
Abstract
Background
The ‘Assessing Cost-effectiveness (ACE) approach’ to priority setting
Although there is nothing new about the task of making difficult choices in health care, policy-makers are now discussing the issue of priority setting with renewed interest. Three main reasons are given in a growing international literature:
growing evidence that the deployment of current resources is far from optimal [1], [2]; continued growth in health-care expenditure, both in absolute terms and as a percentage of gross domestic product (GDP) [3], [4]; and the wish to avoid ‘government failure’ in resource allocation decisions following government intervention in health care to achieve social justice objectives or to correct for ‘market failure’ [5], [6].
Although the importance and need for priority setting is clearly established, the central question of how priority setting is to be achieved remains contested. There are a variety of approaches and models available, offered from a range of disciplines. There are models offered by behavioural scientists based on achieving consensus; by epidemiologists/clinicians based on needs assessment; by philosophers based on notions of social justice; and of course, there are a variety of approaches offered by economists based on efficiency [7]. An important step in assessing these various approaches is to reflect on the question of what constitutes an ‘ideal’ approach to priority setting.
The logical starting point to address this question is to develop a checklist based on a clearly specified rationale. The literature provides few guidelines that focus on priority setting across multiple interventions (as opposed to evaluation of individual projects) or that take a suitably broad-based approach. Carter [7] advises that a checklist be based on four general considerations:
guidance from a review of economic theory: both applied economic evaluation methods as well as their theoretical foundations in normative economics; lessons from empirical experience with priority setting; guidance from a review of literature on the role of ethics and social justice in priority setting; and reflection on the pragmatic needs of decision-makers, evident from the empirical experience and key issues of setting and context.
A central issue is the extent to which priority setting approaches focus on ‘technical analysis’ or ‘due process’ for their legitimacy. The ‘technical school’ is characterized by a reliance on rational decision rules and the development of technical frameworks in which they are applied. This school has in large part been the preserve of health economists (pursuing the goal of efficiency) and epidemiologists/clinicians (pursuing evidence-based medicine guidelines and/or needs-based equity). In the technical school, decisions are based on applying the correct rules whether efficiency, effectiveness and/or equity focused. Provided one accepts these principles results should give guidance to decision-makers on how services should be ranked.
In contrast, advocates of the ‘due process’ school question the assumption that it is possible to devise ‘rational’ decision rules and see the technical approaches as based on a simplistic view of the health-care system. For the due process school the task is less to refine the technical basis of decision-making than to construct a process that enables proper debate and discussion to occur. This does not mean implicit rationing, but instead a systemwhereby decisions are made explicitly and the reasoning behind specific judgements is clearly explained.
However, the debate between the two schools may be drawn too starkly in the literature. There is no inherent conflict between provision of information on the costs, outcomes and evidence-base for different interventions, and strengthening of the processes for debating that information and arriving at judgements on priorities. The reality is that neither option alone is likely to fulfil the theoretical and practical requirements of an ideal approach to explicit priority setting. Technical methods alone will never be able to deal with the complexity and contested nature of priority setting, but ‘due process’ should ideally use the sort of information on needs, efficacy/effectiveness, efficiency and equity provided by technical approaches. Both elements need to be involved in any approach to priority setting, that is, seeking strong theoretical foundations and empirical validity. The ‘ACE approach’ reflects our endeavours to develop such a joint approach. It involves close attention to technical rigour in its economic and epidemiological analyses, but also seeks to ensure due process by involving stakeholders in a steering committee; it takes into account broader considerations that are less amenable to quantification; and seeks consensus decisions after informed discussion.
On the technical side the ACE method applies the key economic concepts of ‘opportunity cost’, ‘marginal analysis’ and a ‘clear concept of benefit’ [8], [9] using standardized evaluation methods clearly documented in an evaluation protocol. Undertaking the evaluations in this way as part of the priority setting exercise, addresses the reservations expressed by economists [10] about the simplistic use of league tables, where economic studies are assembled from the literature with little regard to differences in methods, context and setting. The key technical features of the ACE approach are:
the rationale for the selection of interventions is clearly explained and consistently applied; the evaluation methods are standardized, documented and open to scrutiny; the setting and context is common to all interventions (i.e. target populations within Australia); Australian data have been used for demography, health system costs, disease incidence/prevalence and the description of ‘current practice’; information is assembled by a multidisciplinary research team, preparing briefing papers to a standardized format agreed by a steering committee with policy-makers, experts and representatives of community organizations as members; a range of results is reported (not just point estimates) reflecting explicitly the uncertainty and sensitivity of cost, outcome and value estimates; and the incremental costs per disability-adjusted life year (DALY) ratios are placed within a broader decisionmaking framework that includes ‘strength of evidence’, ‘equity’, ‘feasibility’ and ‘acceptability’, which we have called ‘second-stage filter’ criteria.
