
Abstract
Keywords
Irritable bowel syndrome (IBS) is the major cause of referrals to gastroenterology clinics in the western world and often leads to high health-care use and much time missed from work [1–3]. Psychiatric disorders occur in 50–60% of these clinic patients and contribute to impaired health-related quality of life and increased medical help-seeking [4–6]. The other important predictors of a poor outcome are chronic social stress, often involving interpersonal difficulties [7], [8], a history of childhood abuse and poor coping [9]. For these reasons, we developed psychodynamic interpersonal therapy for patients with severe, refractory IBS [10]. We have shown that, when delivered by a single therapist, this treatment was more effective than placebo-control in reducing abdominal pain, depression and impaired daily function [11].
Recently, two systematic reviews have shown the benefits of antidepressants in IBS, especially tricylic antidepressants [12], [13]. One review included nine studies of IBS and found that symptom improvement, notably abdominal pain, was nearly four times greater with antidepressant than with placebo [13]. It was not clear from these studies, however, whether symptom improvement was related to improved depression and the authors suggested that this should be an aim of future research [13]. The other review, which included 13 studies of IBS, also found marked symptomatic improvement compared to placebo, but in most studies this did not correlate with depression response [12]. In a systematic review of cognitive–behavioural therapy for a wide range of medically unexplained syndromes, physical symptoms appeared to be the most responsive to treatment and this appeared to be independent of improvement in psychological distress [14].
It is not clear, therefore, which mechanism or mechanisms are involved when psychodynamic or cognitive– behavioural psychotherapy or antidepressants lead to improvement in people with medically unexplained (or ‘functional’) syndromes, such as IBS. There are several possibilities. First, the treatment, whether psychotherapeutic or pharmacological, may be effective in improving depression and this leads to symptomatic improvement. Second, the antidepressants might have a direct analgesic effect on the abdominal pain [15–17] or have an effect on the same neurotransmitter system but this effect would be absent in those treated with psychotherapy. Third, the psychotherapymight help the person cope with their symptoms better than previously: ‘the pain is still there but I'm managing it better’ [18]. The mechanism(s) involved in improved coping are not clear but may be related to a history of childhood abuse and lack of a confidant in adult life as these are associated with a poor outcome and frequent medical consultations among people with functional gastrointestinal disorders [19], [20]. At least some of this association between a history of abuse and poor outcome cannot be explained by psychological distress and might be concerned with a changed perception of pain [21], [22] as it appears to be mediated by the number of reported bodily symptoms.
In our most recent trial, we have shown that treatment with both psychodynamic, interpersonal therapy and a selective serotonin re-uptake inhibitor (SSRI) antidepressant (paroxetine) led to improved health-related quality of life in patients with severe IBS compared to usual treatment [23]. In this paper, we examine whether the beneficial effect of our experimental treatments can be explained by improvement in psychological distress and/or is confined to the patients who had psychiatric disorders. We have examined the data in several ways. First, we assessed whether the improvement in health-related quality of life observed in the main trial was correlated with improvement in psychological symptoms. Second, we tested whether this overall improvement in healthrelated quality of life was found only in patients with psychiatric disorder. Third, we reassessed the relationship between improvements in health-related quality of life and psychological symptoms in participants with and without psychiatric disorder.
We tested the first hypothesis that, after controlling for confounders, improvement in Short Form-36 (SF36) physical component summary score (between baseline and 15 months later) would be correlated with improvement in: (i) Hamilton Depression Rating Scale (HRDS) score; and (ii) Symptom Cheecklist-90 (SCL-90) subscale scores for anxiety, somatization and global severity. Second, we tested the hypothesis that the observed improvement in the SF36 physical component summary score in the groups treated with psychotherapy or paroxetine (SSRI antidepressant) would be found only in patients with psychiatric disorder at baseline. Third, we tested the first hypothesis in the patients with and without psychiatric disorder at baseline. This report only concerns data collected at baseline and at 15 months (12months after treatment ended) as the difference between the groups in SF36 physical component score were significant over this time course. Finally, in a multiple regression analysis, we assessed whether the improvement in SF36 physical component score could be explained fully in terms of changes in depression, anxiety, somatization and pain scores, after which the addition of a history of abuse and the individual treatments (psychotherapy and antidepressant) would not increase the variance explained.
Method
The sample was recruited from patients attending seven gastroenterology clinics in the UK. Patients were invited to enter a trial, which involved random allocation to eight sessions of individual psychotherapy, or 3months treatment with 20 mg daily of the SSRI antidepressant, paroxetine or routine care by gastroenterologist and general practitioner [23]. Assessments quoted in this paper were those made at baseline (entry to the trial) and 12months after the end of the 3-month treatment period (i.e. 15months after baseline). Full details of the trial are reported elsewhere [23].
