
Abstract
At a population level little is known about the labour force participation, employment and work performance of people with anxiety disorders. Characteristics of this group are rarely reported in terms of large representative samples. Most prior studies are based on small outpatient or rehabilitation samples, usually comprising a heterogeneous mix of ‘psychiatric disabilities’ or people with ‘serious’, ‘severe’ or ‘severe and persistent’ mental illness [1–3]. Mixed diagnostic samples limit the capacity to differentiate the vocational assistance needs of people with anxiety disorders.
Anxiety disorders are among the most prevalent and treatable mental disorders yet many people do not receive treatment [4–7] or do not receive optimal treatment [8], [9]. Consequently, the impact of anxiety on individual employment trajectories may be underestimated. Furthermore, there is evidence that when anxiety is treated previously impaired work performance can be restored. A recent longitudinal study using objective productivity measures assessed the impact of anxiety on the productivity of medical insurance claims processors [10]. The authors found that claims processors with ICD-9 anxiety disorders (n = 71) recovered a substantial proportion of their pretreatment productivity, and along with those treated for migraines and depression ‘… experienced the greatest long-term percentage improvement in productivity following treatment…’ (p. 25).
Another reason for investigating the impact of anxiety disorders on employment can be found in the challenge of ageing populations. The Organization for Economic Co-operation and Development (OECD) advise member countries [11] to implement policies reducing the dependence ratio of older people (aged 65 years or older) to those of working age (15–64 years). The OECD warns that failure to heed this advice will lead to falling living standards as the dependence ratio increases from 22% to 46% by the year 2050. Hence, a population level understanding of the impact of anxiety disorders on employment could inform public policy development in terms of health, income support, labour market, disability employment and vocational rehabilitation.
To investigate these issues, a secondary analysis was conducted using data from the Survey of Disability, Ageing and Carers, Australia 1998 (SDAC 98, Australian Bureau of Statistics, ABS) [12], [13]. This survey incorporated a multistage probability sample enabling the estimation of population prevalence and standard errors. Labour market participation and employment patterns were examined among people with ICD-10 anxiety disorders in contrast to people without activity restrictions, disability or long-term health conditions.
Expected results
The structural model of mental illness, treatment, and economic outcomes [14] provided a theoretical framework for this investigation. This model suggests that proportionally fewer people with anxiety disorders would be employed part time or full time, while more would rely on Government income support compared to people without disability or long-term health conditions. Within the limitations of a cross-sectional survey, and consistent with the reported treatment benefit [10], receiving treatment was expected to be associated with improved patterns of labour force participation and employment.
Method
Data source
Data were analysed from a confidentialized unit record file (CURF) provided by the ABS. The SDAC 1998 was conducted from 16 March to 29 May 1998 [12], [13]. Data were collected from a household sample of 37 580 people, and from 5716 people living in cared accommodation (i.e. residents of hospitals, nursing homes, aged care and disability hostels and children's homes). The survey was authorized by the Australian Federal Census and Statistics Act, 1905. The ABS protected the confidentiality of individuals in the data set by removing identifiable households from the file, and where necessary, unlinking variables to suppress the detail available. Hence, data from this CURF may not exactly match that reported elsewhere by the ABS. Other than reducing the total sample size by 1.5% these confidentiality protections did not limit these analyses.
Sampling
The survey design and operation are detailed in full elsewhere [13], [15]. The survey took place in both urban and rural areas in all states and territories, except in remote and sparsely settled parts of Australia. Statistical adjustments for not sampling remote residents in the Northern Territory were applied because unlike other states, approximately 20% of Northern Territory residents live in remote areas. Participants included all people except prisoners, non-Australian diplomatic personnel, and members of non-Australian defence forces stationed in Australia. The survey sample was selected using multistage sampling techniques based on census collection districts. The effective sample included 15 316 private dwellings (one per 400 in Australia); 399 non-private dwelling units (i.e. hotels, motels, boarding houses, educational and religious institutions, guest houses, construction camps, short-term caravan parks, youth camps and camping grounds, staff quarters, and self-care components of retirement villages); and 618 cared accommodation establishments. Non-private dwellings and cared accommodation establishments were selected separately from private dwellings to ensure adequate representation. Each had a chance of selection proportional to the average number of people accommodated.
Identifying people with anxiety disorders
All health conditions of at least 6 months duration were coded to a classification based on the International Statistical Classification of Diseases and Related Health Problems, 10th Revision [16]. Experienced household interviewers (who were not medically trained) were provided with three additional days training in the use of the structured computer assisted interview designed specifically for this survey, an update of the 1993 schedule. ICD-10 based pick-lists were incorporated for automatic coding of health conditions in the field. In the household component a diagnosis of anxiety was identified in three possible ways: during the initial and subsequent interviews either with a responsible adult of the household, by self-report, or by another responsible adult person assisting with the interview. In the cared accommodation component, nominated staff members recorded diagnoses using personal knowledge supported by medical, nursing and administrative records.
ICD-10 classifications of anxiety as the primary disorder were excluded when comorbid with schizophrenia, other psychoses, and depression. Anxiety disorders as the primary condition included: phobias (agoraphobia, social phobia and specific phobia, ICD-10 code F40); panic disorder and generalized anxiety disorder (F41); obsessive compulsive disorder (F42); acute stress disorder and post-traumatic stress disorder (F43); and other neurotic, stress related or somatoform disorders (F44–48). Text entries were entered for any disorders reported which did not match items on the pick lists. Codes for text entries were determined by more experienced coders back at the office. This was necessary because some anxiety disorders were collapsed into more general categories within the pick lists. For instance, acute stress disorder (F43.0) and post-traumatic stress disorder (F43.1) were both coded under nervous tension/stress. To ensure coding accuracy, all interviews were checked until interviewers achieved 90% agreement or higher with the experienced coder. Sample monitoring of each interviewer's coding continued thereafter throughout the data collection phase.
Disability, long-term health conditions, and employment restrictions
The survey used the International Classification of Impairments, Disabilities and Handicaps [17] to identify disability and the associated restrictions. Each interview commenced with screening questions about activity restrictions, impairments, and long-term health conditions, before the level of disability and the underlying health condition were identified. It was possible for people to have an anxiety disorder as a long-term health condition, but without activity restrictions and hence, without a disability.
Employment restrictions were assessed at four levels of severity (profound, severe, moderate, and mild). ‘Profound’ was defined as unable to perform employment or always needing assistance. ‘Severe’ was defined as needing assistance to perform employment activities. ‘Moderate’ referred to not needing assistance, but having difficulty. ‘Mild’ referred to having no difficulty, but using aids or equipment because of employment restrictions.
Other standardized measures
Post school educational qualifications were coded according to the ABS Classification of Qualifications [18]. Occupational category was classified to the Australian Standard Classification of Occupations [19]. Industry of employment was classified to the Australian and New Zealand Standard Industrial Classification [20]. Work performance was assessed by the number of hours worked, and by two items from the SF-12 (Short Form 12) [21] a short form health survey. Further descriptions of terms and variables used in this survey are available from the ABS [13].
