
Abstract
Keywords
The integrated cognitive model (ICM) of depression, proposed by Kwon and Oei [1], [2], incorporates Beck's cognitive model [3], which suggests that the activation of depressogenic schemata by stressful events elicits cognitive distortions that directly affect depressive symptomatology. The model postulates that the interaction of negative life events with dysfunctional attitudes increases the frequency of automatic thoughts, which in turn affects the depressive symptomatology of a person [2]. For example, when a person with a high number of dysfunctional attitudes (e.g. ‘If I don't have other people to lean on, I am bound to be sad’ and ‘Being isolated from others is bound to lead to unhappiness’) encounters a negative life event, such as being alone in a foreign country without any kind of social support, that person may develop automatic negative thoughts (e.g. ‘I don't think I can go on’, ‘I wish I could just disappear’ and ‘I can't stand this anymore’). Such automatic negative thoughts might, in turn, lead to depressive symptoms such as feelings of worthlessness, sleep disturbance, loss of appetite and even suicidal ideation. This model is open to the possibility of direct and independent effects of negative life events and dysfunctional attitudes on automatic thoughts and depression [2].
Studies have found a good fit for the ICM in a student population [1] and in a sample of clinically depressed patients [4]. The participants used in both studies were Australian. In their 1992 study, Kwon and Oei [1] found that the Australian student data also fitted an alternative model, namely, the symptom model (SM). Recently, Oei et al. [5] tested the validity of the ICM using Singaporean and Korean populations, respectively. These authors found support for the ICM of depression but not the SM. Specifically, these studies found support for the modified ICM which indicated a moderating role of dysfunctional attitudes and an independent effect of dysfunctional attitudes on depression via automatic thoughts.
It is now generally accepted that cognitive behaviour therapy (CBT) for depression is a treatment of choice in the US and otherWestern countries such as Australia and UK [6], [7]. There are data to suggest that CBT can also be used in Asian countries like China and Indonesia [8]. The use of CBT in non-Western samples assumes that cognitive theories and cognitive therapies developed in the Western world can be applied directly to different populations. Although there are plenty of studies examining the impact of nations on the diagnosis of disorders [9] and psychotherapy [8], very few studies have examined the relevance and validity of psychological theories in different populations in different countries. It is important that the validity of a cognitive theory be examined before a cognitive behaviour therapy is used. In order to further test the generalizability of the ICM, this study examined the validity of the ICM in a Latin-American population. This population was chosen because many studies have found higher levels of depression among Latin-American compared to Anglo-Saxon populations [10], [11].
