
Abstract
Keywords
Overseas studies have produced convincing evidence to suggest that cognitive behavioural treatment (CBT) is effective for people with mild and moderate major depression. One meta-analysis found that cognitive therapy (CT) produced a greater degree of change in clinical depression compared with a waiting list or no-treatment control, pharmacotherapy, behaviour therapy or other psychotherapies [1]. Another meta-analysis of 78 controlled clinical trials on the efficacy of CT for depression by Gloaguen et al. showed that CT appeared to be significantly better than the waiting-list, antidepressants or a group of miscellaneous therapists [2]. A most recent review of 40 years of studies on CT for different types of psychiatric disorders suggests that CT is effective for people with major depression [3]. Another review, which summarizes the current meta-analyses on treatment outcomes of CBT, suggests that the largest effect sizes were found when using CBT for major depression, and further that CBT was superior to antidepressants and equally effective as behaviour therapy in the treatment of adult depression [4]. Some studies have also found a longer-term effect of CBT for people with depression. For example, Hollon et al. found that patients withdrawn from cognitive therapy were significantly less likely to relapse during continuation than patients withdrawn from medications (30.8% vs 76.2%) [5].
Several studies have provided evidence about the effectiveness of group CBT for people with mild and moderate depression [6–8]. A meta-analysis of 48 studies on group therapy (in which two-thirds of these 48 studies involved the use of CBT) by McDermut et al. also confirmed the effectiveness of group CBT for depressed patients [9]. In another randomized wait-list study, group CBT was found to have enduring effects at 6 month and 12 month follow up [10].
In Hong Kong the prevalence rates of depression among men and women in the age group 18–64 years is 1.44% and 2.60%, respectively [11]. Due to the various economic, social and political changes, these percentages are expected to increase [12]. It is estimated that 12–15% of people suffering from depression will require some kind of rehabilitation measure [13]. This increase in the number of people with depression has put enormous strains on psychiatric services in Hong Kong: there is a long waiting period of 6–8 months for the first psychiatric consultation. Moreover, there are very few alternative treatments available for people with depression in the community, and the waiting list for psychotherapy and counselling services is also very long. Given these circumstances, there is an urgent need to explore alternative treatments for people with depression in Hong Kong.
Very few studies have empirically examined the efficacy of CBT for Chinese people. A few recently published studies have found initial evidence to support the efficacy of group CBT for treating people with chronic illness [14], social anxiety [15] and depressive symptoms [8] in Hong Kong. The study conducted by Wong on people with depressive symptoms was based on a relatively smaller clinical sample, and did not contain multiple process and outcome indicators that could provide more convincing evidence of the efficacy of group CBT for depressed Chinese people in Hong Kong [8]. In order to further demonstrate the efficacy of group CBT, the authors decided to conduct a territory-wide clinical trial of a community sample of people who had mild to severe depressive symptoms as indicated by Beck Depression Inventory–Chinese version (C-BDI) scores. These authors had also added multiple process and outcome indicators such as perfectionism and quality of life in that study, thus hoping to illustrate the outcomes of group CBT for depressed Chinese people in Hong Kong.
Relationships between dysfunctional attitudes, perfectionism, depression and quality of life
The cognitive model of depression postulates that people with depression have a stable cognitive structure characterized by biased interpretations (i.e. cognitive distortions) of life events; the existence of rigid dysfunctional attitudes, rules and values (i.e. negative schemas); and a ‘global negative view of self, the world and the future’ (i.e. cognitive triad) [16]. Essentially, people who have negative schemas in the forms of rigid dysfunctional attitudes, rules and values may harbour certain distorted worldviews that can result in unrealistic expectations of self and/or others. This latent dysfunctional schema is relatively stable and serves as a vulnerability factor in the development of depression when it interacts with environmental stressors such as negative life events [17]. In the literature there is still little consensus on the aetiological role of dysfunctional attitudes in depression [18]. While several studies have suggested a positive relationship between dysfunctional attitudes and depressive symptoms [8], others have failed to find such a relationship [19].
Perfectionism is considered to be another cognitive variable related to the development of depression [20]. It is multidimensional and is characterized by a predisposition towards striving for flawlessness [21]. In the literature, perfectionism consists of three dimensions: high standards, discrepancy, and order [22]. ‘High standards’ is interpreted as an indicator of adaptive perfectionism and reflects the high personal standards and expectations that one places on oneself. ‘Discrepancy’ is interpreted as a negative aspect of perfectionism and denotes the degree of stress experienced when individual performance consistently does not meet expected standards. Last, ‘order’ refers to a tendency to value a sense of order and organization. The ‘high standards’ dimension has been positively related to measures of self-esteem, whereas the ‘discrepancy’ dimension has been positively related to measures of psychological distress including depression [23]. One study conducted by Wang et al. among Taiwanese Chinese students produced similar findings [24].
