
Abstract
The corpus callosum (CC) is the largest white matter tract in the brain, and serves as its major interhemispheric commissure, integrating information from the two cerebral hemispheres to facilitate language, affective and sensorimotor function. The CC is a brain region of great relevance to neuropsychiatric disorders, because its maturation through increased myelination through the second and third decades [1] coincides with the onset of major psychiatric illness, in that three-quarters of lifetime mental disorders have had their onset by the middle of the third decade [2]. The role of increased interhemispheric connectivity mediated by the CC is to allow for high-level integration of specialized cortical regions in each hemisphere; and the rapid and efficient transfer of information across the callosum plays an important role in attention, language and memory [3]. Impairments in these functions are frequently present at the onset of major mental disorders, including bipolar disorder, and impaired efficiency of information transfer between hemispheres has been suggested to underlie cognitive impairment in bipolar patients [4]. Because efficiency of information transfer as measured by interhemispheric transfer time (IHTT) is positively correlated with measures of macrostructural and microstructural integrity of the callosum [5], alterations in the integrity of the CC may be an indicator of cognitive and other changes in bipolar illness. Additionally, the intimate association between morphological changes in the callosum and cortical regions suggests that changes seen in grey matter regions in bipolar patients may be reflected in morphological changes to the CC.
Early studies of the structure of the CC in bipolar disorder using measures of overall callosal size produced conflicting results [6, 7], although more recent analyses that have divided the callosum into anatomically meaningful regions have suggested subtle regional reductions in both anterior and posterior callosal regions in both first-episode and established adult patients [8, 9], although not in paediatric patients [10]. Reductions in signal intensity, a sensitive index of myelination, have also been reported in the same regions in adult bipolar patients [11], and reduced callosal length in adult bipolar patients was reported in a single study in the absence of other changes [6]. Given that the CC carries hundreds of millions of myelinated axons connecting homotopic cortical regions, it is possible that relatively crude analyses that do not look for subtle regional changes in this illness may fail to detect true differences, which may be lost when more global measures are examined. Additionally, previous studies have tended to examine only a limited number of callosal variables, with most focusing on global and regional area alone and few studies have examined other callosal variables such as length, curvature or shape in bipolar patients. Furthermore, no other studies have examined regional thickness measures of the CC in bipolar disorder. Given that abnormalities of regional thickness have been described in a number of major mental disorders including schizophrenia, examining this aspect of the CC in bipolar disorder patients would seem warranted to detect subtle regional changes. No previous study has examined the role of psychosis, which could be seen to be a potentially significant modifier of brain structure if psychotic bipolar disorder is, as has been suggested, more similar to schizophrenia than non-psychotic bipolar illness [12]. Finally, bipolar patients with a family history of affective illness may show more significant changes in prefrontal cortical volumes [13], and it could be expected that these changes may be intimately associated with interhemispheric fibres that connect these two regions in the genu of the callosum.
The aim of the present magnetic resonance imaging (MRI) study was to examine regional transverse thickness in addition to measures of callosal area, length and curvature to detect the presence of subtle regional differences in the structure of the CC in a group of patients with established bipolar disorder (n = 24) compared to matched controls (n = 24). In addition to measures of overall and regional callosal area, we also measured callosal length, curvature and regional thickness of the callosum. We sought to compare those patients with and without psychosis, and those with and without a family history of mood disorders, in addition to examining the effect of duration of illness on thickness variables. We hypothesized that bipolar patients would show thickness reductions in anterior and posterior callosal regions corresponding to the region of the genu and isthmus, given that previous work has shown reductions in area in these zones [8, 9]. We also expected psychotic patients to differ from non-psychotic patients, particularly in the genu and isthmus, regions that we have shown to be significantly reduced in schizophrenia [14, 15], and that those patients with a positive family history would differ from those without in anterior regions connecting prefrontal cortical regions.