The ICM was compared to four alternate models of depression: the SM, the alternative aetiologies model (AAM)Aand B and the linear mediational model (LMM) [1], [2]. A diagram of each model and its proposed aetiology of depression can be seen in 2]).
Models of depression: (1) integrated cognitive model, (2) modified integrated cognitive model, (3) alternative aetiologies model A, (4) alternative aetiologies model B, (5) symptom model and (6) linear mediational model. Standardized regression path estimates (∗p<0.001) indicate the change in the dependent variable for one standard deviation in the independent variable. Squared multiple correlations are shown at the top-right corner of variables.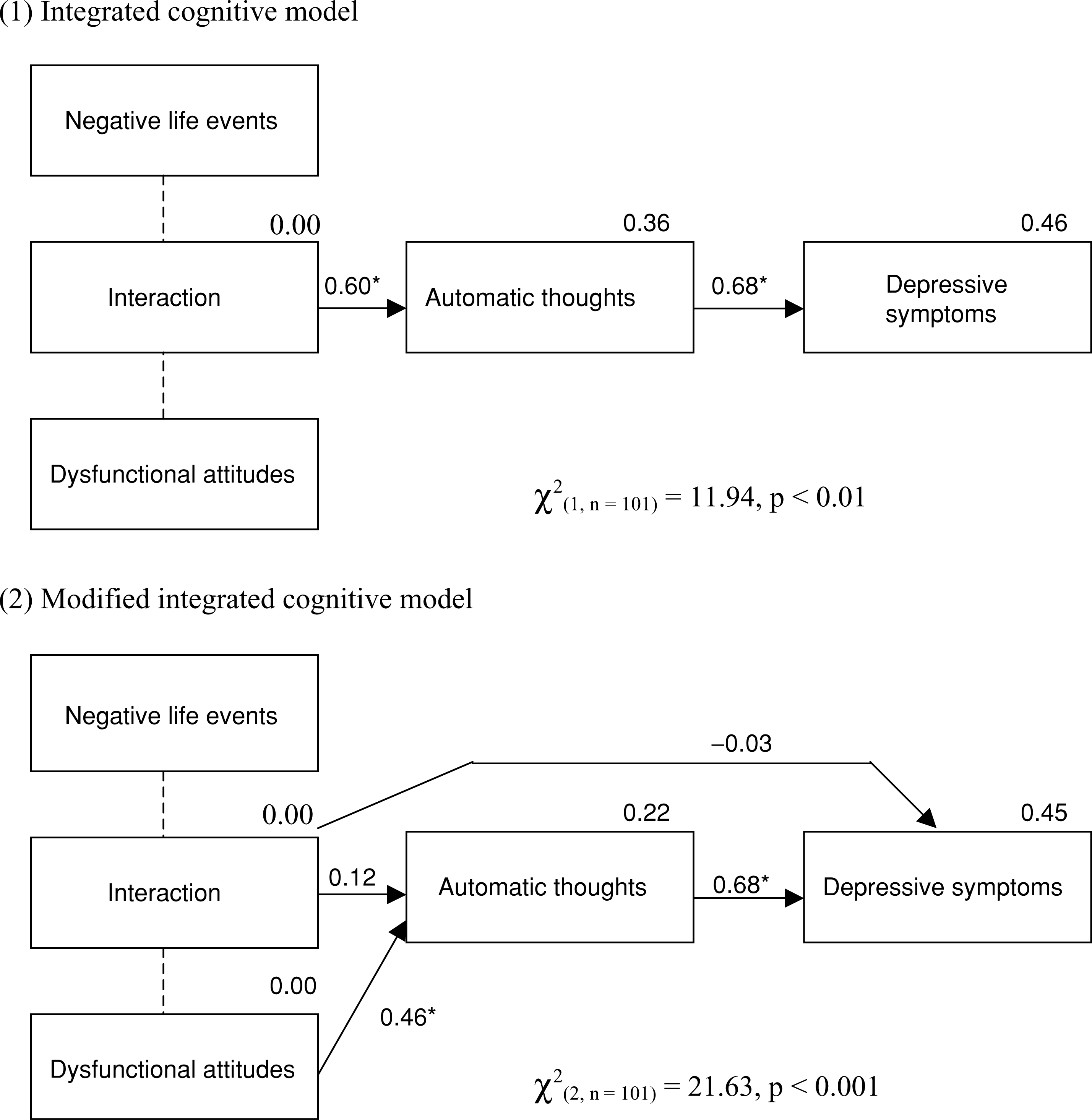
Method
Participants
One hundred and one participants were used in this study. Originally, 167 people living in Brisbane were contacted to participate voluntarily in the study. Thirty-six people did not return the questionnaire, 19 did not complete all four questionnaires and 11 did not fill in the questionnaire correctly. The return rate was 78% which is good for this type of study.
The participants used in the study were 44.6% (n=45) males and 55.4% (n=56) females. The mean age was 35.9 years (SD=14.2). The sample included people from Chile 16.8% (n=17), El Salvador 39.6% (n=40), Argentina 6.9% (n=7), Guatemala 3.0% (n=3), Nicaragua 3.0% (n=3) and non-reported countries in Latin-America 30.7% (n=31). The participants' average length of residence in Australia was 7.9 years (SD=4.5). Participants were recruited from public places such as Spanish-speaking churches, soccer clubs, social events and households. Most of the participants (68.3%, n=69) spoke Spanish at home compared to only 2.0% (n=2) who spoke English and 28.7% (n=29) who spoke both languages (one response was missing). Similarly, the majority of participants (64.4%, n=65) reported that they wrote Spanish better than English, while only 15.8% (n=16) reported they wrote English better than Spanish. The remainder (17.5%, n=18) reported equal writing skills in both languages (two responses were missing).
Measures
Four sets of questionnaires were used: the Life Events Inventory (LEI), Dysfunctional Attitudes Scale (DAS), Automatic Thoughts Questionnaire (ATQ) and Beck Depression Inventory (BDI). These questionnaires have been widely used in the research and literature on depression and only a brief summary of the measures are presented here.
Life Events Inventory
The LEI developed by Cochrane and Robertson [12] consists of a checklist of 55 events. Respondents indicate which, if any, of these events have occurred to them over the specified period of time, which was 6 months for the present study. The total score is calculated by adding the weights of the reported events and high scores indicate experience of stressful life events. The LEI has proven to be equally suitable for use with different populations [13] and other researchers [14] have supported the validity and reliability of the LEI.