There are very few studies that examined the relationship between perfectionism and quality of life of individuals with depression. A study conducted by Gilman and Ashby found that, generally speaking, there was a positive relationship between the setting of high personal standards and all dimensions of quality of life, including friends, self, family, living environment and school among a group of school-aged children [25]. In contrast, the inability to consistently meet these standards was negatively and significantly related to the various dimensions of quality of life. In 2005, Gilman et al. conducted a cross-cultural study that compared the relationship between perfectionism and multidimensional life satisfaction among Croatian and US youth [26]. Results found that ‘high standards’ was a positive predictor of school satisfaction for both cultural groups. In contrast, ‘discrepancy’ was a significant and negative predictor of self-satisfaction between the two groups. Clinical studies using perfectionism as an outcome measure found that the participants in CBT workshops had significant reduction in perfectionist attitudes at post-test and follow-up assessment [27].
Applications of the cognitive model of depression for Chinese subjects
Lin; and Hodges and Oei argue that cognitive behavioural therapy is highly compatible with Chinese culture because the therapy is structured and solution-focused [28], [29]. This suggestion is based on the understanding that Asian subjects (including Chinese subjects) tend to have less tolerance for ambiguity and prefer structured counselling sessions with practical and immediate solutions to their problems [30]. Also, Chinese people prefer that therapists use a direct rather than a non-direct approach, and expect the therapists to play an active role in providing suggestions and advice in the counselling process [28].
Based on the Chinese CBT manual developed by the authors in Hong Kong [31], we designed and implemented group CBT programmes for treating Chinese people with depression in Hong Kong. Each programme contained 10 sessions, with each session lasting 3 h. The contents of our group CBT manuals for depression focused on helping participants to (i) understand and modify their patterns of automatic thoughts and dysfunctional rules; (ii) gradually build up pleasurable activities; and (iii) identify negative coping skills and enhance positive ones. In order to adjust to the cultural characteristics of Chinese people, all technical terms were translated into colloquial expressions. For example, ‘automatic thoughts’ was renamed ‘thought traps’ and the cognitive distortion of ‘personalization’ was rephrased as ‘put all the blame and responsibilities onto oneself’. Second, we designed a number of worksheets and exercises in Chinese to facilitate the understanding of the cognitive and behavioural processes and the learning of cognitive and behavioural skills. Third, we emphasized the exploration and modification of dysfunctional rules relating to family and interpersonal relationships. Clinical experience and a review of the literature both lead to the conclusion that Chinese people have a lot of family and interpersonal relationship rules that can become a potential source of stress for Chinese people [32], [33]. Fourth, the group leaders were actively involved in structuring and facilitating the group processes, particularly in the initial stage of the group development. Last, the group leaders delivered mini-lectures and provided a detailed explanation of the exercises and worksheets to the participants.
In the present study the researcher attempted to further test the efficacy of group CBT for people with mild to severe depressive symptoms in Hong Kong. The two hypotheses were: (i) the members in the experimental groups would have fewer depressive symptoms, fewer dysfunctional attitudes, less discrepancy and ‘higher standards’, and better quality of life than members in the control groups at the end of the group intervention; and (ii) changes in dysfunctional attitudes, ‘discrepancy’ and high standard would be associated with changes in depressive symptoms.
