
Abstract
The importance of developing partnerships between public and private psychiatric services and between these specialized services and general practitioners has been articulated both in the Second National Mental Health Plan [1] and in the National Standards for Mental Health Services [2], [3]. Despite this well documented ideal, however, significant difficulties still exist in many interactions between these service providers [4]. There is also increasing concern that this less than optimal collaboration may negatively affect outcomes for patients and carers [5], [6]. In 1998, with the aim to improve collaboration between private and public psychiatric services, the Commonwealth Department of Health and Aged Care funded a number of National Demonstration Projects in Integrated Mental Health Services. The purpose of these projects was to trial a number of approaches to improve the linkages between these service providers, allowing patients to receive the help they need from whomever could best provide it. The Public and Private Partnerships in Mental Health (‘Partnership Project’) was the first of these Demonstration projects. It was a joint initiative of St. Vincent's Mental Health Service (Melbourne) (SVMHS), The Melbourne Clinic (TMC), and St. Georges' Aged Psychiatry Service (SGAPS). This 2-year Project started in September 2000 [7].
The Partnership Project aimed to improve the effectiveness of mental health services by fostering co-operation and collaboration between private psychiatrists and public mental health services in and around the SVMHS area. It was fully operational from September 2000 to August 2002. The Project had two major components: a Linkage Unit; and a series of trial item numbers which allowed private psychiatrists to be remunerated for activities other than direct patient contact, for example, case conferencing and supervision (‘expanded roles’) [8]. Both are described in more detail below.
The Linkage Unit was designed to: (i) improve service delivery through collaborative arrangements for individual consumers; and (ii) promote systems-level and cultural change necessary for sustaining collaboration between the public and private sectors. It offered a two-way communication flow enabling each service to access its counterpart. For example, private psychiatrists were able to access public sector services, such as multidisciplinary team input into patients, particularly those with chronic psychotic illnesses. Conversely, the Linkage Unit provided information for SVMHS and SGAPS clinicians seeking a private psychiatrist for a particular patient. It also facilitated linkages between mental health services (both public and private) and general practitioners (GPs) and non-government organizations, and supported formal shared care arrangements between public sector clinicians and private psychiatrists and between public sector clinicians and GPs. It was also responsible for facilitating the expanded roles for private psychiatrists [8]. The expanded roles component of the Partnership Project enabled private psychiatrists who satisfied specified requirements to bill the Project for their participation in activities that did not involve direct patient contact, such as supervision and training for staff from SVMHS, case conferences, and secondary consultations [8].
The Partnership Project served Melbourne's inner urban east, a region characterized by both high and low income areas. There are many private psychiatrists practising within the region and a large inpatient private psychiatric hospital, TMC, is within its borders. Thus there is no shortage of private psychiatrists within and near the SVMHS and its outpatient clinics. However, despite the recognition that some patients in the private sector would benefit from public sector input and vice versa, the degree of interaction between the two sectors has traditionally been low. For example, in 1999 only 17 of 345 case managed patients had any input from a private psychiatrist [9]. Hence one of the main goals of the Project was to increase the number of ‘collaborative’ or ‘shared care’ arrangements between private and public psychiatric services. These refer to situations in which a patient is managed by a private psychiatrist in conjunction with a multidisciplinary team at a public mental health service. This arrangement could be short or long-term and may include crisis management.
After the first 6 months, the Project team found that though shared care arrangements had increased, from about 17 to about 35 (although these numbers are approximate as not all shared care arrangements were recorded) numbers remained disappointingly low. Consequently the team decided to investigate the barriers to private psychiatrists and public mental health staff forming shared care arrangements for their patients. A particular potential barrier that we wished to investigate was the perception that the population of patients managed by public psychiatric services is different from that managed by most private psychiatrists. Information from focus groups and informal discussions with colleagues in both sectors, as well as the Project Team's clinical experience, led us to hypothesize that the public system tends to mange people with psychotic illnesses, particularly chronic schizophrenia, whereas the private system tends to mainly manage patients with nonpsychotic disorders. If this were the case, then one possible barrier to shared care arrangements would be that the public sector clinicians may not feel it appropriate to refer their patients with schizophrenia to a private psychiatrist, and a private psychiatrist may not feel able to effectively manage such a patient. In addition, the inability in Victoria, and indeed in most Australian states, for patients to be involuntarily admitted to private psychiatric hospitals may deter clinicians from both sectors from making collaborative arrangements.
