
Abstract
Irritable bowel syndrome (IBS) is a chronic, prevalent disorder for which there is a lack of effective treatment [1]. It results in considerable disability and increased health care utilisation among a subset of sufferers. It has been estimated that symptoms attributed to IBS may affect up to 15%% of the population [2],[3] and that 39%% of patients with IBS take over-the-counter medications [3],[4]. Despite the socio-economic implications of IBS, little is known about its aetiology or pathophysiology and, as a consequence, medical management of the disorder remains unsatisfactory [5].
Irritable bowel syndrome is characterised by a chronically abnormal bowel habit in the absence of demonstrable pathology. To standardise the diagnosis of IBS, symptom-based criteria have been developed which are referred to as the Rome criteria [6]. For IBS symptoms to meet these criteria, there must be at least 3 months of continuous or recurrent abdominal pain or discomfort that is either relieved by defecation and/or is associated with a change in the frequency or consistency of the stools. In addition, there must be at least two of: a change in bowel habit, stool form or stool passage (straining, urgency or a feeling of incomplete evacuation); passage of mucus or feelings of bloating or abdominal distension.
While there is some evidence to suggest that altered gut motility and changes in the sensation of the colon or small bowel occur in IBS [7–9], no distinct structural changes have been identified, suggesting that IBS may, in part, be functional in nature. Such a view is supported by the association between IBS and psychosocial variables, such as stress [1],[10],[11]. Further, persons suffering from IBS have high rates of comorbidity especially with anxiety and depression, particularly among those who present for treatment [12],[13].
There is, however, some difficulty in interpreting the implications of the comorbidity between IBS and psychiatric disorders such as anxiety and depression. For example, although anxiety, via the autonomic nervous system, has effects on the gastrointestinal system and may, therefore, exacerbate pain, it is also reasonable to suggest that suffering the disabling IBS symptoms may make a person more likely to become anxious (or depressed). Thus, anxiety may be a cause or a consequence of gut disturbance. Alternatively, some common factor (such as neuroticism) may underlie both IBS and the comorbid psychiatric disorders. This assertion is supported by an observation that 79%% of patients with IBS and comorbid panic disorder, generalised anxiety disorder or phobias reported that their anxiety symptoms predated their bowel dysfunction by weeks or even years [13],[14]. Moreover, anxiety and depression are more common in sufferers of IBS than among patients with organic gastrointestinal disease [14].
Overall, the data suggest that there is a relationship between psychosocial problems, psychiatric disorders and IBS, at least among those who seek medical help for IBS. Further, there is an accepted lay-association between stress and IBS, such that psychological factors are recognised as its central feature. While the role of psychosocial factors in IBS has been difficult to determine, models have been proposed to explain such associations. Treatment approaches built upon these models have subsequently been developed.
Drossman and Thompson [12] have emphasised the importance of psychosocial treatments in the management of IBS. Psychological treatments including dynamic psychotherapy, hypnotherapy, relaxation training, biofeedback and assertiveness training have been suggested for use in the management of IBS, but only some have been empirically evaluated (for summaries see [15–17]). A recent review of the literature on psychosocial treatments for IBS [18] indicated that 57%% of the studies reported that psychosocial treatments were superior to control therapies. There were, however, significant methodological concerns about the studies, particularly in relation to subject recruitment, randomisation, placebo comparisons, failure to blind assessments and duration of follow up.
The relationship between IBS and psychiatric disorder may be explained by combining individual models of IBS [12] and neurotic disorders [19] with a cognitive model of somatic disorders [20]. A core feature of the hypothesis is that there is a genetically determined visceral hypersensitivity in IBS which is central to its pathogenesis [21]. Irritable bowel syndrome sufferers may experience this visceral hypersensitivity generally; alternatively, among some, it may be linked to particular foods or stress. In the visceral hypersensitivity model, individuals with IBS are particularly vigilant and sensitive about visceral sensation and, as a result of their dysfunctional cognitive style, are more likely to interpret sensations as threatening. Perceiving such sensations as threatening will increase anxiety. This heightened anxiety has a direct effect on the gut which then, in a positive feedback loop, exacerbates the symptoms of IBS (see Fig. 1) and affects bowel habit. This relationship would be very similar to the recognised role of hypervigilance and dysfunctional cognitive style in the aetiology and maintenance of the anxiety disorders. Treatment approaches for IBS aim to reduce overall anxiety levels and, presumably, visceral hypersensitivity by both anxiety management strategies and modifying the dysfunctional cognitive style of the subject; anxiety-related symptoms may then be correctly labelled and symptom exacerbation, resulting from ‘catastrophic’ misinterpretations, should be minimised.
