
Abstract
The availability of mental health services (especially specialists) in rural areas is identified as particularly lacking and is a priority in several national documents, including the National Mental Health and National Rural Health Policies. Some researchers have argued that as a result, rural residents depend more upon general practitioners (GPs) for mental health care [1], p. 18], and recognise them as more pivotal than metropolitan residents [2]. However, very little research has investigated GP service use for mental health problems across rural, remote and metropolitan areas.
The pathway to mental health care
In 2000, Henderson [3] described a five-tier model of mental health and service use called the cone of morbidity. The levels consist of: (i) a broad base of all people in the community with a psychiatric disorder; (ii) people seen by family doctors; (iii) those with psychiatric disorders who are detected and treated by family doctors; (iv) people who are then referred to psychiatric services; and (v) at the apex of the cone the small proportion of the population who are psychiatric inpatients [3], p. 424]. Henderson's model was developed from Goldberg and Huxley's [4] proposal that various filters determine how far an individual progresses along a pathway to psychiatric care. In this article data incorporating the second and third levels will be analysed.
The prevalence of mental health disorders (level 1)
Research has consistently found higher suicide rates in rural and remote than metropolitan areas, particularly for young men [5–7]. However, the prevalence of commonly occurring mental disorders has not been found to parallel suicide rates in rural, remote and metropolitan areas. Judd et al. [8] conducted a review of general population studies and found little difference in the prevalence of mental disorders across rural and metropolitan areas. More specifically, urbanicity was not associated with the prevalence of affective, anxiety and substance use disorders in the Australian National Survey of Mental Health and Wellbeing (NSMHWB) [9].
People seen by general practitioners (level 2)
The rate of GP service use for general health care is not equal across subgroups of the Australian population. Structural aspects of the healthcare system affect the population seen by GPs. For instance, an important difference between rural and metropolitan areas is the relative or absolute unavailability of specialist services and a lack of access to GPs [2]. Overall, people with mental health problems have more contact with health care services than those with no such problems [10], but when access to GPs is more difficult, there is less opportunity and potential for mental health problems to be detected and managed.
Several studies have shown differences in the mental health of rural and urban GP patients. In a large Australian audit of general practices, patients attending urban practices reported more psychological symptoms than patients of rural practices [11]. However, in the NSMHWB the likelihood of accessing help from a GP for a mental disorder was no different for metropolitan, rural and other rural participants [12], [13]. The NSMHWB results were limited by the small number of people surveyed in rural and remote areas and the lack of statistical power may have failed to detect any real regional differences. Additionally, the NSMHWB did not investigate the number of mental health encounters provided by GPs, recognition of mental health problems by GPs, or how the problem was treated or managed. Research needs to investigate these service issues in rural, remote and metropolitan areas.
Consulting a GP for a mental health problem depends on the individual recognizing they have some sort of problem and believing that the GP will be able to help. Research suggests that a large proportion of the Australian public cannot recognize specific disorders or distress [14], [15]. The Australian public prefers GPs as the point of first professional contact for mental health problems [15] and perceives them as more helpful (particularly for depression) than other health professionals, including psychiatrists [15], [16]. However, very little is known about the knowledge and attitudes of rural and remote people about mental health problems and services. One study found that the stigma associated with accessing treatment for a mental health problem was a greater barrier to care in rural areas than the stigma associated with the disorder itself [17]. Researchers have also argued that the critical role GPs play in mental health care is more openly accepted in rural and remote areas and more frequently questioned in metropolitan areas [4], p. 70]. However, beliefs do not necessarily translate into action. In a rural Australian area, seeking help from a GP for a mental health problem was not predicted by prior beliefs about their helpfulness for such problems [18].
Problems detected and treated by family doctors (level 3)
Many factors influence the detection and management of mental health problems in general practice, including characteristics of the patient (e.g. sex, age and severity of problems), the GP and the practice [4]. Rural GPs may see and/or detect a greater rate of psychological problems in their patients. For instance, the Bettering the Evaluation and Care of Health (BEACH) program found that GPs more frequently reported managing depression (but not anxiety) in practices in large rural centres than in metropolitan areas [19]. However, another survey of Australian GPs found that the practice location was not associated with the rate that patients were assessed by GPs as having a psychological diagnosis [11].