Method
Subjects
The sample consisted of 24 patients with DSM-IV bipolar I disorder and 24 matched healthy controls. Patients were recruited from a specialist mood disorders clinic and through local advertisement in Sydney, Australia. Diagnoses were made by a research psychiatrist (GM) using the Structured Clinical Interview for DSM-IV (SCID-IV-P), supplemented by case-note review. Patients who had at least one first-degree relative with an affective disorder were defined as having a positive family history. Subjects were defined as having bipolar disorder with a history of psychosis if hallucinations and/or delusions had occurred during at least one affective episode. Controls were recruited via advertisement and matched for age and education. They were screened for a personal and family history of psychiatric or neurological disorder using the SCIP-NP. Participants were excluded if they had a history of ongoing substance misuse, neurological disease or, in patients, a comorbid Axis I or II DSM-IV diagnosis requiring treatment. Three patients had a family history of bipolar disorder, two had a family history of both bipolar disorder and unipolar depression, and five had a family history of unipolar depression only. Eleven patients had no family history of affective illness, and three had an unknown family illness history. Eight patients were taking lithium at the time of scanning, six were taking valproate, and four were taking a combination of both. One was taking valproate and carbamazepine and one was taking carbamazepine alone, while four patients were medication free at the time of scanning. All patients had previously been exposed to antipsychotic medication, although none within 12 months of entering the study. All participants provided written, informed consent prior to participating and the study was approved by the local hospital and university ethics committees.
Magnetic resonance scanning acquisition and analysis