All clinic patients who fulfilled Rome I criteria for IBS [18], with severe abdominal pain (60 or more on a 0–100 visual analogue scale) and whose symptoms had not responded to ‘usual’ medical treatment were invited to join the trial. Patients were excluded if they had a psychotic disorder, severe personality disorder, active suicidal ideation or consumed more than 50 units of alcohol per week, but patients with other psychiatric disorders were included [23].
The psychotherapywas psychodynamic interpersonal therapy similar to that described in our previous trial [11]. Patients received one long (approximately 2 h) and seven shorter (45min) individual sessions over 3months. They were encouraged to discuss their symptoms in depth; emotional factors were explored, and links between symptoms and emotional factors were identified. Three therapists were trained by a member of the study team (E.G.) using a manual and a videotaped training package; continued conformity by the therapist to the model was ensured by weekly supervision with E.G.
The SSRI treatment comprised paroxetine 20mg orally each day for 3months, prescribed and monitored either by the patient's gastroenterologist or general practitioner. For treatment as usual, patients continued to be seen by either their gastroenterologist and/or general practitioner, usingwhatevermanagementwas deemed appropriate throughout the 15months of the study.
Ethics committee approval was obtained from each hospital taking part in the study and all participants signed written consent after full explanation prior to entering the study. Before randomization, the following assessments were made and they were repeated at 1 year after the end of treatment (15 months later).
Abdominal pain was assessed using a visual analogue scale taken from the McGill Pain Questionnaire [24].
Psychiatric symptoms were recorded by a trained psychiatrist using the Hamilton Rating Scale for Depression [25] and each patient completed the SCL-90 [26]. Psychiatric disorder was recorded only at baseline and was diagnosed (according to ICD10) using the Schedules for Clinical Assessment in Neuropsychiatry (SCAN), administered by a trained psychiatrist [27]. The SCAN produces multiple psychiatric diagnoses and in this report we have included in the psychiatric disorder group patients who had at least one of the following: depressive or panic or generalized anxiety disorder.
Health-related quality of life was measured using the SF36 [28]. This has eight subscales; low scores indicate poor health status. In IBS, the SF36 has been shown to discriminate between different degrees of severity; patients rate the severity of their disorder according to the amount that it disrupts their daily lives rather than symptom severity [29], [30]. In our trial, we found marked improvement occurred in the physical component summary score; this includes the subscales of physical function, role limitation (physical), bodily pain and general health perception [31]. The physical component summary score is included in the present report as the main outcome variable.
Assessment of history of sexual abuse: The Sexual and Physical Abuse Questionnaire [32], [33] was given to patients to complete in the presence of the female psychiatrist performing the assessment. Discussion was not encouraged (as this could have interfered with our trial) but support was provided if necessary. The questionnaire asks whether the respondent has experienced any physical or sexual abuse either as an adult or as a child. In this report, we have included in the multiple regression analysis a variable that uses three categories of reported sexual abuse: (i) none; (ii) forced touching (either some part of the breasts or genitals); or (iii) forced penetration (rape).
Data analysis
All data were entered and analysed on SPSS, V 11.5. In a preliminary analysis, we assessed the sociodemographic characteristics that might be confounders. Following this, we used partial correlation to compare the change in SF36 physical component score and the change in psychological scores between baseline and 15 months follow-up interview. This partial correlation adjusted for age, sex, marital status, years of education (all of these except sex were significantly associated with SF36 physical component summary score at baseline) and treatment group. We also adjusted for baseline values of SF36 physical component and the relevant psychological scores to take account of the fact that higher initial scores have greater scope for large change scores. The psychological scores were Hamilton Depression Rating Scale (HDRS), SCL-90 global severity score, anxiety and somatization subscale scores. We used these as they included unique measures relevant to the psychiatric disorders we included as well as global indices of psychological distress.
In order to test our second hypothesis, we split our sample into those with and without a psychiatric disorder, defined as having one or more of depressive, panic or generalized anxiety disorder at baseline. We then repeated our main trial analysis comparing the three treatment arms controlling for baseline scores [23]. Testing our third hypothesis involved repeating the partial correlation analysis used for hypothesis one, in the groups with and without a psychiatric disorder.
Finally, we performed a multiple regression analysis with mean substitution for missing data to identify the variables most closely associated with SF36 physical component score at 15months follow-up. The first analysis included patients in all three treatment groups and the second analysis included only those patients in the treated groups in whom the most marked changes in SF36 physical component score occurred.
The multiple regression analysis included SF36 physical component summary score (15 months score) as the dependent variable. The following were included as independent variables in the first analysis: age, sex, years of education (12 or more), marital status (as two dummy variables), unemployed through ill-health at baseline, baseline SF36 physical component summary score, HDRS Score (baseline and change score), SCL-90 anxiety and somatization scores (baseline and change scores) and treatment group (as two dummy variables for psychotherapy and paroxetine). In a second analysis, we added abdominal pain score (baseline and changes score) and reported history of abuse.