Dysfunctional Attitudes Scale
The DAS, Form A [15] is a self-report scale composed of 40 items to assess typical, stable depressogenic attitudes or schemas that make individuals vulnerable to depression [15–17]. Scores on the DAS range from 40 to 280 and higher scores indicate greater dysfunctional attitudes. The DAS has been reported to have good reliability [15], [18] and validity [17], [19]. In non-Western samples the reliability of the DAS has also been reported to be satisfactory [5], [20].
Automatic Thoughts Questionnaire
The ATQ [21] is a 30-item scale designed to measure the frequency of automatic negative thoughts associated with depression. Correlations of the ATQ with the BDI, the DAS and other measures of depression, support its validity [21]. The ATQ has been found to have a high internal and discriminate reliability [19], [22]. Its accuracy with non-Western populations has been tested using Turkish [17] and Singaporean participants [5].
Beck Depression Inventory
The BDI [23] is a 21-item self-report inventory designed to provide a quantitative assessment of the intensity of depression. This inventory has been widely used with Western and non-Western participants [5], [10], [17], [24]. The BDI has been shown to be reliable [25] and valid in both psychiatric and student populations [23]. The cross-cultural reliability and validity of the BDI has also been reported to be satisfactory [24], [26].
Procedure
Latin-American migrants were approached at various places including Spanish-speaking churches, soccer clubs, social events and individual households. Fifteen per cent of the participants were composed of first-year psychology students who received credit for one of their introductory psychology courses. Ethical clearance was given by the university's ethics committee and participation was voluntary after signing a consent form. The participants received a set of four questionnaires. To reduce order effects, the questionnaires were randomized in every set. Two separate pages containing a description and purpose of the study, and a sociodemographic information form, were attached to each set of the questionnaire. It took approximately 25 minutes to complete the questionnaire package. In places, such as churches and soccer clubs, where attendance of the participants was regular on a weekly basis, the participants were informed that the data would be collected 1 week later. However, when the participants were approached individually or as a family in their households, they were asked to return the questionnaires within 1 week and a reply-paid self-addressed envelope was provided. This was done in order to save time and for the experimenter to avoid travelling long distances to each individual household. The students at the university filled out the English version of the questionnaire. The Spanish version of the questionnaire was used by people in the community. The Spanish version was translated from English by two independent translators (a psychology student and a psychologist) and subsequently backtranslated into English by two translators blind to the original version. The backtranslated versions were very similar to the original version and to each other. Minor differences in colloquial expressions in both languages were reconciled.
Data analyses
Structural equation modelling with AMOS 4.0 [27] was used to test the ICMs and alternate models to determine the best fitting model. Maximum likelihood (ML) estimation was used and a range of fit indices used to compare models. To evaluate each model, chi-square (χ2) and three descriptive indices of fit were used, the comparative fit index (CFI), the standardized root mean residual (SRMR) and the expected cross-validation index (ECVI). A non-significant χ2 indicates that the data describe the model. The CFI compares the hypothesized model with the independence model and should be 0.95 or greater to reflect a good model [28]. The SRMR provides an average difference between the variances of the sample and estimated populations, and values of 0.05 or less indicate good-fitting models [28]. An index recommended for comparing models in smaller samples is the ECVI [29]. Models with smaller values indicate the best potential of replication in samples of equivalent size and precision of the ECVI can be presented in confidence intervals.
Results
Analysis was performed using SPSS Examine and Frequencies for evaluation of assumptions. The preliminary tests of assumptions led to transformations of the variables to reduce skewness, kurtosis and improve the normality, linearity and homoscedasticity of the data. The BDI was square-root-transformed and the LEI and ATQ were logtransformed due to positive skewness. Due to the presence of negative skewness, reflect and square root transformations were used for the DAS.
The means, standard deviation and Pearson product–moment correlations of the ATQ, BDI, DAS and LEI are presented in Table 1. All variables were intercorrelated. There were negative correlations between some of the variables (ATQ with DAS, BDI with DAS and DAS with LEI). Cronbach's alphas for the ATQ, BDI and DAS were 0.92, 0.90, 0.86, respectively. The Cronbach alpha for the LEI was unnecessary due to the fact that the scale merely measures the amount of negative life events of the participants.
Means, standard deviations and Pearson product–moment correlations between the variables
Six models were tested using AMOS 4.0. A summary of goodness of-fit indices for each model are presented in Table 2. As can be seen from Table 2, the analyses indicate that both the integrated model and the modified integrated model failed to provide an adequate fit for the data. In the ICM all pathways had appropriate parameter estimates (Fig. 1). The modified integrated model also failed to fit the data and had two non-significant pathways. This suggests that for the present data the interaction of negative life events with dysfunctional attitudes did not have a direct effect on depressive symptoms and that there was no independent effect of dysfunctional attitudes on depression via automatic thoughts. Alternative aetiologies models A and B also failed to provide an adequate fit for the data, as did the LMM.