Analyses
Analyses were restricted to people aged 15–64 years with primary anxiety as the ICD-10 condition, in either the household or the cared accommodation component of the survey (n = 745). As no education or labour market information was collected about people living in cared accommodation, subsequent analyses involved only the household component. A control group consisted of people aged 15–64 years without activity restrictions, disability or long-term health conditions (n = 20 366). Population weights were provided by the ABS as an individual level variable within each respondent's record [13], p.21], allowing expansion of estimates to apply to the Australian population within the scope of the survey.
Recommended statistical methods were followed [13], pp.35–41] using SAS statistical software [22]. The tables show population prevalence estimates per 10 000 people aged 15–64 years. Estimates and standard errors (SE) were converted to labour-market-age population estimates by multiplying by 1248.444, a conversion factor derived from the Australian population estimate of people aged 15–64 years in 1998 (12 484 440 people). Significant differences were identified by standardized two tailed z-scores adjusted for multiple pair-wise comparisons by the Bonferroni procedure. Estimates with standard errors less than 25% of the estimate value are considered by the ABS as sufficiently reliable for most purposes. Estimates with standard errors greater than 25% are marked accordingly.
Results
Survey responses
Responses were obtained from 93% of households sampled. Completed interviews were obtained from 35 569 people, 94.4% of the total sample. Partial non-responses included income-refusal, 1.9% of the total sample; income-don't know 3.4%; and carer form incomplete/not obtained 0.1%. Full non-responses included refusals 0.1%; noncontacts 0.1%; and language problems, death/illness, or other less than 0.05%. In the cared accommodation component, 93.4% of establishments responded (577 of 618), providing 5716 completed personal questionnaires.
Prevalence of ICD-10 classified anxiety disorders
The probability sample consisted of 42 664 people, of whom 25 217 were of labour force age (15–64 years). Within this age range, 745 people were identified as having an ICD-10 classified anxiety disorder, 716 of whom resided in private or-non-private dwellings. Of the population estimate of 12 485 444 people of labour market age, 361 326 householders (SE 9156 people) were estimated as having an ICD-10 anxiety disorder. The prevalence of males aged 15–64 years with anxiety disorders (compared to all males aged 15–64 years) was 118.25 males per 10 000 males (SE 5.41). Anxiety disorders were more prevalent (p < 0.001) among females at 170.34 per 10 000 females aged 15–64 years (SE 6.12). Of those with anxiety disorders aged 15–64 years residing in cared accommodation, similar small proportions (p = 0.94) of both males (0.38, SE 0.48) and females (0.43, SE 0.50) were found.
Non-participation in the labour force
Compared to controls, proportionally more people with anxiety disorders were not in the labour force (47.1% vs 19.9%, see Table 1). Among both groups, greater-non-participation was associated with increasing age; female gender; country of birth other than Australia, New Zealand, Oceania, United Kingdom, or Western Europe; and not obtaining post school qualifications (p < 0.001 for all comparisons). Non partnered status and leaving school early were associated with greater non participation among the control group, while among people with anxiety disorders, similar differences emerged but were not statistically significant.
Non-participation in the labour force† by people with ICD-10 anxiety disorders compared to people without disability or long-term health conditions. Prevalence estimates and (standard errors) per 10 000 people aged 15-64 years
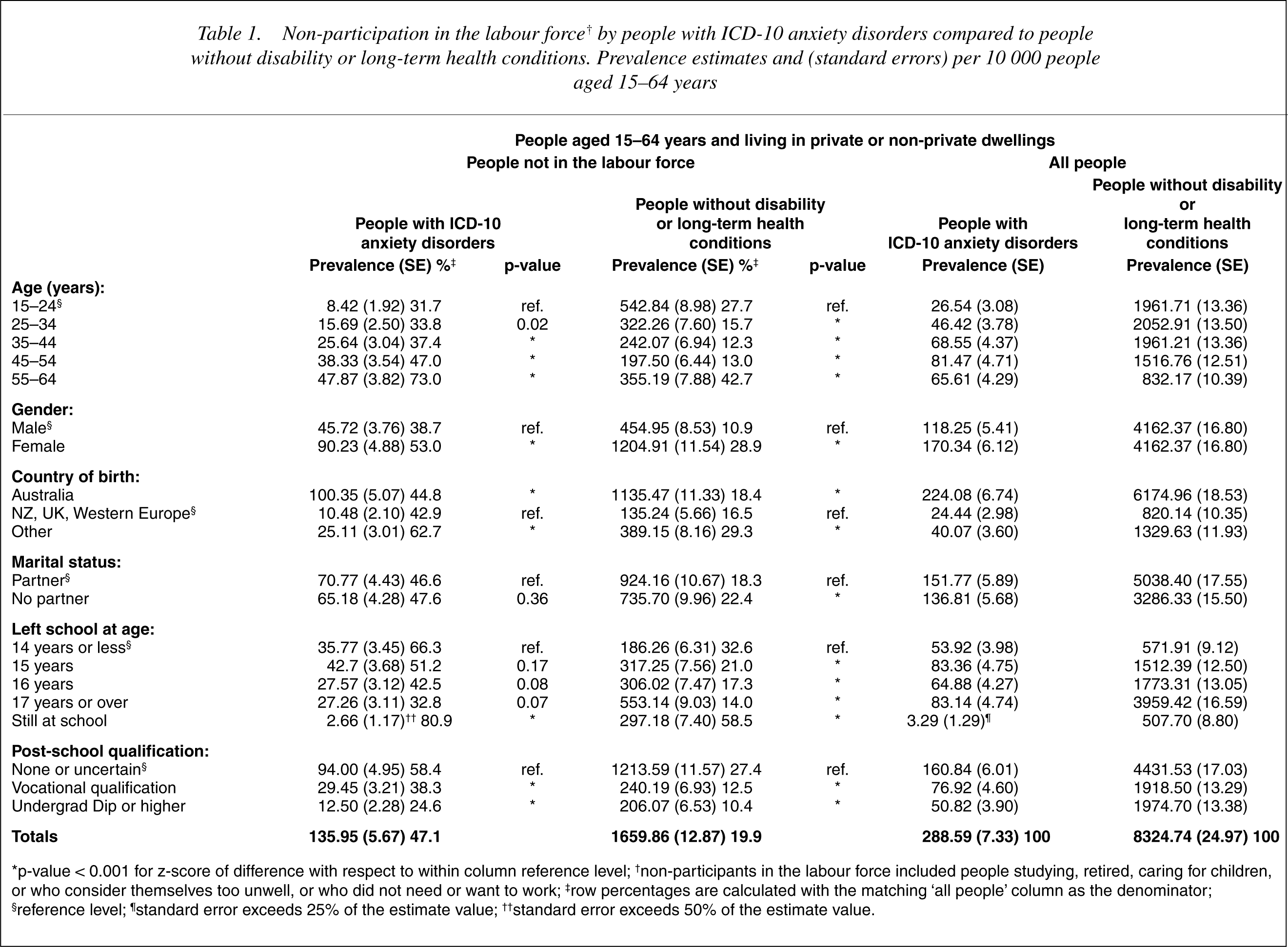
∗p-value < 0.001 for z-score of difference with respect to within column reference level; †non-participants in the labour force included people studying, retired, caring for children, or who consider themselves too unwell, or who did not need or want to work; ‡row percentages are calculated with the matching ‘all people’ column as the denominator; §reference level; ¶standard error exceeds 25% of the estimate value; ††standard error exceeds 50% of the estimate value.