Referral and medication management of psychological problems
Research commonly reports a lack of locally available mental health specialists in rural and remote areas. For instance, in 2000–01 there were far fewer psychiatrists in rural and remote areas than capital cities (2.5 vs. 14.4 per 100 000 population) [20]. Consequently, rural GPs may employ different referral and management practices for psychological problems. Indeed, Britt et al. [19] found that rural GPs were more likely to refer patients with depressive problems to allied health professionals (e.g. psychologists) whereas metropolitan GPs were more likely to refer depression to psychiatrists. Additionally, mental health medications (largely antidepressants) were prescribed at a higher rate in GP/patient encounters in large rural than metropolitan practices [19].
Reduced access to GPs in rural areas is frequently noted by researchers but is rarely evaluated when investigating GP services for psychological problems. This study investigates regional differences in the psychological problems managed by GPs (corresponding to levels 2 and 3 in the Henderson model [2]) in their encounters with patients and per 1000 population. Rates of GP prescriptions (written and filled) for mental health medications are also compared across regions.
Method
Data from the BEACH program, Medicare claims and the Pharmaceutical Benefits Scheme (PBS) were used.
The Rural, Remote and Metropolitan Area Index
The rural, remote and metropolitan index (RRMA) is a sevencategory classification system [21] and was used in this study. First, statistical local areas in capital cities and statistical subdivisions containing an urban centre of 100 000 or more people, are identified. The other statistical local areas are then designated an RRMA category based on population numbers and an index of remoteness relating to distance from an urban centre (≥ 10 000 population) and population density. The RRMA categories and corresponding populations are: (1) capital cities; (2) other metropolitan centres ≥ 100 000; (3) large rural centres 25 000–99 999; (4) small rural centres 10 000–24 999; (5) other rural areas less than 10 000; (6) remote centres greater than or equal to 5000; and (7) other remote areas less than 5000 [21].
Small cell sizes meant that categories 6 and 7 needed to be combined for the analysis. The RRMA refers to the patient's address for the BEACH and Medicare data but the supplying pharmacy's address for the PBS data.
The BEACH program
The Australian Institute of Health and Welfare GP Statistics and Classification Unit (University of Sydney) provided data from the BEACH program, a continuous national study of Australian general practice activity. Random samples of GPs are drawn from Health Insurance Commission (HIC) data. The sampling methods of the BEACH program have been detailed in previous publications [e.g 22]. This article combines data collected from 1998–99 to 2001–02, giving a total of 401 300 encounters (any professional interchange between a patient and a GP) from 4013 GPs (a few may have been involved more than once). The GP response rates for each year were: 1998–1999 (38.4%); 1999–1900 (39.1%); 2000–01 (29.8%); and 2001–02 (32.3%).
General practitioners recorded information on 100 consecutive patient encounters, including problem(s) managed (the GP's description of each health problem managed at the current encounter) and medications prescribed, advised for over the counter purchase or those directly supplied at the encounter, for each problem managed. GPs could record up to four problems for each encounter and up to four medications per problem managed. The problems GPs reported managing were coded using the ICPC-2 PLUS [25].
Medicare and PBS data
In Australia, the HIC collects information about medical services and benefits paid through the Medicare system. The Commonwealth Department of Health and Ageing (DHA) provided the number of GP encounters (defined as general practice items claimed from the Medicare Benefits Scheme) across RRMA categories matching the 4-year period of the BEACH program.
Most prescriptions are subsidized through the Australian PBS. The DHA extracted PBS data (by anatomical therapeutic chemical codes) on the number of GP prescriptions filled for anxiolytic (N05B), sedatives/hypnotic (NO5C) and antidepressant (N06A) medications and each repeat was counted separately. The data refer to prescription claims processed by the HIC during 2001 but do not contain prescriptions costing less than $21.90 or Section 100 items (highly specialized drugs available through hospital pharmacies for outpatients) [20].
Statistics
Standard errors and confidence intervals were generated for all rates (BEACH and PBS)
used in this study. The BEACH program provided data about a cluster of encounters around
randomly selected GPs. Cluster sampling violates the simple random sample assumption of
the independence of observations. Consequently, the standard errors for the BEACH project
were adjusted for the clustered sampling method. Capital cities were compared to each of
the other available RRMA categories using z-scores: 
Here D12 represents the difference between two RRMA category proportions. S is the variance of the corresponding RRMA category. A z-score ≥ 1.96 or ≤ −1.96 indicates a significant difference (p < 0.05).
The number of encounters where GPs managed psychological problems in each RRMA category, was extrapolated from applying the (BEACH) rates that GPs’ managed psychological problems (per 100 encounters of all kind) to the national (Medicare) count of GP encounters for each RRMA category. The number of psychological problems managed was then converted into rates per 1000 population for each RRMA category using Australian Bureau of Statistics population estimates as the denominator.