Results
Subjects
Two hundred and fifty-seven patients (81% of eligible patients) were recruited for the study. The 60 patients who declined to enter the study were similar in baseline characteristics to the participants. The IBS was chronic (median duration 8 years) and severe (mean typical pain score was 67.4 out of 100). The disorder led to restricted activities on amean of 12.1 (SD=11.8) days per month prior to baseline assessment. Seventy patients (27.2%) were unemployed through illness and 37 (14.6%) received invalidity benefits.
Demographic data and SF36 and Hamilton depression scores for irritable bowel syndrome (IBS) patients with and without psychiatric disorder (depressive, panic or anxiety disorder) at baseline
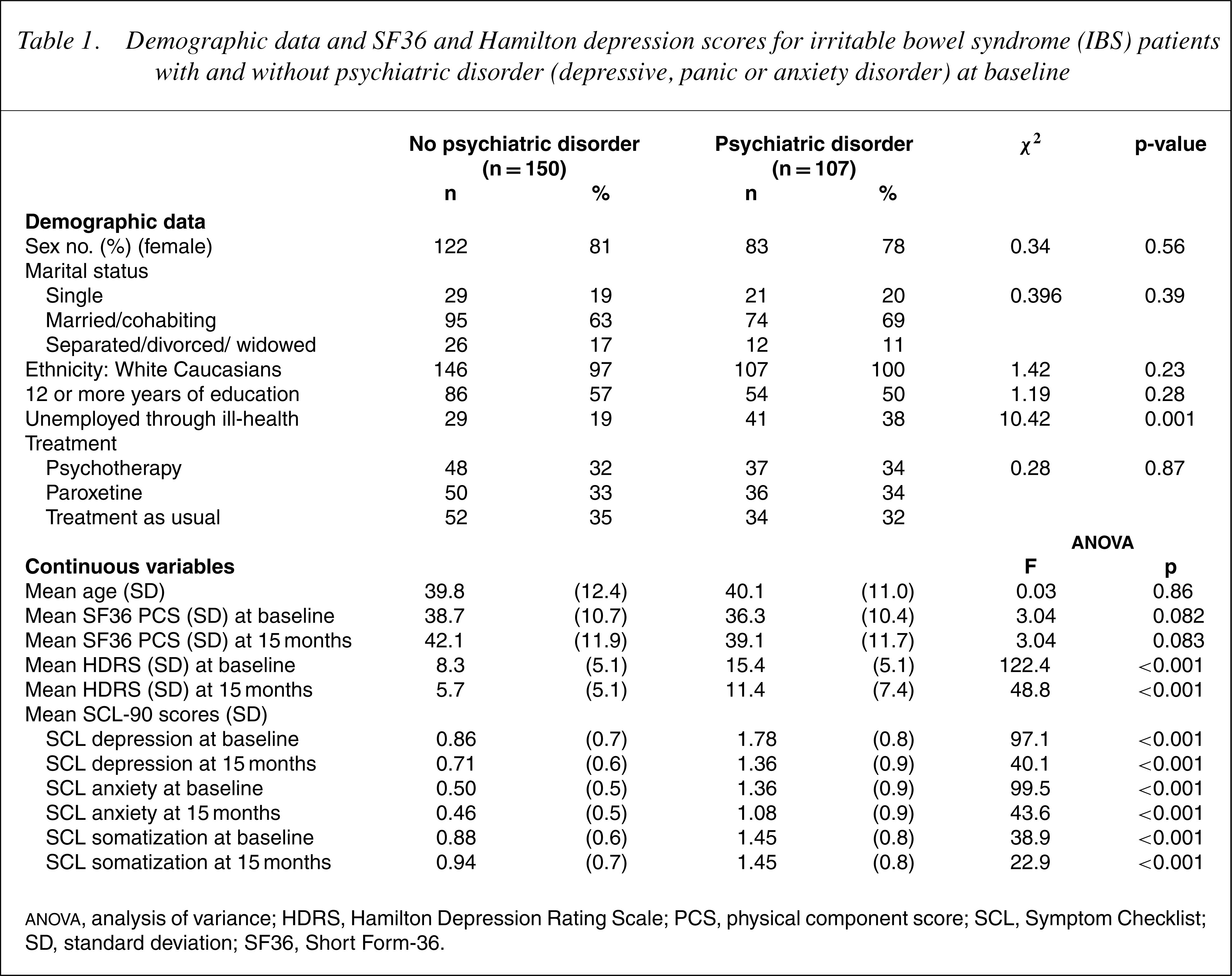
ANOVA, analysis ofvariance; HDRS, Hamilton Depression Rating Scale; PCS, physical component score; SCL, Symptom Checklist; SD, standard deviation; SF36, Short Form-36.