The steering committee in ACE studies has an important role in achieving balance between the technical analyses and achieving due process. On the technical side members contribute in areas of their expertise and discuss issues of method and evidence. On the due process side, members ensure stakeholder interests and views are articulated: assist with ‘value’ judgement aspects of the analysis; assist with sensible interpretation of the technical analysis; and assist in ensuring transparency and appropriate use of relevant data.
‘ACE’ applied to mental health
Previously, the ACE approach has been applied to cancer and heart disease [11], [12] and further studies have commenced on obesity and prevention of noncommunicable disease in general. The choice of mental health reflected a number of considerations. First, mental disorders are the largest contributor to the non-fatal burden of disease in Australia and rank third behind cardiovascular disease and cancer in terms of overall burden of disease [13], [14]. Second, there are efficacious interventions for the main mental disorders [15] but, until now, there was little evidence of their cost-effectiveness under routine Australian health service conditions. The aim of the ACE-Mental Health study was to assess from a health sector perspective, whether there are options for change that could improve the effectiveness and efficiency of Australia's current mental health services by directing available resources toward cost-effective services. The overall methods and results of intervention-specific analyses have been published in a series of papers in this journal [16–23].
In this final paper we present an overview of the results and conclusions from the study. We add one new analytical component by estimating the impact of the recommended options for change on overall expenditure for depression and schizophrenia, which have been the main focus of our analyses. The first step in doing this was to estimate the annual cost of current practice using the same assumptions of health service use, drug costs and adherence as in the cost-effectiveness models for depression and schizophrenia for the baseline year 2000. This ‘bottom-up’ way of assembling total costs based on unit costs for the various elements of an intervention follows usual practice in economic analysis [24]. Thereafter, we estimate the change in annual expenditure that would occur if our major recommendations for a shift toward more cost-effective practice were implemented.
Overview of results
The cost-effectiveness results
The results of the economic evaluations conducted as part of the ACE-Mental Health study can be summarized in a ‘league table’, ranking the interventions in order of their economic merit (18].
The results of the ACE-Mental Health study show that there are cost-effective treatment options for mental disorders that are currently underutilized (e.g. cognitive– behavioural therapy (CBT) for depression and anxiety, bibliotherapy for depression, family interventions for schizophrenia and clozapine for the worst course of schizophrenia). There are also less cost-effective treatments in current practice (e.g. use of olanzapine and risperidone in the treatment of established schizophrenia and, within those atypicals, a preference for olanzapine over risperidone).
Impact on annual expenditure for schizophrenia and depression
We estimate A$119M was spent in 2000 on pharmaceuticals for schizophrenia based on the proportions of people with schizophrenia using different types of neuroleptic drugs from the 1998 Low Prevalence Disorder Study and adjusting for the change in volume of scripts for each drug under the Pharmaceutical Benefits Scheme since 1998. This estimate is close to the A$110M reported by the Australian Institute of Health andWelfare (AIHW) as total expenditure on pharmaceuticals for schizophrenia for the financial year 2000/2001 [25] using a method referred to as ‘top-down’ costing or ‘gross-costing’ [24]. These estimates include costs to government as well as patient contributions.
Changing treatment in those currently on olanzapine to risperidone would result in A$27M cost-saving. Implementation of all our recommended drug treatment strategies [21], that is giving: (i) clozapine to the 15% of patients with the worst course of schizophrenia; (ii) risperidone to those who experience moderate to severe side-effects on typicals; and (iii) low-dose typicals to all others, would cost A$42M or a cost-saving compared to current practice of A$68M with virtually no change in health status. These savings would more than cover the estimated A$36M annual cost of delivering family interventions to the 51% of people with schizophrenia whom we estimated to be eligible and this would lead to an estimated 12% improvement in their health status [22].
