
Abstract
Boundary issues involving professionals and their patients are encountered frequently and present significant challenges to those working in professional settings. These issues may be particularly pronounced in rural and smaller communities as a function of the relatively limited population numbers that characterize those communities [1], [2]. Because there are fewer relationship options, individuals are likely to occupy several roles or role levels and encounter each other in a number of different situations. Unavoidable relationship overlap and greater interdependence among individuals are fundamental aspects of the social norms inherent within smaller communities and may occur at personal, business or other professional levels.
Within the mental health field, the ethics of these socalled dual or multiple relationships assume increased concern [3–5]. It is widely recognized that multiple relationships may affect a patient's ability to develop an open and trusting relationship with a professional, impair clinical judgement or result in other harmful practices [6]. As noted by Roberts et al.: ‘Rural clinicians… naturally function in a context of overlapping relationships, potentially conflicting roles, and altered therapeutic boundaries, which may be riddled with ethical problems’ [7], p. 499].
For the mental health practitioner, the inevitability of dual relationships in rural communities presents unique challenges. Little is known about how practitioners deal with these ethical grey areas, some of which appear suddenly and require an immediate response. In order for these challenges to be met, an appreciation of the nature of the multiple interacting factors – geographical, social and legal – that make up the context in which mental health care is delivered in rural communities is essential.
The aim of this paper is to provide an overview of the literature on non-sexual dual relationships and to discuss these in the context of rural mental health practice in Australia. Although much of this literature is derived from North America, we have attempted to highlight findings that are particularly relevant to clinicians practising in Australian health services. While we acknowledge that the difference between sexual and non-sexual dual relationships may not always be clear, this discussion will focus only on non-sexual dual relationships. Our focus is on ‘everyday’ dual relationships such as when a clinician interacts with a patient who is on the same sporting team, is a member of the same community group or is the teacher of their child. Throughout the paper our use of the term ‘therapy’ is not restricted to specialist or formal types of psychotherapeutic intervention; instead, we employ the term to describe a broader generic category of interventions that more closely reflects the clinical practices of rural mental health clinicians. Accordingly, our discussion is aimed at a range of professionals – nurses, social workers, psychiatrists, occupational therapists and psychologists – who deliver mental health care and whom, for ease of reading, we will refer to collectively as mental health clinicians. The present review forms part of a larger project that aims to identify key questions and issues that might inform the development of education, training and support systems relevant to dual relationship issues in rural mental health practice.
Contextual issues
There are three main features of rural communities that impact upon the capacity of mental health workers to maintain clear professional boundaries: (i) the size of a community; (ii) the isolation of a community; and (iii) community expectations.
While there is great diversity across rural communities in Australia, common elements do exist, including relative isolation and smaller population size compared with urban areas [8]. Smaller population sizes in rural communities mean that mental health service users and practitioners are more likely to have contact in social settings or interact through participation in sporting activities or community services. Unavoidable contact may also occur if a patient happens to be, for example, the local mechanic, grocer or teacher. The more remote the town, the less flexibility clinicians have for social or commercial interactions outside their community. Given the importance of public sector incomes to small rural communities [9], there may also be a community expectation, or clinicians may feel a duty to shop and support businesses within their local area. The significant population decline in some rural areas [8] may also mean that clinicians feel a responsibility to support and participate in community activities such as sporting or recreational clubs, and organizations such as the volunteer fire brigade, which contribute to social cohesion of rural towns. These conditions present unique challenges to rural mental health workers who must negotiate multiple relationships with their patients and patients' families as part of daily life. The longer a mental health worker resides in a rural community, the less likely it is that he or she will be able to completely separate professional and personal relationships.
Community expectations may not only influence where clinicians shop, socialize, or interact, but also the role they play in their community. A study by Humphreys and Fraser [10] of the health workforce in small rural and remote communities found that health workers faced community pressures to always be ‘on-duty.’ Nurses commented that they were approached in a range of settings to provide advice or receive health information about patients. A related issue involved dealing with tragedies in the community such as suicides or car accidents. Nurses felt the emotional impact of these tragedies as much as other community members but believed that there was often an unrealistic expectation for them to provide care and support.