Fifty-nine patients (23%) reported that they had experienced some form of sexual abuse: 31 (12.1%) reported rape and 28 (10.9%) reported unwanted touching of the genitalia.
Hypothesis 1: Is improvement in SF36 score at follow-up correlated with changes in depression, anxiety and distress scores?
Partial correlation coefficients for change in scores (from baseline to 15months) for SF36 physical component and psychological measures – scores adjusted for age, sex, marital status, years of education, baseline scores and treatment
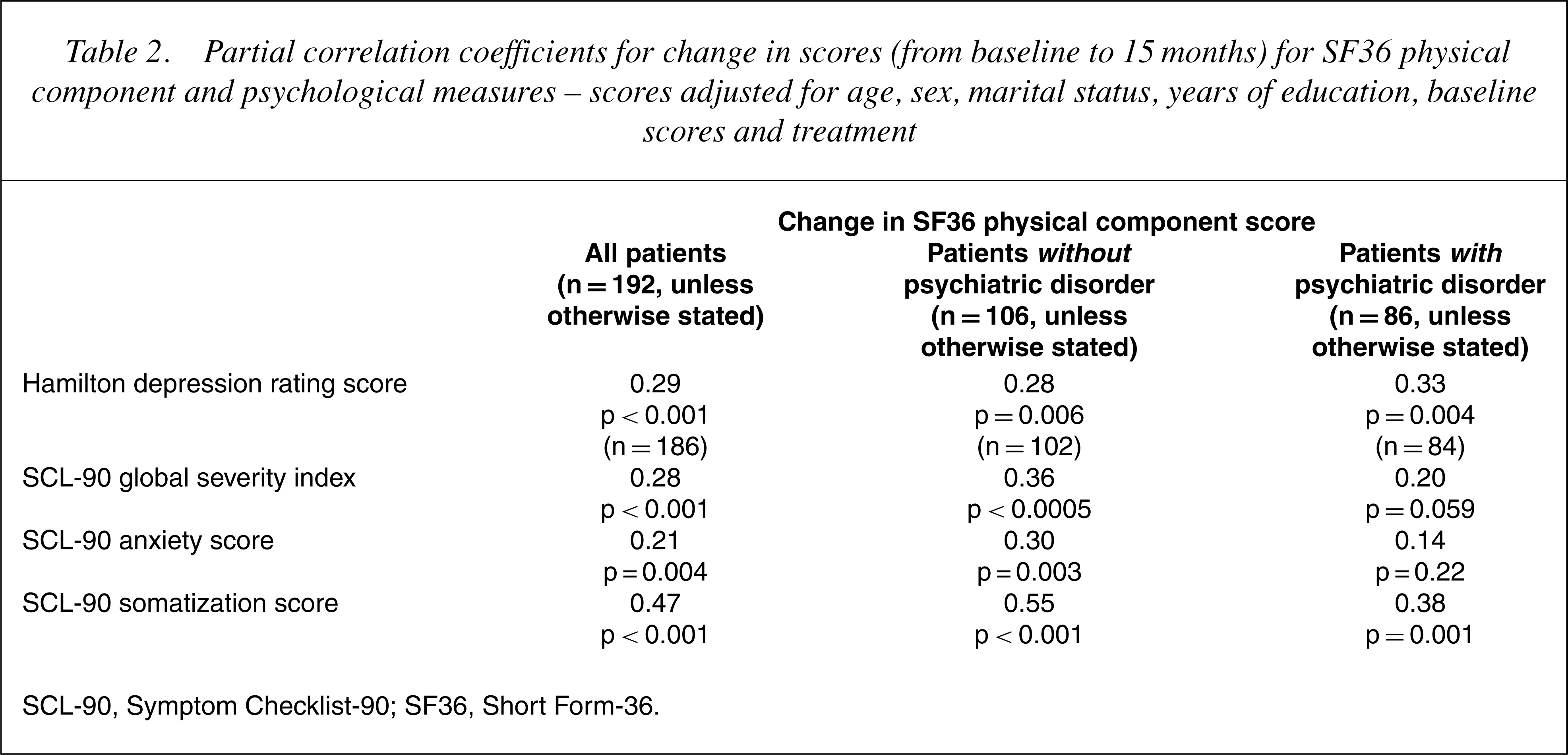
SCL-90, Symptom Checklist-90; SF36, Short Form-36.
Hypothesis 2: Improvements in SF36 physical component score for the treated groups would only be found in patients who had concurrent psychiatric disorder at baseline.
After adjustment for age, sex, years of education, marital status and baseline SF36 physical component score, there was a significant difference between the treatment groups in terms of change in SF36 physical component score for those with concurrent psychiatric disorder at baseline, but only a trend toward difference for those without concurrent psychiatric disorder (Table 3).