Employment restrictions and employment
Employment restrictions were associated with: greater-non-participation in the labour force, reduced job seeking, and less part time or full time employment (see Table 2). Fewer people with anxiety disorders were employed part-time compared to controls (see Table 3). The part time employment difference was greatest among: people aged 15–24 years; those aged 55–64 years; females; people without partners; those still at school; and among those without a post school qualification.
Labour market activity by employment restrictions among people with ICD-10 anxiety disorders aged 15-64 years and living in private or non-private dwellings, compared to people without disability or long-term health conditions. Prevalence estimates and (standard errors) per 10 000 people aged 15-64 years
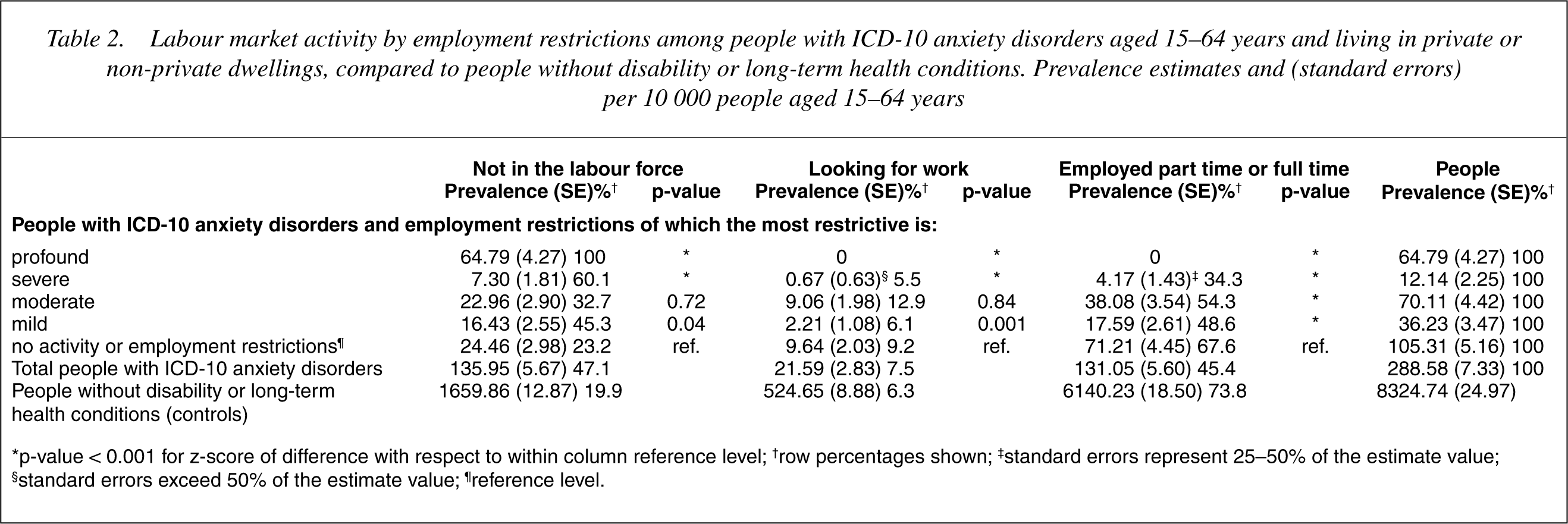
∗p-value < 0.001 for z-score of difference with respect to within column reference level; †row percentages shown; ‡standard errors represent 25-50% of the estimate value; §standard errors exceed 50% of the estimate value; ¶reference level.
Part-time employment† of people with ICD-10 anxiety disorders compared to people without disability or long-term health conditions. Prevalence estimates and (standard errors) per 10 000 people aged 15-64 years
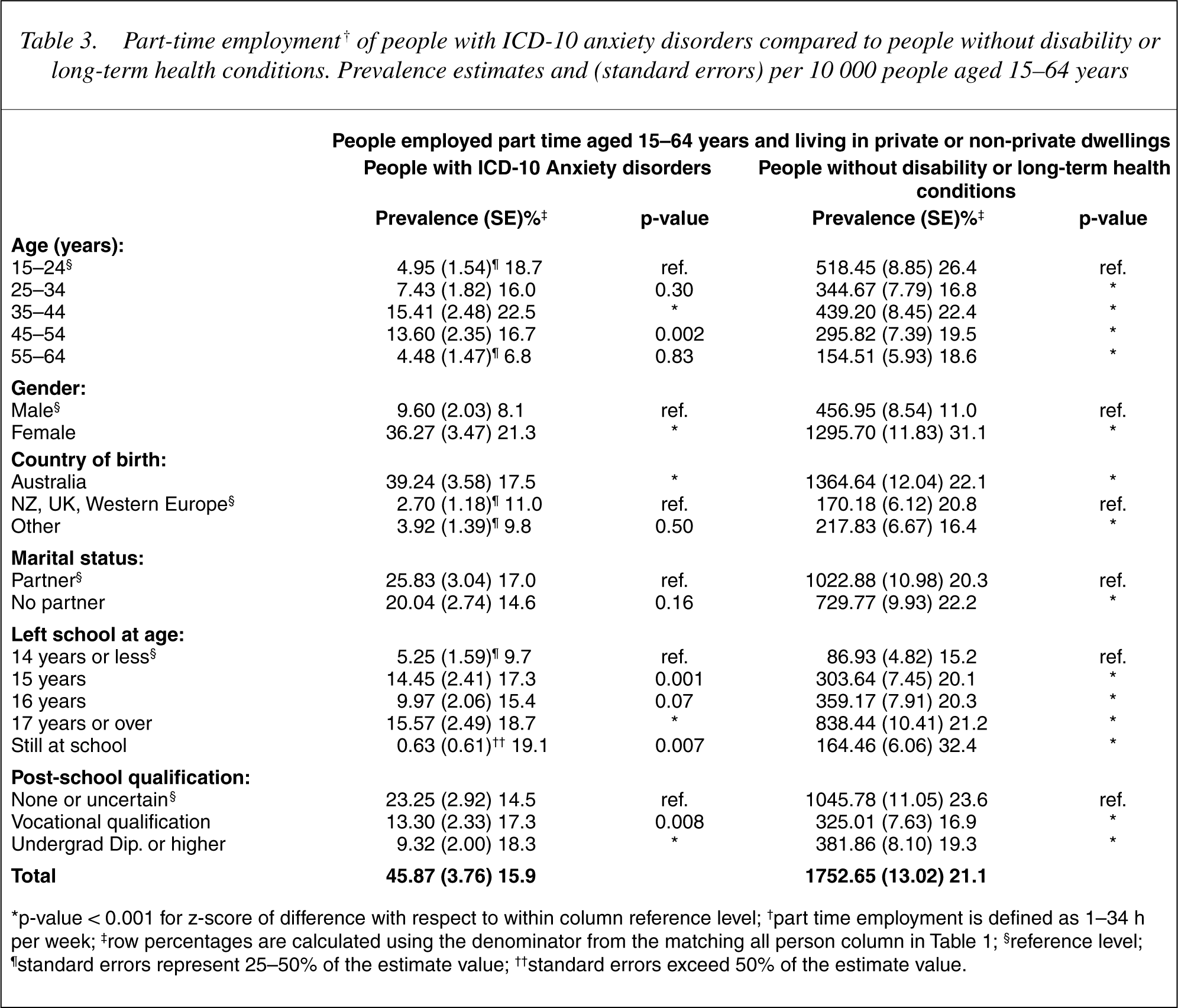
∗p-value < 0.001 for z-score of difference with respect to within column reference level; †part time employment is defined as 1-34 h per week; ‡row percentages are calculated using the denominator from the matching all person column in Table 1; §reference level; ¶standard errors represent 25-50% of the estimate value; ††standard errors exceed 50% of the estimate value.