Scans were acquired on a 1.5 T GE Signa scanner located at St George Hospital, Sydney, New South Wales, Australia. Imaging parameters were: echo time (TE), 5.3 ms; Repetition time (TR), 12.2 ms; field of view, 24.9 cm; voxel dimensions, 0.977×0.977×1.6 mm-thick coronal slices. All MRI data were transferred from CD to a Linux workstation and coded to ensure participant confidentiality and blinded image processing and assessment.
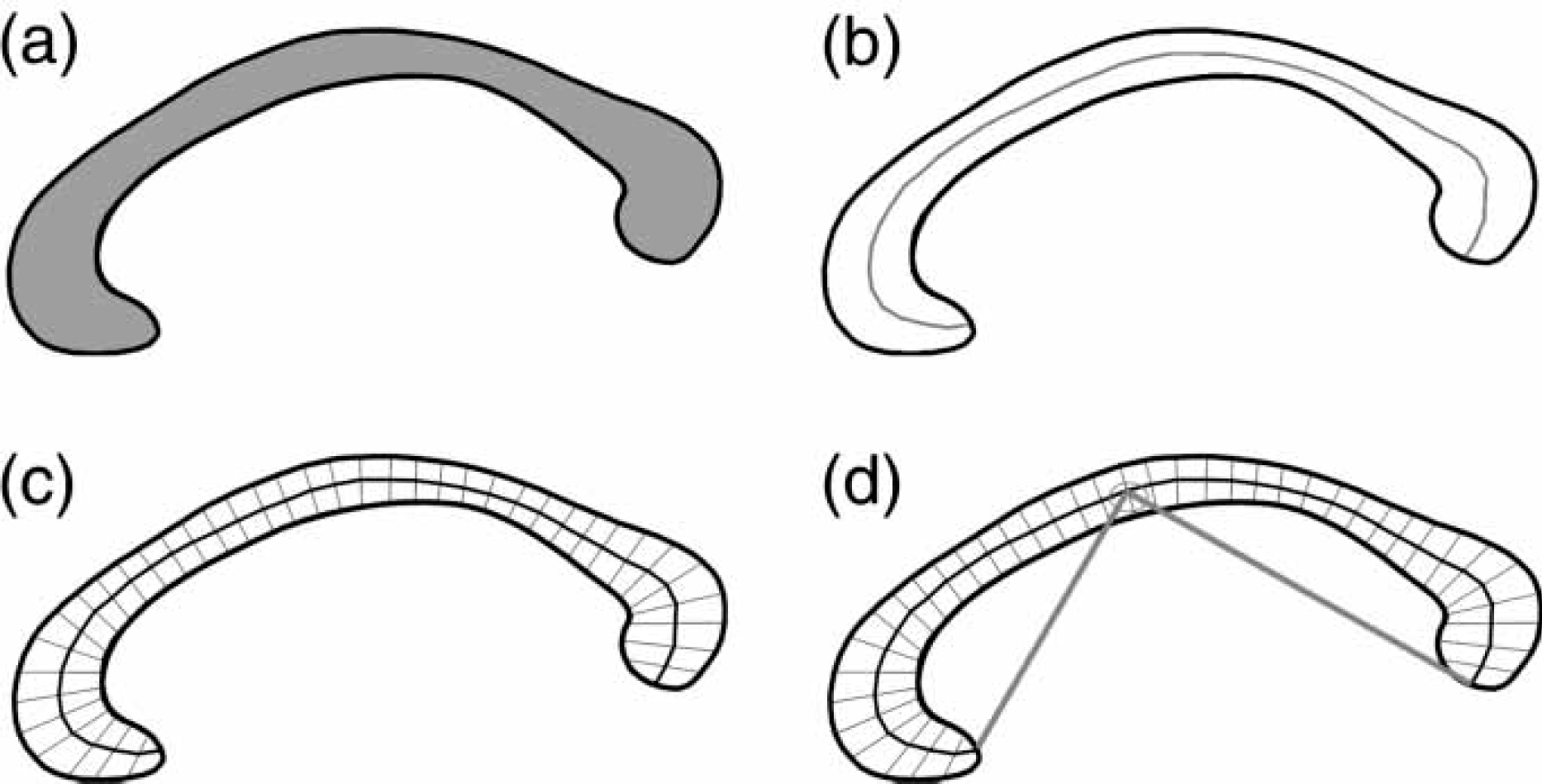
Image processing used in the present study has been previously described [16]. In brief, after segmenting the brain from non-brain tissues, images were registered using a nine-parameter linear transformation to a template image consisting of the average of 152 normal T1-weighted MRI scans previously placed in stereotaxic coordinate space. The midsagittal slice was identified and interpolated to a voxel dimension of 0.5 mm×0.5 mm in the y and z planes, and white matter voxels in the midsagittal slice were identified using histogram segmentation. Non-callosal voxels were then removed manually. A measure of callosal area in total mm2 in stereotaxic space was then generated. To measure regional callosal thickness, voxels at the edge of the callosum were identified and upper and lower edges were defined according to anterior and posterior end-points. An iterative search for optimum end-points that maximized the length of a line segment traversing the centre of the callosum was then performed (Figure 1). The line segment was defined by dividing the upper and lower surfaces of the callosum into 40 equidistant portions by 39 nodes. The midpoints between corresponding nodes on the upper and lower surfaces were identified. The line segment was created by joining end-points and successive midpoints. Once the optimum end-points and corresponding midpoints were identified, a smooth curve joining them was obtained with cubic spline interpolation, and the anteroposterior length of this curve was measured (callosal length). This curve was divided into 40 segments of equal lengths by 39 nodes. At each node, the line orthogonal to the curve was calculated. The distance between its intersection with the dorsal and ventral surfaces of the callosum