
Abstract
A common perception is that persons with severe mental illness (SMI) are liable to commit acts of violence. A number of studies have demonstrated that such individuals may be more prone than the general population to resort to violence [1–4]. Indeed, the legal grounds for involuntary commitment for psychiatric treatment include, among other reasons, the possibility that in individual may harm others [5]. The bulk of the research dealing with SMI and crime has thus focused on these individuals as perpetrators of crime [6]. Less common have been studies indicating that such persons themselves are more likely to be victimized than those without mental illness [7–15]. Hiday et al. noted that violence on the part of a person with SMI may in fact be a response to that individual having been robbed or assaulted in the first place [16]. Studies such as this have all come from the West. To date, however, there have been no published studies of crime victimization in persons with SMI in non-Western countries. We therefore designed this study (i) to provide descriptive data of crime victimization among persons with SMI in Taiwan; and (ii) to identify possible risk factors for such victimization.
Methods
Subjects
Participants were recruited from the Department of Psychiatry, Mackay Memorial Hospital in Taipei. This is a general hospital that includes psychiatric services such as an acute-care ward (54 beds), day-care centre (accommodates 53 patients), outpatient department (7500 persons month−1), suicide prevention centre, and 24 h emergency service. These services are available to the greater metropolitan Taipei population, whose socioeconomic profile is very diverse. In Taiwan, psychiatric services include mental hospitals, general hospitals, and private practices, which are easily accessible and open to all residents. Patients can choose freely among psychiatric providers. Thus, the demographic characteristics of the present sample are likely to be similar to those of patients seen at other such facilities in northern Taiwan. Study inclusion criteria were (i) chart diagnosis indicating the presence of SMI (defined as schizophrenia, schizoaffective disorder, or major affective disorder) for at least 1 year; (ii) age between 12 and 70 years; and (iii) either hospitalization in the acute psychiatric ward or involvement in occupational rehabilitation programmes in the day-care centre within the preceding year (2006–2007). The study protocol was approved by the hospital institutional review board and all participants (or their guardians) gave written informed consent.
Procedure and measures
All participants were interviewed between January and March 2007 using measures modified from the Taiwan Crime Victimization Survey (TCVS), an official survey of approximately 10000 persons conducted by the Ministry of Justice and the National Police Agency in 2000 [17]. The TCVS instrument was based on the National Crime Victimization Survey of the USA (1998) and the British Crime Survey (1996). The questions elicited sociodemographic information; screened for incidents of crime; asked about experiences of crime victimization; and requested self-reporting of delinquent behaviour, living environment, relationship with family, and psychosocial stressors. Because the TCVS was used in the general population, we modified some of the content after discussion with the original author of the instrument. The measures in the present study consisted of three sections: (i) sociodemographic data; (ii) clinical information; (iii) incidents of crime victimization and related information. Prevalence was defined as the percentage of persons victimized among the total number of participants. The victimization rate was defined as the number of incidents of victimization per 1000 persons per year [11, 17].
Sociodemographic data
Information on age, gender, marital status, education, low-income household, mental disability benefit, and occupational status was collected from each respondent. Marital status was recorded either as single or married/cohabitating. The definition of a low-income household was an average monthly salary for each family member of below <NTD10 000 (approx. $USD300). Low-income households receive financial help from the government, reflecting their socioeconomic status in Taiwan. Mental disability benefits are granted when an individual has severe occupational impairment; this measure therefore implies severe impairment in work and daily functioning.
Clinical information
Clinical information extracted from medical records included diagnosis, psychiatric admissions, history of suicide attempts, history of violence, history of alcohol abuse, and history of substance abuse. We reviewed respondents’ medical records and verified the contents with their psychiatrist. The ICD-10-AM symptom checklist for mental disorders [18] was used as a supplementary tool for diagnosis.
Crime victimization
Respondents were asked if they had been victims of certain types of crimes in the previous 12 months. For example, they were asked: ‘During the past 12 months, have you been attacked by anyone? If so, how many times?’ The TCVS inquired about both personal and property crimes. The present study, however, asked only about personal crime, including theft, assault, robbery, mugging or purse snatching, kidnapping, intimidation, rape or sexual assault, fraud, and identity theft. The latter two, fraud and identity theft, are fairly new patterns of crime in Taiwan and had not been included in the TCVS. They were added for the present study after consultation with the original author of the TCVS.