Fewer people with anxiety disorders were employed full time compared to controls (see Table 4). Among controls, full time employment peaked at 25–34 years and did not decline until 55–64 years. However, among people with anxiety disorders full time employment peaked at 25–34 years with gradual decline to 54 years followed by an exodus from full time employment at 55–64 years. Among controls full time employment was associated with age 25 years or over, males, partnered status, remaining at school, and obtaining post school qualifications. A similar pattern was apparent for people with anxiety disorders, although neither partnered status nor post school qualifications were statistically significant. Undergraduate diplomas or higher appeared beneficial to people with anxiety disorders. However, among controls most of the gain in full time employment appeared associated with vocational qualifications (see Table 4).
Full-time employment† of people with ICD-10 anxiety disorders compared to people without disability or long-term health conditions. Prevalence estimates and (standard errors) per 10 000 people aged 15-64 years
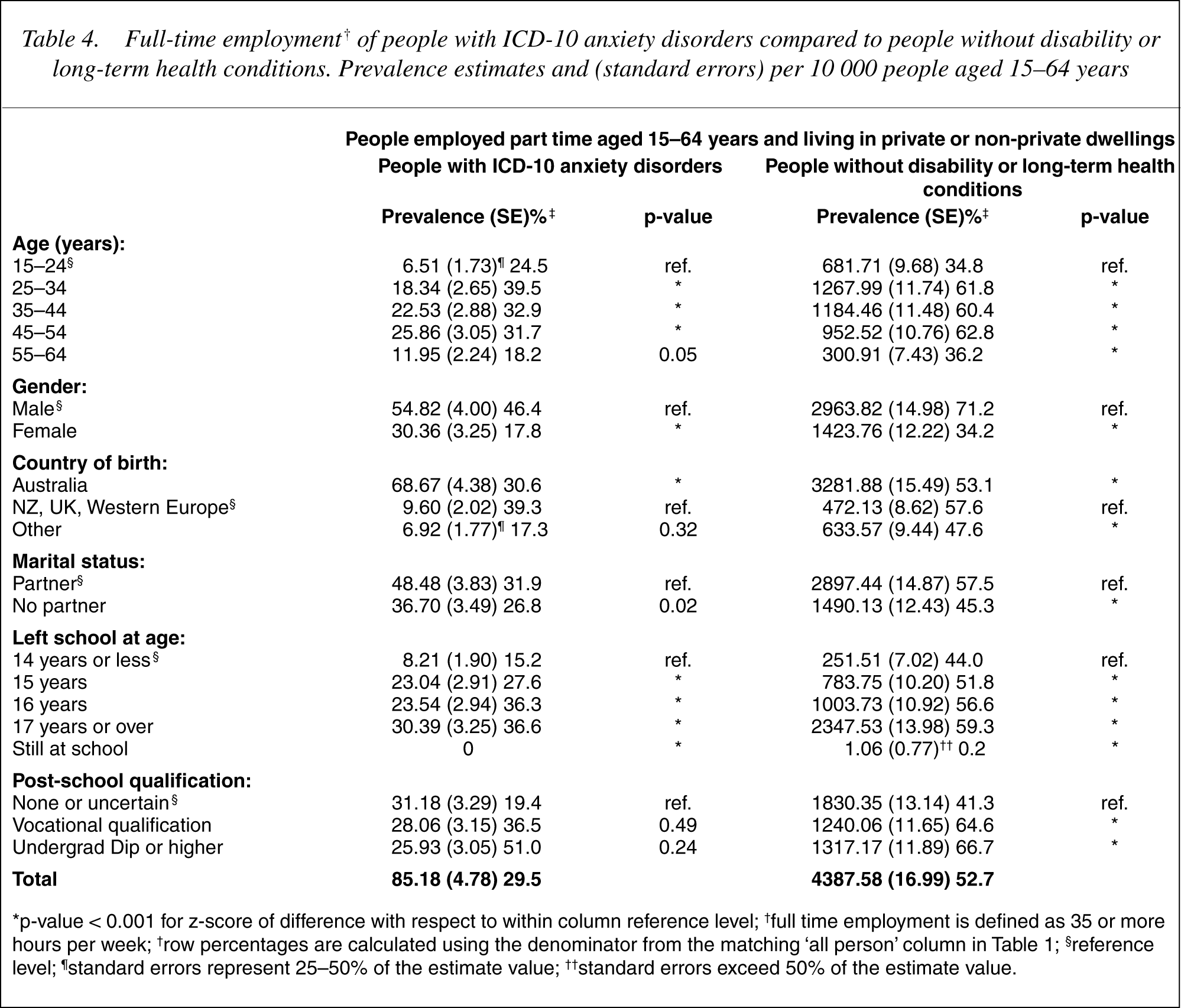
∗p-value < 0.001 for z-score of difference with respect to within column reference level; †full time employment is defined as 35 or more hours per week; †row percentages are calculated using the denominator from the matching ‘all person’ column in Table 1; §reference level; ¶standard errors represent 25-50% of the estimate value; ††standard errors exceed 50% of the estimate value.
Modes of employment
Compared to controls, proportionally more people with anxiety disorders were employed in the Government sector than in the private sector (22.9% vs 18.6%). Proportionally fewer people with anxiety disorders worked as employees (80.9% vs 86.9%), more often working as employers (6.6% vs 4.2%), self-employed (10.0% vs 8.1%), or as contributing family workers working without pay in a family business or on a farm (2.5% vs 0.8%). Work from home was more frequently reported by people with anxiety disorders than by controls (38.2% vs 29.6%) and more people with anxiety held two or more jobs simultaneously (9.2% vs 6.8%).
Occupation category and industry group
People with anxiety worked in all occupational categories and industry groups similar to controls. Differences were noted using proportional divergence of 2% or more. People with anxiety disorders were under represented among tradespeople or related workers, and professionals; while over represented among intermediate clerical, sales and service staff, managers and administrators, and associate professionals. Proportionally more people with anxiety worked in agriculture, forestry or fishing, and in transport and storage industries. Whereas, fewer people with anxiety worked in either the wholesale, or retail industries (see Tables 5,6).