In order to investigate the extent of collaboration between the sectors and to investigate possible barriers to such arrangements, a survey of both public mental health clinicians (psychiatrists, medical officers, and multidisciplinary team members) and private psychiatrists was undertaken. Private psychiatrists accredited with TMC and the public mental health staff at SVMHS were administered questionnaires to examine the attitudes of people within each sector towards each other, the barriers they identified to working effectively together and any possible solutions to these barriers. This paper reports the findings of this survey.
Aims
1. To assess attitudes of private psychiatrists and public sector mental health clinicians to working together in collaborative service arrangements (‘shared care’).
2. To determine which factors present barriers to effective collaborative service arrangements.
3. To establish broadly what type of patients are managed in the private and public sectors.
4. To investigate private psychiatrists' perceptions of and attitudes towards public psychiatry and the perceptions of public clinicians to private psychiatry.
5. To examine suggestions for improving the working relationship between the public and private sector and strategies for breaking down perceived barriers to effective collaboration.
It was hypothesized first, that barriers exist which impede effective shared care arrangements between private psychiatrists and public mental health services and second, that one possible reason for this is that there is a perception that public and private psychiatric services manage different patient populations.
Method
A survey investigating attitudes and perceived barriers to ‘shared care’ was devised and distributed to all clinical staff at SVMHS and to all psychiatrists accredited at TMC.
Setting
SVMHS is a public area mental health service with a comprehensive range of community based and inpatient services. It provides mental health services to adults (16–64 years) who live in the inner urban east area of metropolitan Melbourne and experience mental illness and associated disability. The total sector population is approximately 227 000. The catchment area has a mixture of low and high-income households, as well as a high subpopulation of disadvantaged people, such as people who are homeless, itinerant, residents of public housing and from non-English speaking backgrounds. At the time of the survey there were 154 clinical staff members at SVMHS, working in inpatients, the Community Assessment Team (CAT) (able to provide rapid crisis management as well as home based care), case management (community outpatients), Mobile Support Team (MST) (providing intensive case management) and a community care (rehabilitation) unit.
The Melbourne Clinic is located within the SVMHS catchment area. It is a 108 bed psychiatric hospital which provides a range of general and specialist psychiatric services and includes colocated private consulting suites for outpatient management. It has 194 accredited private psychiatrists as well as day programs and outreach services. TMC also includes an academic unit with a full time Professor of Psychiatry, part time Senior lecturers and a research team.
Instruments
Two self-report surveys were developed, one for public sector clinicians and one for private psychiatrists, with similar questions about attitudes to public/private psychiatric services. A definition of ‘shared care’ was included in the surveys describing the management of a patient by both a private psychiatrist and a member of the public mental health team, usually a case manager, where both clinicians are jointly responsible for the patient's treatment.
Support for shared care was measured on a 1–10 Likert scale. A list of possible barriers to working collaboratively with clinicians in the other sector was developed based on a series of exploratory interviews with private psychiatrists, public psychiatrists and other clinicians in the public mental health system by Pirkis et al. [10]. The lists were slightly modified for public and private clinicians, for example the public clinicians were asked if they felt like they were ‘being used as a backstop’ by private psychiatrists, while private psychiatrists were given the opportunity to endorse the option ‘Patients from the public system are unreliable at keeping appointments and/or paying accounts’ and ‘Access to the public system is difficult’. Also, as cost and access to outpatient private psychiatric treatment were specifically inquired about in the survey of SVMHS clinicians, these 2 options were omitted from the public clinicians' list of possible barriers. However, the majority of survey questions were identical, namely: ‘Difficulty communicating’, ‘Confusion of roles and responsibilities’, ‘Different treatment approach’, ‘Public clinician/private psychiatrist perspective not respected’, ‘Loss of control of patients treatment’, ‘Creates more work than it's worth’, ‘Feeling that patient may be abandoned’. This list was included in the survey and respondents asked to endorse those with which they agreed.