Methods
Participants
This was a 2 year project that began in July 2005 and ended in June 2007. Ethics approval was obtained from the human research ethics committee of the University of Hong Kong. A total of 364 potential participants were recruited either from referrals or advertisements posted at the hospitals, psychiatric clinics, integrated family service centres, and community centres of major geographical clusters in Hong Kong: Hong Kong Island, Kowloon (East and West) and New Territories (Shatin, Tuen Mum and Tung Chung). The inclusion criteria included: (i) age 18–60 years; (ii) presence of major depression as defined in DSM-IV; and (iii) presence of mild–severe depressive symptoms on C-BDI. Those participants who had a psychiatric diagnosis of depression had their psychiatric statuses confirmed through the referrers who were psychiatric nurses, social workers and clinical psychologists of the respective clinics and hospitals. These referrers obtained the diagnoses from the participants’ medical records or by consulting with the participants’ respective psychiatrists or psychiatric doctors before confirming the participants’ diagnoses with us. Individuals who had a psychosis and severely acute depressive symptoms at the time of the interview were excluded from the study and were referred to other places for psychiatric assessment and intervention. Likewise, individuals who had had a recent suicide attempt or active suicide plan in the past 3 months were excluded from the study and were referred elsewhere for active treatment. Information regarding the presence of suicide attempt/plan was obtained from the referrers, who solicited the information using the same procedures as described here. At the telephone screening, nine potential participants with severely acute depressive symptoms and recent suicide attempts were not offered a pre-group interview and were referred back to the psychiatric services for follow up (n = 9). Six potential participants who were offered the services refused to participate in the study because they preferred individual counselling to group counselling after receiving further information about the group processes at the pre-group interview (n = 6). Two did not want to wait for the services and declined to join the wait-list control group (n = 2). Finally, 347 individuals decided to participate in the study after the pre-group interview. All participants voluntarily signed a consent form that explained the purpose and nature of their involvement in the project. As soon as a centre had accumulated enough participants to be selected for the experimental and control groups, a colleague who worked in the same department as the first author but who had no affiliation with the research team would then be invited to randomly assign these participants to the experimental and the wait-list control groups.
Procedure
Each participant was asked to fill out the questionnaire at the beginning and the end of the treatment. A structured group CBT programme was designed and run for the participants in the experimental group between the times of measurement, whereas no group CBT treatment was given to the participants in the control group. The control subjects were given group treatment after the control group study was finished.
The group leaders were trainees of the group CBT training programme at University of Hong Kong. They were 20 social workers (i.e. two from each of the 10 agencies) and had at least 2 years of social work experiences. This training lasted for 1½ years. Essentially the trainees participated in a 3 day in-house theoretical and skills training course in CBT. They were then asked to recruit and run group CBT programmes in their respective agencies under the coaching of three experienced CBT trainers: two of them were on teaching staff at universities, one of whom was a qualified cognitive therapist trained at the Beck Institute in the USA. The third one was an experienced social worker with training in mental health and CBT. All trainers actively participated in the groups and co-ran all the groups with the trainees. Debriefing and supervision took place immediately after each group session. There were 7–8 members in each treatment group.
There were two observers who were invited to examine the treatment adherence of these CBT groups. Each of the observers independently reviewed 12 videotapes from sessions 1,4,8 of four randomly selected experimental groups. The contents of the three sessions revolved around ‘understanding the relationships among cognitive, behavioural, physiological and emotional responses’, ‘identifying automatic thought patterns and developing healthy cognitive and behavioural responses’ and ‘identifying and modifying dysfunctional rules’. Because the group content was manualized, it was easier for the research team to develop a checklist of the tasks to be completed in the three sessions. The two reviewers were asked to check each of the items in the checklist and see if the group leaders had completed the prescribed tasks. Essentially, the checklist contained items denoting the essential tasks and the CBT strategies that had to be performed by the group leaders in a specific session. The checklist was rated in the format of a yes/no answer. The results from the checklists indicated that the group leaders had completed all the prescribed tasks. Therefore, there was no disagreement in the checklists between the two reviewers.
Instruments
The BDI is a 21-item self-report inventory originally developed to measure depression [34]. Previous studies have shown that the BDI is a reliable and valid measure of severity of depression in clinical settings [35]. In the present study the C-BDI was used as the primary outcome measure. The reliability and validity of the C-BDI were confirmed in previous local studies [36], [37]. A decrease in the total score signified a reduction in the severity of depression. The C-BDI achieved high internal consistency in the present study (Cronbach's α = 0.90).
The Almost Perfect Scale–Revised Version (APS-R) is a 23-item scale developed to measure perfectionist attitudes held by an individual [22]. It is a multidimensional concept with three subscales. The Discrepancy Subscale measures the degree to which the respondents perceive themselves as failing to meet their standards for performance (12 items). The High Standards Subscale measures the possession of high standards for achievement and performance (seven items). The Order Subscale measures a preference for neatness and orderliness (four items). It is a 7-point scale, with 1 denoting ‘strongly disagree’ and 7, ‘strongly agree’. Exploratory and confirmatory factor analyses have supported the three-factor structure [22]. The Chinese version of the APS-R was developed by Wang et al. and has high internal consistency, with Cronbach's alpha ranging from 0.73 to 0.87 [38]. In the present study the discrepancy and high standard subscales were used because previous studies found that both subscales were predictive of psychological distress [23]. The discrepancy and high standard subscales achieved good reliability scores of 0.72 and 0.85, respectively, in the present study.
