
Abstract
In 2018, the Australian Government instructed the Productivity Commission to examine the social and economic effects of poor mental health, as well as make recommendations on how they might be addressed. The resulting Draft Report demonstrates both the benefits and risks of an economic approach to these issues. Some of the broader systemic recommendations have merit such as the need for stepped care, coordinated crisis management and the important role of welfare, housing and the workplace in improving mental health. However, there are areas of concern, particularly for mental health services in the public sector. One is a disproportionate emphasis on prevention and intervention in the early years of life for strategies where evidence for effectiveness is limited. Another is the introduction of market-based approaches such as shadow billing or a commissioner/provider split to the funding of mental health services across Australia. Among the numerous problems of such market-driven approaches are the increased costs of additional bureaucracy and the lack of commissioner expertise in planning services or evidence-based practice. As a result, similar arrangements have been abandoned in other jurisdictions. The Commission’s final recommendations and the Australian Government’s response are awaited and the resulting changes to the mental health system, and beyond, may well be influenced by the COVID-19 pandemic. However, reform should be based on evidence and achieved without increasing administrative complexity.
‘Science is the great antidote to the poison of enthusiasm and superstition’.
Introduction
In 2018, the Australian Government instructed the Productivity Commission (hereinafter the Commission) to examine the effect of mental health on economic participation and productivity. The Commission is an independent advisory body that reports on a range of economic, social and environmental issues in the country. The Draft Report (hereinafter, the Report) was released for comment in November 2019, with recommendations to be finalised in the following year although delays are likely given the COVID-19 pandemic (Productivity Commission, 2019).
The Commission identified that mental illness and suicide cost Australia an estimated $500 million a day and up to $180 billion a year. Long-standing systemic problems included under-investment in prevention programmes, an over-reliance on clinical services, difficulties in accessing support and a lack of clarity between Commonwealth and State or Territory governments about their roles and responsibilities. The resulting Report recommends major reforms to health services, and beyond, to address social determinants of mental health including welfare, schools, workplaces, housing and criminal justice. Broad themes include prevention and early intervention, closing critical gaps and services other than health.
In terms of the first, the Report strongly emphasises prevention and early intervention (Productivity Commission, 2019). For instance, there is a proposal that existing physical examinations of infants be expanded to include social and emotional well-being checks, as well as the appointment of a full-time teacher for ‘mental health and well-being’ in every school at a cost of almost $1b a year. However, the evidence for prevention and intervention that is presented in the Report has limitations (Dray et al., 2017). For instance, in children it was restricted to anxiety symptoms and general psychological distress, while in adolescents it was for internalising problems (Dray et al., 2017).
The Report also advocates a system of ‘stepped care’ of five levels (Productivity Commission, 2019). The most basic are resources for self-management that might be used by approximately one quarter of the population. The next level up is treatment in primary care or online, followed by Medicare-funded psychological services. The fourth is high-intensity care generally delivered by a psychiatrist. At the highest level is complex care with a mix of inpatient services and case management in the community. The Report highlights the importance of addressing the needs of the ‘missing middle’; those who don’t require inpatient care but are unable to access private psychiatric care because of cost or unavailability.
The assumptions that frame the Report indicate both the benefits and risks of the Commission’s approach. The focus is through the ‘lens of participation and contribution … how people with or at-risk of mental ill-health can be enabled to reach their potential in life, have purpose and meaning, and contribute to the lives of others’ (Overview, p. 4, Productivity Commission, 2019). The emphases on participation and contribution are arguably founded on economic principles of utility and value, which therefore determine the scope and nature of the Commission’s recommendations. While some address important social determinants of mental health by broadening the view to systemic issues, a few raise considerable concern for effective mental healthcare, which we discuss here.