represented regional callosal thickness at these 39 points. The mean of these thicknesses across the callosum was generated as mean callosal thickness. Finally, a simple measure of curvature, the callosal bending angle, was obtained by measuring the angle between two vectors, each joining each end-point of the callosum to the midpoint, along the mid-spline of the callosum. The main callosal metric types are illustrated in Figure 2.
Extraction of the corpus callosum from mid-sagittal image. (a) Mid-sagittal callosal image; (b) binarized callosal image; (c) mid-spline traversing callosum between two end-points and callosal thicknesses orthogonal to equidistant points alone the mid-spline. Callosal metrics. (a) Total callosal area; (b) length of callosal mid-spline; (c) 39 individual thickness measures perpendicular to mid-callosal spline; (d) callosal bending angle.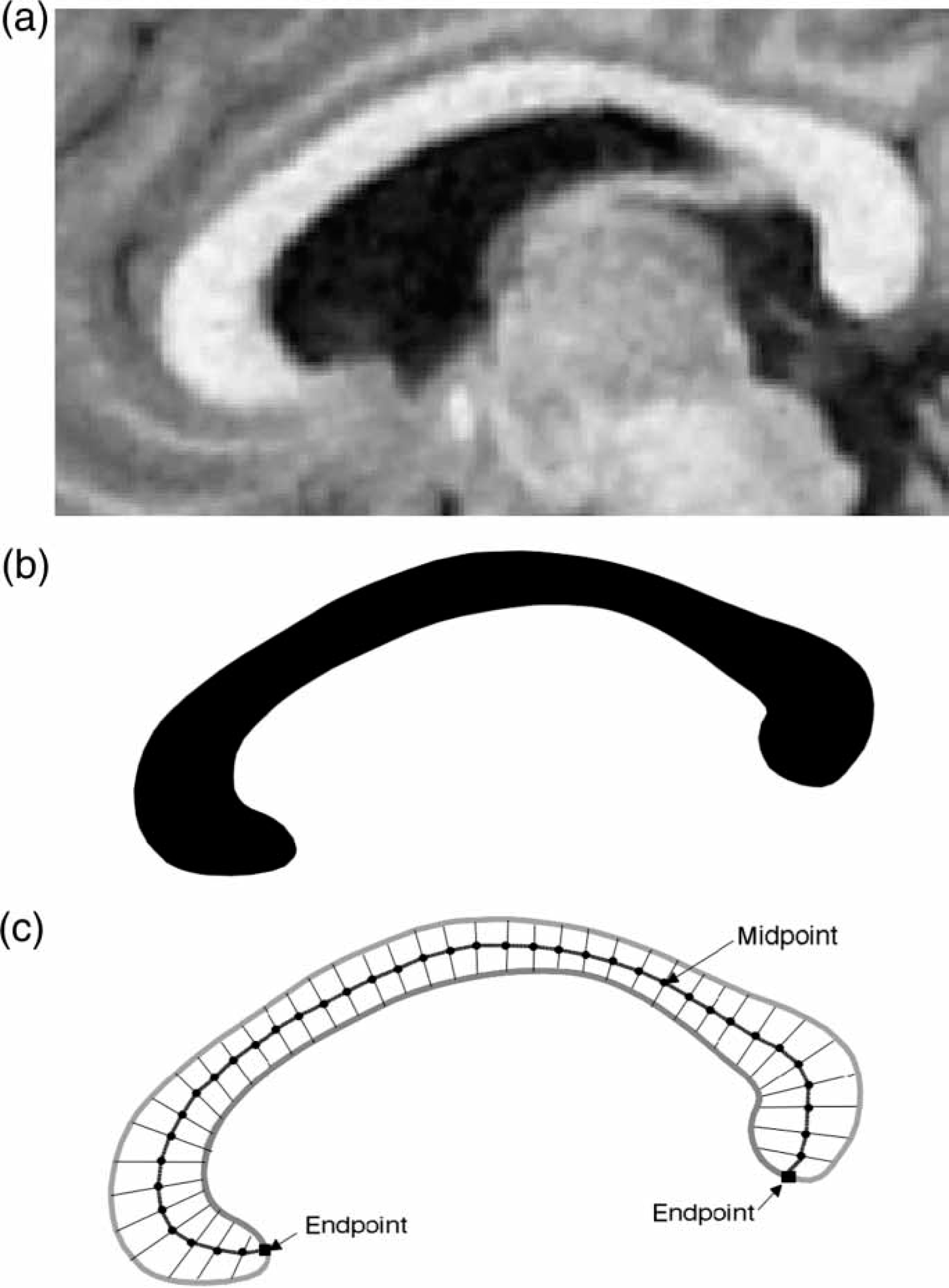
Statistical analysis
Analysis for between-group differences in demographic variables was undertaken with independent t-tests for age in years, years of education, and premorbid IQ measured using the National Adult Reading Test. Unitary callosal measures such as total callosal area, callosal length, mean callosal thickness and callosal bending angle were compared between groups using t-tests. For regional callosal thickness, a non-parametric permutation method of 20 000 randomizations was used for all group comparisons to examine for an effect of group, to account for non-independence between adjacent thickness measurements and for multiple comparisons [17]. Step-down t-testing to determine which regions showed significant change was planned to localize between-group differences in regional callosal thickness. Non-parametric regression analyses using multiple dependent variables were undertaken to determine the effect of duration of illness on regional thickness. Statistical inference was based on the method of Holm, which controls for multiple comparisons of non-independent measures by controlling the family-wise error rate without assuming independence [18].