We estimate A$153M was spent in 2000 on out-ofhospital medical services (largely general practitioner (GP) and specialist care) and A$190M on pharmaceuticals for depression, taking into account a change in prescribing patterns since 1997 (the year of the National Survey of Mental Health and Wellbeing [26]) as indicated by the change in volume of scripts for each drug under the Pharmaceutical Benefits Scheme. These amounts are considerably lower than the A$276M for out-of-hospital medical services and A$340M for pharmaceuticals AIHW attributed to depression in 2000/2001 [25]. This difference in cost estimates can be explained by two reasons. First, our estimates are based on a crosssectional survey asking respondents about health service use in the last 12 months and a sizeable proportion of respondents identified with depression would not yet have completed their episode. Thus, we underestimate the true costs of health care for depression. Second, it is not easy to apportion total expenditure on antidepressant drugs to individual disorders as they are also widely used for other disorders, such as anxiety disorders, dysthymia and subsyndromal depression not included in our estimates. This would lead to overestimation in the AIHW costs for depression.
Our cost-effectiveness analyses of antidepressant drugs and CBT targeted the 24% of people with depression who seek care from a health professional but do not receive an evidence-based treatment. We estimate that in 2000, these people accrued A$27M out-of-hospital medical costs. Providing them with the same mix of therapy and/or drugs by the same mix of providers as those currently receiving evidence-based care, the annual cost would be at least A$172M based on our low estimate of total costs. This amount would reduce to A$121M if: (i) GPs supervise drug treatment; (ii) psychologists in public service provide CBT; and (iii) prescribed antidepressants were equally split between tricyclic antidepressants and newer drugs such as selective serotonin re-uptake inhibitors (rather than the 36–61% split recorded in 2000–2001 which has become a 81–17% split in 2003/2004). All these estimates are considerably higher than the current expenditure on non-evidence based treatments and would be higher still if we take into account that some of the difference between our total cost estimates and AIHW estimates for depression is because of the fact that we underestimate costs in respondents who had not yet completed treatment at the time ofmeasurement in the cross-sectional survey. Moreover, it is not clear howmuch of current expenditure on non-evidence-based treatment would cease if evidence-based treatment were offered instead.
The total amount of expenditure estimated for funding evidence-based care in just a proportion of people with depression exceeds expenditure on medical and pharmaceutical services for people with schizophrenia because of the much higher prevalence of depression. Although our recommendations for depression are costly, it would result in a 20% reduction in disease burden for treatment of depressive episodes including 6 months continuation of drug treatment after the episode. Providing all those seeking care for their depression in the baseline year 2000 with drug-maintenance treatment following an episode would cost A$312M over 5 years and A$160M if maintenance CBT were offered instead. Both types of maintenance treatment are estimated to reduce the disease burden of depression by approximately 50% [27].
A shift toward our recommended strategy to improve health services for people with depression and schizophrenia is not easy because it relies on: (i) changing the practice of clinicians; (ii) flexibility in financing mental health care between different types of health care and between different health-care funders; and (iii) addressing opinions of patients, carers, health-care workers and advocacy groups about the relative merits of different treatments in an environment influenced by intensive marketing efforts of pharmaceutical companies. We have tried to address these issues by shaping our recommendations in discussion with the steering committee taking into account four ‘second-stage filter’ criteria.
The second-stage filters
To date, ACE steering committees have endorsed the valued judgement that in the health sector, it is appropriate to maximize ‘health’ (defined using DALYs), subject to acceptable performance on other criteria (such as the health gain being fairly distributed). Although there are different techniques for taking such broader considerations into account, steering committees have so far chosen to adopt what we have called the ‘second-stage filter’ process. Under this process the broader considerations are selected, clearly defined and presented as qualifying statements together with the evidence of costeffectiveness for each intervention [18].
Second-stage filter issues in ACE-Mental Health that require attention for each of the interventions are summarized in Table 1. For example, provision of CBT to all eligible patientswith depression and anxiety requires the development of implementation arrangements. Resources would need to be committed to ensuring providers have adequate training and are available in sufficient numbers and this would be a greater challenge in rural and outer metropolitan areas. Also, funding mechanisms for psychological care would need to be extended to ensure equitable access in primary care. For schizophrenia, major issues are the acceptability of the side-effects of typical neuroleptics to various stakeholders and overcoming the inertia in mental health services failing to implement family therapy despite two decades of evidence of efficacy.