Results
Psychological problems in general practitioner encounters
Figure 1(a) shows the rates of psychological problems GPs report managing (per 100 encounters) across RRMA. GPs reported managing fewer psychological problems in their encounters with ‘other rural’ (10.7/100 encounters; z = −2.39) and remote (9.8; z = −1.99) patients compared to capital city patients (11.4). Figure 1(b) shows the rate of mental health medications prescribed in encounters where a psychological problem was managed, per 100 encounters of all kinds. An increased rate of prescriptions for psychological problems was evident at encounters with patients residing in large rural areas (7.6; z = 3.62) compared with capital cities (6.5); however, no other significant differences were found.
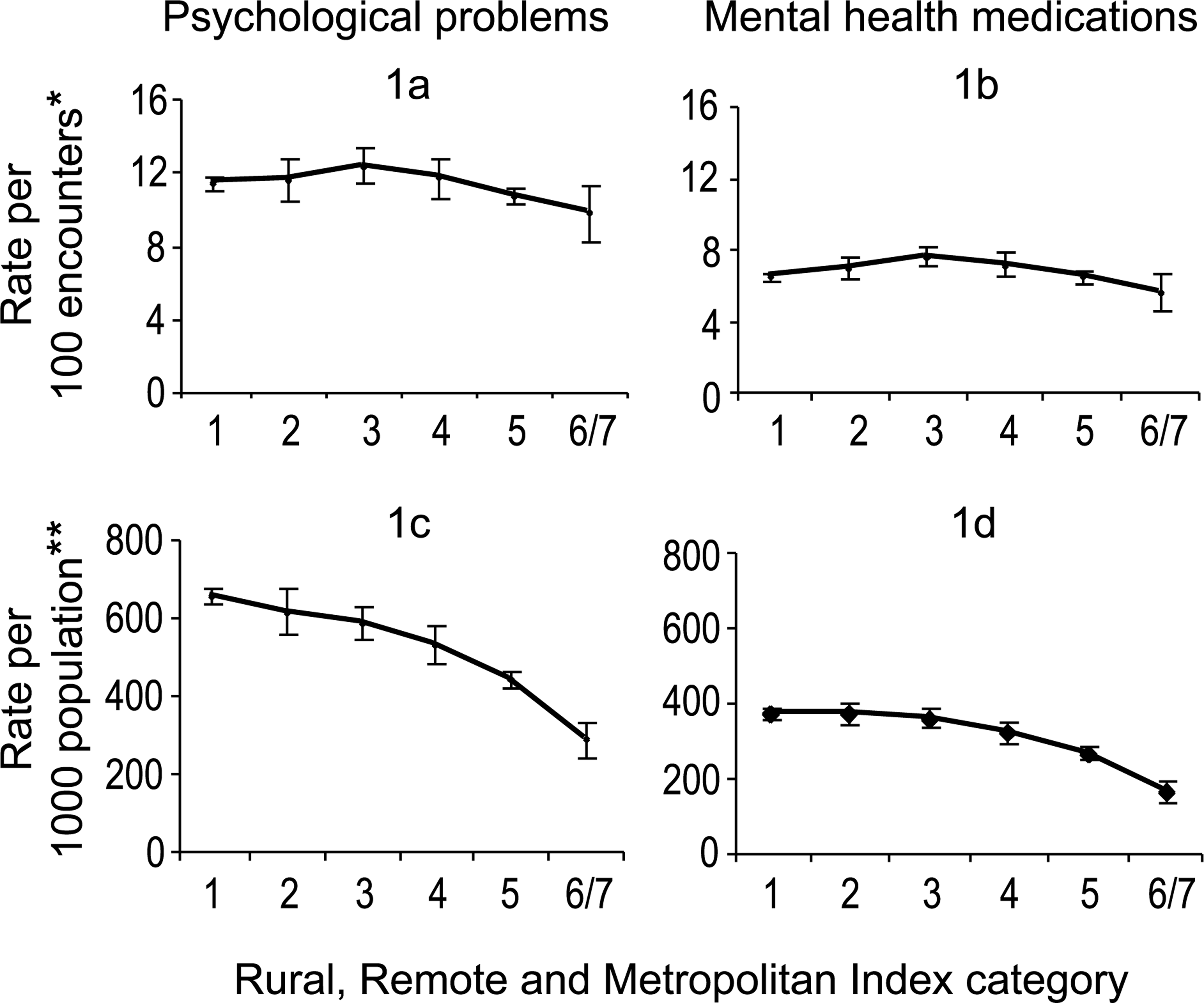
Rates (and 95% CIs) of GP encounters for psychological problems and where mental health medications were prescribed/advised across Rural, Remote and Metropolitan Area Index categories. Rates are given per 100 encounters (of all kinds) and per 1000 population. Sources: ∗BEACH; ∗∗BEACH, Medicare and ABS population data combined. (1) capital cities; (2) other metropolitan areas; (3) large rural areas; (4) small rural centres; (5) other rural centres; (6,7) remote centres and other remote areas.