The Abbreviated Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-18) was developed by Endicott et al.[39] and later validated for use for schizophrenia, schizoaffective, and mood disorder patients [40]. This scale measures the level of life satisfaction of an individual and it contains five dimensions: physical health, subjective feelings, leisure activities, social relationship, and medication. The scale was translated into Chinese by an academic and then back-translated into English by an independent translator. Two academics in the field of social sciences had read and compared the translation with the original English version separately. Modifications were made according to their suggestions. It is a 5-point scale, ranging from 1, not at all, to 5, all the time. It was assumed that the higher the score, the greater the subject's satisfaction. The scale and its subscales achieved high internal consistency, with a Cronbach's alpha of 0.90 for the total scale, 0.71 for physical health, 0.73 for subjective feelings, 0.73 for leisure activities and 0.85 for social relationships. The medication subscale has only one item and no reliability test could be performed.
The Dysfunctional Attitude Scale (DAS) was adopted and translated from Weissman and Beck's original scale which was presented at the meeting of the Association for the Advancement of Behavior Therapy, Chicago, in 1978. The DAS 40-item Form A (DAS-A) was used in the present study. The Chinese version was translated and validated by Chen et al.[41]. This scale measures the dysfunctional beliefs held by the subjects, and reflects the content of one's cognitive schema [42]. It was assumed that the fewer dysfunctional beliefs a person has, the more functional is the person's cognitive processes. This scale achieved a high level of internal consistency in the original study (Cronbach's α = 0.92).
Statistical analysis
All data analyses were primarily conducted for the participants who completed the treatment or the waiting period. For the post-group data, an intention-to-treat analysis, in which the scores at pre-test assessment were entered for the subjects who dropped out from the study before the post-group assessment, was also conducted. Differences between the treatment and control groups were examined using analysis of covariance (ANCOVA), with the pre-test score of each outcome measure treated as the covariate, so that the post-group outcome could be adjusted with respect to the baseline severity. Effect sizes were calculated using Cohen's d (difference between adjusted means divided by the pooled standard deviation) to examine the size of the differences between the experimental and control groups at post-test assessment [43]. In order to ascertain the clinical significance achieved by a participant in the experimental group, a statistical approach to clinical significance suggested by Jacobson and Truax was adopted [44]. Essentially, a participant who had achieved a reliable change index (RCI) score >1.96, >1.28, or >0.84 in the C-BDI at post-test assessment would be considered clinically recovered, remitted, or improved, respectively [45]. This method was preferred because there is no clinical cut-off score for the C-BDI in the Chinese population in Hong Kong. Last, hierarchical regression was performed to examine the independent effects of perfectionism and DAS at pre-test assessment on C-BDI at post-test assessment, and perfectionism, DAS and C-BDI at pre-test assessment on Q-LES-Q-18 at post-test assessment in the experimental group.
Results
Demographic data were compared between the experimental and the control groups, using ANOVAs for continuous variables and χ2 tests for categorical variables. There was no significant differences between experimental and control groups on all demographic variables (all p > 0.22), indicating that the experimental group and the control group shared similar characteristics before treatment began for the experimental group. ANOVAs were also used to compare the pre-test scores of all dependent variables between the experimental and the control groups. No significant differences were found between the two groups (all p > 0.20).
Eleven and four participants from the control and experimental groups failed to finish the wait-list period and the group CBT programme, respectively. There were therefore 322 participants who completed the post-test assessment, 163 of whom were in the experimental groups and 159 of whom were in the control group. The attrition rate differed across the group conditions (Fisher's exact test, p = 0.01). Among the 11 who dropped out of the control group, eight decided to seek help from other services after waiting for a period of time, two were hospitalized when they were called to receive group treatment and one had recently attempted suicide. For the four individuals who dropped out of the experimental group, all of them mentioned that they did not feel comfortable in the group setting, and did not want to continue. Of the 163 participants in the experimental group, approximately 90% (n = 147) completed at least eight group sessions.
In the present study the mean age of the participants was 42.72 years (SD = 8.73). Approximately 77.6% of the participants were female (n = 250) and the rest were male. Approximately 23% were unmarried (n = 76), 55% were married (n = 178) and the rest were separated or divorced. Approximately 60% had completed their secondary education (n = 190), and 28% had even received tertiary education (n = 90). Approximately 39% of the participants were in full-time employment (n = 127) and 14.9.5% were unemployed (n = 48). The mean duration of illness was 4.8 years (SD = 5.1). Approximately 67% had a diagnosable depression (n = 218), 62% were receiving psychiatric treatment (n = 200), and 65% were taking medication (n = 208). Participants who were taking medication were taking tricyclic antidepressants or selective serotonin re-uptake inhibitors and there was no statistical significant difference in the outcome variables at pre-test assessment between those who were taking medications and those who were not.
