
Abstract
Keywords
Historically, doctors have had little more than their bedside manner to offer their patients alongside the few specific treatments available. Although the importance of the patient/doctor relationship is still accepted, it has been made more difficult by the progress of ever more specialized sophisticated evidence-based medicine, progress which is associated with increasing dissatisfaction of the public with their care and suspicion of medical science. This is reflected in media coverage and in the increased use of complementary and alternative medicine even within orthodox health care.
In this paper, both the wider issue of the need for psychological skills in managing all physical disorders and that of the role of liaison psychiatry in providing care and in working with medical colleagues, are explored. It is argued that psychological skills are fundamental in the management of all physical disorders. Additionally, it is argued that just as Michael Shepherd and his colleagues concluded in 1966 that the role of the psychiatrist is to support the general practitioner in the management of psychiatric illness [1], the role of the liaison psychiatrist should be to support others in their management of those with physical disorders. Although this is now multidisciplinary, psychiatrists, who are both medically and psychologically trained, should have a central role. These arguments are influenced by international contributions that have helped to determine the ways in which many of us think and practice, including those of Graeme Smith in helping to establish liaison psychiatry in Australia both as a respected academic subject and as an essential clinical service [2].
Although medical education recognizes the problem in general, there is too little awareness that the psychological and behavioural components of treatment need to be as precise and evidence based as physical treatments. It is difficult to convince more biologically minded colleagues that extra resources can be justified or that better caremay achieve both better outcomes and savings. We therefore need to define and then publicize:
the clinical needs;
effective assessments and interventions;
the skills that all doctors should possess;
the role of liaison psychiatry in providing specialist care; and
the role of liaison psychiatry in supporting and training others.
‘Psychological medicine’ and ‘liaison psychiatry’
As a starting point, we need to consider the ways in which psychiatry has so far tried to answer these needs. Treatment of nervous disorder in general medical settings, especially teaching hospitals, was one of the main elements that came together in the modern specialty of psychiatry [3]. Often known as Psychological Medicine, it began to be replaced approximately 40 years ago by what was wrongly seen by its proponents as a totally new approach – liaison psychiatry (consultation–liaison psychiatry or CL in the US and Australia). It derived from North American experience and especially from changes in medical education.
Over a good many years, the evidence, the theory and practice of liaison psychiatry were best set out by the indefatigable Professor Lipowski in extensively referenced but somewhat uncritical review papers [4]. He covered epidemiology, the meaning of illness, treatment, consultation for individual referrals and liaison with colleagues. He and hisNorth American colleagues saweducation as a primary task, a taskwhich for a while attracted substantial funding.