Results of the AMOS analyses of the different models of depression
Results show that the SM provided a good fit of the data. The fit indices for the SM indicated a close fit: χ2 is non-significant, the CFI exceeded the 0.95 criteria, SRMR is at the recommended 0.05 level and the ECVI had the smallest value compared to the other models and a narrow confidence interval (Table 2). All pathways had appropriate parameter estimates and the model accounted for a reasonable proportion of variance in the variables. The results indicate that depression was caused by negative life events, and automatic thoughts and dysfunctional attitudes were a consequence of depression as the SM proposes.
Discussion
The AMOS analyses support the SM. No support was found for the integrated models of depression and three alternate models (i.e. AAM A and B and the LMM). The SM corresponds to the consequence hypothesis that depressive cognitions are not a pre-existing vulnerability or cause of depression, but rather a consequence [30]. In contrast to the ICM of depression, the SM does not have an interaction between stressful life events and negative cognitions to produce depression.
The rejection of the AAM A indicates that for the present data, the influence of negative life events, automatic thoughts and dysfunctional attitudes on depression is not direct and independent. The AAM B also failed to fit the data which suggests that dysfunctional attitudes and negative life events did not have independent effects on automatic thoughts, which then influenced depressive symptoms. The LMM also failed to fit the Latin-American data showing that negative life events did not influence depressive symptoms by activating dysfunctional attitudes and automatic thoughts.
This study has two major findings. First, it supports the SM of depression showing that in the Latin-American sample depression symptoms can have an impact on negative cognitions. This is consistent with other research that has found more support for the consequence hypothesis rather than for models where negative cognitions were antecedents of depression [30]; and in two samples of Australian students both the symptom and ICM fitted the data [1]. This finding is also consistent with longitudinal studies that have failed to find the interaction between dysfunctional attitudes and negative life events [31–33].
In comparison, the current results are inconsistent with findings of a study using a Singaporean student sample [5] and recent longitudinal studies that support the interaction between dysfunctional attitudes and negative events for undergraduate students [34], senior high school students [35] and seventh-grade students [36]. Failure to find support for the integrated model may be a result of sample differences. The majority of previous studies have used a variety of student samples while this study used a non-clinical Latin-American sample.
Second, the finding that depressive symptoms can influence negative cognitions adds to growing evidence in the literature that the relationship between cognitions and depression can be bidirectional. A bidirectional pathway is not popular in current theories of depression and a unidirectional relationship from cognitions to symptoms is asserted in the cognitive behavioural therapy literature. A bidirectional relationship contends a causal reciprocal relationship between cognitions and depression, in which negative cognitions produce depression which, in turn, increases the frequency of negative cognitions. In 1967, Beck [37] speculated about this bidirectional relationship and since then it has been used to describe how depression is perpetuated and intensified [38]. Although the current study provides evidence for the pathway from depression to cognitions, studies on other communities have found evidence for a relationship operating in both directions [1]. Support for the bidirectional relationship is also found in research on the change processes of treatments for depression. Drug therapy studies for depression have found a significant decrease of negative cognitions, without the use of other interventions [39], [40]. In the future, carefully designed research needs to examine the reciprocal relationships among dysfunctional attitudes, automatic thoughts and depression and to investigate its role in each of the phases of depression.
This study is the first to investigate the causes of depression in a community sample of Latin-Americans in a Western population. It has been said [8], [9] that most CBT theories, and thus CBT treatments, were generated in Western countries and may not be applicable to non-Western countries. Therefore the findings have some implications for the treatment of depression. The similarity to findings in previous research [1] indicate the main cognitive constructs of Latin-American people, such as the roles of dysfunctional attitudes and automatic thoughts, may share similarities when compared to Western populations. This provides initial support that Western-based theories and treatments for depression may be suitable for use in some non-Western populations. However, more research using samples from different cultural backgrounds is needed to provide evidence of cross-cultural suitability.
A few limitations should be kept in mind when drawing inferences from the results. The results of the present study were based on a community sample of Latin-Americans in Australia and cannot be directly generalized to clinical populations or to populations outside Australia. Further research is therefore needed to test the models of depression across other sample groups. The use of cross-sectional data also necessitates longitudinal research in the future to confirm causal relationships between depression and cognition.
In conclusion, the present study supports the SM in the Latin-American sample and not the integrated model of depression or other alternate models. This shows that in the Latin-American sample depression symptoms can have an impact on negative cognitions, adding to the growing evidence that the relationship between cognition and depression is reciprocal.