In terms of mental health services, the common features of rural areas include fewer primary and specialist mental health practitioners [11], [12], fewer support services such as drug and alcohol services and geographically large and sparsely populated service catchment areas. Of particular significance is the issue of confidentiality. In rural settings confidentiality may be more difficult to ensure in practice, thus increasing the potential for a range of problems [13]. Strict adherence to confidentiality, on the other hand, has the potential of impacting adversely on important collaborative relationships in smaller communities.
The concept of therapeutic boundaries
In general terms boundaries imply the defining or determining of a limit. Within the interpersonal context, boundaries suggest a ‘psychological space’ or distance between individuals, one that is often used to emphasize the clinician's stance of anonymity, neutrality and objectivity. Breaching of professional boundaries refers to actions that involve going outside the limits of the therapeutic relationship. Such breaches can occur as a result of actions on the part of the clinician, the patient or both.
Adequate boundary management is a clinical imperative for which responsibility rests principally with the clinician. Its importance in the development of an effective therapeutic alliance is highlighted by Smith and Fitzpatrick [6]: ‘Proper boundaries provide a foundation for this relationship by fostering a sense of safety and the belief that the clinician will always act in the client's best interest. This foundation permits the client to develop trust in the therapist and to openly express secret fears and desires without fearing negative consequences’ [6], p. 500].
A useful distinction can be made between so-called boundary ‘violations’ and boundary ‘crossings’. The former are used to refer to ‘actions on the part of the clinician that are harmful, exploitative and in direct conflict with the preservation of clients' dignity and the integrity of therapeutic process’ [1], p. 6]. Examples include sexual or financial exploitation of patients. Within the professional, legal and broader communities there is a strong consensus that boundary violations are in no way acceptable. Boundary crossings, on the other hand, refer to benign and sometimes beneficial departures from traditional therapeutic settings or constraints. These may include such things as attending a function such as a funeral with a patient or socializing with a patient. Not all boundary crossings can be considered to be instances of dual relationships. Self-disclosure and (non-sexual) physical contact with patients are examples of the latter.
Boundaries and dual relationships
In general terms, a dual relationship is a situation in which there are two (or more) distinct kinds of relationships with the same person [14]. In the context of mental health care this may exist when a clinician has a relationship with a service user outside the context of an established professional relationship with that person; for example, where that person is a relative, employer, friend, member of the same sporting team or recreational group, or business associate.
Divergent opinions concerning the appropriateness of dual relationships in the mental health context exist and these fall broadly between two extreme positions. Opponents advocate that they are inevitably harmful and should be avoided [1], [15], [16] – the so-called ‘urban analytic risk management model’ which interprets familiarity with patients outside the clinical setting as inimical to therapeutic aims. Proponents of this position assume that any boundary crossing, no matter how trivial, inevitably leads – via a ‘slippery slope’ – to boundary violations. Strong emphasis is placed on maintaining a psychological distance from patients through rigid standards; these relate, for example, to non-disclosure of personal information by professionals and restricting contact to the professional setting alone. At its extreme, then, this view holds that boundaries between professionals and service users should never be crossed.
An alternative position emphasizes the positive value of dual relationships as a critical ingredient in therapeutic work, warning that distancing through anonymity and neutrality is not only likely to be counter-therapeutic [1], but also to increase the likelihood of exploitation [17], [18]. As noted, the unique bonds between mental health service users and professionals are heightened in small and rural communities. Parallels to this can be found in literature relating to religious, gay, military, feminist and ethnic communities [19]. In small and close-knit communities, such as rural communities, familiarity through community involvement may lessen suspicion and increase approachability [1], indirectly enhancing clinical effectiveness. For example, in their study of community nurses and domestic violence Cox et al. [20] found that the visibility of nurses allowed women who were being abused to meet with these health workers in ‘neutral’ situations such as at the football or supermarket. These opportunities allowed women to be supported by health workers without arousing the suspicions of their partner. Given the stigma attached to mental health care, it is likely that this may also be true for mental health workers.