Data collection
The study research assistants were nurses or social workers working in the mental health field, all of whom participated in a standard TCVS training course. The research assistants inspected the medical records of all patients in the acute psychiatric ward and day-care centre to select eligible subjects. All those meeting the inclusion criteria were asked by their charge nurse if they were willing to participate. A research assistant spoke with those who agreed, explaining the aims of the project and asking for signed consent. A face-to-face, structured interview to complete the modified TCVS was then conducted. One author reviewed the hospital discharge diagnosis using the ICD-10 symptom checklist for each participant. If there was any uncertainty about the diagnosis, the participant's psychiatrists were asked to confirm the diagnosis.
Statistical analysis
The sociodemographic data and clinical data were compared between participants who were and who were not victims of crime by using χ2 test or t-test. Those who reported victimization were further divided based on whether they had experienced a single or repeat episodes of victimization, with similar analysis of the data for these two subgroups. The relationship between victimization and each independent sociodemographic and clinical variable was evaluated using logistic regression. All analysis was conducted using SPSS, version 15.0 (SPSS, Chicago, IL, USA).
Results
Sociodemographic and clinical characteristics
A total of 182 individuals who met the study criteria, of whom 27 (14.6%) refused to participate, leaving 155 subjects entered into the study. The mean age was 37.4±11.9 years, ranging from 17 to 66 years. Two-thirds (104, 67.1%) were female. Most had no current partner living with them (120, 77.4%) and no regular job (102, 65.8%), and most lived with their family (143, 92.3%). Only a few of the respondents’ households (19, 12.3%) received low-income benefits from the government. A diagnosis of schizophrenia was more common than of affective disorder (92, 59.4% vs 63, 40.6%). More than half the subjects (94, 60.6%) were involved in the day-care programme. The prevalence of other characteristics varied, including attempted suicide in 51.6% (80), a history of violence toward others (58, 37.4%), alcohol abuse (21, 13.5%) and substance abuse (9, 5.8%). Of the 27 subjects who refused to participate, 16 (59%) were female and 15 (56%) had schizophrenia. These proportions did not differ significantly from the characteristics of those who did participate.
Crime victimization
Twenty-six patients (16.8%, 95% confidence interval (CI) = 10.8–22.7) had been victims of at least one personal crime in the previous year, higher than the annual prevalence (11.3%, 95%CI = 10.7–11.9) of personal crime victimization reported in the TCVS in 2000 (Table 1). Eleven patients (7.1%) were victims of violent crime (assault, robbery, mugging or purse snatching, intimidation, and sexual assault). Just over half (n = 14) had been victimized more than once. Of a total of 82 incidents reported, 39 were violent. The victimization rate was 529 incidents per 1000 persons per year, higher than that found in the general population (208.7 incidents per 1000 persons per year). The rate of victimization involving violent crime was 251.6 incidents per 1000 persons per year, compared with 68.1 in the general population. Assault was the most common type of violent crime, and theft was the most frequent non-violent crime.