Change in SF36 physical component summary scores between baseline and follow-up for the three treatment groups – scores and p-values (ANCOVA) adjusted for age, sex, years of education, marital status and baseline value of SF36 physical component score
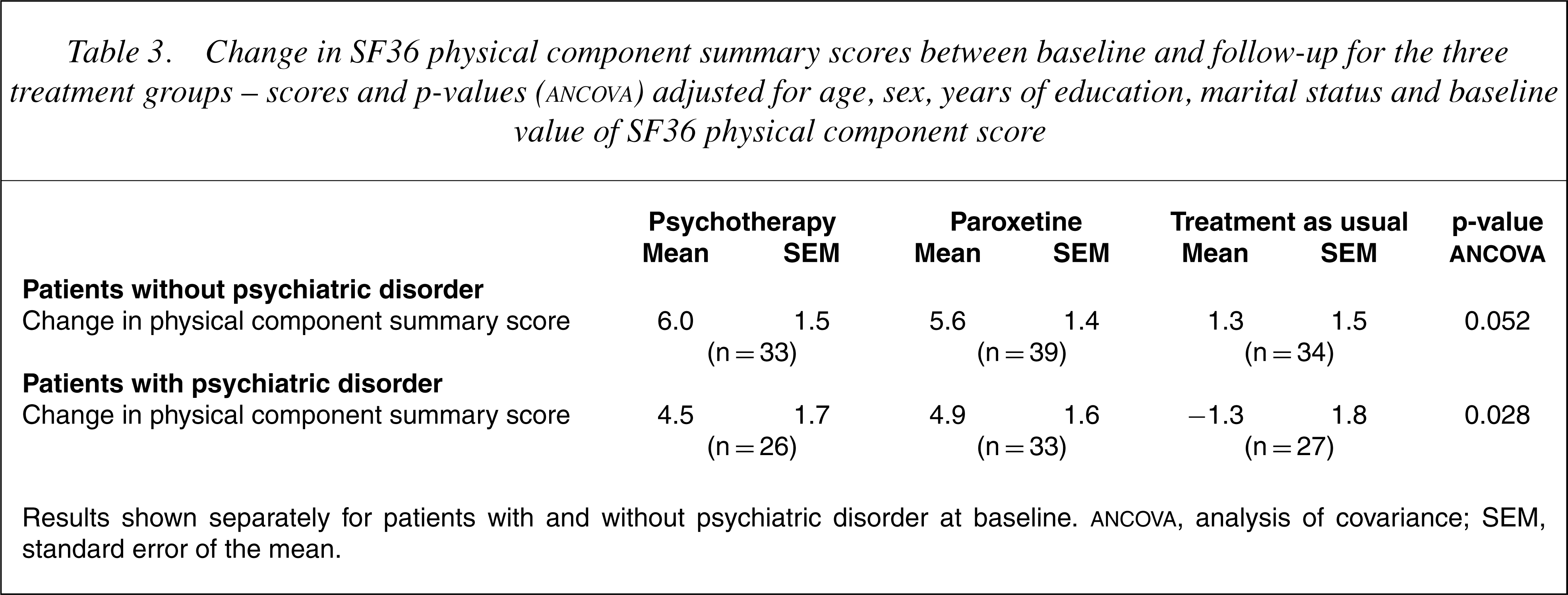
Results shown separately for patients with and without psychiatric disorder at baseline. ANCOVA, analysis of covariance; SEM, standard error of the mean
There was a very similar pattern of correlations between change in SF36 physical component score and changes in psychological scores in patients with and without psychiatric disorder at baseline (Table 2 right hand columns). For SCL-90 scores, the correlation coefficients for anxiety and global severity did not reach significance for patients with psychiatric disorder.
Multiple regression analysis to assess the variables most closely associated with change in SF36 physical component score.