Table 1 presents the pre-test and post-test results of both the experimental and control groups. The ANCOVAs indicated that there were significant between-group differences in the C-BDI (F(1,321) = 57.44, p = 0.00), Q-LES-Q-18 (F(1,321) = 30.16, p = 0.00), perfectionism–high standards (F(1,321) = 10.28, p = 0.00) and DAS (F(1,321) = 16.52, p = 0.00), but no significant group difference was found in perfectionism–discrepancy (F(1,321) = 1.82, p = 0.18). Thus, when compared with the control group, the experimental group members had a reduction in the severity of depression, had better quality of life, and fewer perfectionist and dysfunctional attitudes. Effect size analyses using Cohen's d [44] indicated small to medium differences in the C-BDI (Cohen's d = 0.74), Q-LES-Q-18 (Cohen's d = 0.61), DAS (Cohen's d = 0.44), perfectionism–discrepancy (Cohen's d = 0.22) and perfectionism–high standards (Cohen's d = 0.32) between the experimental and control groups at post-test assessment (Table 2).
Outcome measures (n = 322)
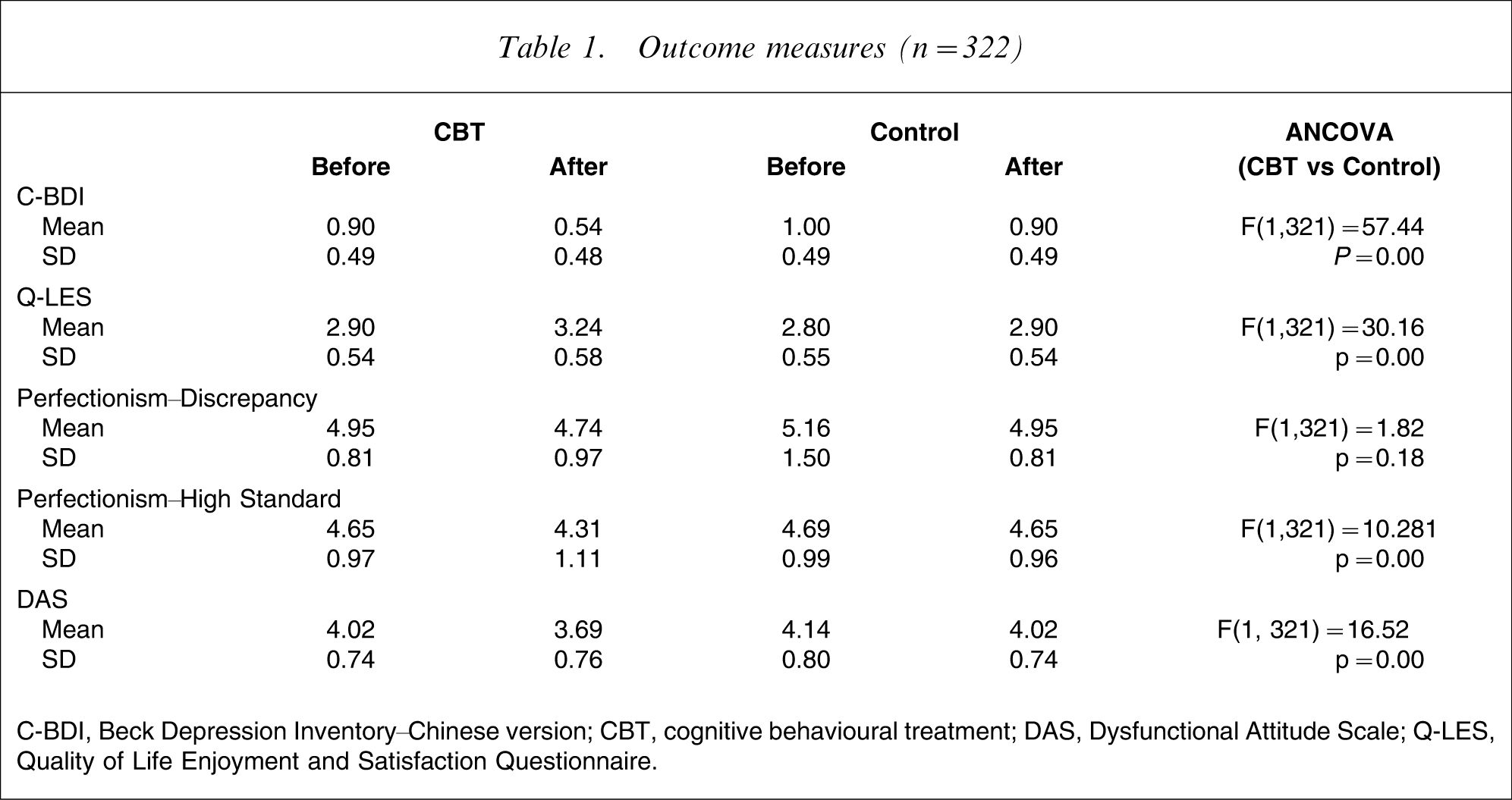
C-BDI, Beck Depression Inventory–Chinese version; CBT, cognitive behavioural treatment; DAS, Dysfunctional Attitude Scale; Q-LES, Quality of Life Enjoyment and Satisfaction Questionnaire.