The benefits: mental health care extends beyond specialist psychiatric services
One recommendation is to lessen demand on emergency departments by better integration of after-hours and mobile crisis services, as well as formalising follow-up after suicide attempts. Another is to highlight the role that welfare, housing and the workplace can play in improving mental health. For instance, the Commonwealth government could broaden the requirements for both the Carer Allowance and Carer Payment and increase funding for State and Territory government-provided housing and homelessness services. In addition, the National Disability Insurance Agency should include those with psychosocial disability when funding supported accommodation.
Another recommendation is that the Department of Health should cease directing agencies such as Primary Health Networks (PHNs) to fund Headspace centres or other specific service providers. Rather, they should have the discretion to redirect funds to areas they feel better meet the needs of their local areas. Although the Report acknowledges some of the limitations of the Better Access programme, a Commonwealth-funded scheme to improve the accessibility of psychological treatments, it recommends that funded sessions be increased in some cases.
However, there are at least two major areas of concern, particularly for public mental health services, which in part arise from the economic focus inherent in the Report.
The risks: a disproportionate emphasis on the early years of life
The Report places a disproportionate emphasis on the early years of life, while psychiatric illness occurs across the lifespan. Through a strictly economic lens, this could be understood as maximising the utility of life through early prevention, although the reality is more complex. The Report cites 15-year-old data from the United States indicating that one half of those who develop mental illness experience mental illness before the age of 14 years and 75% by the age 24 years (Kessler et al., 2005). However, this information was based on a retrospective survey of adults including seniors and so is particularly vulnerable to recall bias. Moreover, although the median age of onset for anxiety and impulse-control disorders was 11 years old, it was 30 years for mood disorders. More recent prospective data cited by the Commission show that much of the increased prevalence in younger ages is due to substance use disorders, not anxiety, depression or psychosis (Productivity Commission, 2019). This is mirrored by other data that show many new cases of schizophrenia occur after the age of 25 (Allison et al., 2019), as well as service use data from the Australian institute of Health