Procedure
Surveys were distributed to all clinical staff at SVMHS (including psychiatrists, psychiatry trainees and medical officers, psychologists, nursing staff, social workers and occupational therapists) (n = 154), and to all psychiatrists accredited at TMC (n = 194) in July and August 2001, respectively. Surveys were anonymous, and a separate tear-off slip was included to keep track of respondents. Surveys were distributed in person and by mail. Reminder letters and duplicate questionnaires were distributed to those who failed to respond after 2 weeks.
Results
Response rate
One hundred and five of the 154 (68.2%) public sector clinicians (psychiatrists, psychiatric trainees, medical officers, psychologists, social workers, occupational therapists and nurses) and 103 of the 194 (53.1%) private psychiatrists returned surveys. It was not possible to compare survey respondents with non-respondents in terms of age, gender or other demographic features as this data was not available for non-respondents.
Public clinicians' contact with private psychiatrists
Public mental health clinicians estimated the percentage of their total patient caseload that they had discussed the option of outpatient private psychiatric treatment with (21.3%), referred to a private psychiatrist (11.1%) or had in a shared care arrangement with a private psychiatrist in the last 12 months (3.7%).
Private psychiatrists' contact with public mental health clinicians
Private psychiatrists estimated the number of patients they had in shared care arrangements with public sector psychiatric services (mean: 7.23, median 5 per psychiatrist) and the number of patients they had referred for public psychiatric management (mean 2.64, median 1) in the last 12 months.
Support for shared care arrangements
All those surveyed generally supported the concept of shared care arrangements. There was no significant difference between public mental health clinicians (mean supportiveness = 6.9 out of a possible score of 10, SD = 2.44) and private psychiatrists (mean = 6.7, SD 2.65). However, public sector medical staff (psychiatrists, psychiatric registrars and medical officers) (mean 8.3, SD = 1.49) were significantly more supportive of shared care arrangements than public sector non-medical staff (mean 6.7, SD = 2.5, 2 tailed t-test, p = 0.002), and all private psychiatrists (mean = 6.7, SD = 2.65, p = 0.002). Psychiatrists working exclusively in private practice were the least supportive of shared care arrangements (mean = 6.2, SD = 2.69 p = 0.005).
Level of support for shared care arrangements by the public mental health clinicians (including medical staff) was then further analysed according to the nature of their work. CAT workers were the most supportive (mean Likert scale score of 7.71), followed by case mangers (7.10), inpatient staff (6.74) and MST staff (5.60). However, these differences were not statistically significant.
Private psychiatrists' support for shared care arrangements was analysed according to age (dichotomized into 50 and below and over 50) and gender. Females aged 50 and under were the least supportive, whilst males in the same age range were the most supportive, however, these differences were not significant.
Private psychiatrists' level of support according to length of time working in the mental health field (including training), and in private psychiatry was analysed. The correlations between supportiveness and years in mental health and years in private psychiatry only were −0.18 (p = 0.07) and −0.14 (p = 0.18), respectively. Thus neither is significant, but there is a trend to significance for years in mental health. As expected, years in mental health and years in private psychiatry are highly correlated (0.85) and for both the tendency is for increased years to be associated with lower supportiveness.
Possible barriers to successful shared care
Cost of private psychiatric treatment
Public mental health clinicians were asked to estimate the total outof pocket expense per visit to a private psychiatrist. It was hypothesized that perceived cost of outpatient private psychiatric treatment was a potential barrier to discussing and arranging this treatment for patients. As clinicians were asked to tick a response it is not possible to calculate a mean estimated cost per visit. Most clinicians (50.5%) estimated between $15.00 and $49.00, with a sizable proportion (24.8%) estimating an out of pocket expense of between $50.00 and $80.00. The differences between the mean supportiveness scores is not significant (F = 1.05, df = 4.95, p = 0.39) although the 10 who estimated the cost to be over $80 were on average the least supportive.