Boundary crossings, it is argued, are likely to increase familiarity, understanding and connection, and hence the likelihood of success for the clinical work. Dual relationships and familiarity with patients, moreover, tend to decrease the probability of exploitation – not increase it – as the power differential in a more egalitarian relationship is reduced. Patients often emphasize the benefits that accrue when clinicians interact with them in the community outside the office. A fuller picture of the patient's history, family and interactions within the community gives context to patient's accounts of their lives [21].
In practice it is likely that clinicians tend mainly to operate somewhere between these two extreme positions on what might be described as the patientclinician distance spectrum. In practice there is considerable variability regarding where on the spectrum a clinician might stand. The reasons for decisionmaking are poorly understood but are likely to include: the nature and severity of the patient's problems; the clinician's background, training, and experience; and features of the treatment setting, such as private practice, multidisciplinary team, small or isolated community.
Research regarding non-sexual dual relationships is limited. However, there is evidence to suggest that controversial boundary-related activity is prevalent among mental health professionals. Pope et al. [22] for example, found that 39% of psychologists they surveyed disclosed details of personal stresses to a patient and 35% accepted a patient's invitation to a special occasion. When presented with vignettes depicting non-sexual dual relationships, Lear, cited in Campbell and Gordon [2] found that rural psychologists were more likely than non-rural ones to engage in those relationships. In their survey of community mental health workers, Perkins et al. [23] found that rural practitioners experienced more professional role boundary dilemmas and were less likely to make ethically conservative decisions than their non-rural counterparts. In a survey of psychologists, psychiatrists and social workers, Borys and Pope [24] found that respondents living and working in small towns tended to rate dual professional roles as more ethically acceptable than respondents in suburban or urban settings.
There has been very little attention directed to examining the benefits and/or problems for clinicians resulting from non-sexual dual relationships. Obvious problems include difficulty being ‘off duty’ [10] and being able to have a social life where one is not under scrutiny and expected to behave ‘as a professional’. The study conducted by Cox et al. [20] also highlighted the difficulty for workers in small towns having confidential information about people, particularly in relation to violence or abuse, who they then interact with outside the clinical setting. A clinician who knows a person socially can be placed in a difficult position when called to assess or treat them as a patient. Both the clinician and the patient may be reluctant to discuss mental health issues, cognizant of their other roles. Additional potential problems for the clinician include a conflict of interest and loss of objectivity. These factors can create stresses for workers and are likely to contribute to burnout.
Ethical codes of mental health professional bodies
The two central principles that underpin ethical codes of practice are impaired objectivity and risk of exploitation. These are explicitly referred to in the Australian Psychological Society (APS) Code of ethics [25], which highlights the need for psychologists to avoid dual relationships that could impair judgement and increase risk of harm. The APS code includes a guideline for managing professional boundaries and multiple relationships that refers to psychologists practising in small communities such as rural or ethnic communities. It acknowledges that in some situations multiple relationships are not avoidable and highlights the need for psychologists to be especially mindful of confidentiality issues. Discussion with clients and seeking advice from colleagues about ways to manage such situations are recommended.
The Royal Australian and New Zealand College of Psychiatrists' Code of ethics [26] makes no explicit reference to dual relationships nor does it identify any special issues that may be relevant to psychiatrists practising in rural or smaller communities.