and Welfare (2016) (Figure 1). This is reflected in the finding that over 80% of both the prevalence and disability-adjusted life years (DALYs) relate to schizophrenia occur in people aged between 25 and 64 years (Adult Psychiatry Imperative Consortium, 2019). The comparable levels for bipolar affective disorder are 65%. Finally, suicide in Australia is most common in 45–54 year olds (Adult Psychiatry Imperative Consortium, 2019).
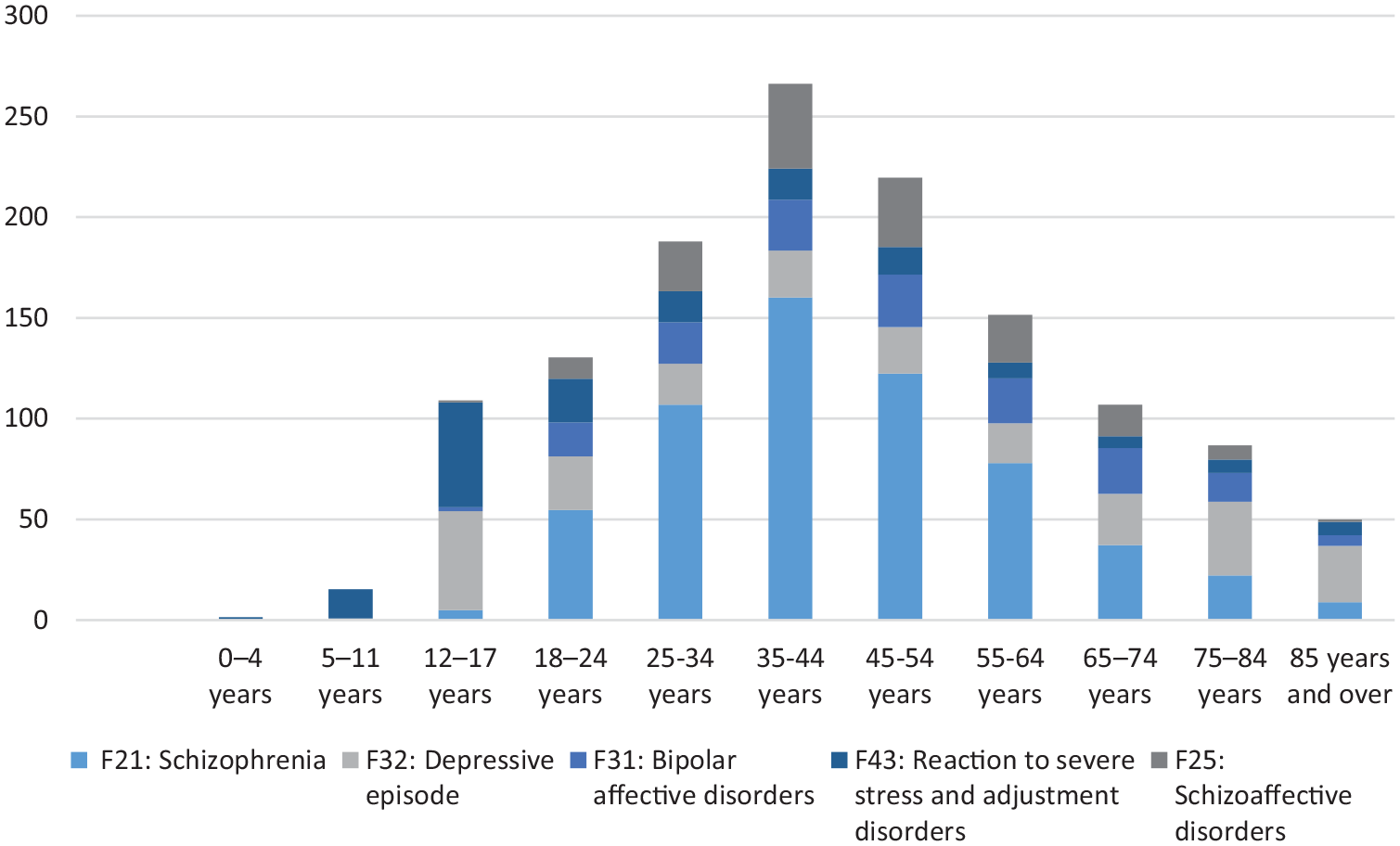
Mental health service use by age for five mental health conditions.
As a result of this focus on the early years of life, the Draft Report emphasises interventions directed at children and youth even though the document presents very limited evidence of effectiveness for its recommendations 17.1-17.6 (Productivity Commission, 2019). These include expensive checks of infant social and emotional well-being even though the level of supporting data is limited (Productivity Commission, 2019). The danger is that a focus on children and youth mental health could potentially detract from appropriate attention to mature and older adult mental health, especially considering the preliminary findings on mental health in the Aged Care Royal Commission (Royal Commission into Aged Care Quality and Safety, 2019).
Further risks: unproven market-based funding models
The second major area of concern is a proposal for market-driven ‘pooled funding’ to address the current division of financial responsibilities between Commonwealth and State/Territory governments (Recommendations 23.1-23.3; 24.1-24.2, Productivity Commission, 2019). Specifically, the Report recommends that the Commonwealth, States and Territories identify and pool their resources to improve access to a wider range of services such as social workers, occupational therapists, mental health nurses and counsellors. General practitioners (GPs) and private psychiatrists funded directly, or indirectly, through the Medicare Benefits Schedule (MBS) with varying degrees of patient co-payment would be excluded from this arrangement. The Report suggests the level of these ‘pooled’ funds would be linked either to existing or projected use of MBS-related services for allied health professionals. However, the danger of the former is the perpetuation of existing inequities in areas of geographical or socio-economic disadvantage. In particular, these are communities where there is often a shortage of GPs or private psychiatrists and whose residents may struggle to pay the difference between MBS payments and doctors’ fees. Unfortunately, the Commission’s alternative of using projected MBS use may also be challenging given the difficulty in accurately estimating future needs.
