
Abstract
A significant number of studies have explored the relationship between severe mental illness and the conduct of acts of violence [1–3]. However, despite a recognition that psychotic disorders may render individuals vulnerable, there has been considerably less research into the experiences of patients with these disorders as the victims of violence and crime. The few studies that have been conducted to date, have suggested that criminal victimization is higher in patients with mental disorders. For example, Brekke et al. studied a group of 172 patients with schizophrenia or schizoaffective disorder living in a community setting in Los Angeles over a period of 3 years [1]. They found that 38% of the sample had been a victim of crime over that time period and that rate of victimization in regards to violent crime was 14 times that of the rate of being arrested as the perpetrator of a violent crime. A second American study also found an increased rate of victimization in patients with severe mental illness, especially associated with living in an urban setting [2]. A recent report from the UK also found an increased rate of victimization, on this occasion in an inner urban cohort of patients participating in a large trial of models of case management [3]. Although most studies have looked for a variety of potential correlates of victimization, limited research has looked specifically at the relationship between specific symptoms and victimization. Both Walsh et al. [3] and Brekke et al. [1] found a relationship between total symptom scores (on the Brief Psychiatric Rating Scale [1] or the Comprehensive Psychopathological Rating Scale [3]) and victimization, while Walsh et al. did not find a relationship between victimization and negative symptoms (rated with the Scale for the Assessment of Negative Symptoms [SANS]). Hiday et al. found that patients reporting more paranoid symptoms reported greater victimization [4].
Aims
The aim of this study was to explore the relationship between schizophrenia and the experience of victimization in an outer metropolitan urban community sample in Melbourne, Australia. We aimed to document the 1 month prevalence of self reports of violent and nonviolent victimization, to determine correlates of this victimization and to explore the relationship of victimization to specific aspects of psychopathology, especially specific positive symptoms.
Method
Subjects
The sample for the study consisted of 348 patients who were recruited as part of the Schizophrenia Care and Assessment Program (SCAP). The SCAP was a prospective longitudinal observational study of patients with schizophrenia and related disorders conducted at the Dandenong Psychiatry Research Centre in Victoria, Australia between December 1997 and May 2003. The service covers an outer metropolitan region of Melbourne with a relatively low socioeconomic profile and a high degree of racial diversity. Patients included had a diagnosis of schizophrenia, schizoaffective disorder or schizophreniform disorder, were older than 18 years, and had sufficient capacity to communicate with the investigators in simple spoken and written English. Subjects were recruited into the SCAP from two sources: (i) the files of all consecutive admissions to the two acute in-patient units of Dandenong Area Mental Health Service (DAMHS) were screened and patients meeting criteria for the study were approached. Patients regarded as too unwell for inclusion into the study were approached later during the admission. The in patient admissions were typically brief and these patients were not resident in the hospital; and (ii) outpatients and patients receiving case management by the adult community psychiatry services of DAMHS were approached following random selection from case lists. Data for this analysis has been taken from the assessments conducted at baseline study visits.
Measures
The primary dependent variables were subject ratings of victimization. The subjects were asked the following questions taken from the Lehman Quality of Life Interview [5]:
In the past 4 weeks, have you been a victim of any violent crimes such as robbery, mugging, assault, or rape?
In the past 4 weeks, have you been a victim of any non-violent crimes such as burglary, theft of your property or money, or being cheated?
In addition, they were asked to rate how they felt about ‘the protection you have against being robbed or attacked’ on a 7 point Likert scale. For analysis this was collapsed into three ratings, satisfied, non-satisfied and mixed.
A range of other variables were included in the analysis. These included clinical ratings performed during the SCAP including the Positive and Negative Syndrome Scale (PANSS) [6], the Montgomery-Asberg Depression Rating Scale (MADRS) [7] and the Global Assessment of Functioning Scale (GAF) [8]. In addition, all patients completed the SCAP instrument, which is a 100-item self-report instrument designed to measure a broad variety of outcome variables (including the ratings of victimization). This includes a series of subject rated domains of quality of life and functioning, ratings of substance and alcohol misuse and subject reports of injuring or threatening to injure others. Alcohol misuse was rated in the SCAP instrument with the CAGE alcohol use screening instrument [9]. Drug misuse was rated with an adaptation of the CAGE extracted from the Arkansas Schizophrenia Outcomes Module [10]. Domains of subject rated quality of life included in the analysis were ‘social needs’ and ‘basic needs’ which rate satisfaction with social and basic functional aspects of the individual's life circumstances. We also included a single item ‘general life satisfaction’ rating where subjects rate how they ‘feel about life in general’ on a seven point scale. All participants were also rated using the Quality of Life Scale (QLS) [11] and were questioned in regards to illness and demographic characteristics such as illness duration and number of hospitalizations.