Interventions analysed in Assessing Cost-effectiveness – Mental Health: cost-effectiveness and second-filter issues that require attention
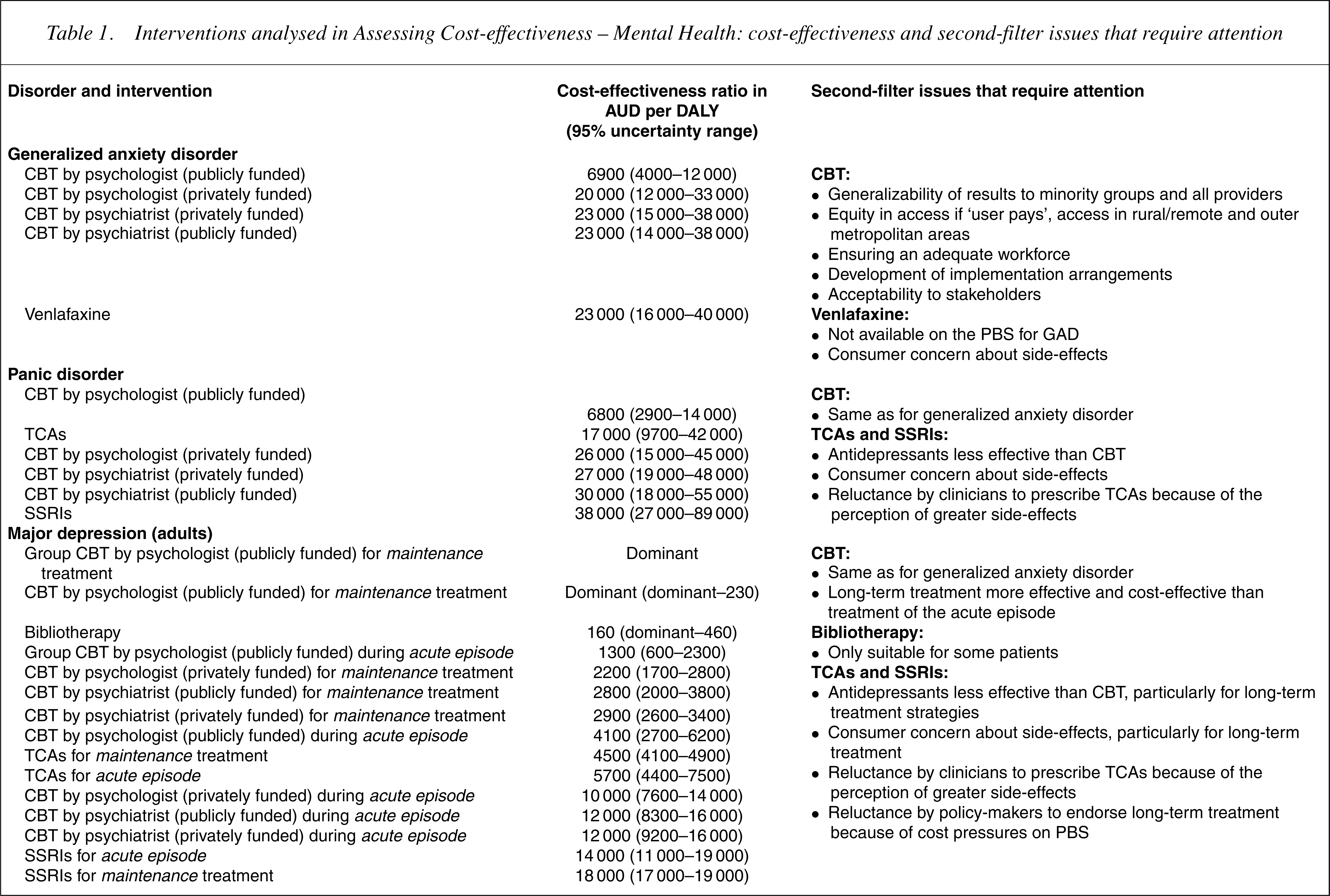
AUD, Australian dollars; CBT, cognitive–behavioural therapy (individual unless otherwise specified); GAD, generalized anxiety disorder; DALY, disability-adjusted life year; NESB, non-English-speaking background; PBS, pharmaceutical benefits scheme; SSRIs, selective serotonin re-uptake inhibitors; TCAs, tricyclic antidepressants.