Access to private psychiatrists
Public mental health clinicians were asked to estimate the average waiting period to see a private psychiatrist. Again a tick-box response format was used and so average waiting time per se is not able to be calculated. Most clinicians (50.5%) estimated between 8 days to less than 1 month, with 27.6% estimating between 1 and 2 months. The differences between the mean supportiveness scores was not significant (F = 0.96, df = 4.95, p = 0.43).
Other barriers
Table 1 shows the responses to the barriers identified in the survey instrument. It is noteworthy that very similar endorsement rates were found for many of the items, and barriers were placed in roughly the same rank order by both private and public clinicians. For example, ‘Difficulty communicating’ was identified as a barrier by 75 (71.4%) public clinicians and 74 (72%) private psychiatrists, ‘Confusion of roles and responsibilities’ was endorsed by 66 (62.9%) public clinicians and 68 (66%) private psychiatrists, and ‘Different treatment approach’ by 50 (47.6%) public clinicians and 47 (45.6%) private psychiatrists. Over 60% of private psychiatrists identified problems with access to the public system as a barrier to successful shared care arrangements.
Additional barriers to ‘shared care’ reported by private psychiatrists (some suggested more than one)
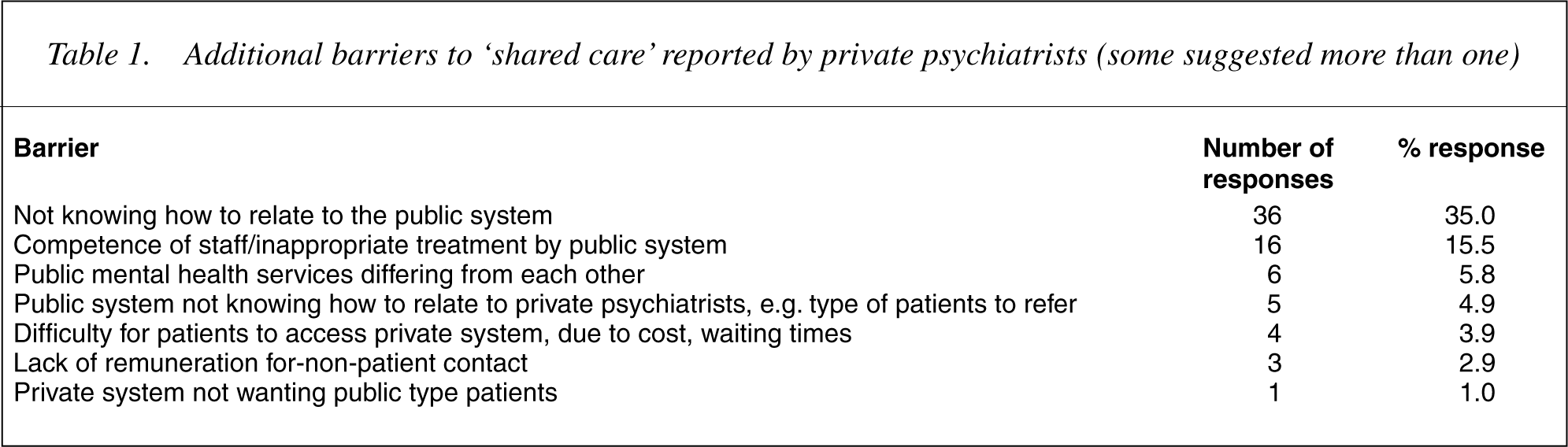
Thirty-eight (36.9%) private psychiatrists suggested other barriers to successful shared care arrangements (see Table 1).
Different patient populations
To test the hypothesis that perceived different patient populations are managed by the different sectors, we asked public mental health clinicians and private psychiatrists to nominate 3–5 areas (diagnostic groupings) in which they felt they had expertise. We also asked them to nominate 3–5 areas in which they felt the other sector had expertise in order to compare self-perceived areas of expertise with the perception of the other sector. Results are shown in Table 2.