This work was invaluable as a basis both for our understanding of the psychological impact of physical disorder and for an expanding area of clinical practice. However, it was an approach based on inpatient practice at a time when acute medical care had a greatly more measured pace than it does now. In these circumstances, Lipowski assumed that psychiatrists should aim to assess most of the high proportion (10–20%) of inpatients with diagnosable psychiatric disorder. This never seemed realistic to those who found seeing even 1% of admissions an impossible target.
Components of a liaison service
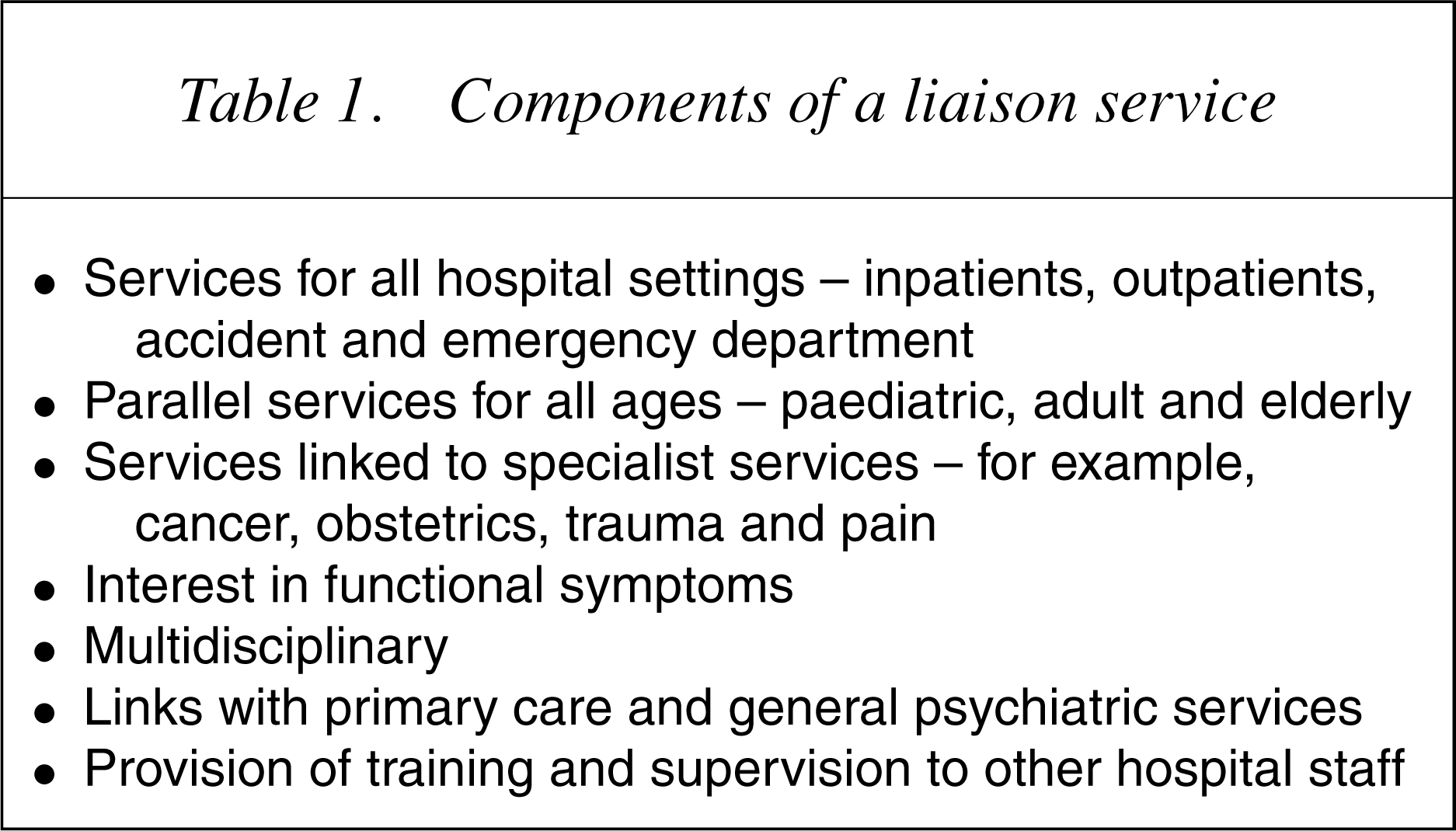
Despite the successes, the problems remain considerable. The lack of awareness within Medicine of the need for clearly defined and evaluated psychiatric skills is a major obstacle despite evidence that many apparently common sense procedures, such as much health-care advice, are ineffective or even harmful. One might hope that there would be more support within psychiatry but this is not so. Pre-occupied with so-called severe mental illness, psychiatry has neglected the greater proportion of disabling psychiatric disorder.
This lack of awareness is even more apparent in other medical disciplines, such as nursing. The contribution of clinical psychology – Behavioural medicine – is much more encouraging although sadly it is often entirely separate from psychiatry. In these circumstances, it is perhaps not surprising that there is a lack of interest by planners.
As a liaison psychiatrist who has had a career that has spanned the majority of this 40-year period, this author has been involved in the four complementary approaches described by Graeme Smith as being essential to the development of psychological medicine in its broadest sense and of liaison psychiatry [2]:
The remainder of this paper concentrates on the first approach – the evidence base – but in the conclusions it returns to the other three equally important themes. Throughout there is a consideration of what all doctors should be doing as a matter of routine and how the liaison psychiatrist can best assist.
Evidence base: the clinical problem
Psychiatric disorders are highly prevalent (approximately 20–30%) in all medical settings [5]. Many more people experience psychologically or behaviourally determined consequences of physical problemswhich affect their feelings, everyday life or use of medical care. Psychological Medicine neither implies a wider labelling of all such psychologically determined problems as psychiatric, nor does it require that psychiatry takes on responsibility for care. Rather the answers to the question posed in the title depend upon all doctors understanding the nature of the clinical problem, the effectiveness of simple and more complex interventions and what is possible within hard pressed health systems.
Major physical disorder
Liaison psychiatry is concerned with physical disorder as a threat and loss-causing psychological complications. Yet the evidence points to the fact that most people are remarkably resilient, coping with the most awful of illness even without much medical support. However, they frequently have unmet psychological needs [5–7]. The issues can be summarized as follows:
Our 15-year program of research on victims of road traffic accidents is an example. Although more than 80% of consecutive attenders at an Accident and Emergency Department suffered not more than trivial injury (such as bruises), one-third reported psychiatric disorder (depression, phobic travel anxiety and posttraumatic stress disorder) at 3 months and 1 year. Many others described chronic musculoskeletal pain, and other psychological, behavioural, social and financial sequelae. Those with evidence of previous psychological vulnerability, those who experienced very frightening accidents and those initially distressed or numbed were especially at risk. Postaccident variables, including negative cognitions and especially vague or ambiguous medical advice, also had important effects [8],[9].