Selection of the interventions
In addition to the interventions included in 28–30] indicated no clear advantage of either.
Second, integrated treatment for clients with the dual diagnosis of severe mental illness and substance abuse showed a greater availability of evidence at the level of controlled trials, including seven randomized and six non-RCTs, summarized in one systematic review [31] and one narrative review of the literature [32]. However, these studies gave no clear support for integrated programs over standard care because of the lack of differential impact on health-related quality of life.
Third, a review of the evidence for assertive community treatment (ACT) of psychoses including 30 studies, 25 of which were RCTs, found no clear health benefit with ACT nor sufficient evidence to suggest overall health system cost-savings associated with ACT. However, greater satisfaction was reported by clients of ACT and this may make ACT a preferred option as has been reported previously by advocates [33].
Fourth, a cost-comparison analysis was conducted for supported employment in schizophrenia because of the lack of evidence for a clinical benefit [16]. This analysis showed that, largely because of disincentives in welfare legislation to taking up full-time employment, supported employment costs more than it saves from both a patient and government perspective.
Finally, we investigated a stand-alone early psychosis intervention and enhanced standard care for early psychosis versus standard care. The evidence for the effectiveness of the two interventions from a non-RCT was inconclusive, thus preventing a full cost-effectiveness analysis. However, a comparison of average first year costs showed that the two interventions were not significantly more expensive than standard care [34].
Discussion
Despite considerable uncertainty around key input variables, clear distinctions in cost-effectiveness between mental health interventions (particularly within disorders) are apparent. The results suggest that substantial opportunities exist to improve efficiency within our current mental health resources, if resources were shifted toward more cost-effective interventions. We have also identified a significant amount of undertreatment, particularly for depression and anxiety, which would require considerable additional resources but which would lead to sizeable improvements in health outcomes. A previous study found similar order of magnitude findings of the cost-effectiveness of interventions for schizophrenia and depression and drew the same conclusions about the potential for greater efficiency in mental health services [35–37]. Results between the two studies are not directly comparable because of some differences in methods (we use a longer time horizon, include mortality outcomes and have not included hospital costs) and presentation of results (we present cost-effectiveness ratios for individual interventions, while the other study presents the cost-effectiveness of the current and an optimal mix of interventions per disorder). However, the main underlying data sources describing the epidemiology of mental disorders in Australia and the effectiveness of interventions are the same and hence the similarity of results is not surprising.
The brief analysis of the impact of our recommendations for more efficient services for depression and schizophrenia shows the value of combining information on cost-effectiveness with the size of health problems, thus refuting the criticism of some health economists that burden of disease studies are awaste of valuable resources [38–40]. Clearly, the quantification of the potential impact on mental health budgets of implementing change is essential to policy-makers and this requires basic burden of disease information on prevalence, incidence and duration of disease.
However, the cost-effectiveness results of this study need to be considered in the context of the second-stage filter criteria and the limitations of data and methods.
Limitations in the selection of disorders and interventions
The ACE-Mental Health study is limited to interventions for major depression, panic disorder, generalized anxiety disorder, schizophrenia and related conditions and attention deficit hyperactivity disorder (ADHD). Clearly, some important mental disorderswith significant health burden were not included, such as substance use disorders, bipolar disorder, dysthymia, borderline personality disorder, eating disorders, posttraumatic stress disorder, social phobia, obsessive–compulsive disorder and conduct disorder. Although the steering committee expressed interest in these disorders, given the 2-year time-constraint and limited-project budget, it was simply not possible to cover all mental disorders. Preference was given to disorders for which the disease burden was greatest, current practice could be quantified and for which evidence-based interventions could be specified. Thus, the ACE-Mental Health study did not intend to provide a comprehensive strategic plan formental health, but rather to suggest options for directing available resources toward cost-effective services.