The Report proposes two market-driven options. One is the Renovate Model (Figure 2). Agencies such as PHNs would have greater flexibility in funding services, including employment and psychosocial supports outside of the National Disability Insurance Scheme (NDIS), while public hospital and community mental health services would remain the responsibility of State and Territory Governments. The exact responsibilities of each would be agreed through detailed regional plans. However, a major change would be to extend activity-based funding to community-based services as the Commission asserts that the current system is inefficient. Unfortunately, this is on the basis of a single guesstimate from unpublished data that only 29% of clinical staff time was spent on activities related to people with mental illness in community mental healthcare services across Australia (Productivity Commission, 2019). If true, this is certainly of concern, but much depends on how this is defined. The report is inconsistent – in one sentence relevant activities include face-to-face care, writing notes, individual care planning and liaison, while in another this is restricted to only face-to-face contact, to the exclusion of even telephone calls. Following the admission that no adequate activity-based funding classification for community care exists, it suggests a market-driven solution of shadow-pricing based on an unevaluated model from Victoria as an interim solution. In this model, funds are allocated solely by hours of work, rather than case complexity, with a weighting that favours face-to-face clinical contact. By this approach, the Report clings to a rather dated concept of individual clinician-based treatment, rather than multi-disciplinary care, so that only face-to-face time is billed at the full rate. The Report fails to consider that multi-disciplinary care also involves collaboration with other agencies, travelling to meet people in their homes, and contacting them by phone. It is not a model where a clinician sits in their office and ‘bills’ Medicare for appointments. Shadow pricing for a limited range of services also does not take into account that specialist mental health services also have responsibilities for teaching and research.