Personal crime victimization
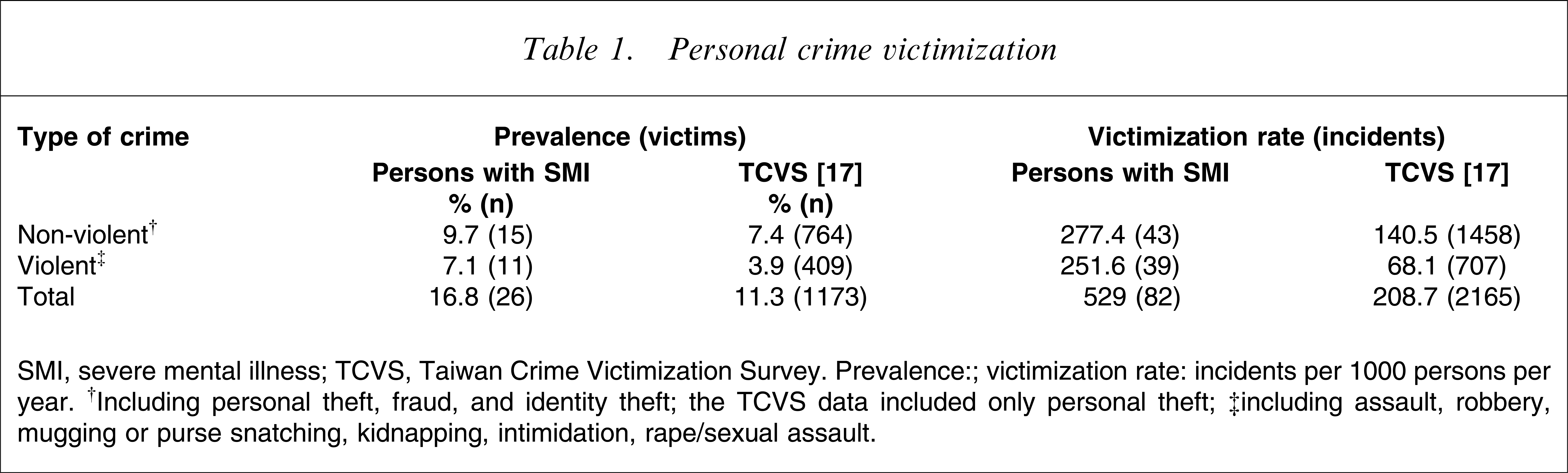
SMI, severe mental illness; TCVS, Taiwan Crime Victimization Survey. Prevalence:; victimization rate: incidents per 1000 persons per year. †Including personal theft, fraud, and identity theft; the TCVS data included only personal theft; ‡including assault, robbery, mugging or purse snatching, kidnapping, intimidation, rape/sexual assault.
Characteristics of victims
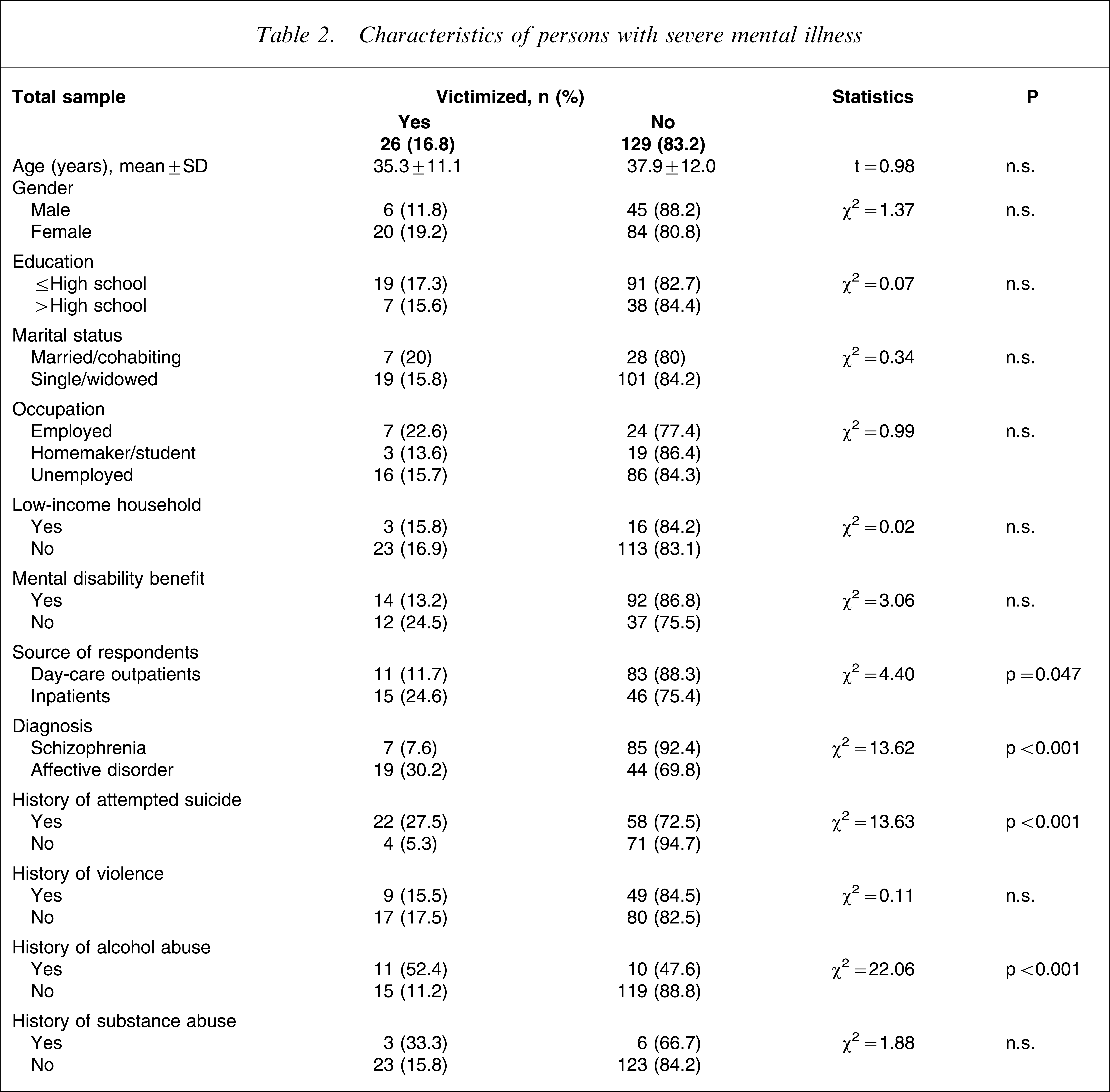
Personal crime victimization was significantly associated with several sociodemographic and clinical variables. Victimization was significantly more likely to be reported by inpatients than by day-care outpatients (15/61, 24.6% vs 11/94, 11.7%; p = 0.047), by those with a history of alcohol abuse (11/21, 52.4%, p < 0.001), by those diagnosed with major affective disorder (19/63, 30.3%, p < 0.001) as opposed to those with schizophrenia (7/92, 7.6%), and by those with a history of attempted suicide (Table 2).
Characteristics of persons with severe mental illness
On multivariate analysis, individuals were at significantly increased risk of being victimized if they had a major affective disorder (odds ratio (OR) = 3.02, 95%CI = 1.08–8.46) or a history of alcohol abuse (OR = 3.96, 95%CI = 1.27–12.36). In this analysis, suicide attempts and being hospitalized were not significant risk factors (Table 3).
Logistic regression of risk factors for personal crime victimization
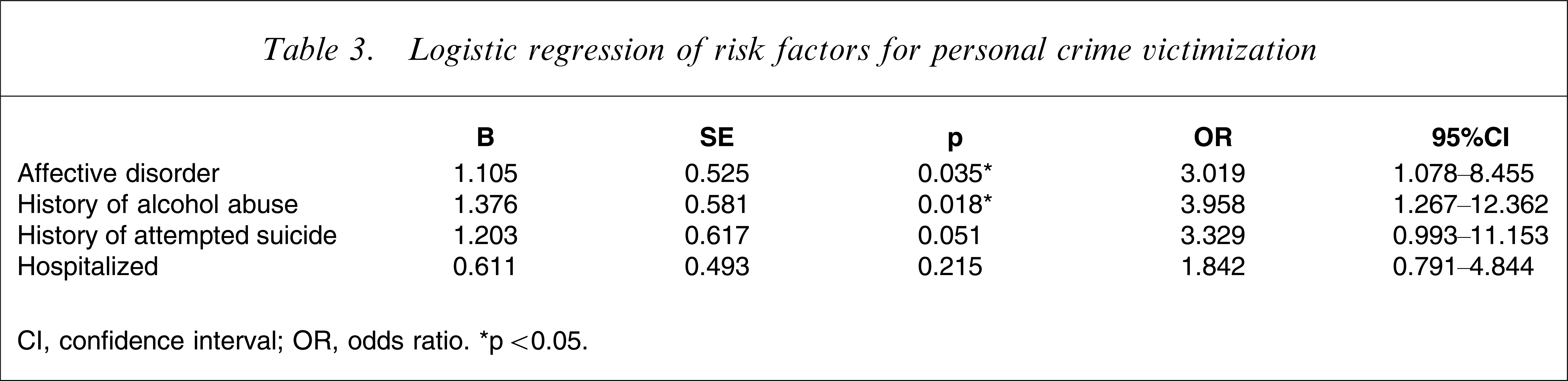
CI, confidence interval; OR, odds ratio. ∗p < 0.05.