Within the disorders included in the study, not all possible interventions were analysed. Important omissions include physical exercise [41] and electroconvulsive treatment [42] for depression, CBT for schizophrenia [43] and benzodiazepines for anxiety disorders.
We failed to complete full analyses for a number of interventions with limited and inconclusive evidence of effectiveness. This raises the point of selection bias in economic analyses toward interventions with a stronger evidence-base and often these include pharmacological and surgical interventions driven by commercial interests.
An important simplification made in the ACE-Mental Health study was to ignore comorbidity with other physical and mental disorders because evidence of efficacy for interventions for comorbid disorders is lacking. Randomized controlled trials often exclude subjects with comorbid conditions and/or do not present the results stratified by comorbidity. This raises doubts about the applicability of trial findings to patients in routine health services as comorbidity between mental disorders is very common.
Limitations in the cost per DALY results
As mentioned in the individual papers, there were limitations in the methods used to calculate the cost per DALY, the most significant being the measurement of health benefits. Although the measurement of the effect size is based on accepted methods [44], [45], the translation into a change in the DALY disability weight required the development of new methods [18]. The absence of an established method of translating effect size into health gain in DALY units is further compounded by the lack of health-related quality of life outcome data from trials and survey data and the availability of only two to four DALY disability weights, which coarsely describe severity for each mental disorder. However, it is important to recognize that the effect size is usually the main driver of the cost-effectiveness ratio and that, within disorders, the method for translating the effect size into a change in the DALY disability weight is the same. Thus, comparisons within disorders have greatest validity, but it is more problematic to compare results between mental disorders. Furthermore, comparison of mental health interventions where health gains are dominated by non-fatal outcomes, with interventions for heart disease and cancer where extension of life dominates health outcomes, are less certain even though the studies have been conducted with comparable methods [12], [46].
Second-stage filters process
The second-stage filter process involved the assessment of issues that either influence the degree of confidence that can be placed in the cost-effectiveness ratios (such as the level of available evidence), or broader issues that need to be taken into account in decision-making about resource allocation (such as equity and acceptability to stakeholders). The second-stage filter process was facilitated by the involvement of policy-makers in the steering committee. This helped ensure that the research was conducted from within a policy context, thus having ‘real-life’ applicability. However, this also challenged specific interests. For example, the recommendation that patients with established schizophrenia be switched to low-dose typicals (rather than olanzapine or risperidone) goes against current practice and was not supported by all members of the steering committee. It would also not be supported by pharmaceutical companies that are gradually withdrawing typicals from the market and continuing to introduce newer and higher cost atypicals. Thus, for some interventions and for some criteria, the steering committee could not reach complete consensus. Where this was an issue, the researchers were guided by the weight of evidence and by the majority view.
A significant limitation of the process was the limited consumer input into the project. The steering committee included a representative from SANE Australia (a community advocacy organization) and a representative from the Mental Health Council but no consumers. Thus the view of consumers is incorporated indirectly only, from data presented in trials on side-effects and dropouts, from consumer perceptions recorded in survey data [26], [47] and from the perception of the mental health experts and representatives from community organizations.
Overall, the cost-effectiveness analyses conducted in the ACE-Mental Health study are all based on level I evidence of efficacy, that is, systematic reviews of all relevant RCTs [48]. The number of patients/trials included for each intervention was good for CBT and drug interventions, but modest for family interventions for schizophrenia. An issue relevant for all intervention trials is the lack of patient-rated quality of life measures. The quality of trials was reasonable, but there are worries about the validity of some of the trial results. This was a particular problem with drug interventions for schizophrenia, which are mostly funded by drug companies and suffer from multiple reporting, which is not always obvious to the reader [49], [50]. A more insidious issue is the use of high-dose levels of the typical comparators, which bias the results to a better outcome for atypicals [51]. Not only does this inflate the apparent benefit of atypicals on extrapyramidal side-effects, but it may also inflate the apparent symptom benefits. In the analysis of the risperidone versus haloperidol RCTs from a Cochrane systematic review [52] and supplemented with a more recent RCT [53], we found an effect size (based predominantly on symptom measures) of 0.35 (95% CI = 0.08–0.62) for trials in which risperidone was compared to 12 mg or greater of haloperidol and a lower, non-significant effect size of 0.13 (95% CI = 0.11–0.36) for trials which used mean haloperidol doses of less than 12 mg. This finding is consistent with that found for atypicals in general in the systematic review by Geddes et al. [54].