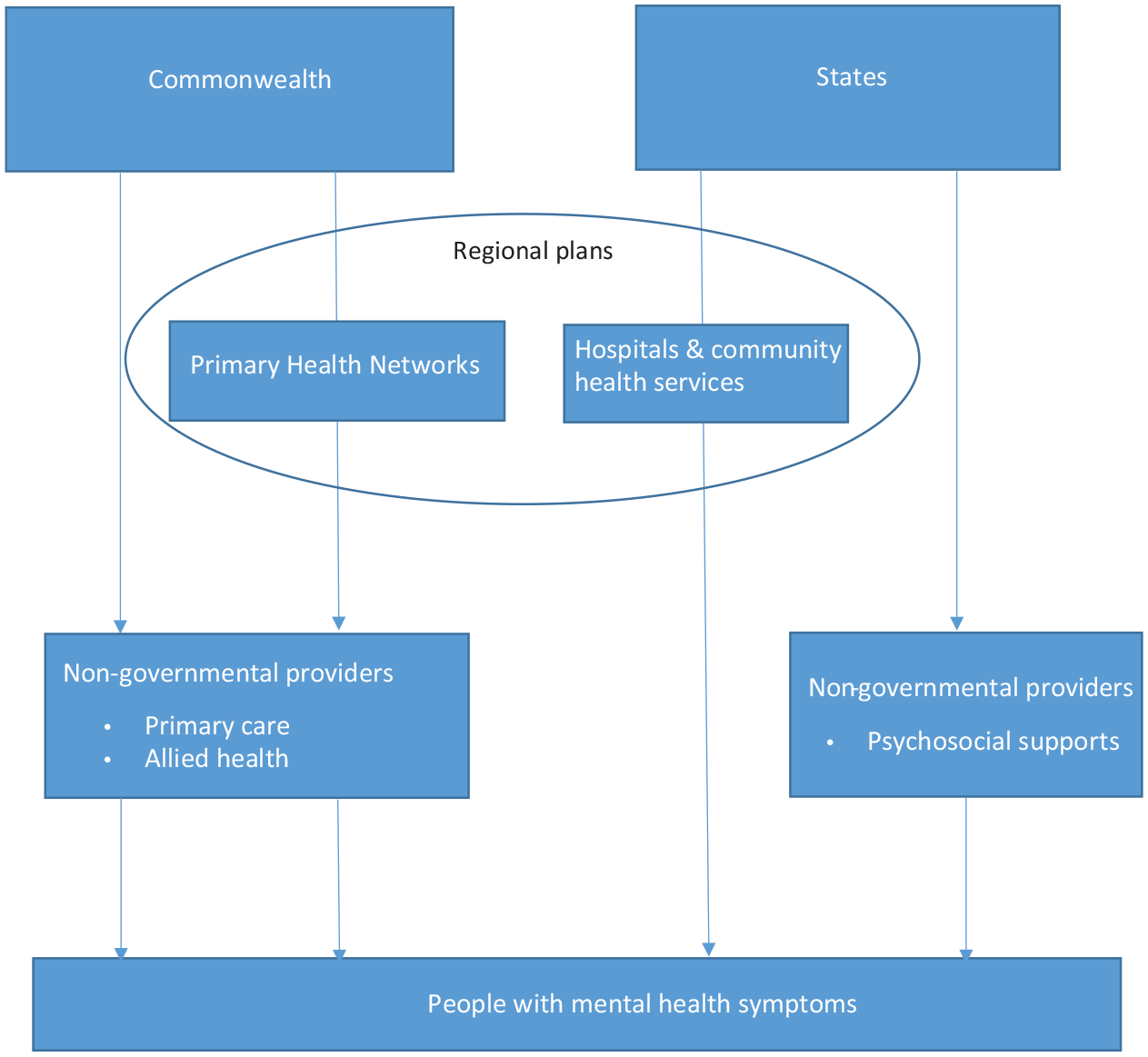
Renovate model.
The second option is the Rebuild model where federal and state funding for all mental healthcare (inpatient and community care), as well as psychosocial and carer supports, would be administered by Regional Commissioning Authorities (RCAs) (Figure 3). This would include funds currently channelled through PHNs, or other routes, with the exception of NDIS funding (Figure 3). RCAs would then buy, or commission, all services in the geographical area, for which they were responsible. RCAs would therefore fund a far greater range of services than those currently funded through PHNs, given that practically all mental health care would be included. Disappointingly, the Report makes no specific recommendations on the precise number of required beds in spite of persistent concerns about the safety of current provision, basing their figures on the National Mental Health Service Planning Framework (Consortium of Australian Psychiatrists and Psychologists, 2020). However, the Report leans towards modelling that suggests Australia only needs a 3% increase in acute beds even though Australia is 26th of the 34 countries in the Organisation for Economic Co-operation and Development (OECD) for hospital psychiatric beds per 100,000 population (Allison and Bastiampillai, 2015). This translates into 29 fewer beds per 100,000 than the OECD average and a risk of increased acuity on admission. Although the same modelling suggests a considerable increase in subacute beds, experience from South Australia suggests that one does not substitute for the other (Allison and Bastiampillai, 2015).
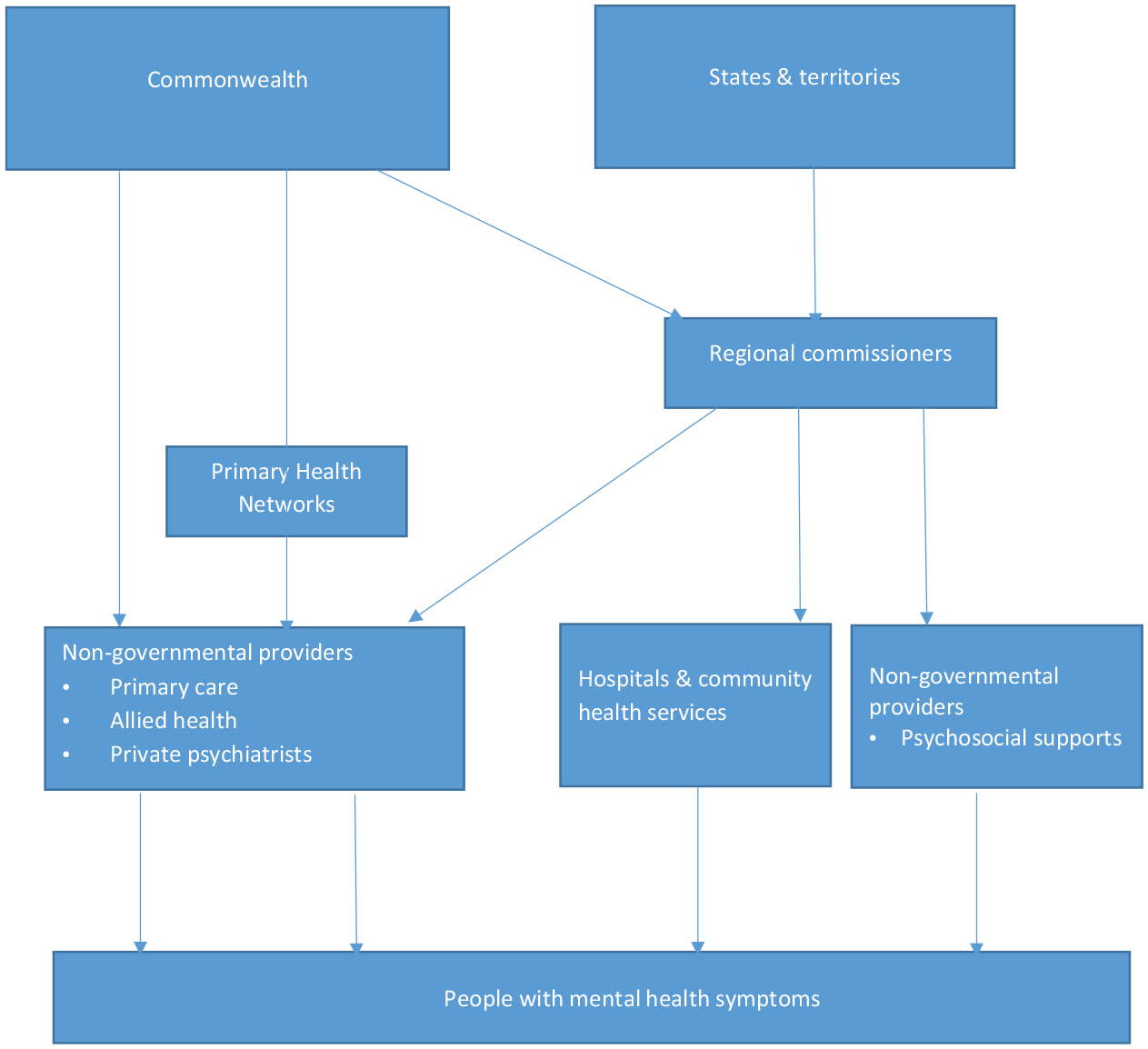
Rebuild model.