A proposed model for irritable bowel syndrome (IBS) which describes the relationship between visceral hypersensitivity, cognitive appraisal and IBS symptoms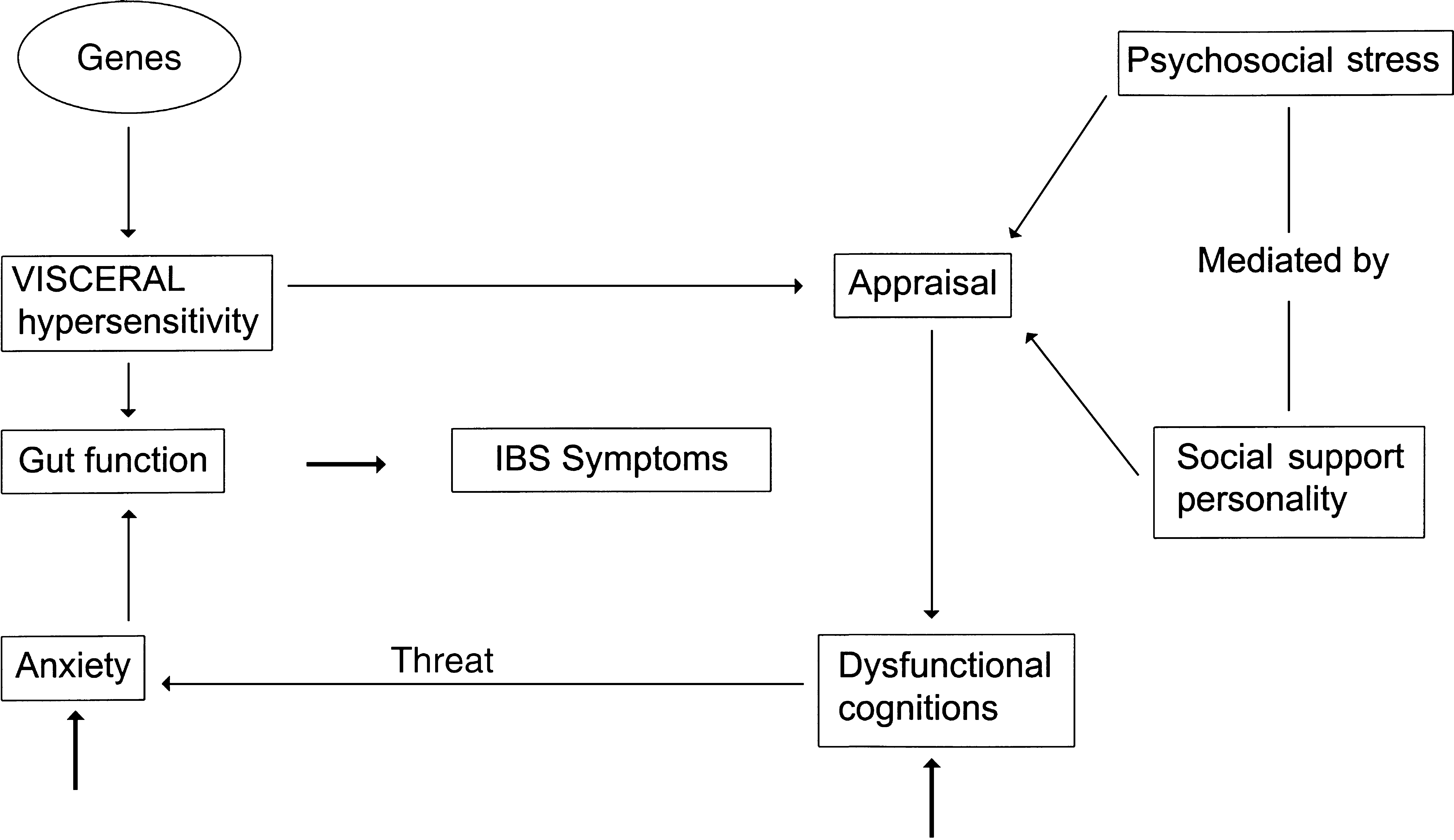
The effectiveness of cognitive-behaviour therapy as a treatment for IBS has been reported in three controlled studies. Blanchard et al. [22] compared the impact of multi-component therapy (a combination of psychoeducation, relaxation training, biofeedback and cognitive ‘stress coping training’) relative to placebo on GI symptoms. Although multi-component therapy was effective, there was also evidence that an ‘attention placebo’ was equally effective [22]. However, the attention placebo, which comprised biofeedback and pseudomeditation could be considered an active treatment. Greene and Blanchard [23] compared cognitive therapy with symptom monitoring as a placebo condition. Cognitive therapy was superior to symptom monitoring in reducing bowel symptoms, with the improvement being maintained at a 3-month follow up. Of particular note, increases in positive and reductions in negative automatic thoughts were reportedly associated with treatment gains, supporting the argument that IBS symptomatology is mediated by the individual's threatening perceptions of his or her physical health and environment. Finally, in a randomised controlled study of 34 IBS sufferers, Payne and Blanchard [24] compared individualised cognitive treatment, self-help support and a wait list control. Patients in the cognitive therapy condition demonstrated significantly greater improvement on measures of gastrointestinal symptoms, anxiety and depression than the remaining two conditions.