Characteristics of repeat victims
The 14 individuals who suffered two or more incidents of crime were compared with the 12 who had experienced only one incident. The only significant difference between these two groups in terms of sociodemographic and clinical characteristics was that patients with major affective disorders were more likely to be repeat victims than were those with schizophrenia (χ2=6.0, df = 1, p = 0.03, Fisher exact test).
Discussion
To our knowledge this is the first study to investigate crime victimization among persons with SMI in an Asian country. The 1 year prevalence was higher than that in the general population, a finding in basic accord with studies from the West. In contrast to those studies, however, we found the risk of crime victimization to be greater for persons with major affective disorders than for those with schizophrenia.
Vulnerability of persons with SMI
Exact numbers from various studies may be difficult to compare because the measures used are sometimes different. We found the 1 year prevalence of crime victimization in persons with SMI in the present sample to be 16.8%, significantly higher than the 11.3% reported in the general Taiwan population [17]. The prevalence involving only violent crime was twice as high in the present sample (7.1% vs 3.9%). The reported overall prevalence of violent victimization in persons with SMI in the West has ranged from 8.2% to 44.1%, consistently higher than in the general population surveyed in those studies [6–15, 19–23]. According to a review by Choe et al., only one study has used the rate of violent victimization as a measure [6]. This was the investigation by Teplin et al., from which we drew the definition of this measure [11]. They found 168.2 incidents of violent victimization per 1000 persons with SMI per year as compared to 39.9 incidents in the general population. In the present study there were 251.6 incidents of violent victimization per 1000 persons with SMI per year compared with 68.1 incidents per 1000 persons per year in the TVCS [17]. This is a nearly fourfold difference, very similar to that reported by the Teplin study. The rate of violent victimization in the present series, however, was higher than in that study (251.6 vs 168.2). Violent victimization was also more common in the TCVS compared to National Crime Victimization Survey (68.1 vs 39.9), which may in part explain the discrepancy between the present results and those of Teplin et al. The fact that more than half the victims in the present study were repeatedly victimized may also contribute to the relatively high rates of violent victimization. Regardless of the particular measure used, it is apparent that SMI increases the risk of crime victimization. This is not particularly surprising, but it would be useful to confirm the observation among other non-Western populations.
Risk of crime victimization in schizophrenia versus affective disorder
Previous studies of victimization among those with SMI have either not compared schizophrenia with affective disorder [11, 14, 16, 19–23] or have found little or no difference in risk regardless of diagnosis [9, 12, 15, 24–26]. One study showed that people with schizophrenia were at higher risk for victimization [13], while several investigators focused only on individuals with schizophrenia [7, 8]. The present findings therefore are in contrast with all these studies in that people with schizophrenia in the present sample were at lower risk than those with affective disorders, both for any history of victimization at all and for repeat victimization. In fact, the overall prevalence among those with schizophrenia (7.6%) was lower even than in the general population as reported in the TCVS (11.3%) [17].