Results of multiple regression analyses (n = 200)
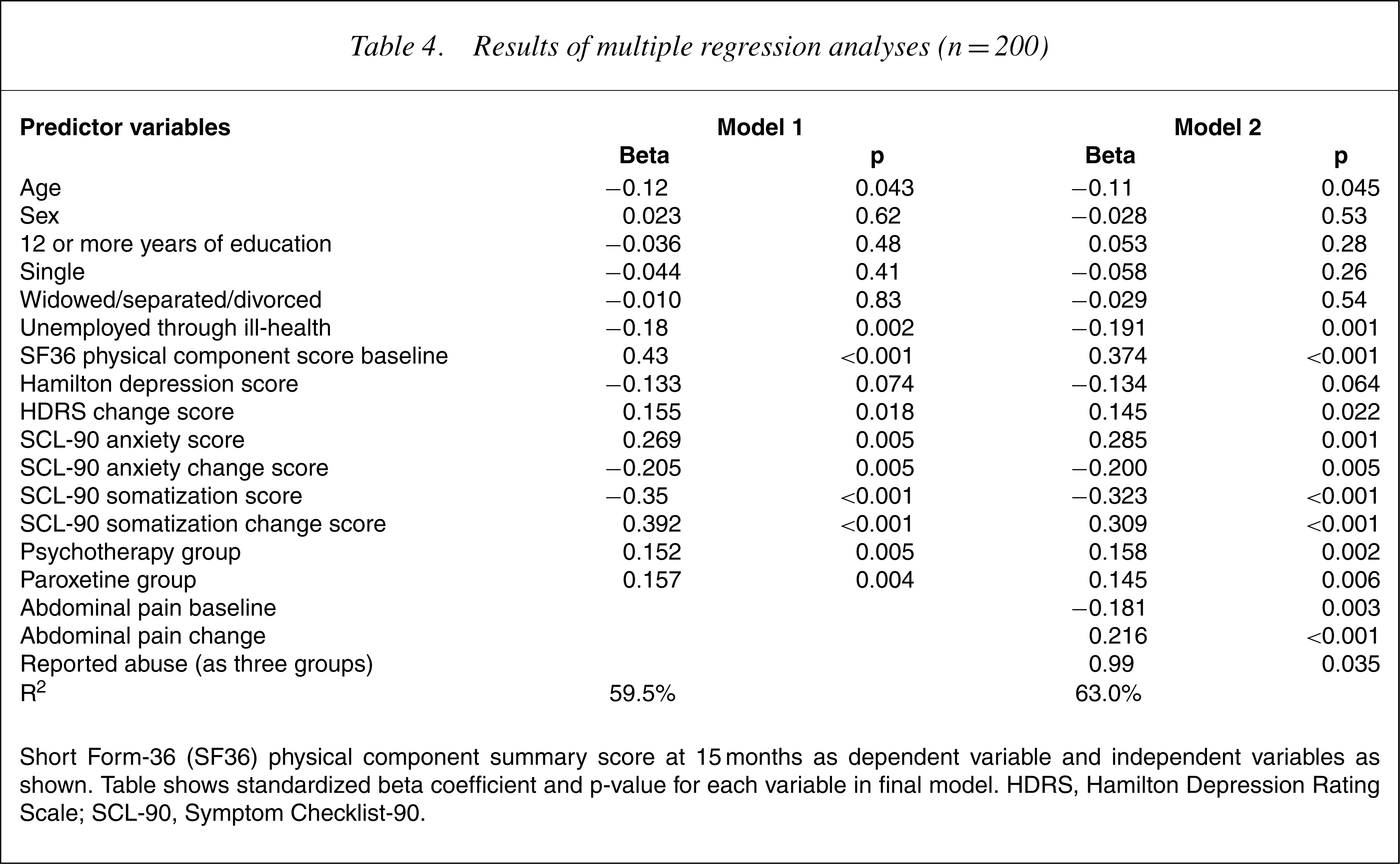
Short Form-36 (SF36) physical component summary score at 15 months as dependent variable and independent variables as shown. Table shows standardized beta coefficient and p-value for each variable in final model. HDRS, Hamilton Depression Rating Scale; SCL-90, Symptom Checklist-90.
Results of multiple regression analyses including only the patients in the psychotherapy and paroxetine groups (n=136)
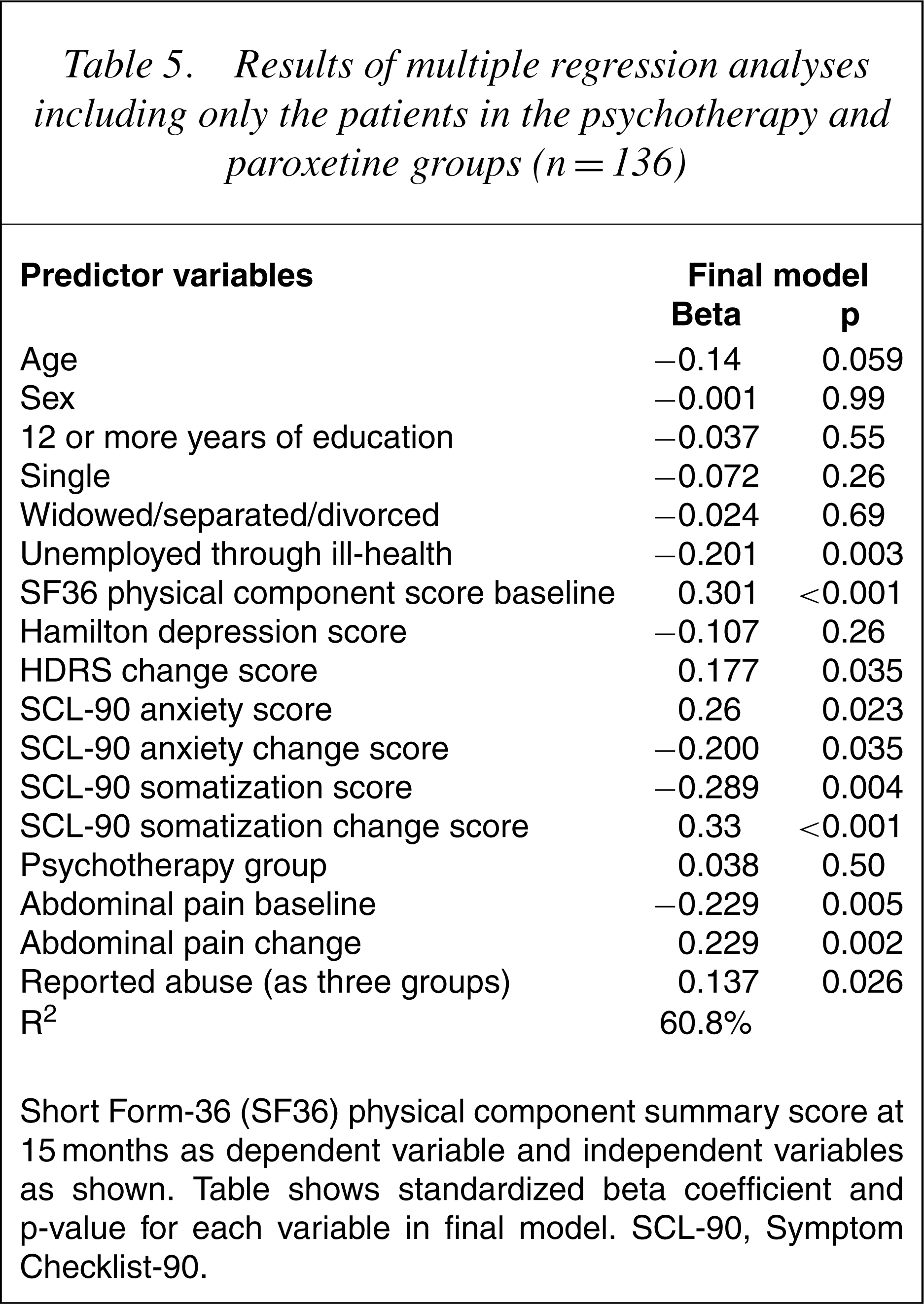
Short Form-36 (SF36) physical component summary score at 15 months as dependent variable and independent variables as shown. Table shows standardized beta coefficient and p-value for each variable in final model. SCL-90, Symptom Checklist-90.
Discussion
In this sample of patients with severe IBS we found, after controlling for the relevant confounders, a moderate but significant correlation between change in SF36 physical component summary score and changes in depression, anxiety and somatization scores. The magnitude of the association was limited, however, and we were able to show in the multiple regression analysis that even when changes in psychological scores, change in pain severity and a history of sexual abuse were included, there was still significant variance associationwith each of the treatments. This indicates that the changes brought about as a result of these treatments were not being mediated solely by changes in psychological parameters or pain severity or those associated with a history of sexual abuse. Furthermore, we could not find evidence that the improvement of the whole group could be explained solely by