In its Code of conduct for nurses in Australia, the Australian Nursing Council [27] states that a nurse must be aware that dual relationships may compromise care outcomes and always conduct professional relationships with the primary intent of benefit to the individual. The individual state Nurses Boards provide more extensive recommendations in the form of standards and guidelines. The Nurses Board of South Australia has produced a Standard for Therapeutic Relationships and Professional Boundaries [28], which highlights the need to ensure that where dual or multiple relationships exist, mechanisms are established to avoid prejudicial practices. In Professional Boundaries: Guidelines for Registered Nurses in Victoria [29], the Nurses Board of Victoria underscores the significance of dual relationship issues in nursing practice. It states: ‘The presence of dual relationships in small and isolated communities may be unavoidable. Nurses who work in these communities need to remain particularly mindful of the potential impact of dual relationships. The fact that a nurse lives in a small and isolated community does not diminish the nurse's responsibility to maintain professional boundaries’ [29], p. 2].
The inevitability of dual relationships with clients – including former clients – is also noted in the Australian Association of Social Workers' (AASW) Code of ethics [30] along with the need for members to ‘set and enforce explicit, appropriate professional boundaries to minimise the risk of conflict, exploitation or harm.’ In situations where there may be an unavoidable conflict of interest – such as may happen when working in a rural community – social workers are advised to declare this to the appropriate senior person and to seek to negotiate a solution. The code states that it may be necessary for the social worker and client(s) to acknowledge and work with such conflicts within the situation. In cases where no adequate professional support or supervision is available, the code advised contact with the AASW Branch Office or AASW National Office for assistance in accessing a support person.
The Code of ethics of The Australian Association of Occupational Therapists (OT Australia) states that OTs ‘Shall not enter into personal relationships which damage the establishment and maintenance of professional trust’ [31]. It acknowledges the possibility of therapists experiencing strong feelings toward patients and clients that may be harmful to the therapeutic relationship and advises that consideration be given to changing therapist.
While some of the codes of ethics from the mental health professional regulatory bodies acknowledge the inevitability of establishing dual relationships with patients in small communities, and the need to exercise caution in those cases, very little is offered in terms of guidance on how to manage these situations. Within smaller and rural communities, where sound ethical practice may not completely parallel the practice of professional counterparts in urban environments, this issue is of particular significance. Ethical codes or standards therefore must be seen as: ‘necessary but not sufficient when rural… psychologists [and other mental health professionals (added)] are faced with difficult ethical decisions regarding professional–personal boundaries’ [19], p. 32].
Managing dual relationships in rural and small communities
There is little published data regarding how mental health professionals manage dilemmas in terms of dual relationship issues in rural settings. One exception is an American study by Schank and Skovholt [4] in which psychologists who lived and practised in rural areas and small communities were interviewed about the ethical dilemmas they faced in their daily practice. These authors found that decisions about who to see as patients were based on three different criteria. For some, the decision was based on their own comfort level as to whether they could successfully manage overlapping relationships with particular patients. Others involved prospective patients in the decision-making process. The third group used type and severity of patients' presenting problems as indicators of whether they would enter into overlapping relationships. Among the latter, some were more likely to see patients for situations requiring problem-solving or advice-giving but not those with a possible diagnosis of personality disorder. Most of the psychologists interviewed spoke directly with their patients about the likelihood of out-of-therapy contact, making it clear that patient privacy would be respected by waiting to see if patients wanted to acknowledge or greet them.
Decision-making models for considering the ethics of dual relationships have been proposed by Kitchener [5], Gottlieb [33] and more recently, Younggren [34]. The model proposed by Kitchener focuses on role conflict and identifies three dimensions associated with risk of harm to, or exploitation of, the patient. These are the extent of incompatibility of expectations between roles, the degree of divergence between obligations associated with each of the roles and the difference in prestige and power between therapist and client.
The issue of power is also highlighted in the five-step decision-making model developed by Gottlieb. This model involves an assessment of the current relationship on three dimensions of power, duration and termination, followed by an assessment of future relationships on the three dimensions and a judgement by the clinician of the role-incompatibility of these relationships. This is followed by consultation from colleagues in an objective situation and discussion with the potential patient in terms of possible ramifications.