The overall proposal to introduce a commissioner/provider split to the funding of virtually all of mental health services across Australia is deeply concerning, and risks repeating the errors already made in other jurisdictions of re-disorganisation (Looi and Kisely, 2019). In the United Kingdom, a similar approach merely added a further bureaucratic layer of unclear utility in the planning of mental health services. Among the numerous issues were increased administrative costs and the lack of expertise in planning services or evidence-based practice (Health Care Commissioning, 2018), especially in areas of specialisation such as eating disorder. Commissioning was also difficult because of the complex nature of healthcare and further limited by the scarcity of relevant technical and managerial skills, as well as information asymmetries between commissioners and providers (Health Care Commissioning, 2018). In particular, commissioners lacked capacity and capability in needs assessment, risk profiling and budget management (Health Care Commissioning, 2018; Miller and Rees, 2014). The concept failed to gain legitimacy in the eyes of the public. Transactional problems included adherence to agreed deadlines for tenders, maintaining records and paying bills (Miller and Rees, 2014). There have also been concerns that outcomes set by commissioners/purchasers did not fully reflect the clinical work that was being done (Rizq, 2014). Furthermore, consultation-liaison services often faced uncertainty as it was unclear whether funding should come from mental health services or the general hospital where they were located. Following Scottish and Welsh devolution, both countries abolished the commissioner/provider split in 2009 and reintroduced integrated health boards responsible for both planning and running services within defined geographical areas (Health Care Commissioning, 2018). The report fails to consider any of these issues; indeed, it does not even mention what size of population the proposed RCAs would cover.