the improvement occurring in those patients with psychiatric disorder following treatment. We conclude, therefore, that the mechanisms accounting for the improvement in health-related quality of life following psychological treatments in severe IBS cannot be accounted for fully by changes in psychological state.
This is the conclusion reached by the relevant systematic reviews [12–14]. We are really quite ignorant of the precise mechanisms underlying the improvement of patients with medically unexplained symptoms when they are successfully treated with antidepressants or psychotherapeutic means. One review reported the ‘intriguing’ finding that the beneficial effects of cognitive behaviour therapy (CBT) in these patients are independent of psychological distress [14] and went on to suggest that CBT might lead to a decrease in symptom-specific distressing cognitions or dysfunctional behaviours but also suggested that the following might be responsible: improved coping, reduced avoidant behaviour, greater perceived control, reduced catastrophizing and reduced preoccupation and amplification of bodily symptoms.
A decrease in symptom-specific distressing cognitions certainly occurs after hypnotherapy for IBS [34]. In this form of treatment, the therapist makes suggestions directed at increasing the patients' ability to control their gut, so the hypnotherapymight act as a form of ‘cognitive restructuring’. However, because the IBS-related cognitions are closely correlated with symptom severity, the improvement might have resulted from a direct effect of hypnotherapy on symptoms, which, in turn, led to fewer negative thoughts about bowel dysfunction [34].