Results
Subject characteristics
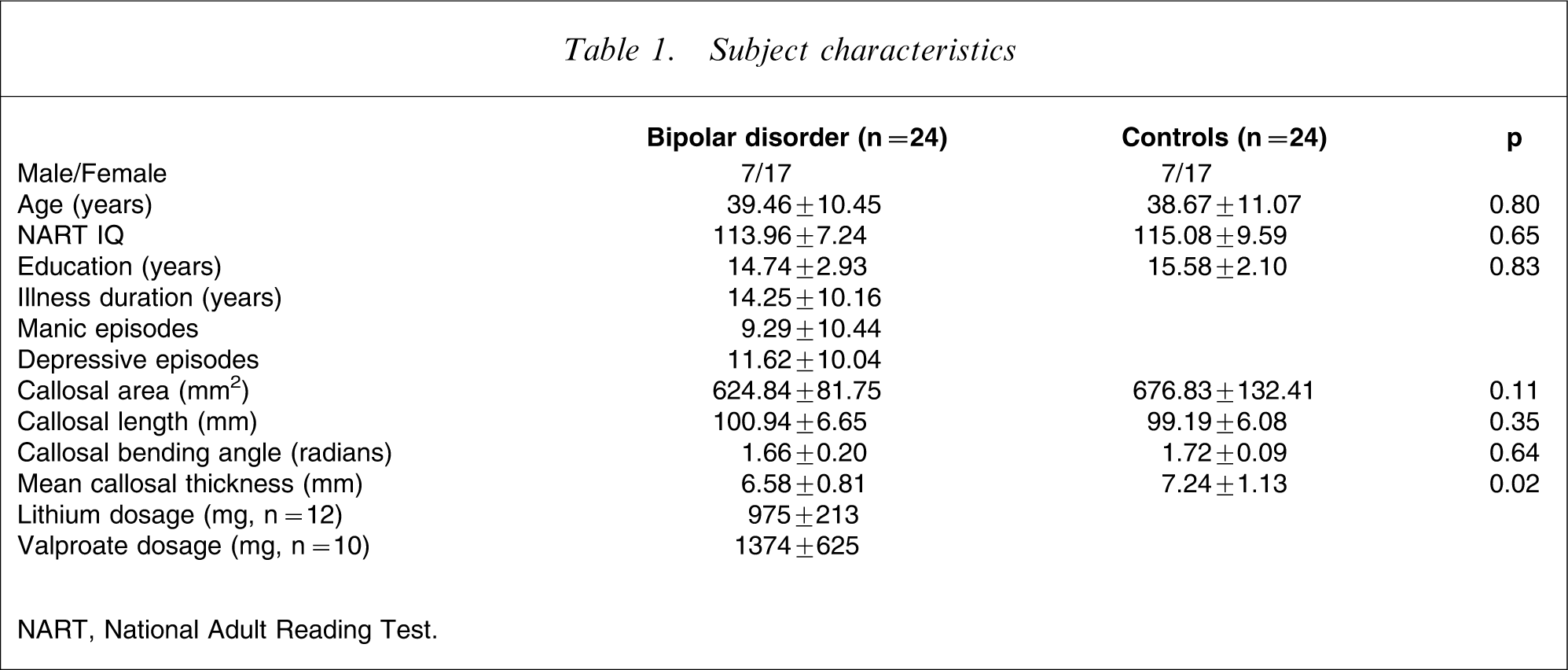
NART, National Adult Reading Test.
When known psychotic (n = 10) and known non-psychotic (n = 11) bipolar patients were compared, there were no differences on measures of total area (t = −0.32, p = 0.75), length (t = 3.67, p = 0.72), mean thickness (t = −0.41, p = 0.69) or curvature (t = 0.43, p = 0.67). When those patients with a known family history of major affective illness (n = 10) were compared with those known to have no affected family members (n = 10), patients with a family history had a significantly larger total area (t = −2.52, p < 0.05) and a trend towards a longer callosum (t = −1.74, p = 0.09) but no difference in curvature (t = 1.01, p = 0.33) or mean thickness (t = −1.43, p = 0.17). Age, duration of illness, dosage of lithium or valproate, or number of past manic or depressive episodes did not significantly correlate with any main callosal measure.
When regional callosal thickness was analysed (Figure 3), an overall effect of group was found, with the bipolar group having a significantly thinner callosum in all regions (p < 0.05). When localizing shape differences beyond the global group effect, significant reductions were found in the bipolar group in nodes 38 and 39 in the splenium, each significant at the p < 0.05 level (Figure 4). There were no between-group differences in regional thickness between psychotic and non-psychotic bipolar patients (p = 0.55), nor between those patients with and without a family history of major affective illness (p = 0.37). Duration of illness was not predictive of regional callosal thickness (p = 0.11).