Occupations reported by employed people with ICD-10 anxiety disorders aged 15-64 years compared to people without disability or long-term health conditions. Prevalence estimates† and (standard errors) per 10 000 people aged 15-64 years
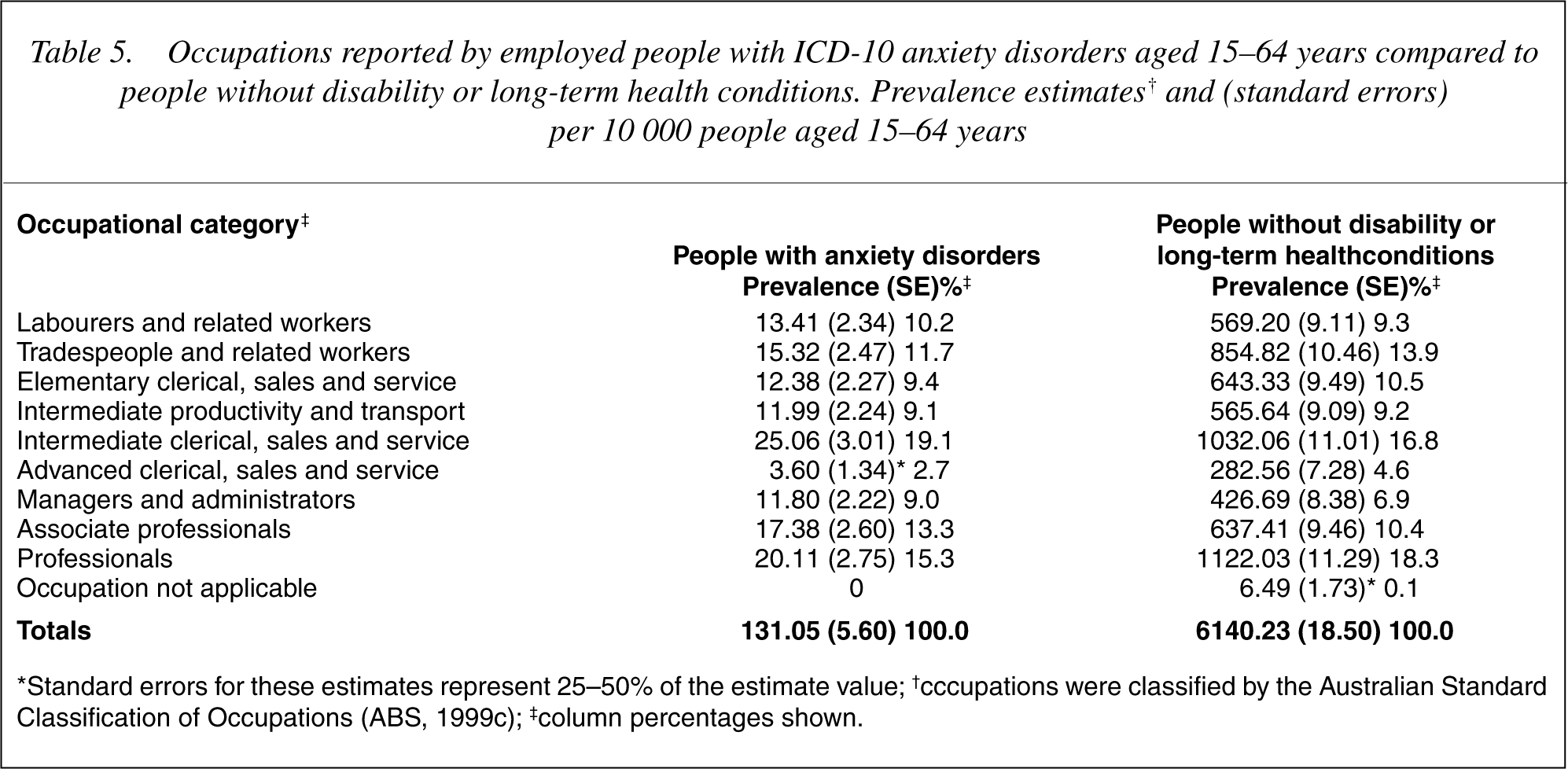
∗Standard errors for these estimates represent 25-50% of the estimate value; †cccupations were classified by the Australian Standard Classification of Occupations (ABS, 1999c); ‡column percentages shown.
Industry group reported by employed people with ICD-10 anxiety disorders aged 15-64 years compared to employed people without disability or long-term health conditions. Prevalence estimates and (standard errors) per 10 000 people aged 15-64 years
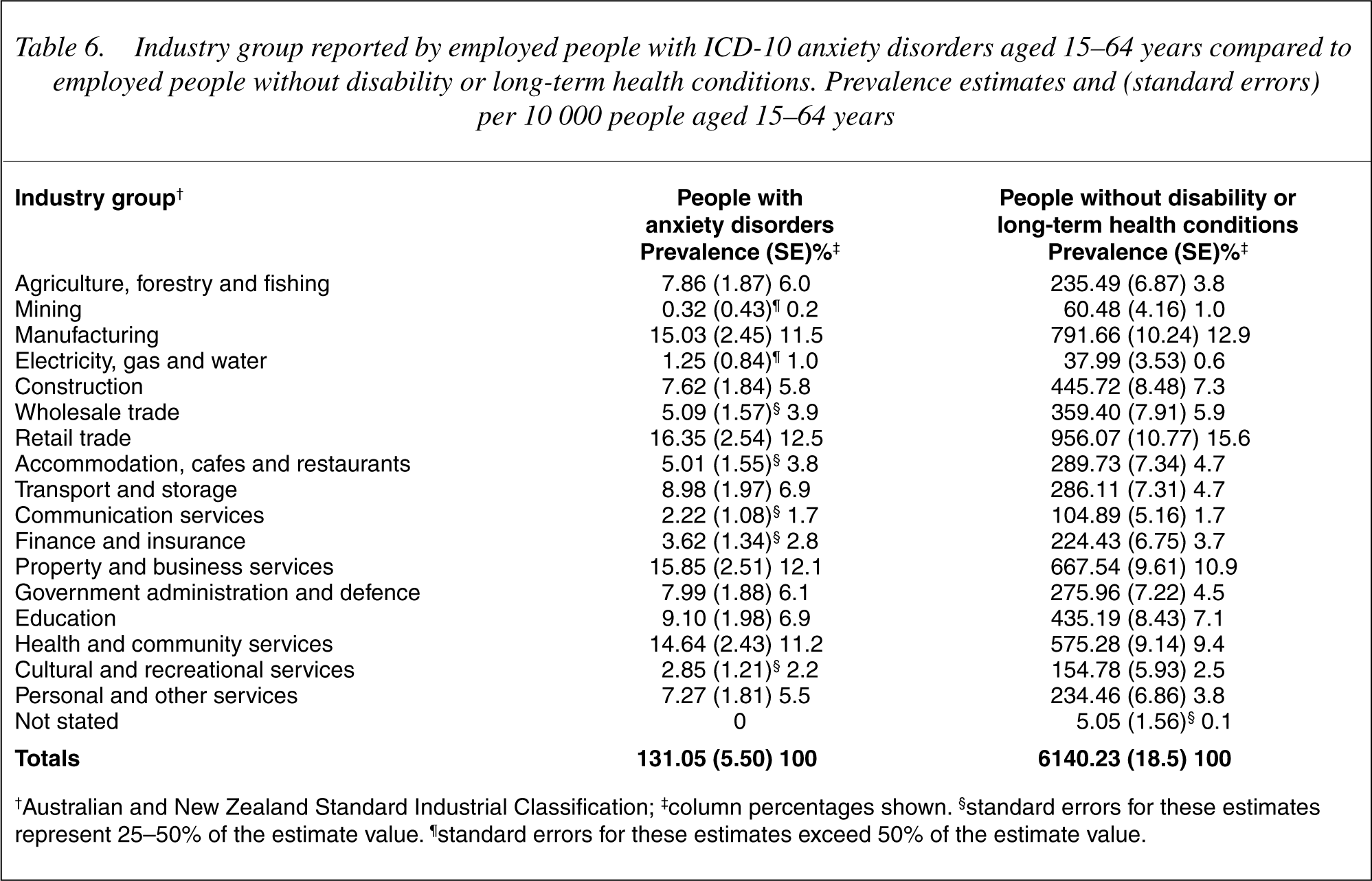
†Australian and New Zealand Standard Industrial Classification; ‡column percentages shown. §standard errors for these estimates represent 25-50% of the estimate value. ¶standard errors for these estimates exceed 50% of the estimate value.