Similar changes have been reported following cognitive–behavioural therapy for the IBS, when the number of successful coping strategies increased and patients' avoidance behaviour decreased [35]. These cognitive changes were also recorded, however, following routine appointmentswith gastroenterologistswhen there was a reduction in patients' anxiety, fear of cancer and catastrophizing cognitions and, in the longer term, a greater tendency to attribute their symptoms to a busy life rather than serious illness of their intestines or stomach [36], [37]. Furthermore, these positive changes were associated with a reduction of subsequent use of primary health care [38]. They occurred most in patients who saw the same gastroenterologist for all of their appointments, who reported high satisfaction with these appointments and when level of general anxiety was reduced at the last appointment [37]. Because these changes can all occur in the context of routine care as well as following hypnotherapy, we should be cautious about regarding them as specific to CBT – they might be regarded as non-specific benefits that occur with a variety of psychological treatments, including high-quality routine care. Because these studies of both hypnotherapy and CBT in IBS found that improved complaint-related cognitions occurred in the context of improved bowel symptoms and anxiety and depression we cannot infer their independence from reduced psychological distress.
We had no measure of IBS-related cognitions in this study, so we cannot examine this relationship further in our study. We have reported elsewhere, however, that patients with a reported history of sexual abuse did particularly well with psychotherapy [23]. This is probably related to a change in the perception of pain as an abuse history was associated with increased tolerance to gut distension following treatment. This was independent of changes in depression, indicating possibly the importance of a change in cognitions. A demonstration that the pain could be induced by bowel distension (at first testing) might be a powerful way of demonstrating that the pain does not necessarily indicate disease. In addition, people with a reported abuse history might use cognitive styles of self-blame and a self-silencing approach to close relationships, which are independent of depression [39]; such a cognitive style would be modified by successful psychotherapy.
Studies in back pain have indicated that changes in catatrophizing cognitions, reduction of fear-avoidance beliefs and increased perception of control over pain can occur in association with reduced disability but without change in pain intensity [40], [41]. Reduction in fear-avoidance beliefs is thought to be associated with reduced hypervigilance toward bodily sensations [42], [43]. In our study, we found that somatization score had the strongest correlation with improved disability. Interestingly, the authors of one of the back pain studies suggested that the full explanation of the rationale behind CBT, specifically exposure in vivo, may have led to a change in the patients' cognitions [40]. It is very likely therefore that there are a number of cognitive changes that take place simply as a result of a full and acceptable explanation regarding the cause of the symptoms.
Some patients may respond more favourably than others to receiving such an explanation; we did find that patients with psychiatric disorder, who received treatment as usual, tended to get slightly worse (Table 3 bottom line). This finding is entirely explained by depressive disorder as panic and generalized anxiety disorders were associated with a slight improvement in outcome like the patients without psychiatric disorder (data not shown). There are a number of limitations of this paper, which need to be recognized. The paper includes secondary analyses of data collected in a trial, which was not designed specifically for this purpose; this was a pragmatic trial designed to assess cost-effectiveness, not an explanatory trial. The results may only be pertinent to patients with severe IBS and may not be generalizable to a wider group of patients with medically unexplained symptoms. There was an inadequate improvement in depression (only four points on HDRS – Table 1) in patients who had psychiatric disorder.
However, this paper does overcome some of the limitations of previous studies as it includes detailed measures of change in psychological symptoms as well as pain and health-related quality of life; it included psychological treatment as well as antidepressants and it includes data concerning an SSRI antidepressant which have been lacking in most previous reports. We conclude that much more work needs to be done to understand why psychological treatments help patients with medically unexplained symptoms. We have shown that improvement in health-related quality of life is related to reduction of psychological distress but this might be a minor part of the reason for the overall improvement. It is possible that there are a number of non-specific ingredients in these therapies, which include cognitive changes possibly brought about by clear explanation, and which could be introduced fairly readily into routine clinical practice. There may be other experiences which are important – temporarily feeling better as the results of antidepressants, being able to go some distance from a toilet without disastrous consequences (at the explicit instruction of a therapist) or clearly linking exacerbation of symptoms to stress (perhaps as a result of keeping a diary) might all play a large part in positive cognitive change and lead to reduced fear-avoidance behaviour with subsequent increased daily functioning.
The main clinical implication of this study is that patients with severe IBS, which has not responded to usual treatment, may benefit from psychological treatment. Such psychological treatment needs to be available for such patients, whom are quite numerous in gastroenterology clinics, and for whom little specific treatment is available. Currently, most patients do not reach liaison psychiatry services but there is an argument for such services being proactive in relation to this group of patients. How exactly the treatment works must be subject of future research but improvement in anxiety and depression is worthwhile in itself as well as contributing to improved health-related quality of life.
Footnotes
Acknowledgements
The study was supported by Medical Research Council (MRC), UK and North West Regional Health Authority Research and Development Directorate. The research team thank the following: the MRC for financing the study, the Health Authorities for financing the psychotherapists, the patients who consented to take part in the trial and the doctors who prescribed the antidepressant medication.