Another example is diabetes. We have followed two representative cohorts of adolescent and young adults with type 1 insulin-dependent diabetes for 10 years. Psychiatric disorder (anxiety and depression, eating disorder) is somewhat more common than in comparable general populations. However, outcome in terms of mortality, physical morbidity, quality of life and very considerable use of resources is very poor, apparently because psychological and behavioural variables result not only in poor adjustment but also in poor self-care and unsatisfactory glycaemic control and thereby a greatly increased risk of serious physical complications [10].
Functional symptoms
Functional symptoms unexplained by physical disease account for more than a half of all visits to doctors [11]. They are very varied; in a minority they are persistent. Their consequences are very similar to those following illness because of major pathology. Previously seen as clinically unimportant, many now see such symptoms as a major focus for liaison psychiatry. Unfortunately, their nature and aetiology remain misunderstood and treatment is generally poor.
We have had a considerable long-term interest in understanding these symptoms. The arguments for an interactive aetiology are compelling and poor management appears to be a powerfulmaintaining factor [11]. Figure 1 summarizes aetiology and also provides a framework for management. We believe that misinterpretation of minor pathology or physiological perceptions results in worry or conviction of having a physical disorder; such beliefs can be powerfully reinforced by somatic consequences of anxiety and by iatrogenic factors such as contradictory or ambiguous medical care. The model is supported by the efficacy of cognitive–behavioural treatment. The figure also makes apparent the similarity to reactions to major physical illness.
Aetiology of functional symptoms.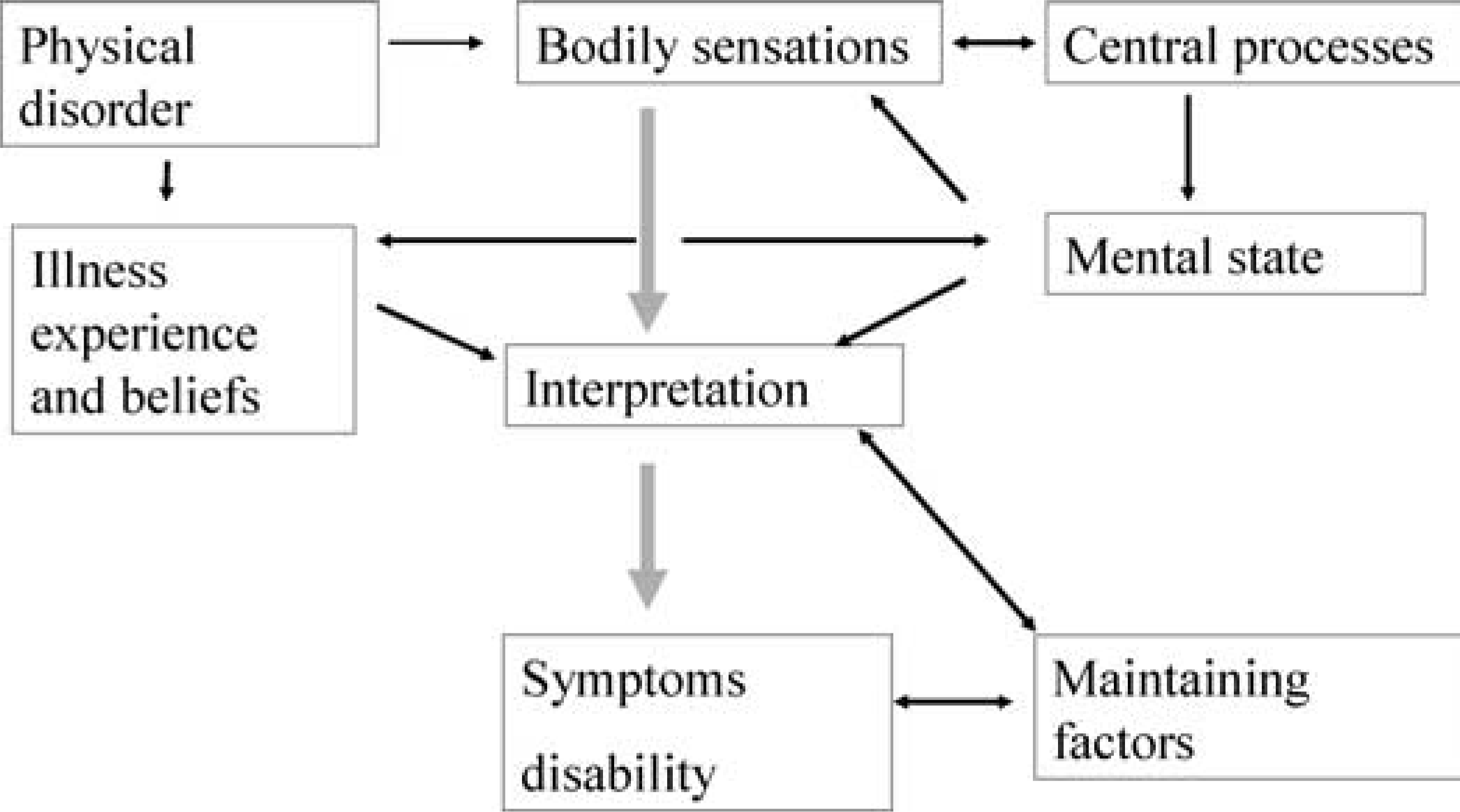
Views on the management of functional symptoms in general are based on our long-standing research interest in non-cardiac chest pain [12]. Non-cardiac pain is very common and often chronic. It is unsurprising that it is worrying to those who perceive themselves as being at risk of ischaemic heart disease, for instance those with bad family histories. It is encouraging that there is evidence for substantial benefits of psychological treatments of persistent symptoms and also for rather simple early procedures to improve patient understanding and to prevent chronicity at the time of initial presentation.
