comprehensible series of questions that aim to illuminate what the CLP assessor is trying to achieve, so offering colleagues a ‘user-friendly’ way to make sense of the patient's story and to recommend treatment.
Footnotes
Acknowledgements
We thank Joel Aizentros, David Clarke, Jeremy Couper, Edwin Harari, Beate Harrison, David Kissane, Mike Salzberg, Julie Sharrock, Graeme Smith, Jeremy Stone and Robert Yewers for their helpful contributions.