Hours worked
People with anxiety were over represented in the extemes of hours worked per week. Proportionally more people with anxiety (16.7% vs 12.7%) worked 0–15 h each week. Differences converged at 25–34 h (8.1% vs 7.9%). People with anxiety were under represented among those working 35–69 h (55.1% vs 67.3%) and were over represented in the 70–97 h range (9.9% vs 4.1%). More males than females worked extremely long hours in both groups (anxiety 83.4% vs controls 84.9%).
Source and level of income
More people with anxiety received Government pensions or allowances as their principle source of income (48.5% vs 17.7%). In addition, fewer people with anxiety reported wages or salary as their main income source (33.7% vs 61.2%), and fewer reported having no income source (5.0% vs 8.6%). The two groups did not appear to differ on income from partnerships or business (anxiety 7.4% vs 8.5% for controls), rental property (0.1% vs 0.7%), dividends or interest (1.7% vs 0.7%) child support or maintenance (1.9% vs 1.5%), superannuation or annuities (1.7% vs 0.7%), or income source not known (0.0% vs 0.5%).
Mean weekly cash income was estimated by mid points of income groups and group prevalences. Those with anxiety earned 4.4% less than controls when receiving wages, salary or business income (A$556.31 per week vs A$582.16); 10.6% more when receiving Government pensions, benefits or allowances (A$168.79 vs A$152.60), and 37.1% more from other sources of income (A$218.41 vs A$159.31). These sources included rental properties, dividends and interest on investments, superannuation or annuities, and income from child support. The estimate of mean weekly income from wages, salary or business income among controls (A$582.16 per week) appeared reliable at 98.4% of the official average weekly wage in 1998 (A$591.40 [23]).
Work performance
Work performance was assessed by self reported work accomplishment and care taken at work in the past 4 weeks. Compared to controls, more employed people with anxiety reported accomplishing less in the past 4 weeks (26.5–33.4% vs 0.2–0.7%). Furthermore, among those with anxiety disorders, work accomplishment decreased monotonically with labour market status (see Table 7). Although a similar pattern emerged in the control group, work accomplishment among part time workers did not differ from those not in the labour force. More employed people with anxiety took less care in the past 4 weeks, and this proportion increased monotonically with decreasing labour force status (see Table 8). No equivalent pattern was found in the control group where differences were not statistically significant.
Work accomplishment by people with ICD-10 anxiety disorders aged 15-64 years compared to people without disability or long-term health conditions. Prevalence estimates and (standard errors) per 10 000 people aged 15-64 years
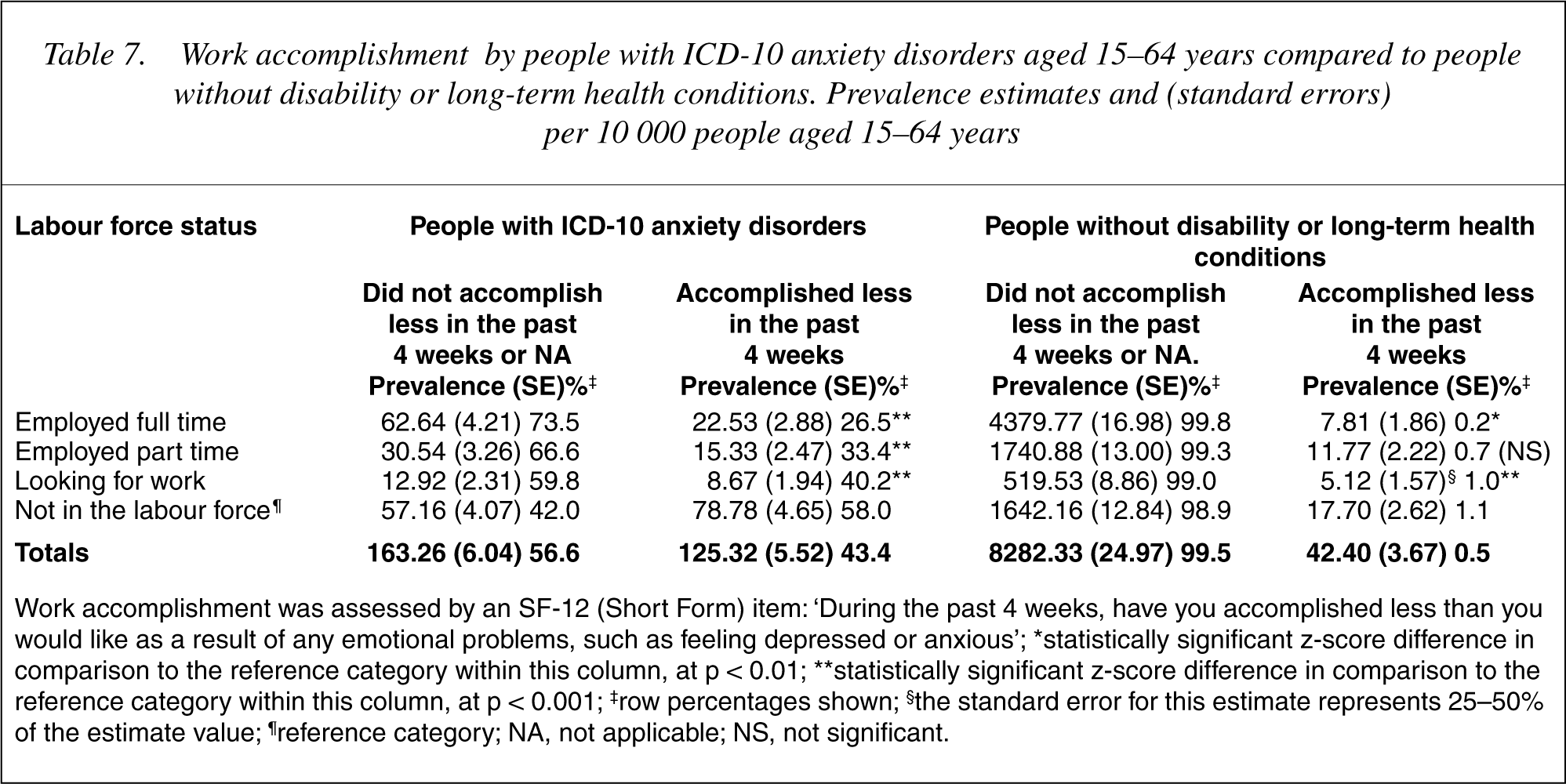
Work accomplishment was assessed by an SF-12 (Short Form) item: ‘During the past 4 weeks, have you accomplished less than you would like as a result of any emotional problems, such as feeling depressed or anxious’; ∗statistically significant z-score difference in comparison to the reference category within this column, at p < 0.01; ∗∗statistically significant z-score difference in comparison to the reference category within this column, at p < 0.001; ‡row percentages shown; §the standard error for this estimate represents 25-50% of the estimate value; ¶reference category; NA, not applicable; NS, not significant.