This lower risk among the present subjects with schizophrenia may relate to differences in the way such individuals are dealt with in the West compared with in non-Western societies. Theories of victimization suggest that a crime requires the convergence in time and space of a motivated offender, a suitable target, and the absence of a capable guardian. Further factors include particular vocational and leisure activities, being away from home, especially at night, engaging in public activities while away from home, and associating with people who are likely to be offenders [27–30]. Interestingly, the prognosis overall for schizophrenia appears to be better in developing countries, the extended family system in such societies perhaps conferring a degree of protection not seen in more developed countries [31]. Although there is some debate over the assertion [32], several comparative ethnic studies of schizophrenia in the West have suggested that there are cross-cultural differences in outcome of schizophrenia, with persons with schizophrenia in ethnic minority groups perhaps having a better prognosis than those from majority groups. Collective/sociocentric cultural orientation, interdependence and family integrity may be possible explanations for this observation [33–36]. In the Chinese culture of Taiwan, persons with SMI, particularly those with chronic schizophrenia, usually live with their families. As a result, individuals with schizophrenia often have less social interaction than do those with affective disorders. With less exposure outside the home, the risk of crime victimization is likely to diminish. People with affective disorders, in contrast, often function relatively well in social and occupational situations, so they are more independent than those with schizophrenia. In fact, an acute manic episode in bipolar disorder may actually increase the chance of victimization if the person engages in riskier activities than usual or stays out all night. We believe that these factors may explain the higher prevalence in the present study of personal crime victimization among those with affective disorders and their greater risk for repeated victimization. These societal differences in caring for people with schizophrenia versus those with affective disorders in Taiwan contrast with the situation in the West, where persons with SMI are more likely to live independently in the community, regardless of diagnosis. Those with schizophrenia are therefore less likely to have a capable guardian, and their sometimes obviously disturbed mental functioning may make them appear to be easier targets for criminals.
Another possible reason for the lower prevalence of crime victimization in patients with schizophrenia may relate to cognitive impairment. They may not remember the events that occurred within the study time frame. In addition, they may be less cognizant of what constitutes violation of their personal boundaries, which perhaps also leads to underreporting of crime.
Crime victimization and history of alcohol abuse
In common with previous studies [7, 9, 10, 19, 20, 22, 24], we found that people with SMI who had a history of alcohol abuse were at higher risk of crime victimization. Alcohol abuse among those with SMI may be a form of self-medication or may occur during poor adherence to psychiatric therapy [22]. The influence of alcohol on already disordered mental functioning thus may further increase patient vulnerability, diminishing their ability to fend for themselves and increasing their chance of encountering dangerous situations [7, 9, 24]. Because the present study was cross-sectional, we could not assess the potential contribution of alcohol abuse to particular incidents of criminal victimization. Nevertheless, this observation, across a range of studies of persons with SMI, that a history of alcohol abuse is associated with a higher risk of victimization, suggests that more attention should be paid to this issue. If a cause-and-effect relationship is clearly borne out by studies designed to detect such a relationship, then potential interventions directly addressing this problem should be explored.
Strengths and limitations
By using essentially the same instruments and measures as in the TCVS study, we were able to make a useful comparison between results and reliable national data. Limitations included the relatively small sample size. In addition, because the subjects were drawn only from northern Taiwan, we should view the results with some caution. The cross-sectional study design, as noted here, demonstrates associations but does not allow assertion of direct causal relationships between risk factors and crime victimization.
Conclusions
The present study raises important clinical and research issues to consider. Because crime victimization may exacerbate existing SMI and increase the likelihood of repeat victimization, effective prevention programmes for persons with SMI must be developed and implemented. Mental health service providers should be aware of the risk for crime victimization among persons with SMI, and they should be encouraged to screen their patients for a history of victimization. Having been victimized might exacerbate the underlying mental disorder, and the risk for repeat victimization should be considered, particularly in Taiwan among those with affective disorders. Educating persons with SMI about modifiable risk factors and ways to protect themselves is certainly a reasonable step. Beyond these individual concerns, it is also important to disseminate information about victimization of persons with SMI to policy makers and the public. Police officers, especially, need training about mental illness as well as the provision of crisis assistance when dealing with persons with SMI who have been victimized. An understanding of cultural differences in crime victimization may yield further insight into specific risk factors. The goal of all such efforts is to reduce the burden of crime victimization on individuals with SMI, who are already disadvantaged by their illness.
Footnotes
Acknowledgements
The authors thank the staff and patients of Mackay Memorial Hospital who participated in or aided in the study. We also thank Professor Susyan Jou and Dr Yu-Shu Chen for their insightful comments, and Dr Mary Jeanne Buttrey for English revisions of this manuscript.