Effect size at post-test assessment (n = 322)
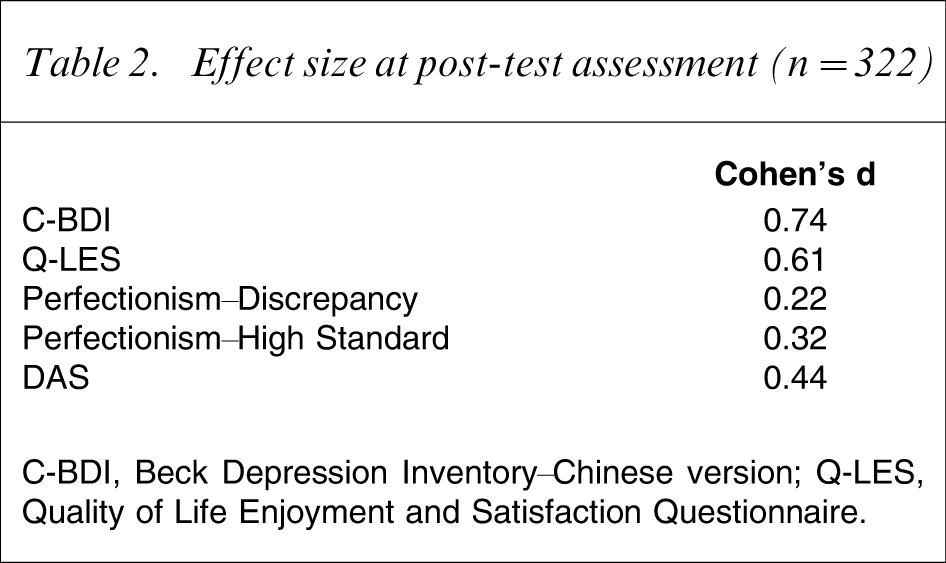
C-BDI, Beck Depression Inventory–Chinese version; Q-LES, Quality of Life Enjoyment and Satisfaction Questionnaire.
Based on the RCI score for the C-BDI for each participant, approximately 45%, 19.7%, and 7.4% of the participants in the experimental group could be considered as clinically improved, remitted and recovered, respectively (Table 3). Hierarchical regression was done to examine the independent effects of perfectionism and DAS at pre-test assessment on C-BDI at post-test assessment; and perfectionism, DAS and C-BDI at pre-test assessment on Q-LES-Q-18 at post-test assessment in the experimental group. The results indicated that perfectionism–discrepancy, perfectionism–high standards and DAS independently, respectively, contributed 6% (B = 0.24, F change = 18.39, p = 0.00), 4% (B = 0.25, F change = 13.65, p = 0.00) and 6% (B = 0.26, F change = 17.95, p = 0.00) of the explained variances in C-BDI among the participants in the experimental group. Also, perfectionism–high standard, DAS and C-BDI, respectively, explained 6% (B = − 0.29, F change = 18.05, p = 0.00), 13% (B = − 0.43, F change = 47.36, p = 0.00) and 12% (B = − 0.37, F change = 49.00, p = 0.00) of the variances in Q-LES-Q-18 among the participants in the experimental group. To conclude, it seems that both DAS and perfectionism are important cognitive variables that significantly predicted C-BDI and Q-LES-Q-18 of the participants in the experimental group.