Perceived areas of expertise by broad diagnostic groupings
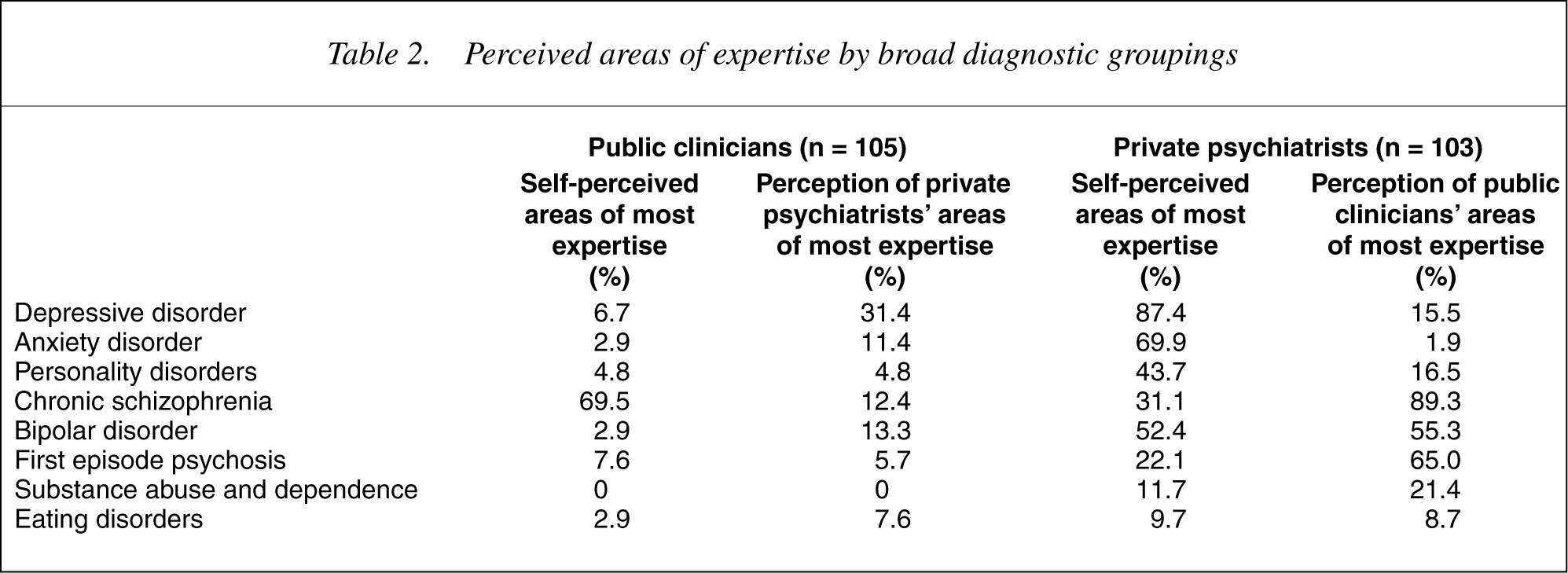
As can be seen, the two sectors differ markedly in what they perceive to be their own areas of expertise. Public mental health clinicians overwhelming endorsed the category ‘chronic schizophrenia’ as their area of expertise. No other broad diagnostic or clinical area was endorsed by more than 8% of respondents, the next highest area being first episode psychosis (7.6%) followed by depressive disorders (6.7%). Only 2.9% of respondents thought they had expertise in managing patients with bipolar disorder. In contrast, private psychiatrists had a broader range of patient types they felt they had some expertise in managing. Most (87.4%) felt they had expertise in managing depressed patients, followed by patients with anxiety disorders (69.9%), bipolar disorders (52.4%), personality disorders (43.7), and first episode psychosis (22.1%).
Private psychiatrists agreed with public sector clinicians that chronic schizophrenia was an area of expertise within the public sector. However, private psychiatrists also thought that public clinicians had expertise in managing patients with bipolar disorder (55.3%) and first episode psychosis (65%). In fact they perceived that public clinicians have a wider range of expertise than the public clinicians perceive themselves.
Public mental health clinicians gave a broad range of responses to the question of perceived expertise of private psychiatrists suggesting little knowledge of the practice of private sector psychiatry.