Table 1 shows the rates (per 100 encounters) for the management of depression and anxiety problems. GPs reported managing depression at encounters with patients residing in metropolitan non-capital city areas, and all rural areas more often than for those residing in capital cities. In contrast, GPs reported managing anxiety problems less frequently in their encounters with residents from ‘other’ rural and remote areas compared to capital cities.
Rates (95% CIs) and z-scores† of GP encounters (per 100 encounters) where specific psychological problems were managed and medications were prescribed/advised across Rural, Remote and Metropolitan Area Index categories
Table 1 also shows that GP encounters with patients residing in metropolitan areas (non-capital city) and most rural areas less frequently resulted in the prescription of sedatives/hypnotics but more frequently involved the prescription of antidepressants. A lower rate of anxiolytic medications was prescribed/advised or supplied per 100 encounters with patients residing in ‘other rural’ areas than capital city centres.
Psychological encounters with general practitioners in the population
The number of GP encounters (per person/year) for the Australian population by RRMA (1998/89–2000/01) was estimated from the Medicare data: (1) 5.76; (2) 5.31; (3) 4.73; (4) 4.53; (5) 4.14; and (6/7) 2.94. On average, residents of rural, but particularly remote areas, had fewer encounters with GPs than capital city residents.
Figure 1(c) depicts the rate of all psychological problems managed by GPs across RRMA, per 1000 population. Psychological problems were far less frequently managed for residents of large rural (586.4 per 1000 residents, z = −2.89), small rural (529.9, z = −4.58), other rural (443.4, z = −14.59) and remote (288.3, z = −14.49) areas than capital cities (656.8). Additionally, Fig. 1(d) shows that mental health medications were less frequently prescribed for residents of small rural (323.9, z = −3.02), other rural (266.9, z = −10.45) and remote areas (165.0, z = −12.43) than capital cities (373.3).
Table 2 shows the rate at which GPs reported managing depression and anxiety problems per 1000 population. Depression was less frequently managed for residents of other rural and remote areas. The rate at which antidepressant medications were prescribed/advised/supplied generally followed the rate at which GPs reported managing depression. Small and other rural and remote residents were prescribed these medications less frequently than capital city residents. However, a greater rate of antidepressant medications was prescribed for non-capital city metropolitan and large rural area residents (per 1000 population) compared with capital cities. Anxiety was less frequently managed by GPs for all rural and remote than for metropolitan residents and anxiolytic medications were less frequently advised/prescribed for other rural and remote residents.
The rates (95% CIs) and z-scores† of encounters per 1000 population where psychological problems were managed and various medications were prescribed/advised/given across Rural, Remote and Metropolitan Area Index categories
It is possible that the number of repeats a GP writes per prescription and the number of times a prescription is filled, differ across metropolitan and rural areas. Table 3 shows the rate of mental health medications provided by rural, remote and metropolitan pharmacies (per 1000 population). The data specifically consists of claims made for GP-written prescriptions for mental health medications. The PBS and BEACH data could not be statistically compared because the RRMA measure in the PBS refers to the supplying pharmacy (not the patient) and the PBS data only relates to a single year (2001), whereas the BEACH data combines 4 years of data (1998/99–2001/02). Table 3 shows that a higher rate of GP prescriptions for mental health medications were filled than written (compared with Table 2). This is likely to be related to repeat prescriptions, which were each counted separately in the PBS data, whereas the prescription was counted once in the BEACH data, regardless of the number of written repeats. Table 3 indicates that remote pharmacies filled GP written prescriptions for antidepressants, anxiolytic and sedatives at a lower rate than capital city pharmacies (per 1000 population).
The rates (95† CIs) and z-scores† per 1000 population of general practitioner prescriptions filled by pharmacies across Rural, Remote and Metropolitan Area Index categories
Discussion
Only a few differences were found in the management of psychological problems in GP encounters with patients residing in rural, remote and metropolitan areas. However, on average, rural and remote residents visited GPs far less frequently than metropolitan residents. As a result the rate of psychological problems that GPs managed (per 1000 population) was much lower in rural and particularly in remote, populations than capital cities. The regional differences in the rate of GP mental health services refers to levels 2 and 3 of Henderson's cone of morbidity [3]. The NSMWHB findings found few differences at level 1 of this model, that is in the overall prevalence of disorders between metropolitan and non-metropolitan. Assuming that these latter findings are true, the present findings suggest large regional differences in mental health services provided by GPs (levels 2 and 3).