Callosal slice means from slice 1 (genu) to 39 (splenium) in the ( Callosal significance map, showing significant between-group changes in slices at the splenium of the callosum.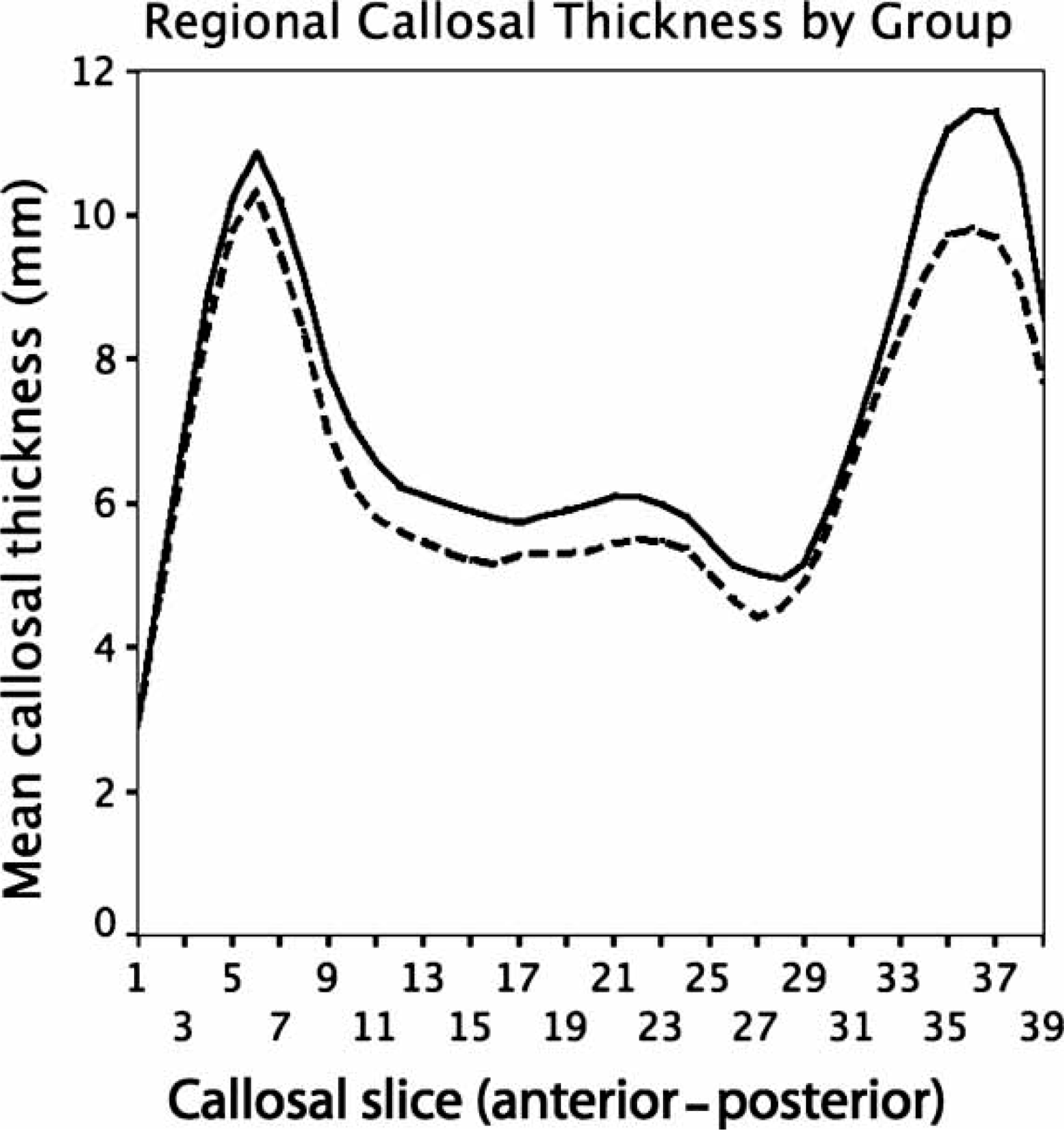

Discussion
By combining a variety of callosal metrics, we were able to show that although there are no significant size differences between bipolar patients and controls, there are significant shape changes in this patient group, with a globally thinner callosum and regional reductions at the level of the splenium when compared to controls matched carefully for age, gender, education and premorbid IQ. That these differences at the level of thickness were not seen significantly in global measures of callosal size (area, length and curvature), suggests that global measures may not be sensitive enough to detect what may be subtle changes in shape.