Finally, the issue of proposed RCAs leads into the Report’s recommendations on governance of mental health services (Recommendations 22.1-22.2; Productivity Commission, 2019). While we agree that a whole-of-government strategy to mental healthcare is necessary (Looi et al., 2019), it is important that governance reforms do not introduce further layers of administrative complexity (e.g. RCAs) and thus detract from effective implementation of needed reforms.
What are the alternatives?
The fragmented nature of mental health services and multiple funding streams from both the Commonwealth, on one hand, and the states and territories, on the other hand, have long been impediments to the effective delivery of care (Looi and Kisely, 2018; Looi et al., 2019). Thus, better governed, coordinated mental health care in all jurisdictions is needed. However, existing problems with the disorganisation and inefficiencies of public mental health services are not merely economic, they relate to specific issues of governance, policy, planning, implementation and limited evaluation of service provision (Looi and Kisely, 2018; Looi et al., 2019; Looi and Kisely, 2019).
The quality of care can also be improved for severe mental illness. A recent submission to the PC Draft Report highlighted the potential for a national network of Specialist Mental Health Centres (SMHC), involving consumers, carers, clinicians and researchers collaborating to improve the treatment of severe mental illness in all states and territories (Consortium of Australian Psychiatrists and Psychologists, 2020). This would be based on the SMHC established in Victoria as recommended by the Royal Commission into Victoria’s Mental Health System as proposed by the Adult Psychiatry Imperative Consortium (2019).
The resourcing of mental health care needs to be adequate. There is a need for significantly increased levels of community and inpatient mental health care that are based on expert inputs beyond those of the National Service Planning Framework (Allison and Bastiampillai, 2015; Consortium of Australian Psychiatrists and Psychologists, 2020). Minimum service and staffing levels should be mandated at Commonwealth/Council of Australian Government levels similar to the manner in which mental health care is formally regulated in Germany ( Consortium of Australian Psychiatrists and Psychologists, 2020). Moderate increases in acute, non-acute and forensic beds for the general adult population are needed (Allison and Bastiampillai, 2015; Consortium of Australian Psychiatrists and Psychologists, 2020).
The Report would have been strengthened if it had contained more modest proposals for structural change, particularly for financing, the effect of which could be easily evaluated before further steps were taken. For instance, aspects of the Renovate model such as the development of regional collaborations between state-based health services and PHNs could eliminate duplication and improve continuity of care (Figure 2). In addition, more health services research is required to establish appropriate activity data on community mental health before the current funding model is changed. Furthermore, all age groups need to be equally considered to ensure a comprehensive approach to population mental health. Finally, mental health service reform will need to take into account the consequences of the COVID-19 pandemic such as increased need and a possibly greater reliance on telehealth (Looi and Pring, 2020). The appointment of a chief medical officer for mental health may also increase the Commonwealth’s role in leading change. However, as with the Commission’s recommendations, the response should extend beyond the health service to encompass interventions for domestic violence and alcohol use, as well as financial aid in areas such as housing and unemployment (Gunnell et al., 2020).
Conclusion
The Commission’s Draft Report follows a series of reviews, inquiries and similar processes that are short on evidence but long on radical ideas based on unclear evidence. Indeed, some of the recommendations on mental health services echo those from the National Mental Health Commission’s 2014 Review that thankfully were never implemented (Kisely, 2016; National Mental Health Commission, 2014). Mental health deserves better than serving as a laboratory for the latest ‘idée du jour’. The Report may not only be an opportunity, but potentially a threat unless recommendations are subject to sustained critical review of the policy and practical implications. We have suggested alternative recommendations, based on the scientific and policy literature to date, including some of the submissions to the Commission when it was writing the Draft Report.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.