
Abstract

While the rate of suicide completion ranges between 10 and 40 per 100.000, the rate of suicide attempts, non-suicidal self-injury (NSSI), and suicide ideation in the general population worldwide is around 1-2.5%, 6%, and 9%, respectively (Klonsky, 2011; Nock et al., 2009; ten Have et al., 2009). Most patients displaying suicide ideation in primary care are referred to mental health services (Gardner et al., 2010). Equally, most self-injurers and suicide attempters contact mental health care services before attempting suicide (Parra Uribe et al., 2013). One might expect that, most patients displaying the most severe suicidal behaviour, completed suicide, would contact specialized mental health care facilities prior to suicide, but this is not true. Indeed, most suicide victims contact non-mental health services (i.e. primary care) prior to completing suicide, but only a minority contact mental health care facilities (Lee et al., 2008; Luoma et al., 2002). With regard to suicidal behaviour, is the world upside down?
Figure 1 displays the % of suicide attempters and completers and the health care service where they most frequently had their last contact before either attempting or completing suicide. Up to 84% of suicide attempters are followed-up in mental health services (Parra Uribe et al., 2013). On the other hand, in one study, only one-third of suicide completers had contacted mental health services the year before completing suicide, while 77% had visited primary care providers (Luoma et al., 2002). More extreme results were described in another study from Taiwan. The authors reported that 83% of individuals who complete suicide had previously contacted non-mental health services, whereas only 22% presented to mental health services the year before their suicide (Lee et al., 2008). Indeed, primary care is the most frequently visited clinical service in the month prior to suicide (Trofimovich et al., 2012), thus giving an opportunity for detection and prevention (Da Cruz et al., 2010). A limitation of our arguments is that they are based on the limited available literature from Western countries. Figure 1 is a composite using data from multiple articles. As far as we know, no single study provides statistics for suicide ideation, suicide gestures, suicide attempts and suicide in a single population. Similarly, these numbers may not be representative of non-Western countries in which suicide may be a somewhat different phenomenon (Blasco-Fontecilla et al., 2012).
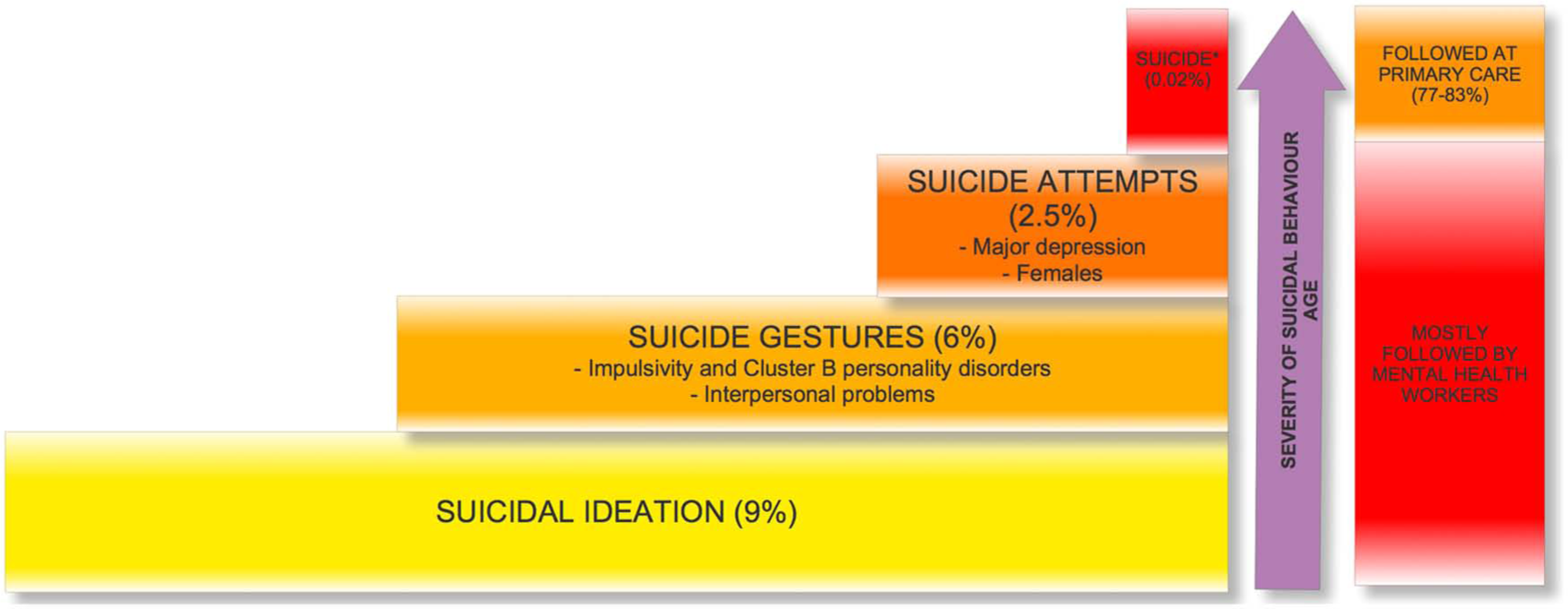
Graphical representation of the different types of suicidal behaviours, and the health setting where the individuals displaying each specific behaviour are followed-up. The graphical representation of rates of suicide completion is not proportional as the prevalence is very low (i.e. 20 suicides per 100,000 or 0.02%). Furthermore, do note that figures represented here are summarizing data from literature, and not data from a single population. Patients who completed suicide are characterized by the presence of somatic disorders, social isolation, alcohol use, narcissistic personality disorder, and male gender.