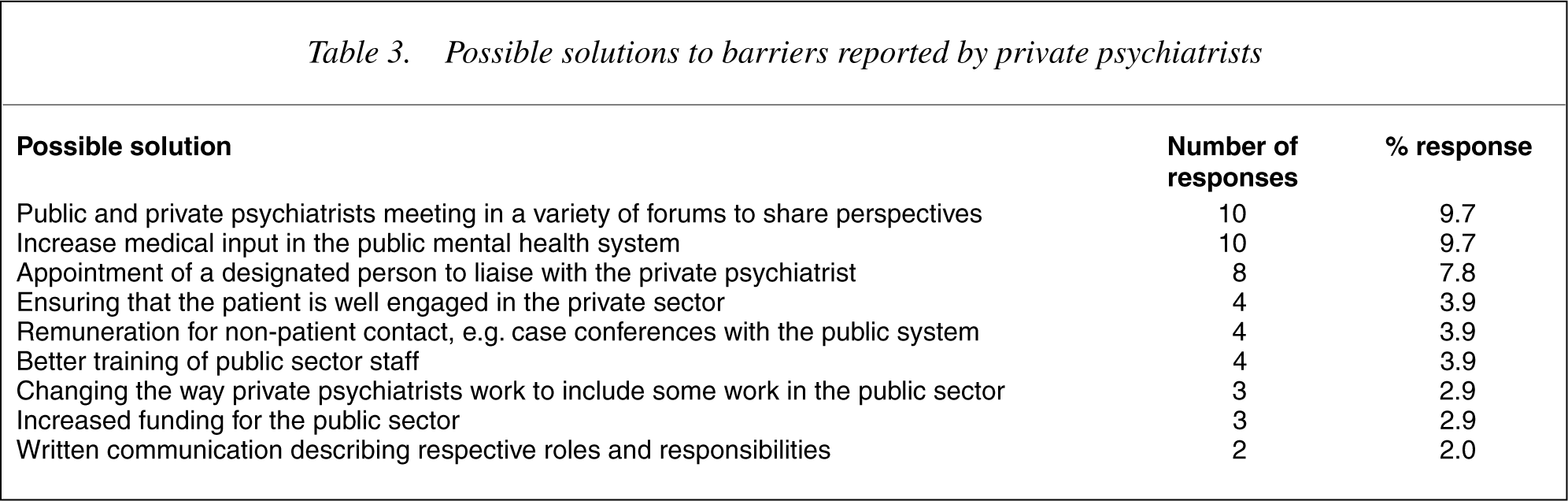
Possible solutions to barriers to shared care
A number of strategies were proposed to enhance collaboration between the sectors in patient management (Table 3). Enhanced communication between the sectors was a major theme, including suggestions that public and private psychiatrists should meet in a variety of forums to share perspectives, the appointment of a designated person to liaise with the private psychiatrist and written communication describing respective roles and responsibilities of the different sectors.
Possible solutions to barriers reported by private psychiatrists
Discussion
Developing ‘partnerships’ between service providers in order to optimize treatment of psychiatric patients is one of the key planks in the Australian Second National Mental Health Plan [1]. Our experience in the Partnerships Project and the results of this survey indicate that building partnerships is a complex task. Cultural differences appear to be present between the public and private sectors and a number of barriers to working together have been identified.
There have been major changes in the structure and function of the public mental health system during the last decade in Victoria. ‘Mainstreaming’ of general hospital psychiatric units has resulted in a shift in the patient mix within these units so that apparently many more patients with chronic psychotic disorders and fewer patients with non-psychotic disorders are treated by them. This is reflected in our results, which indicate that the public sector clinicians perceive themselves to have a narrow focus of expertise, that is, chronic schizophrenia. Private psychiatrists report a broader range of perceived expertise, but with a trend towards greater expertise in non-psychotic disorders.