The NSMHWB also found no difference in the odds of visiting a GP for a psychological problem for rural and remote residents compared to metropolitan residents. However, the NSMHWB findings did not take into account the number of encounters provided by GPs for mental health problems. The lower rate of GP encounters for psychological problems in rural and remote areas (per 1000 population) in the present study could reflect less support and fewer follow-up consultations, or completely unrecognized/untreated problems. Further research is needed to clarify these issues.
This study has also confirmed that GPs report managing slightly different problems within their encounters with residents of metropolitan compared to non-metropolitan areas [23]. GPs reported managing a higher rate of depression per 100 encounters with patients living in rural areas than capital cities. This may be due to a higher prevalence of depression in rural patients [11] or it may reflect an absence of mental health specialists and the GP taking on a broader role in the management of depressive problems in rural areas. In contrast, GPs managed fewer anxiety problems within their encounters with patients residing in remote areas. GPs and/or residents of remote areas may not recognize anxiety problems and/or remote residents may access GP services less frequently for anxiety problems. However, overall, there was very little difference in the rate GPs reported managing psychological problems within their encounters with patients residing in rural, remote and metropolitan areas.
When a GP reported managing a psychological problem, prescription rates for mental health medications were broadly similar in encounters with rural and metropolitan residents. However, prescription rates for mental health medications differed substantially for rural, remote and capital city residents, per 1000 population. This was due to the fact that on average, non-metropolitan residents have far fewer encounters with GPs than metropolitan residents. Remote residents were prescribed mental health medications at half the rate of capital city residents. Remote pharmacies also provided far fewer prescriptions (and repeats) for mental health medications per 1000 population.
A higher rate of GP-prescribed antidepressant medications were supplied by pharmacies in large rural areas than capital cities per 1000 population. This could reflect a concentration of pharmacies in large rural centres, where patients from more remote areas go to fill prescriptions. However, GP prescription rates for antidepressants were higher for large rural area residents and lower for remote residents than capital cities. This could reflect greater reliance on medication for management of psychological problems in large rural areas. It remains possible that rural and remote residents fill prescriptions and seek care for mental health problems away from their area of residence, for reasons relating to choice rather than a shortage of services.
Strengths and limitations
The RRMA index is available across many national datasets, but has been criticized for confusing distance and density and is being replaced [24]. Ascribing a single definition to a statistical local area does not allow for diversity within areas [24]. Research needs to investigate diversity and a wide range of experiences. We have also not investigated reasons why GP service rates were lower for non-metropolitan residents. Alternative services or means of support may be used by rural residents.
From 1998 to 2002 around 4000 GPs participated in the BEACH program: 20% of Australian GPs. However, annual response rates for GPs ranged from 30% to 39%. A comparison of BEACH participants with Australian GPs has been reported in previous publications [e.g. 22]. In spite of the annual response rates, previous reports suggest that BEACH encounters represent all GP/ patient encounters well when compared to MBS item claims for general practice services [22], [25].
Lastly, BEACH encounter rates do not measure prevalence of psychological problems among general practice patients in metropolitan and non-metropolitan areas. The findings reflect what GPs reported and represents their recognition and treatment of psychological problems.
Conclusions
Mental health policy and research stress two important points. First, GPs are considered the first port of call for mental health help and second, rural areas rely more heavily on a limited number of GPs, because mental health specialists are in short supply. The particularly low rate at which GPs report managing psychological problems in the non-metropolitan population demonstrates sparse provision of general practice care for mental health problems in non-metropolitan areas.
Footnotes
Acknowledgements
This report was funded by beyondblue: the National Mental Health Inititative. The BEACH program (1998–2002) was supported by: the Australian Department of Health and Ageing (DHA), Astra-Zeneca (Australia), Roche Products, Aventis-Pharma, Jansen-Cilag and the Commonwealth Department of Veterans’ Affairs (1998–1900), the National Occupational Health and Saftey Commission (1998− 1900) and Merck Sharp and Dohme (Australia) (2001–02).
Thanks to participants in the BEACH program and to the Hospitals and Mental Health Services Unit at the AIHW. The Pharmaceutical Access and Quality Branch of the DHA supplied the PBS data and the Medicare Benefits Branch of the DHA supplied the Medicare data. Thanks also to Helen Berry for editorial suggestions.