Improvement in C-BDI at post-test assessment (% test group; n = 163)
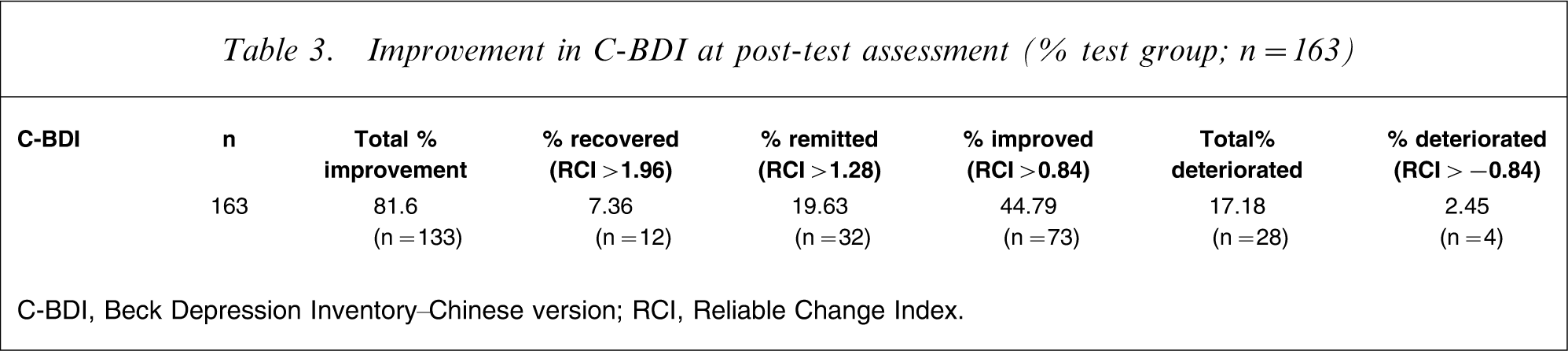
C-BDI, Beck Depression Inventory–Chinese version; RCI, Reliable Change Index.
Discussion
Hypothesis 1 was confirmed, indicating that the participants from the experimental group had a substantial decrease in depressive symptoms, better quality of life, and fewer perfectionist (i.e. high standard) and dysfunctional attitudes, when compared with the members of the control group at the end of treatment. The improvement found in the two outcome variables (depressive symptoms and quality of life) echoes the findings of other studies that suggest that group CBT is effective in treating people with depressive symptoms. It is also impressive that as many as 81.6% of the participants in the experimental group had improvement in depressive symptoms. Indeed, as many as 19.7% and 7.4% of the participants in the experimental group could be considered as clinically remitted or recovered, respectively. The results of this territory-wide project provide stronger support for the efficacy of the present group CBT programme for Chinese people suffering from mild to severe depressive symptoms in Hong Kong. With the increase in the number of people suffering from depression, this type of group CBT can serve as a possible treatment alternative for people with depression in Hong Kong. But the present study did not have follow-up data on the longer-term effect of CBT for depressed Chinese subjects in Hong Kong.
The present study also contributes significantly to the current literature on CBT in two ways. First, there have been very few clinical studies on CBT for Chinese people. The present study represents a major attempt to collect evidence, using a larger scale, territory-wide clinical trial of group CBT for Chinese people in Hong Kong. Second, to the best of the author's knowledge, there are few clinical studies on CBT that have used quality of life as an outcome variable. The inclusion of such a variable in clinical study on CBT for depression is important because, if effective, it provides evidence that CBT is not only effective in reducing symptoms, but that it contributes to the overall improvement in well-being of the individuals concerned. Nonetheless, there is a need to further examine the clinical significance of CBT and how it influences the relationship between symptom reduction and change in the overall well-being of an individual.
The present study also examined whether changes in cognitive variables would be associated with changes in depressive symptoms. The results indicated that the cognitive variables perfectionism (i.e. high standards) and dysfunctional attitudes significantly related to the outcomes in depressive symptoms and quality of life of participants in the experimental group. This result echoes the findings of other studies conducted by Wong; Lamberton and Oei; and DeRubeis et al. that there was a possible significant association between change in dysfunctional attitudes and changes in depressive symptoms and quality of life for people who had undergone cognitive behavioural therapy treatment [8], [46], [47]. Moreover, the present study constitutes initial evidence to support the possible relationship between changes in perfectionist attitudes and changes in depressive symptoms and quality of life, which, until now, has been limited. But researchers such as Jacobsen and Gortner [48] and Oei et al. have raised the argument that cognitive therapy might not be the primary change agent in reducing depressive symptoms and that the reduction in depressive symptoms might have been subsequent to receiving positive reinforcers from the environment [49]. In addition, as Oei et al. suggest, the positive post-therapeutic changes might also have resulted from certain non-specific factors such as the effects of the therapist's communication skills or support from other members if it were delivered in the group format [49]. Indeed, current literature has produced mixed results regarding a causal model of the relationship between cognition and emotion and appears to suggest a bi-directional relationship between the two variables [50]. Thus, further studies are needed to examine the nature of the relationship between changes in cognitive processes and changes in depressive symptoms among Chinese people with mild–severe depressive symptoms.