Statistical analysis
Statistical analysis was conducted using the Statistical Package for Social Sciences (SPSS 10.0). Chi square and t-tests were initially used to compare the subjects reporting victimization (either violent and/or non-violent) to those not reporting victimization on all potential predictor variables. To determine predictors of victimization, a two-stage logistic regression analysis was performed with reported victimization (yes or no) as the dependent variable. Potential predictors were initially divided into four groups (clinical, clinical symptoms, functioning/quality of life, history of legal or substance abuse problems). Each group was entered into a separate regression model with the variables entered as a single block. Variables found to have a significant relationship with the dependent variable (p < 0.10) were then included in the final model analysis. A separate model was calculated including scores for the seven positive symptom dimensions from the PANSS. There was a small percentage of missing data on a number of variables: where relevant data for these subjects was excluded for specific analyses relating to these variables.
Ethics
The study was described in writing and verbally to all subjects and written consent obtained on a form approved by the Southern Health Care Network Human Research and Ethics Committee.
Results
348 patients participated in the study. Victimization data was available for 347 subjects. Of these, 169 were recruited from the acute inpatient service or had been an inpatient in the 4 weeks prior to recruitment. One hundred and seventy-nine were recruited from community programs and had not had a recent hospital admission. 13.2% of the sample reported being the victim of violent or non-violent crime: 11.2% reported victimization in regards to non-violent crime and 4.3% in regards to violent crime. 23.2% described themselves as being unsatisfied with their protection from being attacked or robbed and 59.2% described themselves as satisfied.
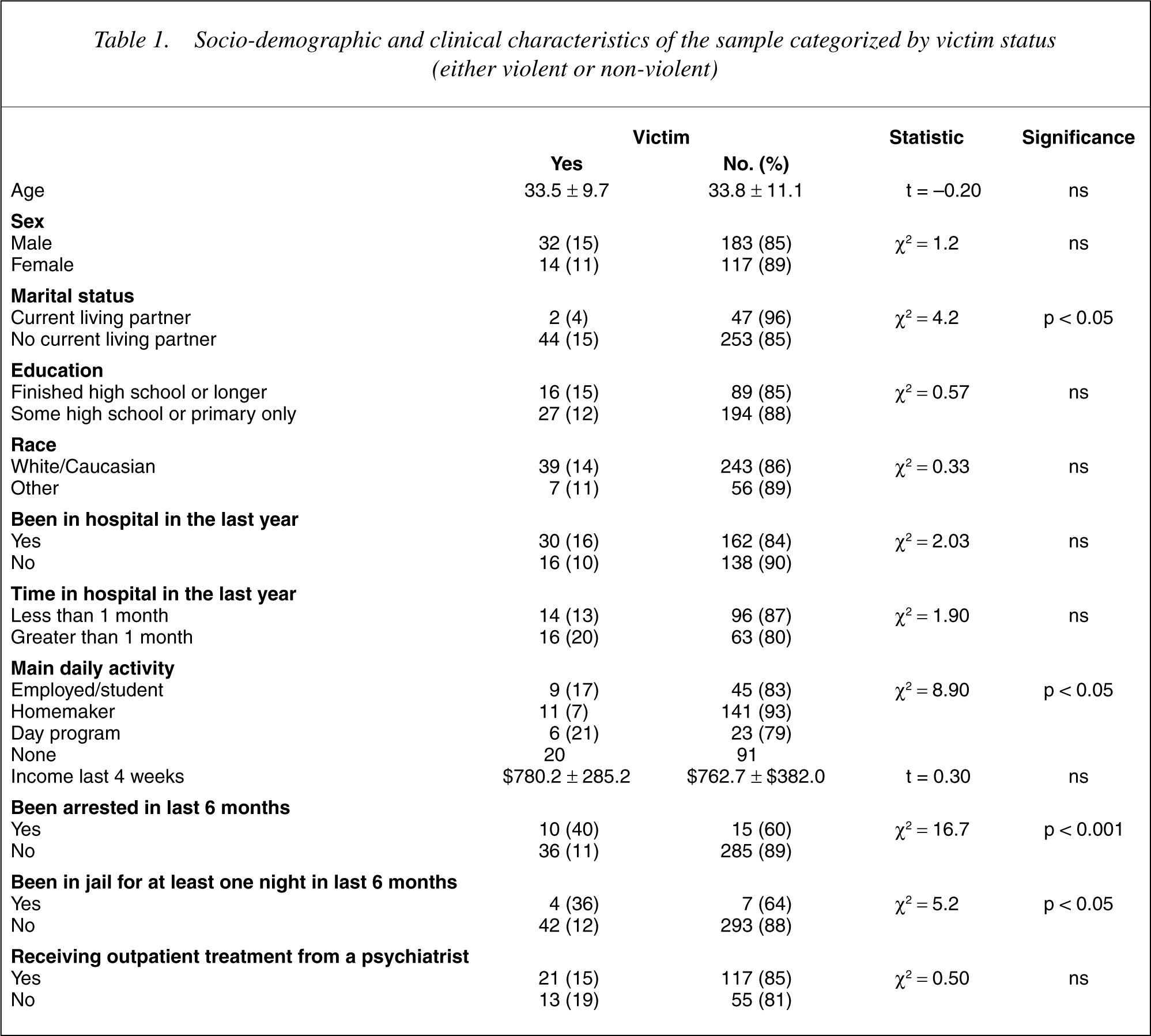
The socio-demographic and clinical characteristics of the sample are presented in Tables 1 and 2. Subjects who reported being victims were more likely to have no living partner/spouse, to report no significant daily activity/occupation and to be more likely to have been arrested and spent at least one night in jail in the last 6 months. They had an earlier age of illness onset and higher scores on the PANSS positive and general symptom scales. They reported lower satisfaction with basic needs of daily life but marginally