Our research and clinical experience have persuaded us that much current terminology (e.g. somatization) and the DSM classification of somatoform disorder have been deeply harmful for the understanding of functional symptoms. The current plans for a major review of classification over the next 10 years provide an opportunity for a radical rethinking. The author is one of a group of British and North American authors arguing that functional symptoms and syndromes are the best available general terms and that the somatoform category should be dropped from DSM-V and ICD-11 [13]. Our key proposals are that:
Brief review of the evidence relating to both major physical disorder and functional symptoms allows clarification of needs. Even though only a minority of those with physical disorders suffer diagnosable psychiatric complications, psychologically determined and unnecessary consequences are very frequent and clinically significant [6]. Routine medical care needs to be improved so as to either prevent or treat such complications; it is a task for liaison psychiatry to show how this can be achieved.
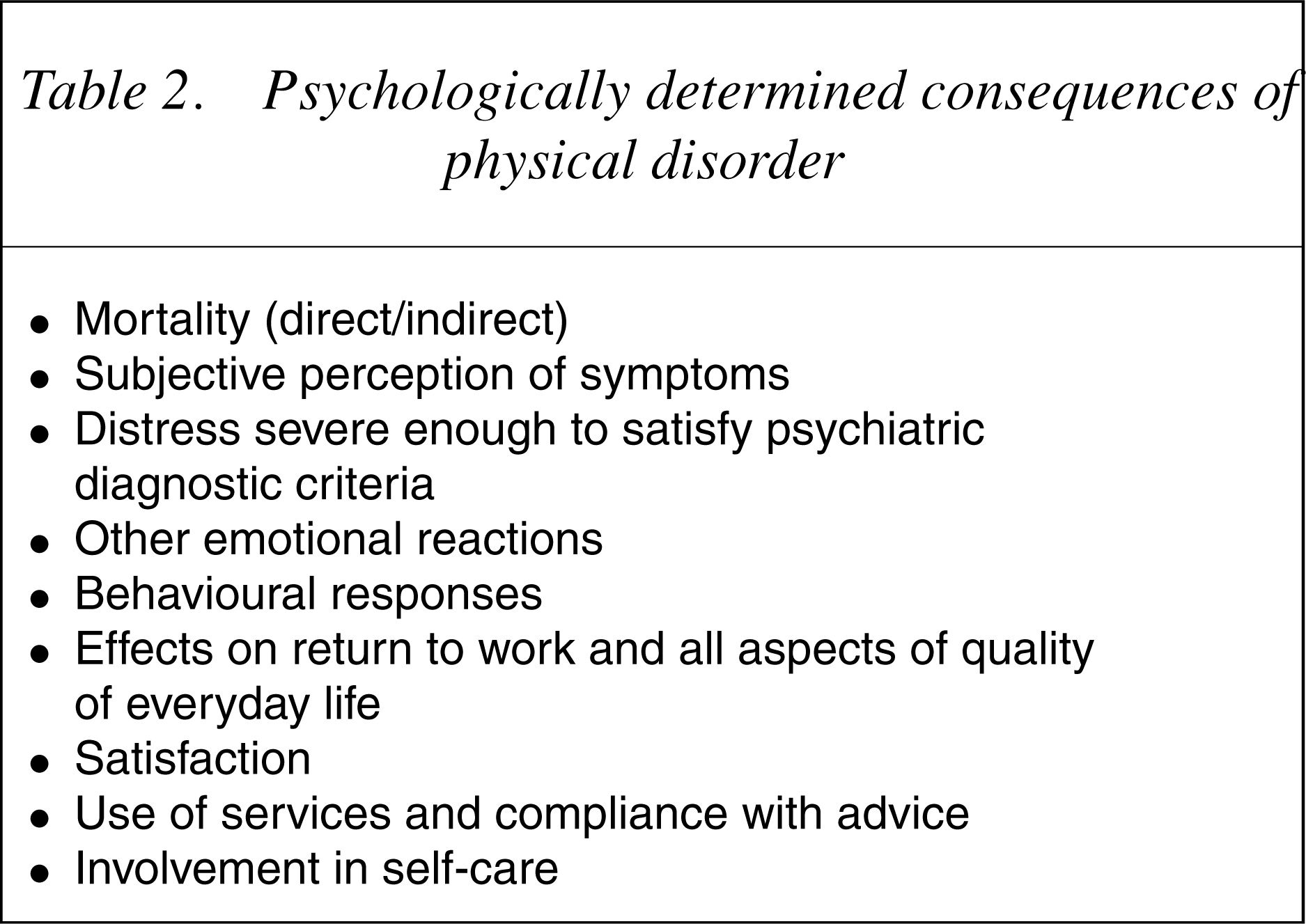
Evidence base: efficacy of psychiatric and psychological treatment
Psychologically determined consequences of physical disorder
Effective psychological and behavioural treatments
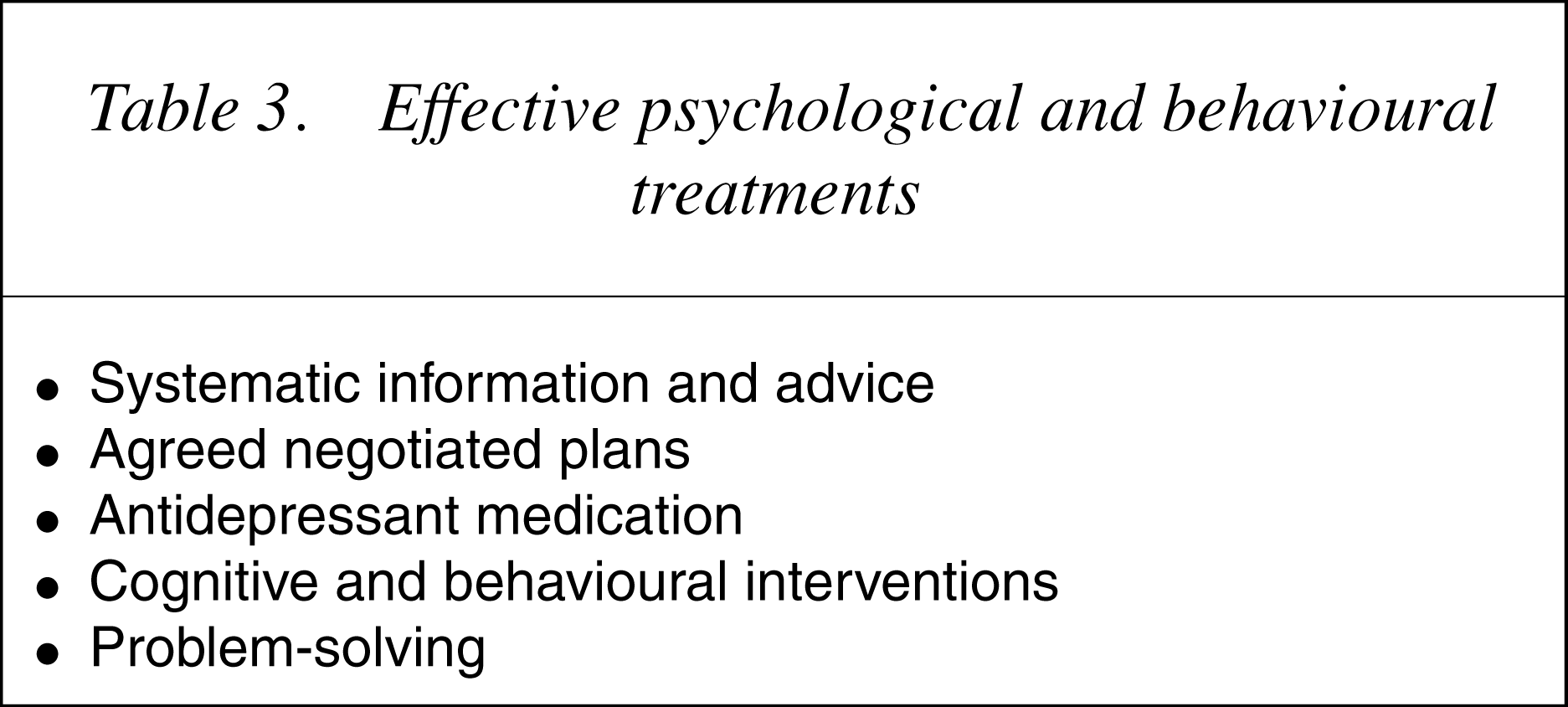
Delivering better care
Those who work with people with physical symptoms and disorder know from that clinical experience that the need for better psychological care and better outcomes is very large. Unfortunately, we also know that delivery of proven treatments in the everyday world is difficult. There are obstacles at several levels: lack of awareness, inadequate training, poor access to specialist skills, lack of organization of care and a general assumption that better psychological care is impossible within current resources. We need to tackle these obstacles and above all to make the case that this is an issue that offers the best hope for a major improvement of health care in the foreseeable future.