That the bipolar patients demonstrated a thinner callosum as a whole suggests that these volumetric changes may be reflective of a diffuse process affecting the brain, rather than of local changes at a cortical level. The relationship between changes in white and grey matter compartments in major mental disorders is probably bi-directional, and reductions in white matter structures may reflect a primary pathology of white matter, be secondary to grey matter structural change, or a process affecting both [19]. A thinner callosum in bipolar patients may reflect fewer interhemispheric axons, reduced axonal size, or impairments to myelination [19]. Some evidence suggests that reduced size of the callosum in bipolar disorder may be associated with reduced signal intensity, suggesting impairments to myelination [11] or alterations to the maturation of the axonal cytoskeleton in these fibres [20]. Because the onset of the illness occurs during this period of early adulthood interhemispheric myelination, it is possible that any process that impairs or interrupts this may result in these findings, although it is equally plausible that these changes are the result of a reduced number of interhemispheric fibres and thus may have pre-dated the onset of the illness. Regional area reductions in the callosum appear to be present at the first episode [9], and match those seen in established illness [8], suggesting that this process is already under way or has already occurred at the time of first presentation. Grey matter changes have been described in this sample, with voxel-based morphometry demonstrating alterations in medial and lateral temporal cortex [21], and cortical thickness analysis demonstrating bilateral paracingulate thickness reductions [22], suggesting that the callosal changes described may be occurring in concert with alterations to cortical regions.
Accompanying this globally thinner callosum is an apparent disproportionate reduction in thickness at the level of the posterior splenium. This finding diverges from those of studies of a similar sample group, in which a global size reduction was present but regional reductions were found in the anterior two-thirds of the callosum only in first-episode and established illness [8, 9]. Findings of a regionally thinner splenium in the present sample appear similar to the findings of a reduced circularity of the splenium in an adolescent sample [10], although that group did not show other regional reductions nor a global reduction; conversely, the same methodology did not find reduced splenial circularity in an adult sample group but found global and anterior reductions [8]. Size and shape changes do occur in the posterior callosum in the adolescent period, with a disproportionately greater expansion of mid-sagittal area occurring in the splenium in adolescence, suggestive of a more pronounced development of interhemispheric connections between association areas [23]. Given this, a process that interrupts or impairs neurodevelopmental processes during this period could be expected to cause disproportionate changes to the posterior callosum, which are apparent in the present sample.
The differences between the present findings and those previously described may also relate to the sample group studied. The present sample size is, however, comparable to or larger than other reported cohorts; the patients have a similar mean duration of illness; and, like other studies, the DSM-IV diagnosis was based on standard structured interview using the SCID-IV. One potential point of divergence is medication usage, because lithium therapy is reported to have trophic effects on grey matter structures, which are detectable on group-level MRI analysis [24]. The present patient was much more heterogeneous as regards medication than two comparable studies, the patients in which were primarily on lithium monotherapy [8, 11], although a study of medication-naïve first-episode patients showed anterior reductions [9]. If lithium does indeed result in subtle grey matter volume increases (which may be reflected in subtle regional shape changes in the callosum), a lower level of lithium usage in our population as a whole may reduce any potential modulating effect that lithium may have on any illness process that results in volumetric reductions in the CC.
The lack of effect of psychotic symptoms on these morphological changes argues against the notion that psychotic bipolar disorder shares more neurobiological underpinnings with schizophrenia than it does non-psychotic bipolar disorder [12]. These results, however, need to be interpreted cautiously because of the modest numbers in each group, and examining a larger sample is warranted. What is notable is the significant difference between patients with a family history of mood disorders and those without, with patients with a positive family history having a significantly and unexpectedly larger callosal area and a trend towards a longer callosum. Although mean and regional thickness did not show an overall effect of group, the means of each are greater in the group with a positive family history, suggesting that there may be separate processes occurring in patients with and without a family history of mood disorders. Mood disorder familiarity in bipolar patients has been consistently associated with reductions in the anterior cingulate region [25], although the only white matter structural change previously associated with genetic risk has been reductions in left frontotemporal white matter [25]. Similar reductions have been seen in monozygotic bipolar twins [26]. In healthy individuals, cerebral lateralization results in a greater white matter volume in the left hemisphere [27], and thus left hemispheric reductions in patients with a family history could indicate altered laterality in this group. Because an inverse correlation exists between laterality and callosal size [28, 29], it may be that these bipolar patients have a genetically driven alteration to lateralization, which may not be seen in those without a family history of affective illness, and which results in a larger callosal area than non-familial patients. But the small numbers under study – particularly given that those with a family history of depression and manic episodes are conflated into one group – necessarily limit the conclusions that can be drawn.