Recently, Younggren [34] has produced a list of questions aimed to assist clinicians in decision-making concerning dual relationships. The questions are: Is the dual relationship necessary? Is the dual relationship exploitative? Who does the dual relationship benefit? Is there a risk that the dual relationship could damage the patient? Is there a risk that the dual relationship could disrupt the therapeutic relationship? Am I being objective in my evaluation on this matter? Have I adequately documented the decision-making process in the treatment records? Did the patient give informed consent regarding the risks of engaging in the dual relationship?
Each of the models outlined above assumes that the option of deciding a priori whether to engage in a dual relationship is in fact available to clinicians. However, for rurally based, and particularly isolated mental health practitioners this is often not the case. The issue for rural practitioners is not how to decide whether to engage in dual relationships but how to manage the dual relationship.
The various codes of ethics and decision-making models make it clear that the priorities must be to ensure that there is no harm to, or exploitation of, patients and that confidentiality issues are appropriately managed. Ensuring this requires action at several levels: patient, clinician, service and professional bodies (Fig. 1). A further priority must be to identify and address any potential negative effects for the clinician.
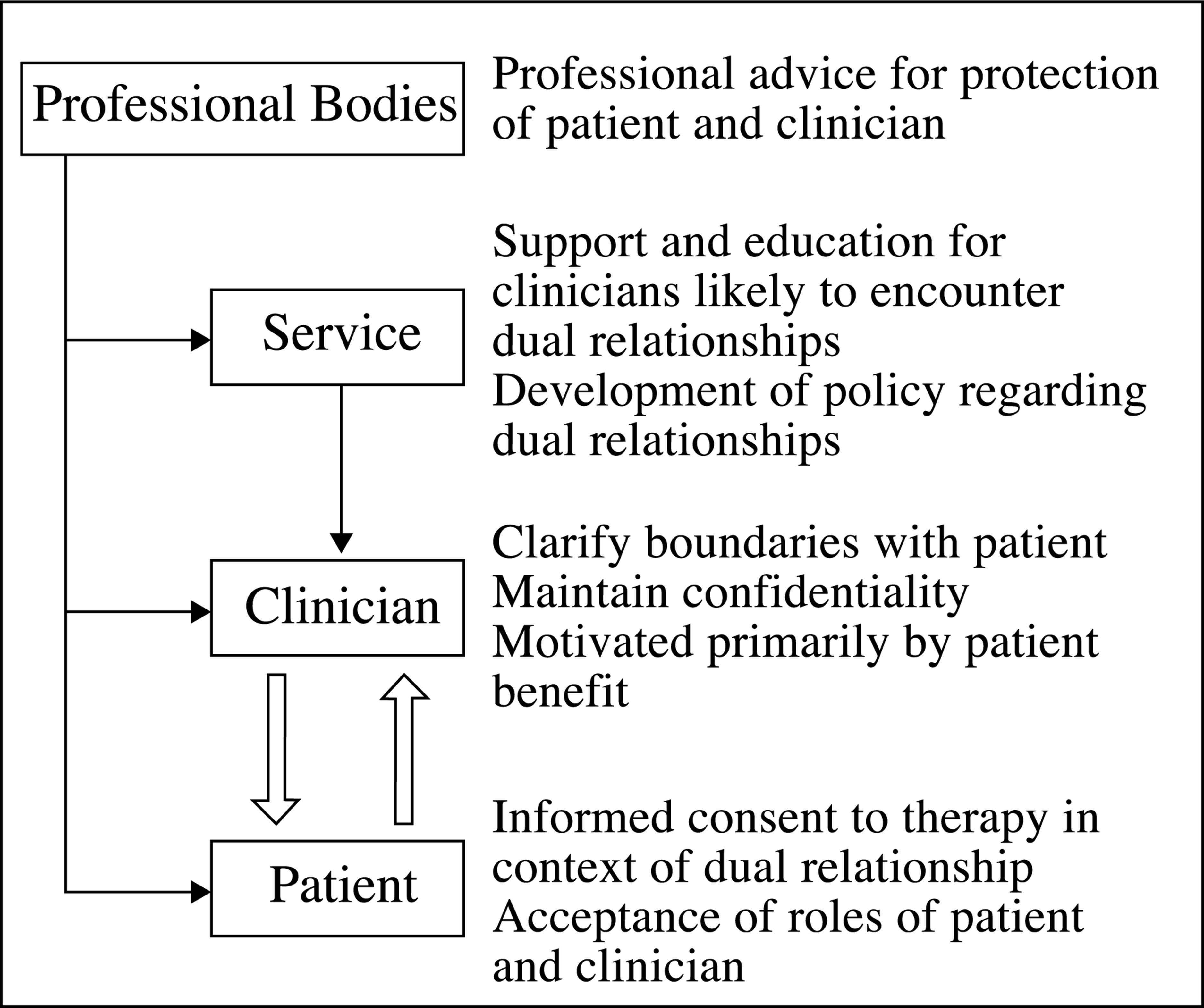
Responsibilities of those involved at different levels of the client–clinician interface.