greater satisfaction with social needs. Seven variables were associated with victimization in the first step of the logistical regression and were entered into the second stage analysis. The final multivariate model from the logistical regression analysis is presented in Table 3. The only significant predictor of victimization was rating of daily activities.
Socio-demographic and clinical characteristics of the sample categorized by victim status (either violent or non-violent)
Clinical characteristics of the sample categorized by victim status (either violent or non-violent)
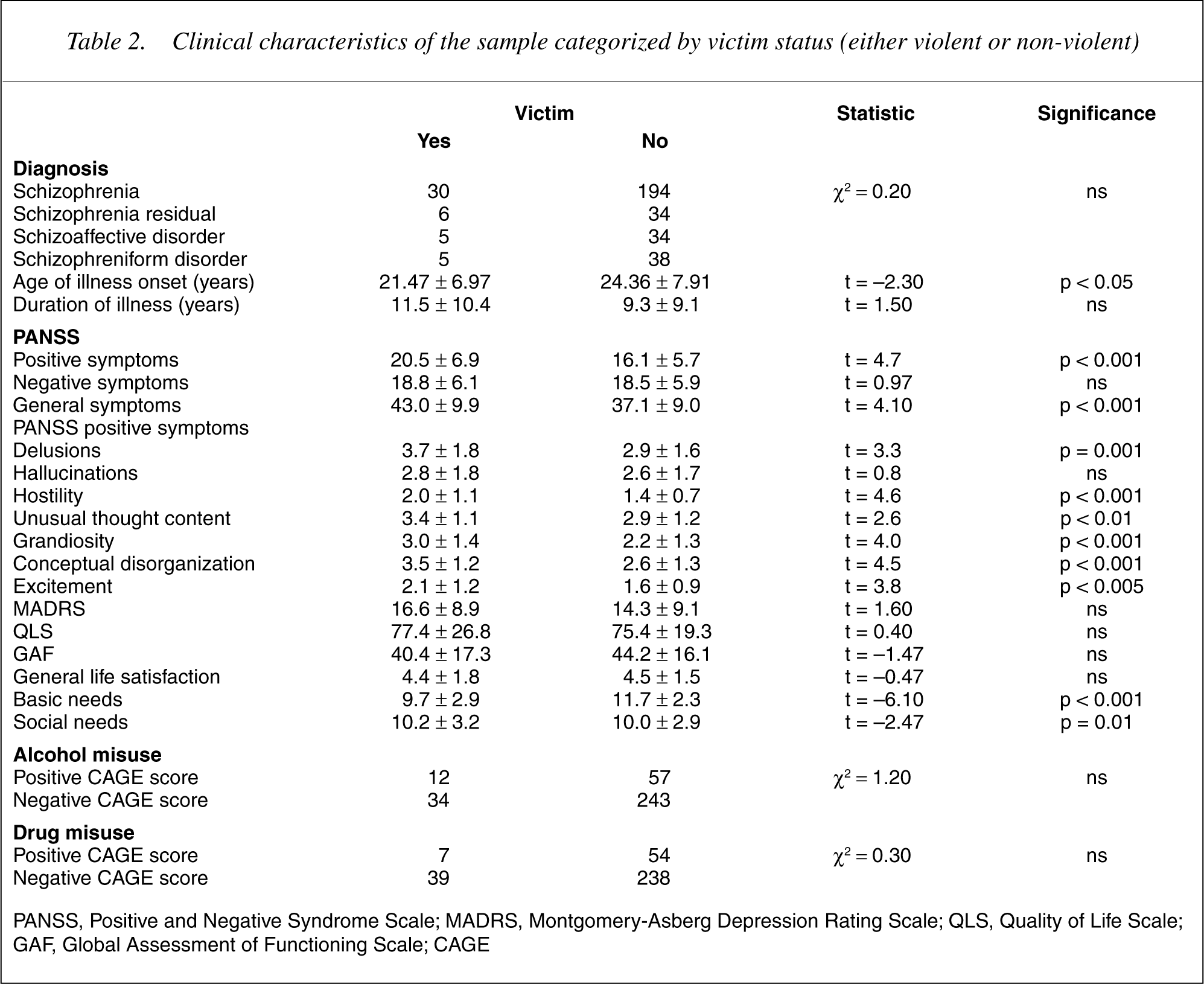
PANSS, Positive and Negative Syndrome Scale; MADRS, Montgomery-Asberg Depression Rating Scale; QLS, Quality of Life Scale; GAF, Global Assessment of Functioning Scale; CAGE
Variables predicting reports of victimization
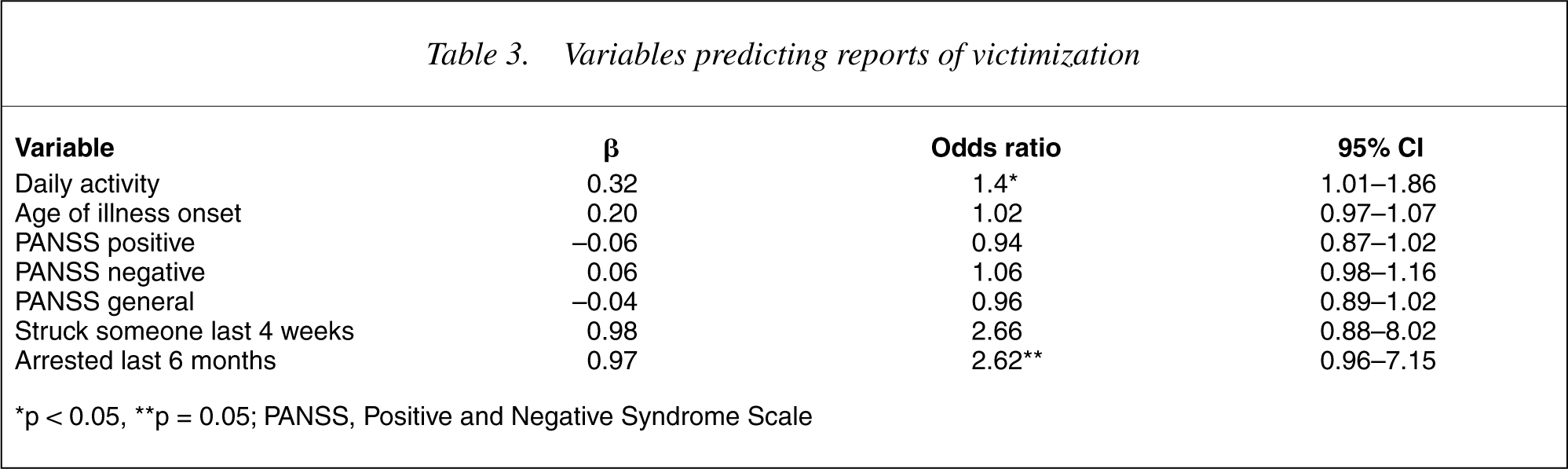
∗p < 0.05, ∗∗p = 0.05; PANSS, Positive and Negative Syndrome Scale
A separate model was calculated including the seven positive symptoms extracted from the PANSS. Although there was a relationship between several symptoms and victimization including delusions, uncooperativeness, hostility and unusual thought content, the odds ratios for each of these symptoms were non-significant in the regression model.