Because of the public health importance of IBS and the lack of efficacious medical therapies, there is a need to develop an effective and practical psychological treatment for IBS. The purpose of the present study was to examine the effectiveness of a comprehensive cognitive-behaviour treatment program, developed by the authors, in the treatment of IBS. Participants with a diagnosis of IBS each underwent a structured, eight-session, individual cognitive-behaviour therapy which was designed to modify their appraisal, interpretation and ability to cope with bowel sensations, and what may have been perceived to be medically threatening stimuli. The impact of therapy on the participants' health and wellbeing was assessed using self-report measures of bowel symptom severity and psychological morbidity.
Method
Participants
All participants were recruited from among gastroenterology outpatients attending Nepean Hospital, Sydney, Australia. They were invited to participate if aged 18 years or over. Patient exclusion criteria included undergoing psychiatric treatment; taking antipsychotic, anxiolytic or antidepressant medication; concurrent physical or psychotic illness; history of alcoholism and insufficient literacy skills. Following appropriate tests to eliminate structural bowel dysfunction, the diagnosis of IBS was made according to the international Rome criteria [6] and written informed consent was obtained from all participants.
Measures
Participants were asked to complete a battery of measures of bowel-symptom severity and psychological distress at the baseline assessment. This battery consisted of a diagnostic instrument for functional bowel disease, the Structured Interview for Bowel Symptoms (SIBS) and a measure of bowel symptoms, the Bowel Symptom Severity Scale (BSSS). The SIBS is a structured interview developed at Nepean Hospital. It follows the same format of probing for symptoms as the widely used Composite International Diagnostic Interview (CIDI), and is used to determine the presence of functional bowel disease using the Rome criteria (over the previous 3 months). The frequency and degree to which bowel symptoms interfere with life and activities are also elicited in the SIBS. There is a high level of agreement between a SIBS diagnosis and that made by a gastroenterologist (a full validation study with blinded assessment comparing a gastroenterologist diagnosis with a SIBS diagnosis is underway). These interviews and administration of the questionnaires were conducted by an independent psychologist (DR) blind to the process of treatment.
The Bowel Symptom Severity Scale provides a measure of frequency, disability and distress for each of the eight gastrointestinal symptoms associated with IBS (loose stools, hard stools, abdominal pain, bowel motion frequency, bloating, urgency to defecate, constipation and discomfort in the abdomen) over the previous week (see Appendix 1). Each of the symptoms is given a severity rating between 0 and 4, a higher rating being indicative of greater severity (with anchor points determined by the type of symptom). In addition to the SIBS and BSSS, participants also completed a daily self-report disability rating of abdominal pain, diarrhoea, constipation, belching, bloating, flatulence and nausea on a five-point Likert scale (from 0 = not a problem, to 4 = debilitating).
To assess psychological wellbeing and disability, participants were asked to complete the Beck Depression Inventory (BDI [25]); the State-Trait Anxiety Inventory (STAI [26]); and a well standardised measure of disability, the Medical Outcomes Study Short Form 36 (SF-36 [27]).
Treatment protocol
The cognitive-behaviour treatment protocol was based on a cognitive model for hypochondriasis [20] and the treatment described by Greene and Blanchard [23]. A treatment manual, modelled on and incorporating parts of that produced by Andrews et al. [28] was written (full details are available from the authors). The treatment was conducted by a clinical psychologist trained in cognitive-behaviour therapy (JG). The intervention consisted of the following eight components.