Where dual relationship situations occur there needs to be a clear mutual understanding of the roles of both patient and clinician. It is important that clinicians attempt to make explicit the nature of their professional relationship with patients, how it differs from an extratherapeutic relationship, the limits or boundaries around this and confidentiality issues. In this regard there is a need to compartmentalize roles but not relationships.
In terms of treatment planning, some authors have highlighted the need to address specific areas of concern in writing, recommending that clinicians document dilemmas encountered, decisions made, and justifications used for engaging in dual relationships [34]. It is important that clinicians use an open, transparent and collaborative approach in addressing these issues. Perkins et al. suggest that ‘we should encourage a process that gives explicit attention to ethical grey areas and to educating clients in boundary and privacy issues’ [23], p. 35].
Borys and Pope [24] have emphasized the need for mental health training programs to help increase the sensitivity of clinicians to dual relationship issues. Support and continuing education for clinicians including consultation, supervision and reflective practice, play a crucially important role in ensuring that dual relationship issues are well managed. Some authors have highlighted the need in rural settings for extra-therapeutic contact between clinicians and clients to be integrated into the therapeutic process [35]. Awareness of, and strategies to minimize, risk issues should be balanced against the need for clinicians to be sensitive to prevailing community expectations and standards [36].
Current professional codes of ethics are severely limited in their capacity to assist the rural mental health clinician confronted by the inevitability of dealing with dual relationship issues. Acknowledging that these issues are an inevitable part of rural practice needs to be followed by the provision of guidelines to assist clinicians to manage these difficult situations and ensure that there is no harm to patients. Decision-making models offer some structure to clinicians working through these issues but only in cases where an option for not engaging in a dual relationship is available.
As can be seen from the material presented here, the focus when addressing dual relationships has been the possible impact of these on the patient. There has been very limited attention directed towards examining the impact of such relationships on the clinician. However, such attention is necessary, and any identified or potential negative effects, such as increased burnout, need to be considered when developing strategies and supports to manage dual relationships.
Conclusions
The reality of limited mental health resources in rural and small communities presents inevitable dilemmas to practitioners in terms of dual role relationships. ‘Everyday’ dual relationships such as when a clinician interacts with a patient who is on the same sporting team, is a fellow member of a community group such as the volunteer fire brigade, or the teacher of one's child, are a predictable part of rural mental health practice. Despite the divergence of opinion on the appropriateness of dual relationships, their inevitability in the rural context means that clinicians need to find ways of working with these relationships. This requires that all of those involved in the patient–clinician interface, as illustrated in Fig. 1, are aware of and actively manage the impact of context. Joint responsibility and action offer the best chance of safety for the patient, therapeutically beneficial outcomes, and understanding and management of any negative impact of such relationships on the clinician.