Work care reported by people with ICD-10 anxiety disorders aged 15-64 years compared to people without disability or long-term health conditions. Prevalence estimates and (standard errors) per 10 000 people aged 15-64 years
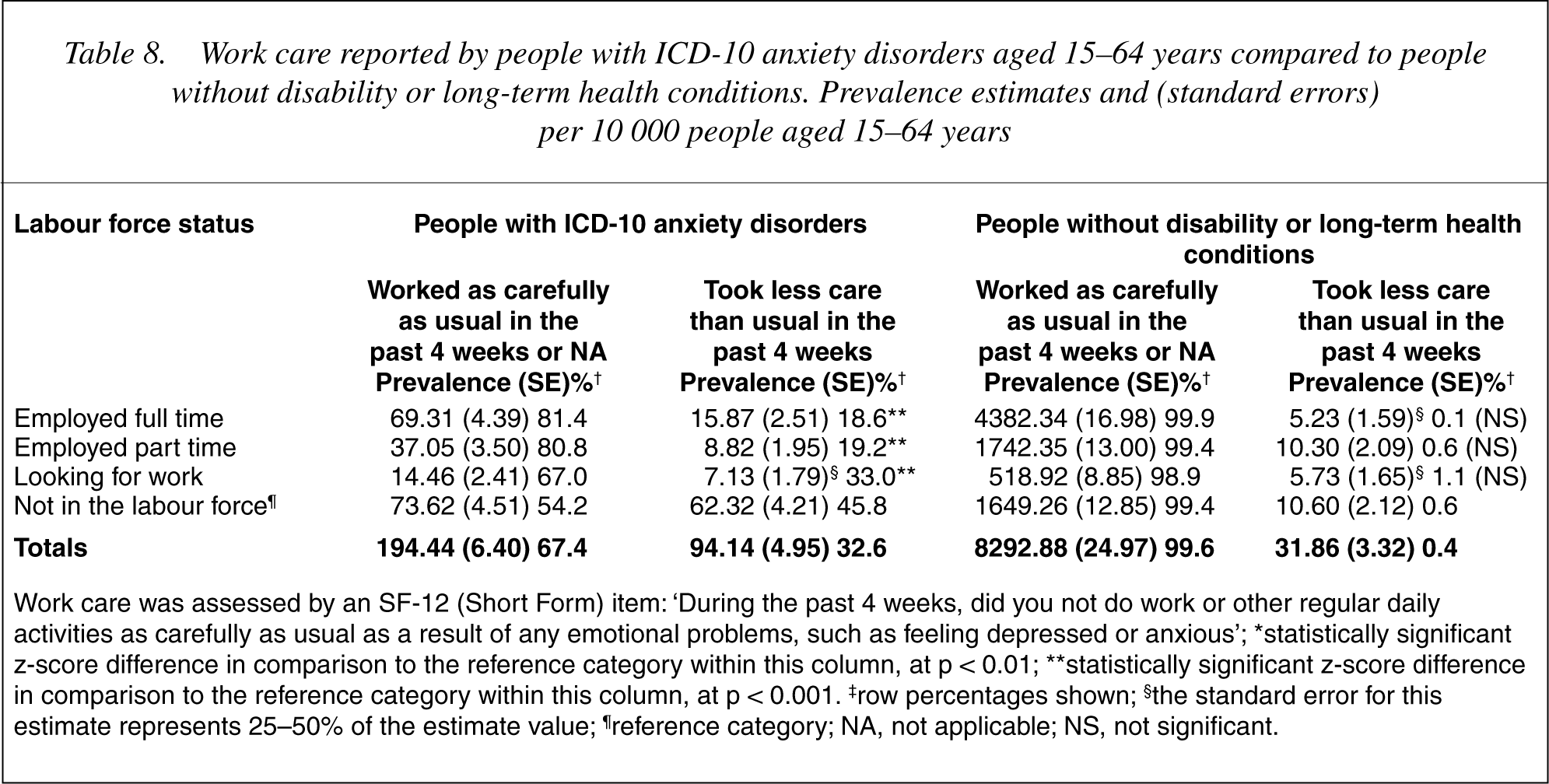
Work care was assessed by an SF-12 (Short Form) item: ‘During the past 4 weeks, did you not do work or other regular daily activities as carefully as usual as a result of any emotional problems, such as feeling depressed or anxious’; ∗statistically significant z-score difference in comparison to the reference category within this column, at p < 0.01; ∗∗statistically significant z-score difference in comparison to the reference category within this column, at p < 0.001. ‡row percentages shown; §the standard error for this estimate represents 25-50% of the estimate value; ¶reference category; NA, not applicable; NS, not significant.
Mental health treatment received
Mental health treatment was assessed among the 56.6% of people with anxiety disorders aged 15–64 years who specifically stated they had a nervous or emotional condition. Of those, 59.1% reported receiving treatment for that condition while 40.9% did not. Among the 1.3% of controls who reported a short-term nervous or emotional condition, 66.8% reported receiving treatment, and 33.2% (p < 0.001) reported not receiving treatment. Among those with anxiety disorders, receiving treatment was associated with females (60.8% vs 56.5%, p < 0.001), labour force status (p < 0.001 for all comparisons), and was not associated with severity of employment restrictions (severe to profound 60.1%, mild to moderate 59.5%, no restrictions 57.5%). More people receiving treatment for anxiety disorders were not in the labour force (62.9% vs 37.1%), employed full time (57.3% vs 42.7%), and employed part time (54.1% vs 45.9%), while fewer were looking for work (45.0% vs 55.0%). Among controls a similar pattern emerged. More control females and fewer control males received treatment (control females 72.1%, anxious females 60.8%; control males 54.5%, males with anxiety disorders 56.5%).
Discussion
Survey responses
The survey response rate of 93–94.4% exceeded that of similar population surveys, including the 78.1% response rate obtained by the National Survey of Mental Health and Wellbeing (NSMHWB) [4], [5]. Other related population surveys include the Epidemiological Catchment Area (ECA) study [24], 76% response rate, the National Comorbidity Survey (NCS, [6] 80%), and the National Psychiatric Morbidity Surveys of Great Britain [25] 79.4%. High response rates avoid bias because the prevalence of mental disorders is known to be higher among-non-responders than among people who first agree to participate [6].
The prevalence of anxiety disorders
An estimated 361 326, or 2.9% of working age Australians were found to have a primary ICD-10 classified anxiety disorder of at least 6 months duration. Anxiety disorders were similarly distributed in the SDAC 98 and NSMHWB by sex, and to a lesser extent by age (NSMHWB males 36.2%, females 63.8%; SDAC 98 males 38.0%, females 62.0%). Similar prevalence peaks were found at 45–54 years, and a common prevalence decline at 55–64 years. The SDAC 98 prevalence estimate at age 15–24 years was lower than the NSMHWB estimate (see Table 1). However, due to the use of a different age range in the NSMHWB (18–24 years) these data were not directly comparable.