Psychoeducation
The treatment began with an explanation of the rationale for the therapeutic approach, particularly the relationship between cognition and feelings (both physical and emotional). Education was provided about the gastrointestinal system, the interaction between visceral sensation and dysfunctional thoughts and the role of diet and lifestyle factors in IBS.
Participants were introduced to the cognitive, behavioural and physiological components of anxiety and, in particular, the impact of over-breathing and muscular tension in the precipitation and maintenance of the anxiety response.
Anxiety management
The participants were instructed on two anxiety management techniques; ventilation control and relaxation training. Participants were taught standard Progressive Muscle Relaxation (Jacobson, 1938) [29], with the aid of an audiotape, and isometric relaxation.
Cognitive therapy
Following Beck's model [30], participants were trained to identify anxiety-provoking dysfunctional thoughts, expectations and assumptions, both as they related to bowel symptoms and in general terms. Participants were then taught to challenge or modify errors in their thinking to produce more accurate, rational and helpful thoughts.
Behavioural testing and graded exposure
To illustrate the role of faulty predictions and avoidance in the maintenance of anxiety and IBS symptomatology, methods of using behaviour to test predictions, and graded exposure techniques were introduced. For example, participants may predict that they are unable to attend or enjoy social functions when constipated, or to drive long distances for fear of diarrhoea. They were encouraged to gradually change their behaviour to confront such fears and challenge predictions.
Dealing with worry
Building on the cognitive techniques covered in the earlier part of the treatment program, participants were taught to use distraction, thought stopping, worry sessions, coping self-statements and cognitive restructuring as techniques to overcome excessive worrying.
Problem solving
As anxiety may result from unsatisfactory resolution of external events, specific problem-solving skills were included in the treatment program. This involved instruction on defining problems, brainstorming possible solutions, reviewing and choosing solutions and evaluating outcomes of strategies chosen to aid future problem solving.
Relapse prevention
To maintain therapeutic benefits, skills for coping with setbacks and lapses in progress were discussed with participants in the final treatment session.
In addition to a manual with comprehensive written material on each treatment session, a detailed, structured workbook (for daily homework exercises) was given to each participant. The homework exercises included daily symptom monitoring, tension ratings for the relaxation exercise, monitoring of dysfunctional thoughts, problem solving, behavioural experiments and graded exposure exercises.
Statistical analysis
Paired t-tests were used to compare pre- and post-treatment scores on the BSSS, SF36, BDI and STAI. The alpha level of significance was set at p < 0.05; all p-values were two-tailed.
Results
Eight participants (seven female and one male), aged between 24 and 71 years (mean = 41 years and 8 months) participated in the study. Ten participants were initially recruited but one subject withdrew from the study because of the development of a concomitant physical illness and a second failed to complete treatment due to unavoidable circumstances.
Gastrointestinal symptom frequency and severity
We first examined changes in the number of bowel symptoms reported. Prior to treatment, the participants reported a mean of 6.75 (SD = 1.98) symptoms on the SIBS which had occurred in the previous month, which fell following treatment to 5.38 (SD = 2.78). However, the difference was non-significant. Responses to diagnostic questions on the SIBS were examined pre- and post-treatment. Five of the eight patients no longer met criteria for a diagnosis of IBS and two remained ill. One of the patients did not receive a diagnosis of IBS on the structured interview at pre- or post-treatment but, having been diagnosed by the physician at pretreatment, was included in the study.
Mean scores obtained on each assessment measure pre- and post-treatment and summary of t-test statistics
Distress and disability associated with bowel symptoms
The distress and disability associated with bowel symptoms were calculated by summing the severity ratings on the eight symptom areas of the BSSS. A significant reduction was evident in distress from a mean rating of 2.78 (SD = 0.91) to 1.52 (SD = 0.38) and disability from 2.57 (SD = 0.98) to 1.25 (SD = 0.38) (see Table 1).
In addition to the clear face-validity of the BSSS, reliability analyses (conducted on this data) indicated that the scale has a high internal consistency (α = 0.88).
Measures of anxiety and depression
To compare pre- and post-treatment measures of both trait and state anxiety, ratings given to each of the 21 questions of the STAI (with anchors reversed where appropriate) were summed for each subscale. There was a significant post-treatment reduction in trait anxiety from 45.6 (SD = 10.1) to 35.0 (SD = 6.7), but not in state anxiety. There was also a significant reduction in mean score obtained on the BDI from 11.4 (SD = 5.9) to 4.3 (SD = 2.8) (see Table 1).