Discussion
Over a 4 week period, 13.2% of the study sample reported being the victim of violent or non-violent crime. Victimization in this study was most clearly related to the subject not having a significant daily activity in which to engage. Although these factors were not significant in the final regression model, the results of the study also suggest that there are relationships between reported victimization and previous involvement by the subject in criminal activity as well as a variety of positive symptoms. The study also found that a large proportion of the sample felt unsatisfied with their protection from significant crime.
The main limitation of this study is the lack of a matched non-psychiatric sample with which to compare victimization rates. The main aim of the study, however, was to gather data that may be compared to previous international reports and to look at the relationship of victimization to other variables within the group. However, we did obtain the relevant Australian Bureau of Statistics data on victimization but the available data was not sufficiently related to the data collected in this study to allow meaningful comparisons. The other main limitation, which this study shares with all previous studies, is its inability to directly address causal relationships and the biases these may produce. For example, in the area of psychopathology, it is possible that increased positive symptoms make individuals with schizophrenia vulnerable to victimization. However, it is also possible that specific symptoms, such as persecutory delusions, could lead to the reporting of events of victimization that have not actually occurred, falsely elevating the rates of reported victimization. Given that it is not uncommon for patients with persecutory symptoms to report being victimized in some way, this is an important bias that has not been addressed in research to date. To address this, studies are required that analyse the relationship between qualitative elements of psychopathology and victimization. On the other hand, it is also possible that there is a substantial under reporting of victimization. The subjects were asked two questions about violent and non-violent crime and were not specifically probed any further.
The reported rates of both violent (4.3%) and nonviolent (11.2%) crime in this study are lower than those in other published reports (see 1] and 16% over 1 year [3]. A high rate (15.2%) was also found over a shorter period (10 weeks) in the study by Silver et al. [12] although it is difficult to compare this to the other research due to the heterogeneity of diagnosis in the sample. All other quoted studies were restricted to patients with psychotic and/or major affective disorders whereas the study of Silver et al. also included patients with substance use and personality disorders. Taking into account the differences in reported rates between the shorter and longer duration studies, it would appear likely that the 1 month rate of 4.2% in our study would translate to comparably high rates of victimization over longer periods of time. It is also of note that the proportion of violent to-non-violent victimization in our sample is quite similar to that in the two studies in North Carolina. They reported rates of 1/2.7 [2] and 1/2.9 [4] whereas the ratio of violent to-non-violent victimization in our sample was 1/2.6.