Suicide attempters and completers are two different, partially overlapping populations (Giner et al., 2013; Parra Uribe et al., 2013), and this may explain the differences in the access to mental health care mentioned above. This is critical, because access to mental health care is inversely correlated with suicide rates across the life span (Mann et al., 2005). Suicide attempters are usually young women diagnosed with personality disorders, particularly borderline, and previous suicide behaviours (Giner et al., 2013). A previous suicide attempt is the most relevant risk factor for subsequent suicidal behaviour, and therefore acts as a warning signal for physicians. Thus, self-injurers and suicide attempters appear to be more easily detected as individuals in need of mental health care by primary care providers, in addition to those detected in emergency departments, and consequently, referred to mental health services. Unfortunately, a prior history of suicide attempts has very limited sensitivity to predict later suicide (Parra Uribe et al., 2013), only between 10 and 14% of suicide attempters eventually complete suicide (Diekstra, 1993), and repeated suicide attempts are concentrated in individuals who attempt but fail to complete suicide (Parra Uribe et al., 2013).
On the other hand, suicide completers are usually middle-aged depressed men with narcissistic traits, and importantly, alcohol use and somatic problems (Giner et al., 2013). Furthermore, most suicide completers have no previous antecedents of suicidal behaviour (Parra Uribe et al., 2013), do succeed in their first or second attempt (Parra Uribe et al., 2013), and do not mention their suicidal ideation or plans (Smith et al., 2013). In this context, it is not surprising that primary care clinicians face difficulties in detecting suicide completers (Nutting et al., 2005). Accordingly, suicide completers are usually not referred to mental health services.
Most studies devoted to prevention of suicidal behaviour are focused on ‘at risk’ populations (Caine, 2013). Suicide prevention programs should not be restricted to preventing the repetition of suicide attempts (Daigle et al., 2011), although they should be included because of their effectiveness in reducing them (Cebrià et al., 2013). Specifically, our results stress the need to better identify patients with suicide risk in the primary care setting. The prevention of suicide could be strengthened at primary care sites by: 1) Improving the detection of suicide completers so that they can be either treated at this setting or referred to specialized mental health services (preventing the predictable). For instance, the creation and use of short, high-sensitivity screening instruments by primary care providers may help in identifying individuals at increased risk for suicide. Moreover, general practitioners (GPs) could improve suicide prevention by expanding the range of patients referred to mental health facilities (i.e. depressed alcoholic males) (Giner et al., 2013). Finally, rather than enhancing primary care GP vigilance to suicide risk in all patients, a more successful strategy would target those mental health patients with a ‘suicide prototype’. 2) Developing and implementing general prevention plans (preventing the unpredictable). Even if primary or mental health care workers are not capable of predicting which patients will complete suicide, they can prevent it. In a recent study, the authors demonstrated that achieving ‘zero suicides’ is feasible in some communities (Hampton, 2010). These authors implemented a prevention plan aimed at providing ‘perfect depression care’. Suicide rates dramatically dropped from 89 suicides per 100,000 individuals to zero from 2000 to 2009. Although these figures are impressive, it remains to be demonstrated that such a preventive program can be extrapolated to other settings and communities worldwide, particularly in developing countries where resources are limited. In conclusion, given that the allocation of the scarce resources available for the prevention of suicide is critical, we believe that suicide detection and prevention strategies should be implemented at primary care settings and mental health services (While et al., 2012). It is time to turn the world upside down.
Footnotes
Acknowledgements
The authors thank Lorraine Maw, MA, for editorial assistance.
Declaration of interest
Hilario Blasco-Fontecilla has received lecture fees from Eli Lilly, AB-Biotics and Shire. The remaining authors report no conflict of interest.
Funding
Paula Artieda-Urrutia has obtained competitive funding from IDIPHIM.