Health function
Significant changes over the course of treatment were evident in two of the subscales of the SF-36: mental health and health transition (see Table 1). Scores on physical function, bodily pain and general health also showed significant improvement with treatment. Scores on the remaining scales also improved, although the changes did not reach significance. The results are summarised in Table 1.
Discussion
Irritable bowel syndrome is a functional bowel disorder which, despite its prevalence and negative psychosocial impact, has eluded effective treatment [1]. We have carried out a pilot study of a cognitive-behaviour treatment for IBS. This treatment is based on the premise that IBS symptoms are, in part, the result of dysfunctional cognitions about visceral sensation. The therapy was designed to educate participants about physical, cognitive and behavioural factors which contribute to IBS; to teach them methods of enhancing self-control over stress, anxiety and IBS symptoms; to correct dysfunctional thoughts (such as catastrophising visceral sensations) and to prevent symptom relapse.
In this study we found that five of the eight participants did not meet criteria for a diagnosis of IBS at the conclusion of treatment. However, while there was a reduction in symptom frequency this failed to reach significance. This discrepancy may be a result of the different assessment measures. While the BSSS assesses the frequency of discrete bowel symptoms (such as loose stools or abdominal pain), the structured interview considers frequency in the context of other bowel symptoms. For example, it enquires about the frequency of a change in stool form at times when abdominal pain was present. Discrete bowel symptoms are insufficient to warrant a diagnosis of IBS which, according to the Rome criteria, should be based on an association between particular bowel symptoms within a given time period.
Perhaps the most salient finding in the present study was that the participants reported significant reductions in the amount of distress and disability associated with their symptoms. They also reported improvements in their physical functioning, pain and general and mental health. Improvements were also evident in reductions in generalised anxiety and depressive symptomatology. This suggests that while the bowel disturbance was not substantially reduced by this treatment, the participants became less concerned about the symptoms and that both their daily life and mental health improved.
There was some reduction in symptoms that could be attributed to the reduction in anxiety about bowel function. This would have an effect in reducing autonomic changes in the bowel and tend to normalise bowel activity. Even a small change in symptom frequency would have a positive effect in reducing anxiety.
A recent paper by Bennett et al. [10] reported that chronic life stress predicted the intensity of bowel symptoms. Intensity was calculated as the product of symptom frequency and severity (which was based on whether remedies had been sought and the degree of disturbance to daily activity). The measures of distress and disability used in the present study, when combined, could be considered similar to the severity measure employed by Bennet et al. [10]. Had we calculated a measure of intensity, we may have found a reduction in the intensity of bowel symptoms following treatment, despite there being no reduction in symptom frequency. The observations of Barrett et al. that symptom intensity is predicted by life stressors, supports the premise that our cognitive-behaviour treatment may have affected bowel symptoms by enhancing general stress management skills and reducing the impact of chronic stressors.
Our results are also consistent with, for example, psychosocial treatments for chronic pain, in which the treatments are variably effective in the alleviation of pain, but which often result in improved quality of life and reduced pain-related disability [31].
The findings of this study offer some support for the cognitive model of IBS. The participants were reportedly less troubled by their symptoms and, given our proposition that visceral hypersensitivity in IBS has a genetically determined biological predisposition, the reduced distress is likely to be attributable to changing cognition, which reduces the impact of this visceral sensitivity.
Whether changes in cognition related to visceral sensation produced changes in psychological well-being, or vice versa, requires clarification. Regardless, if it is the case that psychological dysfunction is a predisposing as well as a maintaining feature of IBS [14], the reduction in generalised anxiety and depressive symptoms demonstrated here may be a powerful relapse prevention strategy.
The purpose of the study was to pilot a psychological treatment program for IBS. The finding of this study suggest that cognitive-behaviour intervention is an effective treatment for IBS. There are however, limitations in this pilot study: a small sample size and no control group. These limitations are acknowledged. However, the purpose of this pilot study was to establish the effectiveness of the treatment package described and this was clearly achieved. Of course, the findings will need to be replicated in a randomised, controlled study before more definitive statements can be made about the package's general efficacy.
Notwithstanding previous reports that psychological interventions [12], particularly cognitive-behaviour therapy, are effective treatments [22],[23], the depth of knowledge is currently inadequate to set out in guidelines for optimum health care in IBS. We believe that continued investigation of a variety of psychological management approaches is required to determine the most effective and practically viable treatment.
Footnotes
Acknowledgements
This study was supported in part by a seeding grant from the Faculty of Medicine, University of Sydney.
Appendix 1