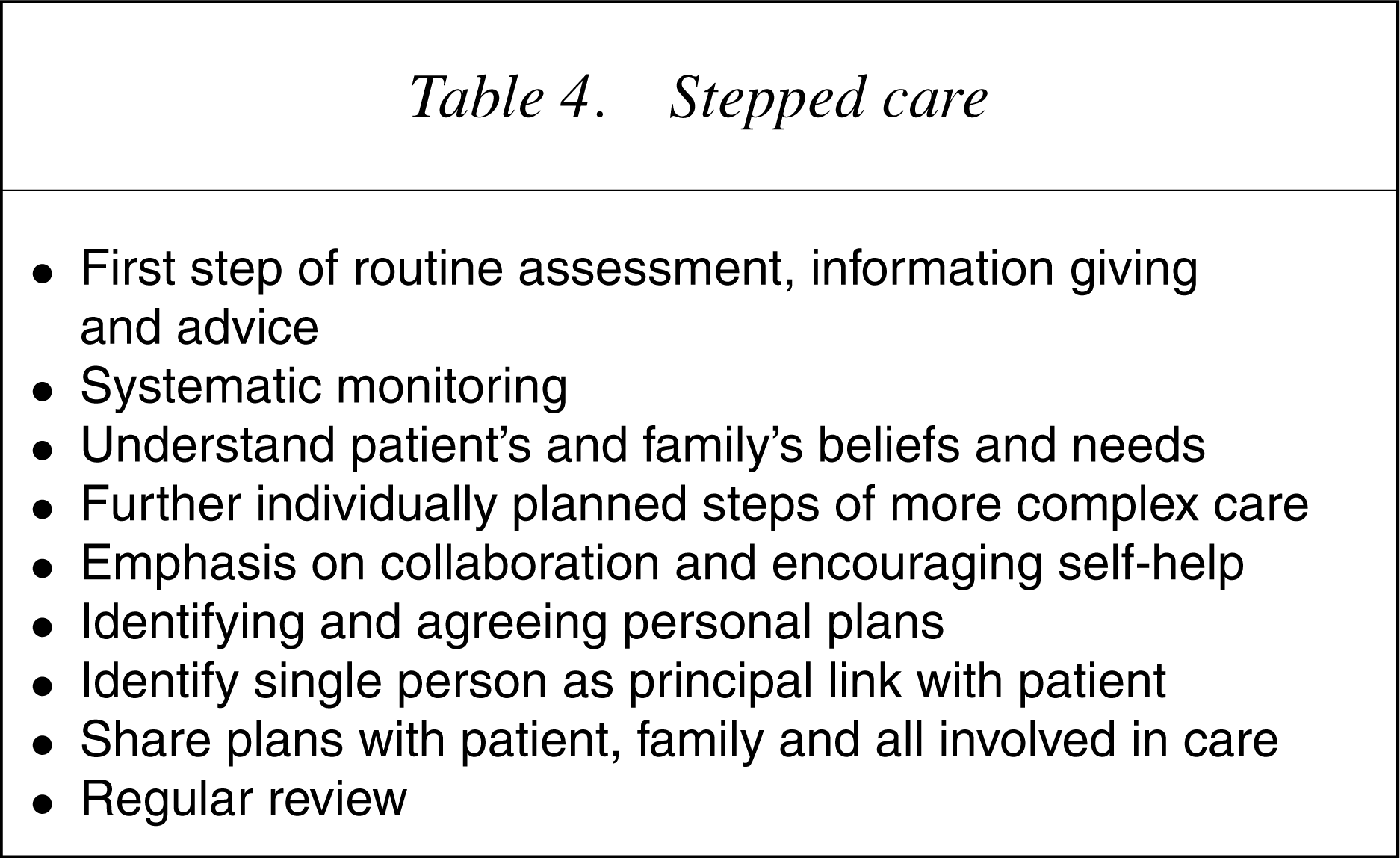
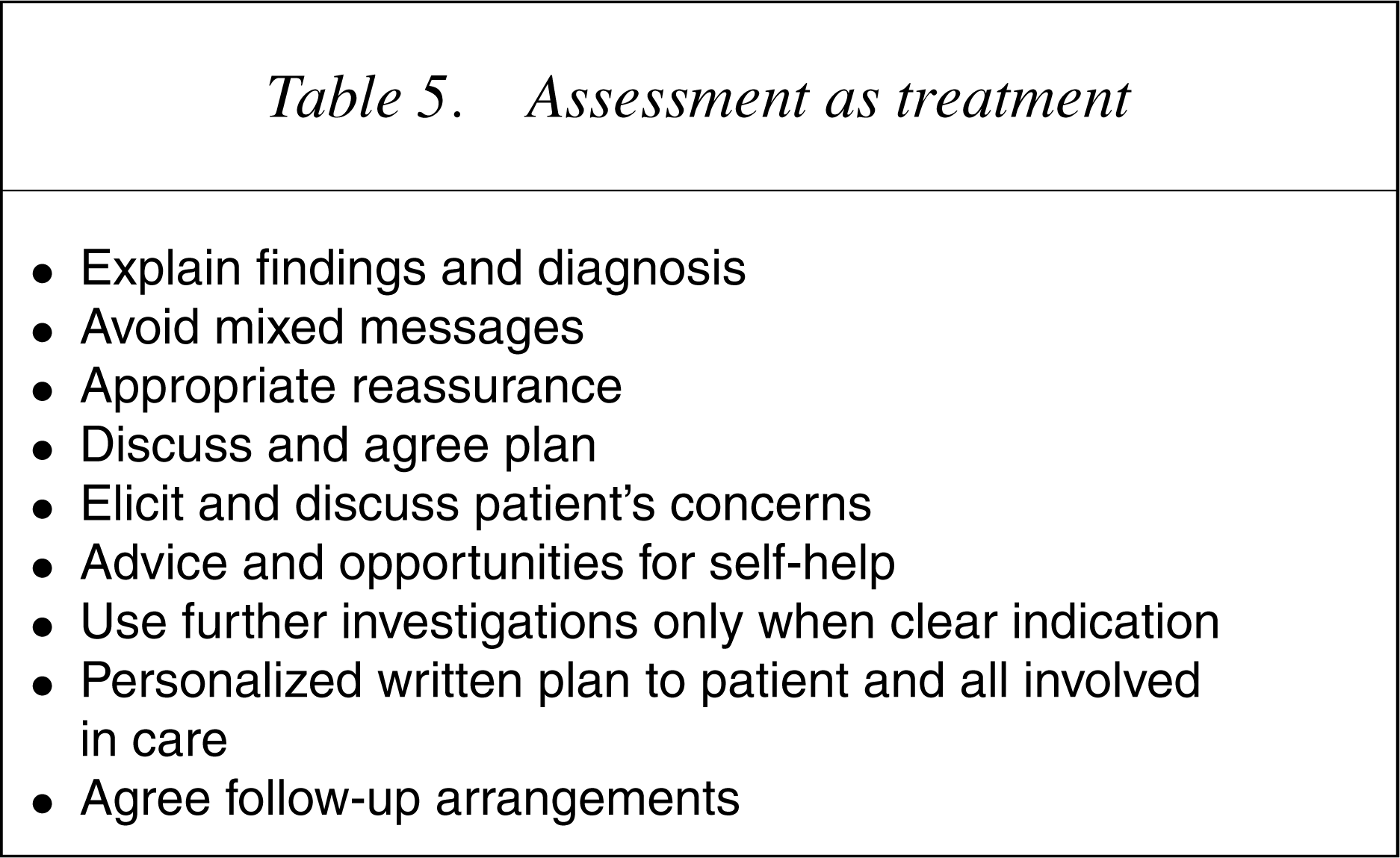
General principles
Stepped care
Assessment as treatment
We have been able to show the efficacy of such an approach in reformulating stage 1 of rehabilitation after myocardial infarction in cognitive and behavioural terms, adding a cardiac nurse-delivered session to cardiac clinic assessment and reassurance of patients presenting with palpitation. Very recently we have used quantitative and qualitative methods to investigate and modify a new nurse-led rapid access chest pain clinic [14].
A rather different example is the management of accident victims seeking personal injury compensation. Membership of a working group with a psychologist, lawyers and insurers, has emphasized the fact that cautious medical care and legal processesmay not only exacerbate problems but also delay care. In this example, there is a need, not only to move to stepped medical care principles with much earlier recognition of problems, but also to address wider legal and social factors. There are now some encouraging signs, not least in Australia, which insurers and lawyers are realizing the benefits to all of compensation procedures that promote treatment and rehabilitation [15].
Role of liaison psychiatry
Discussion of the principles and components of stepped care allows us to clarify the roles of liaison psychiatry:
Although I argue that psychiatrists should have a unique role in organizing and providing care, success in working in all medical settings must depend on the multidisciplinary team, a team that both shares skills and can offer a range of more specialized skills. The role of specialist nurses is likely to be large.
Way forward for liaison psychiatry
As the evidence base expands and issues and solutions become more convincing, we will need to return increasingly to other more political themes of liaison psychiatry so that we can have a substantial effect on delivery. Showing that we offer high quality clinical services is a starting point. In the UK, despite encouraging expansion, services are currently patchy and ‘there is a lack of rational planning’ [16]. Similar problems are evident worldwide.