The ‘case management’ system in which non-medical clinicians have a key role in the day to day treatment of psychiatric patients was also introduced into the public system over the past 10 years. The development of Crisis or Community Assessment Teams, which perform initial assessments, make decisions about suitability of admission for patients and provide home based treatment, also resulted in non-medical clinicians having more clinical input and responsibility in patient management. It is possible that many psychiatrists who trained in the era prior to these changes now have great difficulty relating to a system of which they have little knowledge. The results of this survey support this theory. For example, private psychiatrists who have worked in mental health the longest and those with no joint public sector appointment tended to be the least supportive of collaborating with the public system. On the other hand, public sector medical staff were particularly supportive of working collaboratively with their private psychiatric counterparts. This may be a result of many public sector psychiatrists also undertaking some private work and hence being knowledgeable of the workings of both systems. However, public sector medical staff face their own challenges when a ‘shared care’ arrangement is in place with one of their patients. Different methods for working collaboratively with private psychiatrists need to be explored and roles clarified, including that of medico-legal responsibility.
Clinicians from both sectors indicated that difficulty communicating and confusion of roles and responsibilities were impediments to collaborating in shared care of patients. Practical changes to work practices may remedy this situation to some extent. For example, the identification of one worker in the public system to contact, even when the patient is being managed by a team, agreed upon days, times and methods of communicating, use of newer technologies such as E-mail, jointly developed and agreed management plans with clearly documented roles and responsibilities, are all possible solutions that could be easily implemented in the short term. Occasional case conferences, either face to face or over the telephone, with appropriate remuneration for private psychiatrists so they are not financially penalized for non-patient contact work, would also assist communication. This is now possible if private psychiatrists use the case conferencing items of the Medicare Benefits Schedule. Training and practice in their use would be of benefit. Equally or even more important is the development of shared trust between public and private provider. This may take longer to achieve than the practical changes listed, but is possible if there is ongoing commitment to optimize the care of jointly managed patients from workers in both sectors.
As hypothesized public clinicians and private psychiatrists perceived themselves to have quite different areas of expertise. Public clinicians in particular are not fully aware of the private psychiatrists' range of expertise, suggesting little understandings of the workings of the private system. This would result in fewer referrals for shared care across the sectors.
Another implication of this finding is for training. Psychiatry registrars and trainees of other disciplines spend most of their training time in public mental health facilities, which have become increasingly focused on psychotic disorders. A concern is that they may not be receiving sufficient training and experience in management of non-psychotic disorders. This raises the question: are those psychiatrists who are choosing to enter private practice in psychiatry less well equipped to do so compared with their colleagues who trained in the more broadly based public system over a decade previously? Innovations in psychiatry training to ensure a wider range of experience for trainees are needed. Rotations to private psychiatric services are one solution. This is currently in place with psychiatry registrars from SVMHS spending some of their training rotations at TMC. Consideration could also be given to some experience in primary care psychiatry. Training in the area of substance use disorders is particularly problematic since this area was split from psychiatry training some years ago. This hiatus in knowledge is reflected in our survey with the finding that only 11% of private psychiatrists and no public sector clinicians believed they had much expertise in the field. On the other hand, psychiatry training is becoming more broadly based within public psychiatry as it changes to include the development of skills and attitudes likely to assist working in teams and in shared care arrangements [11].
It must be acknowledged that our study took place in an urban setting with high numbers of private psychiatrists. It is possible that in more rural and remote areas with fewer private psychiatrists, public sector clinicians would manage a broader range of patients, including those with non-psychotic disorders. Thus a more widespread expertise might be expected.
In conclusion, the survey highlighted the scope for change in attitudes and in education, employment, communication and practice protocols that seem likely to facilitate effective working relationships between private psychiatrists and public mental health services. Despite obvious differences between the sectors, on average all groups surveyed seemed to be more supportive than not of jointly managing patients. The experience of the Partnership Project suggests that these changes are possible as stronger relationships develop between people working in the two services. While time and energy need to be invested in developing sustainable local arrangements for cross-referral and shared care, it is hoped that interventions such as the Project can pave the way for more effective collaboration in the future.
Footnotes
Acknowledgements
Thanks to Tony Pinzone for assistance with data management, and to all participants in the surveys.