Duration of illness was not associated with any callosal measure in the present study, and no previous study has examined this illness variable in relation to callosal size and shape. Illness duration has been correlated both positively and negatively with grey matter volume in bipolar disorder [30, 31]. In a voxel-based analysis of this sample, duration of illness only negatively correlated with caudate volume but no cortical region [21]. Given that there is significant variance in this illness variable in the sample under study, it is suggestive that the changes seen either pre-dated or occurred at the time of first episode of bipolar affective illness. This is consistent with the almost identical findings when the methodology of Keshavan et al.[20] is applied to both first-episode and established bipolar patients [8, 9], although longitudinal studies from the pre-illness phase would be required to demonstrate this conclusively.
The present analysis of callosal size and shape in bipolar disorder differs from other studies in this field in two chief ways. Most other studies examining callosal structure in bipolar disorder compared differing callosal regions without taking into account the non-independence of adjacent callosal measures, and have not corrected for multiple comparisons of the same structure [8, 10, 11], whereas only one study has used a Bonferroni correction [9]. Utilization of a non-parametric permutation method with step-down procedures statistically controls for multiple comparisons and the non-independence of adjacent callosal regions, thus minimizing false-positive findings. Additionally, the use of a nine-parameter transformation to a standard template on all images, rather than covarying for brain size, is unique to the present study, and it could be suggested that this may minimize subtle differences between the two groups. The use of brain volume as a covariate, however, does not account for the fact that the relationship between brain and callosal size may vary between sexes, whereas the use of normalization into stereotaxic space, as applied in the present study, more directly deals with gross brain size differences and ensures robust and consistent measurement in the mid-sagittal plane, particularly in mixed-gender samples [32]. Additionally, the image processing methodology and non-parametric permutation analysis has demonstrated subtle regional changes in pre-psychotic, first-episode and established schizophrenia in large cohorts using identical callosal metrics [15, 16].
Limitations
The limitations of volumetric analysis in examining white matter structures in mental illness are also worth acknowledging, and it may be that this type of analysis lacks the spatial resolution and thus sensitivity to detect microstructural change. In the schizophrenia literature, two decades of callosal size and shape analysis has produced an irresolute body of work, suggestive of but not conclusive for both subtle global and regional reductions in callosal size [19]. The use of MRI methodologies such as diffusion tensor imaging has allowed for the examination of in vivo microstructure of white matter in this disorder, and studies examining the callosum in schizophrenia have demonstrated significant alterations to interhemispheric connectivity in this disorder [19] that may not otherwise be detectable by volumetric measures alone. Finally, the analysis of a single structure or region in the brain in isolation may provide clues about neurobiological processes, but without comparable metrics of other, related brain regions, it can be difficult to place these changes in a whole-brain context, which is important in major mental disorders where illness processes are unlikely to be focal. Finally, the limited sample size limits the conclusions that can be drawn from subgroup analyses, and future analyses of much larger cohorts are required to more clearly define the effect of comorbid illness variables on callosal shape in bipolar disorder.
Conclusion
The present study of bipolar I disorder patients has demonstrated that this population has a significantly thinner CC, particularly in the region of the splenium, than age- and gender-matched healthy subjects. These changes may be the result of widespread impairments to late myelination, or be reflective of subtle grey matter changes in this disorder. To resolve the role of the CC in bipolar disorder, imaging methodologies that go beyond volumetric analysis of a single structure are warranted.
Footnotes
Acknowledgements
Dr Walterfang was supported by a Pfizer Neuroscience Research Grant and a Stanley Research Centre Grant. Professor Malhi was supported by an NHMRC Program Grant (510135) and an Australian Rotary Research Grant. Dr Wood was supported by an NHMRC Clinical Research Training Fellowship (251755). Dr Yücel is supported by an NHMRC Clinical Career Development Award (I.D. 509345). Neuroimaging analysis was facilitated by the Neuropsychiatry Imaging Laboratory managed by Ms Bridget Soulsby at the Melbourne Neuropsychiatry Centre and supported by Neurosciences Victoria. The authors also thank Dr Christopher Adamson for his assistance in generating callosal significance maps.