Tasks
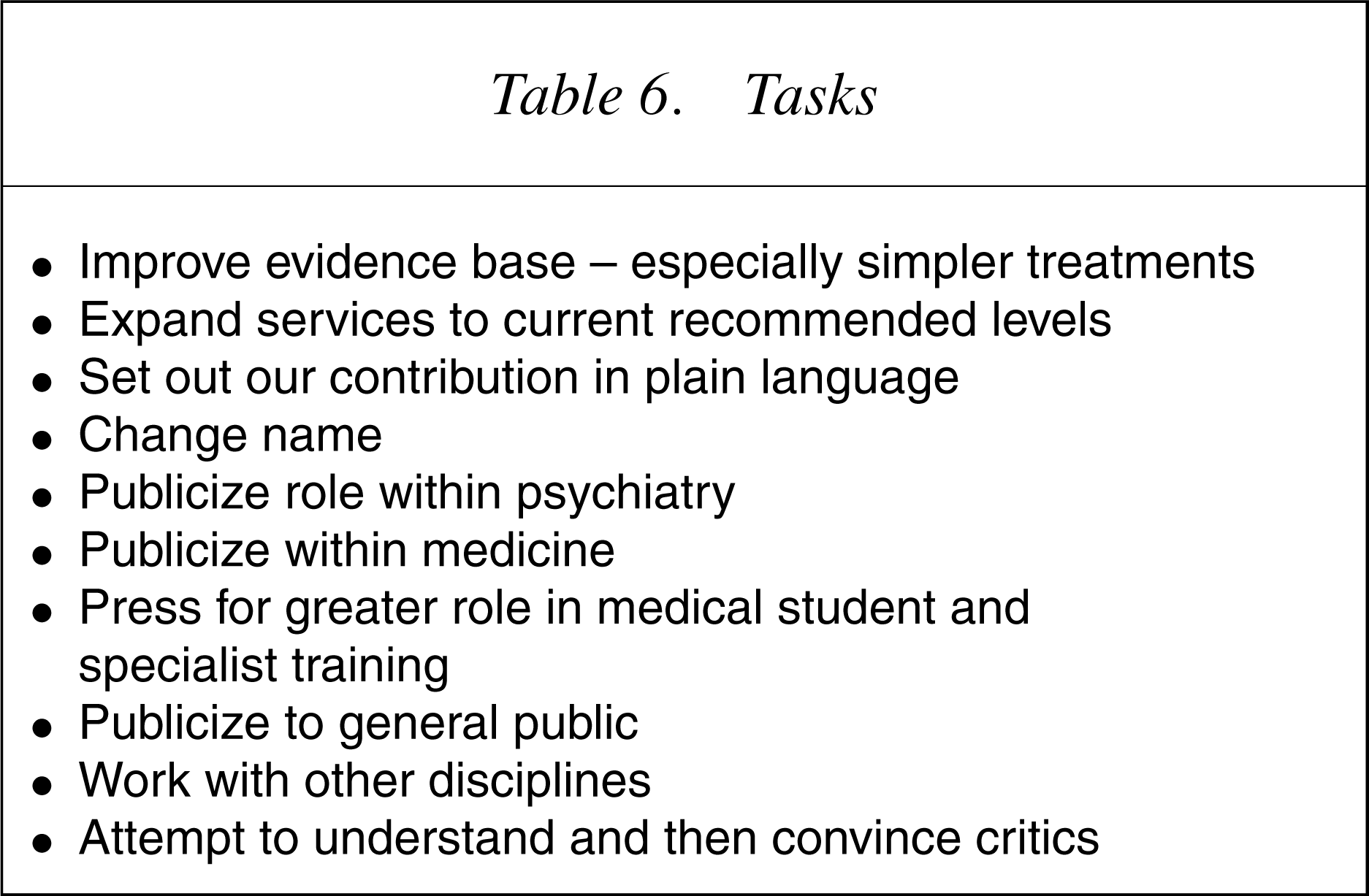
Failure to convince others should not be blamed on their obtuseness. It will be more sensible to be self-critical. There is potentially much to be gained from trying to understand the views of others including lay and patient groups, some ofwhich are excessively dominated by individuals pre-occupied with their own overvalued ideas. Liaison psychiatrists need to be prepared to change. A good start would be to abandon our meaningless terminology – liaison psychiatry, somatization, psychosomatic – and to return to a psychological medicine which meets the very obvious public wish for more caring medical service.
Conclusions
Setting out a role for liaison psychiatry, as part of a much wider approach to the effective use of psychological care, is a very large but important task. Failure will mean continued reliance on ineffective and even harmful ad hoc and alternative methods. It will mean unnecessary distress and disability and limit the delivery of powerful physical treatments. Liaison psychiatry must ensure that psychological skills are part of the treatment of all physical disorders.
Footnotes
∗Based on the 3rd Graeme Smith Lecture delivered at Monash Medical Centre, Southern Health, Melbourne, on 5 November 2004.