In addition to the second-filter criteria of ‘strength of evidence’, ‘equity’, ‘feasibility’ and ‘acceptability’, the steering committee proposed a filter based on ‘severity of the disorder’. Such a criterion would have to apply similarly to all interventions for the same disorder unlike the other second-filter criteria that are intervention-specific. As the greatest validity of comparisons is for intervention options addressing the same disorder, we decided not to incorporate severity as an additional second filter. However, while conventional economic analysis does not accord any weight to the severity of the illness per se, there is evidence [55–58] that people often do wish to give greater priority to treatment of those who are worse off, above and beyond the priority it already has within a cost-effectiveness analysis as captured by the incremental health gain. For example, given the greater disability associated with schizophrenia, policy-makers may decide to accept a higher willingness-to-pay threshold for interventions for schizophrenia. Alternatively, greater weight may be given to minor health gains associated with severe conditions, thus increasing the health benefit associated with any particular effect-size change. In fact, there is evidence to suggest that even when more severely ill patients are clearly receiving less benefit than patients with less severe illnesses, there remains a distinct preference for treating the more severe illnesses [59].
What next?
The results of these cost-effectiveness analyses provide valuable material likely to contribute to future policy deliberations by all service providers in mental health. The recommendations should not be seen as ‘one size fits all’. Not all patients respond to any one treatment and patients (and doctors) have their own preferences for treatment, which will inevitably impact on its effectiveness. For example, some people with depression may prefer antidepressants, while others prefer psychological approaches to treatment. Further, CBT may not be appropriate for all peoplewho prefer psychological therapies. Bibliotherapy (a self-help form of CBT) is also cost-effective and suitable for some patients [23]. Interpersonal therapy may also be an efficacious treatment [60] that may better suit some patients. A combination of antidepressant and psychological therapies may be appropriate for others. Thus, the results of the study should not be seen as prescriptive. However, current practice patterns in mental health services indicate that there are inadequate incentives to promote efficiency. The intention of the ACE-Mental Health project was to raise awareness about these inefficiencies. We realize that presenting these results and recommendations will not automatically translate into changed practice. With our discussion of second-filter criteria we have identified potential barriers to implementing change.
Policy could benefit from a more comprehensive analysis of mental health care including analyses of the efficiency of services for other mental disorders, for prevention and for high-cost services (e.g. hospital care), which we have not included in this study. The value of these analyses will be further enhanced by comparison with interventions in other areas of health if the same methods are used. This would indicate whether there are cost-effectiveness arguments to change the share of total health funding dedicated to mental health services.
Caveat
The ACE-Mental Health project was jointly funded by the Australian Department of Health and Ageing, Mental Health and Suicide Prevention Branch and the Department of Human Services, Mental Health Branch, Victoria, in recognition of the importance of research into the cost-effectiveness of interventions in mental health treatment and care. This work draws upon, but is also limited by, the available research and the assumptions necessary to complete the work.
The results of the analyses provide valuable material likely to contribute to future policy deliberations by all service providers. Conclusions drawn from the economic evaluations should be considered within the context of the second-stage filter process, which qualifies the results taking into account issues of equity, feasibility, strength of evidence and acceptability to stakeholders. This second-stage filter process addresses some of the practical considerations required for changes in actual service practice.
Footnotes
Acknowledgements
Principal investigators for the project are: Theo Vos, Rob Carter and Gavin Andrews. We thank members of the ACE-Mental Health Steering Committee for their input into the project: David Barton, Graham Burrows (Chair), Sue Caleo, Vaughan Carr, Dermot Casey, Joy Easton, William Hart, Helen Herrman, Barbara Hocking, Assen Jablensky, Anthony Jorm, Lyn Littlefield, Patrick McGorry, John McGrath, Paul Morgan, Lorna Payne, Deb Podbury, Kristy Sanderson, Suzy Saw, Bruce Singh, Bruce Tonge, Ruth Vine and Harvey Whiteford. We also thank the other researchers who have worked on the project: Justine Corry, Ruth Rossell, Maturot Chalamat, Marie Donnelly and Louise Heuzenroeder.