Age and anxiety prevalence
Although anxiety prevalence estimates in the SDAC 98 declined from age 45–54 years to 55–64 years, the prevalence of people without disability or long-term health conditions (see column 6 of 4] anxiety disorders expressed as a ratio of the nondisabled population, increased monotonically across age groups.
Discrepancies in prevalence estimates
Much of the discrepancy in overall anxiety prevalence estimates between the SDAC 98 and other population surveys is accounted for by the different purpose, scope and methods of each. For instance the NSMHWB targeted the prevalence of adult mental disorders using a household sample of 10 600 people aged 18 years or over and estimated 12 month prevalence using a diagnostic screening tool, the CIDI-A [26] along with ICD10 and DSM-IV classifications [27]. This method is likely to be more sensitive than the self-report/third person application of the ICD-10 classification system by lay interviewers using computer assisted interviews. In addition, anxiety comorbid with depression was excluded. When differences in anxiety specification are taken into account, SDAC 98 estimates remain below yet are broadly comparable to other population surveys. The similarity of age and sex profiles indicate a degree of convergent validity.
Anxiety disorders and career development
Anxiety disorders appeared to impact on career development both directly through the production of employment restrictions, and indirectly through education disruption. This result is broadly consistent with findings in respect to a range of mental disorders [4], [15], [28], [29]. Among those employed, anxiety disorders appeared to impair career progression because formal study was seldom undertaken simultaneously with part time or full time employment. In addition, anxiety disorders were associated with considerable career truncation (see Table 1).
Predicting the labour force consequences of anxiety disorders
The structural model [14] successfully predicted that proportionally more people with anxiety disorders: were not in the labour force; relied on Government income support; had truncated careers; were not employed full time; and had difficulty with work accomplishment and care taken at work. However, the model did not predict the more complex associations with part time employment, hours of employment and modes of employment. Although the major economic consequence of reduced labour force participation was predicted, the decline in participation over the working life and the exodus at age 55 years were not.
A majority (59.1%) of people with anxiety disorders reported receiving treatment. Although more encouraging than the 28% who reported receiving treatment in the NSMHWB [4], [5] this is a promising area for further investigation. As expected, employment restrictions were associated with less part time and less full time employment. However, receiving treatment was not associated with reduced employment restrictions. Receiving treatment was linked to improved part time and full time employment, however, a stronger association emerged with respect to not participating in the labour force.
Possible explanations include: (i) that few treatments are effective; (ii) treatment does not reduce employment restrictions; (iii) beneficial effects are not sustained; (iv) those not currently in treatment previously received effective treatment; and (v) those not in the labour force are more likely to seek treatment. Distinguishing among these explanations is beyond the scope of this crosssectional survey and represents another promising area for further research. Nevertheless, the absence of the expected treatment effect suggests that treatment alone is unlikely to improve employment outcomes for people with anxiety disorders unless employment capacity is also improved. This suggestion is congruent with anecdotal evidence in vocational rehabilitation that treatment is most effective when coordinated within a rehabilitation plan to target specific employment restrictions and assistance needs.
Utilizing labour force resources
Scope exists to increase the labour force participation of people with anxiety disorders. For instance, if optimal evidence based treatment were available and a conservative 50% to a maximum 90% [8], [9] respond sufficiently in order to participate in vocational rehabilitation, then demand for labour force participation could increase to 40–72% of controls (50–90% of the 80% participation rate among controls). Hence, from Table 1, 48 840–87 907 people may benefit from appropriate assistance. Furthermore, if the SDAC 98 under estimates the prevalence of anxiety disorders by as much as 2.6 times as the comparison with the NSMHWB indicates, 126 984–228 556 people with anxiety disorders may benefit from appropriate assistance.
In line with OECD recommendations [30] there is also scope to increase participation among the 42.7% of healthy controls aged 55–64 years who were-non-participants in the labour force. Increasing participation by this age group to the same level as controls overall (80%) could engage a further 235 675 people.
Strategies to increase Australian labour force participation
The OECD supports existing government strategies to increase labour force participation, including: reducing workplace age discrimination; reducing superannuation, private pension, and Government income support incentives for early retirement; increasing secondary school completion; providing more equitable access to vocational and higher education; improving the work capacity of people with disabilities; tightening the eligibility requirements for Disability Support Pension; providing a differential fee structure in the Job Network (a contestable employment placement market); and linking Job Network assistance to other welfare programs.
Yet more specific strategies appear needed for people with anxiety disorders. For non-labour force participants, increasing the use of evidence based treatments colinked to income support arrangements and tailored vocational assistance may be needed. Restoring education disruption may require specialized programs and improved access to secondary education, vocational training and higher education. It may be necessary to review eligibility criteria for publicly funded disability employment, vocational rehabilitation, and more intensive Job Network services. As anxiety disorders can produce high levels of disability and employment restrictions, vocational professionals could be trained in routine screening for anxiety and related disorders, and encouraged to obtain evidence-based treatment [8] and specialized vocational rehabilitation for clients with more severe employment restrictions [31].
For those already employed, the feasibility of workplace screening and treatment warrants investigation. In addition, work place accommodations and support [32], [33] may improve work performance. Scope for this is indicated by the proportion of employed people with anxiety disorders who flagged difficulties with work accomplishment and work care (see Tables 7,8).
Limitations
This study has several important limitations. Through methodological differences in anxiety specifications and classification protocols, these findings are not easily compared to other population surveys. The study was limited by the use of ICD-10 classifications by lay interviewers, a necessary method given the large scale nature of the survey, but less rigorous and with relatively unknown reliability and validity compared to standardized screening or diagnostic interviews. As mental disorders were not the primary focus of the SDAC 98, not all relevant population sub groups were included in the sampling strategy. Prisoners, indigenous communities, residents of psychiatric institutions, and homeless people were not specifically targeted. Limited information was available on the type and nature of treatment provided, and on the nature of employment assistance obtained. In addition, as the focus of this analysis was descriptive, multivariate methods investigating the relative strengths of individual correlates and their interactions were deferred to a subsequent investigation. These limitations were offset by a large and representative community sample characterized by multiple vocational variables which will provide useful reference points for subsequent surveys.
Conclusions
People with anxiety disorders not participating in the labour force represent an under-utilized community resource and may increase the burden on community health services and income support programs. Individuals may need more effective treatments linked to assistance with completing education and training, joining or rejoining the workforce, developing career pathways, remaining in the workforce, and sustaining work performance. The case for providing this assistance is strengthened by contemporary OECD and Government concern for ageing populations, and increasing demands for skilled labour. Such assistance may reduce the burden on both individuals and the community and help meet the challenge of ageing populations.
Less clear however, are the precise policy initiatives needed to increase and maintain labour force participation by people with anxiety disorders. In the meantime, clinicians can encourage participation in effective treatments and in suitably intensive forms of vocational assistance. Vocational professionals can help by routinely screening for anxiety disorders and by assessing the extent of employment restrictions to avoid under or over estimating assistance needs. Policy makers in health, income support, labour market, disability employment, and vocational rehabilitation, can contribute to a whole of Government approach by collectively reviewing existing programs to improve the inclusion and retention of people with anxiety disorders. Trial innovative programs may be needed to explore and comprehensively evaluate alternative, specialized, or more coordinated approaches to service delivery.