Rates of victimization in all published studies presented by study duration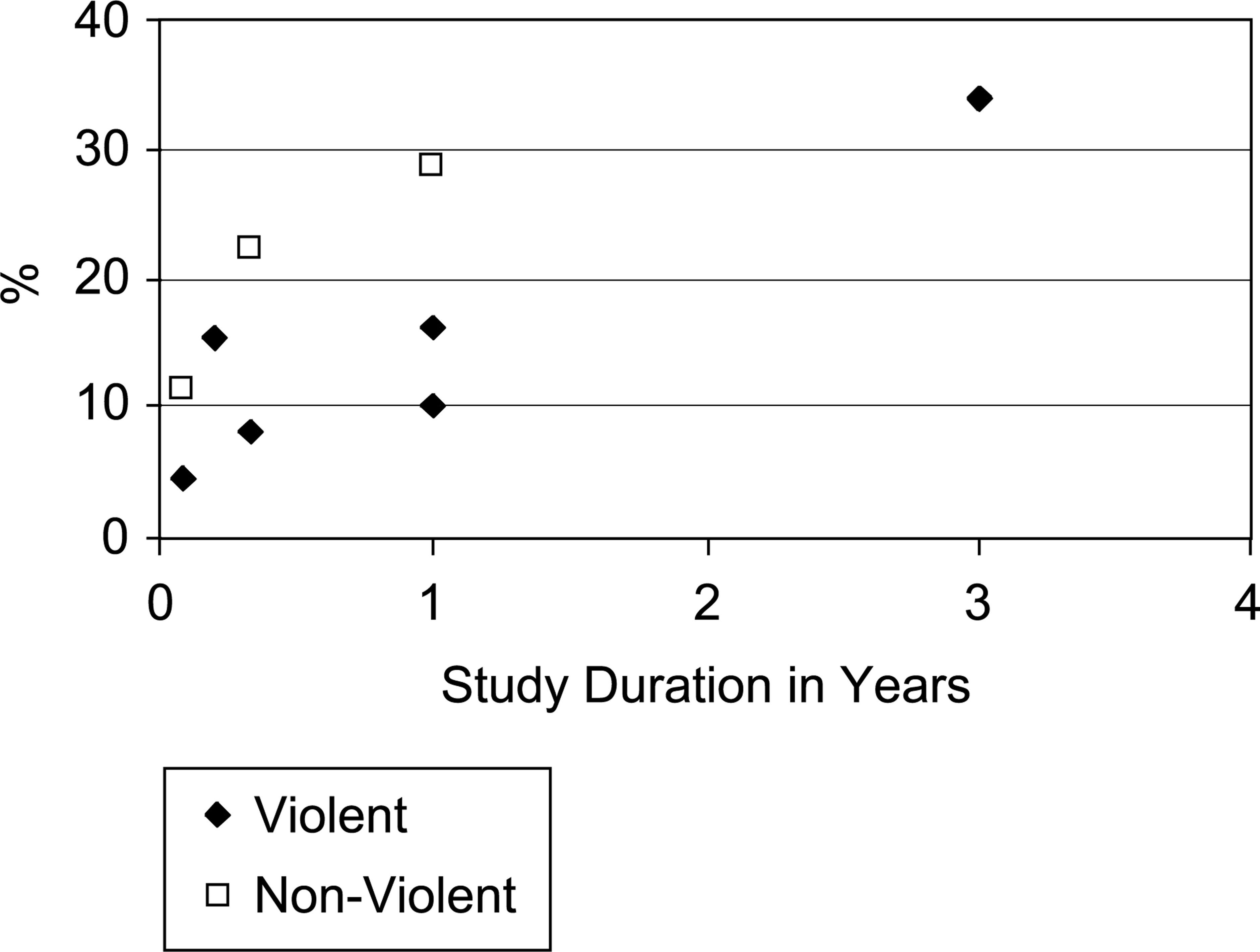
Recent studies of victimization in psychiatric patient samples
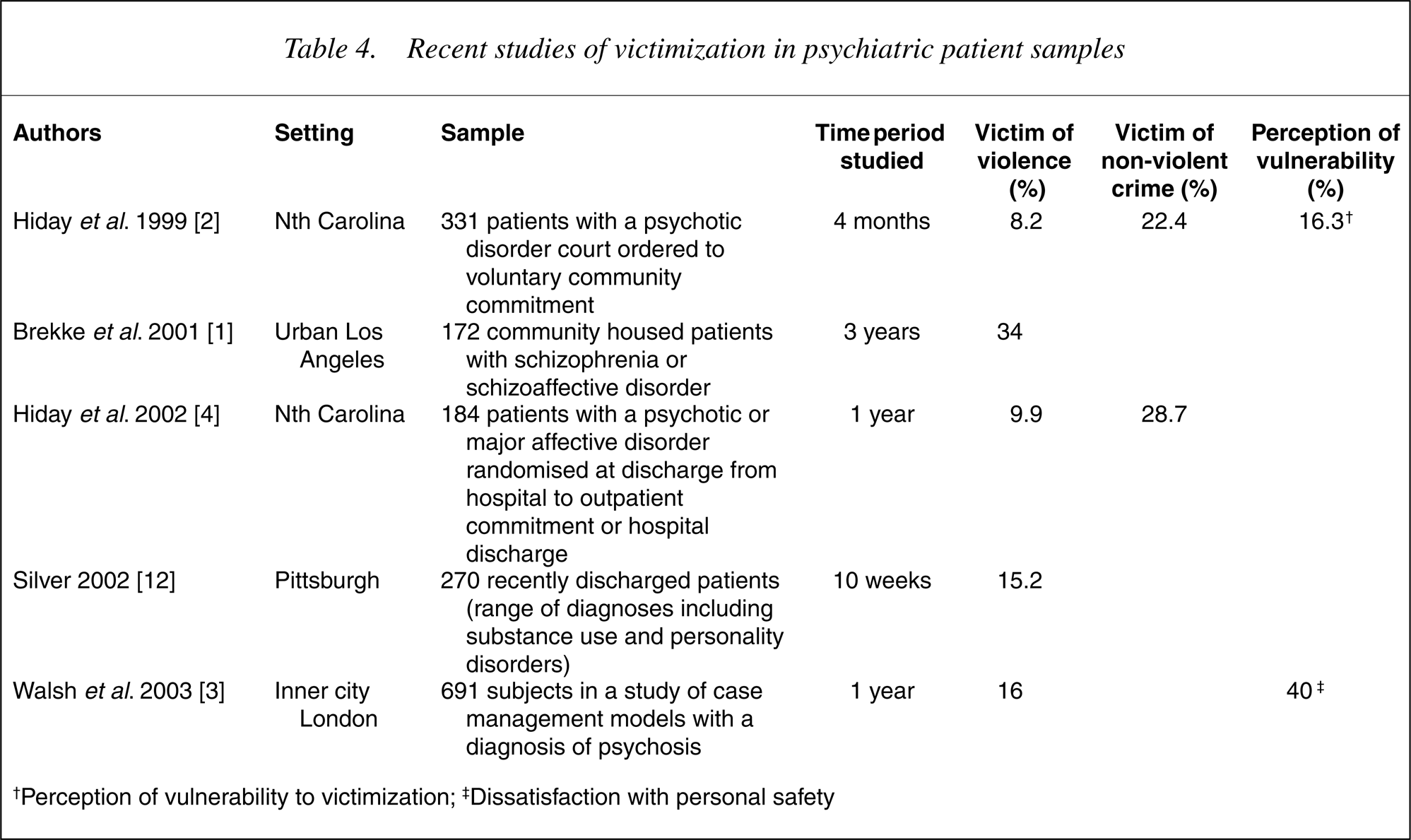
†Perception of vulnerability to victimization; ‡ Dissatisfaction with personal safety
The major predictor of victimization in our sample was the reported daily activity of subjects. In particular, subjects who reported having no substantial daily activity were considerably more likely to report victimization. It is possible that this relates to a high degree of psychosocial disability experienced by patients who are not engaged in meaningful activities. It is also possible that the lack of activities leaves the individuals more exposed to threatening circumstances. This relationship has not been reported in previous studies although this variable does not appear to have been specifically analysed. Other variables that have been reported to relate to victimization include greater psychiatric symptoms [1], [3], homelessness or unstable housing [2], [3] and substance abuse [1–4]. The data in regards to psychiatric symptoms in our study, whilst not significant in the final regression model, would seem to support the relationship between symptoms and victimization. It seems likely that the lower rate of victimization in our sample may have affected the capacity of the multivariate analyses to confirm significant relationships for these variables which were significantly related to victimization in univariate analyses. There was a very low rate of reported homeless in our sample and this was not included as a potential predictive variable. In regards to substance and alcohol misuse, data was collected with the CAGE instrument and although there was not a relationship between alcohol/substance misuse and victimization, this may have been affected by a lack of sensitivity of the instrument applied.
This study confirms that there is a significant rate of victimization reported by patients with psychiatric disorders. These patients appear to be vulnerable to be both violent and non-violent crime. Further research is required, however, to explore the specific nature of the relationship between reported violent and-non-violent events, the nature of patient symptoms and living circumstances. Victimization is an outcome dimension that should be included in the assessment of interventions for this patient group.
Footnotes
Acknowledgements
The authors thank the staff and patients of Dandenong Area Mental Health Service who participated in, or aided in the conduct of, this study. We also thank Bill Montgomery from Eli Lilly for facilitating the project. Eli Lilly, Australia Ltd has provided funding for the study.