One therapeutic goal of CBT is to help participants examine and relax their dysfunctional/perfectionist attitudes so that they can place more realistic demands on self and others. Specifically, the present group CBT programme attempted to facilitate participants to acquire an attitude of letting go of certain things that they could not change and to learn to place realistic demand on self and others. During the treatment process a substantial proportion of the group content focused on helping participants identify, challenge and modify their negative automatic thoughts and dysfunctional rules and assumptions. Through these activities, participants might have gained more self-acceptance and might have improved their interpersonal relationships with others. Thus, it is not surprising that a decrease in perfectionism–high standards could bring about a reduction in depressive symptoms and an improvement in quality of life in participants. But the present results did not indicate any significant relationship between changes in perfectionism–discrepancy and changes in quality of life. One possible reason is that, by definition, perfectionism–discrepancy denotes the degree of stress experienced when individual performance consistently does not meet expected standards. Therefore, when a person experiences less stress as a result of positive changes in dysfunctional attitudes, he/she may immediately experience symptom relief (i.e. C-BDI). In contrast, it probably takes a longer time for the changes in perfectionism–discrepancy to exert an effect on quality of life of an individual, because the person needs time and life experience to appreciate how changes in his/her dysfunctional attitudes have impacted on his/her life. Nonetheless, future studies with a larger sample size are needed to clarify the relationship between these variables.
The present study had several major limitations. First, because depression is a recurrent illness, there is a need to examine the longer-term effect of CBT for depressed Chinese people in Hong Kong. This would provide stronger evidence for the efficacy of CBT for Chinese people with depression. Second, the present study cannot rule out the fact that positive changes in the C-BDI, Q-LES-Q-18, perfectionism, and DAS might have been due to group effects such as emotional support and advice provided by others. In order to ascertain the therapeutic value of the cognitive and behavioural skills taught in a group CBT programme, it would be useful to introduce a social group as a comparison group in the study design. Third, the present results might have been complicated by the fact that 65% of the participants were taking medications at the time of the study. As Oei and Dingle have suggested, medication and CBT may interact and function in a circular process to influence the outcomes in depression [50]. Thus, this factor should be taken into consideration when designing the types of comparison groups to be included in future clinical studies. Fourth, in clinical research, one of the aims is to examine if and how process variables influence outcome variables in the treatment process. In reality, however, the relationship between process variables (i.e. perfectionism and dysfunctional attitudes) and outcome variables (i.e. depressive symptoms and quality of life) is complex. Some researchers have suggested an interaction or bidirectional relationship between the two sets of variables [50]. Future clinical research needs to develop different strategies to address this issue. For example, content analysis of the group process can be done to explore how certain cognitive and behavioural strategies have been performed and how these strategies may be related to the therapeutic outcomes. Fifth, the present results could have been inflated because of the positive reaction of the participants in the waitlist control group to being able to enter the group CBT programme after a few months of waiting. Future research using a true randomization can minimize this ‘Dodo bird effect’. Last, because there is a strong stigma against mental illness among Chinese people, those who had participated in this clinical trial might be those who were more open and ready to receive treatments. Thus, the present results might apply only to this sample of depressed Chinese adults in Hong Kong. Indeed, those depressed individuals who are more withdrawn may be more resistant to therapies, and therefore this might affect the outcomes of the CBT treatment.
Conclusion
With the increase in the number of people suffering from depression and the lack of alternative treatments available for people with depression in Hong Kong, the aim of the present territory-wide clinical study was to provide more evidence on the efficacy of group CBT for Chinese people with depressive symptoms. Initial findings suggest that after 10 weeks of treatment, the participants in the present structured group CBT programme had significantly greater improvement in quality of life, and fewer symptoms of depression, dysfunctional rules and perfectionist attitudes compared with the control group. Further analyses suggested that changes in outcomes might be related to changes in cognitive factors in the present study.
Footnotes
Acknowledgements
This project was supported by the Mrs Li Ka Shing Fund of University of Hong Kong. The authors would also like to thank all the frontline social workers who participated in the training and the participants who joined the group CBT programme.