
Abstract
The intrinsically stressful nature of rural health practice is well recognized. One aspect of this stress relates to the complexity of professional and ethical dilemmas in rural environments, with dual relationships a key feature of rural practice [1,2]. A dual relationship is defined as ‘two or more distinct kinds of relationship with the same person’ [3].
Rural mental health workers are often required to provide treatment for patients with whom they have had a previous or concurrent personal or other relationship [4–7]. These dual relationships pose particular challenges in a rural setting. For example, rural mental health professionals may experience difficulties in maintaining their own privacy encountering current and past patients outside the clinical situation. While the dual relationship may provide some benefits [8], it has traditionally been considered unethical in some areas of health practice, particularly mental health [9,10].
While dual relationships are part of the fabric of rural health practice [11], this has received scant attention in the research literature [12]. The limited research evidence available focuses on the impact of a dual relationship on the patient, rather than the clinician. Similarly, advice provided by decision-making models addressing the ethics of dual relationships focuses on considerations of whether to enter a dual relationship [13], implying that the clinician has a choice, and stops short of advising how such relationships should be managed.
When considering dual relationships, distinction has been drawn between boundary crossings and boundary violations [12] with the latter used in the context of clinician violation: ‘actions on the part of the clinician that are harmful, exploitative and in direct conflict with the preservation of clients’ dignity and the integrity of the therapeutic process' [1]. Such violations perpetrated by clinicians or patients are deemed unacceptable. Boundary crossings, on the other hand, are ‘benign and sometimes beneficial departures from traditional therapeutic settings or constraints’ [12], p. 955].
This study aims to compare the issues associated with dual relationships and professional boundaries for mental health workers in metropolitan, regional and rural settings. The focus of the study was on ethical dilemmas that arise for clinicians when a dual relationship results in a breach of professional boundaries.
Aims and research questions
The aims of the study were to:
explore the frequency of dual relationships and boundary crossings explore the nature and impact of professional boundary crossings identify strategies clinicians use to manage dual relationships
Design
Method
The research questions were addressed through a total of nine focus group interviews conducted in rural, regional and metropolitan settings. Focus groups capture communication between research participants in order to generate data [14]. Their added benefit, above individual interviews, comes through the synergy generated between group members and their ‘permissive’ and peer support function in encouraging participants to divulge opinions and beliefs that might not emerge through an individual interview [15].
Sample
The study was carried out in four rural towns, one regional city and a metropolitan health service in Victoria. Each of the rural towns has a rural hospital located within the town, which provides a hub for local health services. In total nine focus groups were conducted: four in rural settings, three in a regional city and two in a metropolitan area. Participants were mental health workers employed in a mental health setting. A total of 52 participants were interviewed; demographic details are provided in Table 1.
Summary demographic data for the three focus group settings
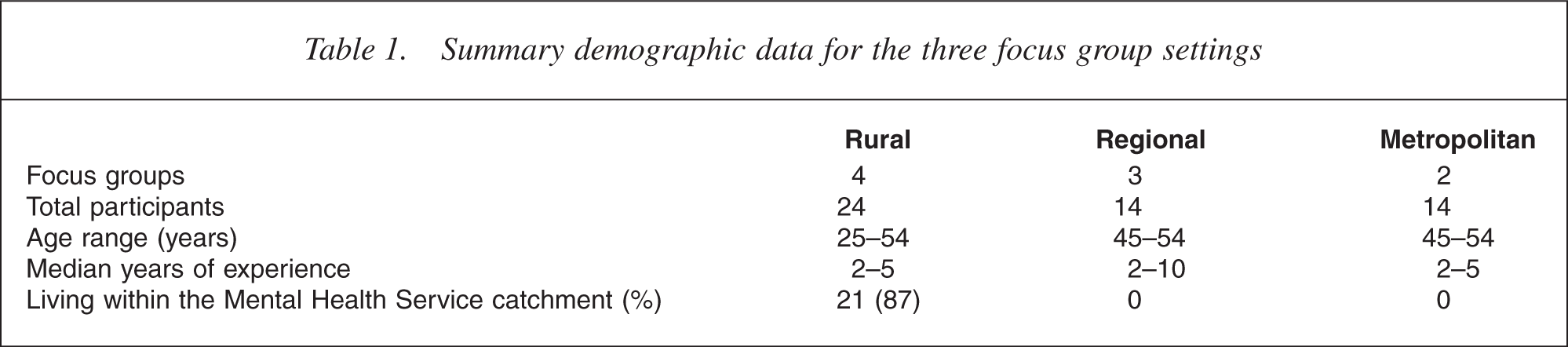
A purposive sampling strategy was used in order to target mental health clinicians. Information about the project was circulated to local mental health services and participants invited to attend a focus group. Written consent was obtained from participants when they attended the focus group.
Data analysis
Qualitative content analysis was used to identify themes in the data [16]. Data were then compared across sites to ensure that themes were pursued in subsequent focus group interviews until saturation was achieved [17]. A qualitative approach enabled in depth exploration of the perspectives of each participant. This approach acknowledges and explores the diversity of perceptions rather than purely seeking to aggregate data. Importantly, this qualitative strategy allowed the identification of common themes across focus groups.
The following nomenclature denotes category of focus group for data excerpts: M1/2 = metropolitan; RC 1/2/ 3 = regional city; R 1/2/3/4 = rural.
Findings
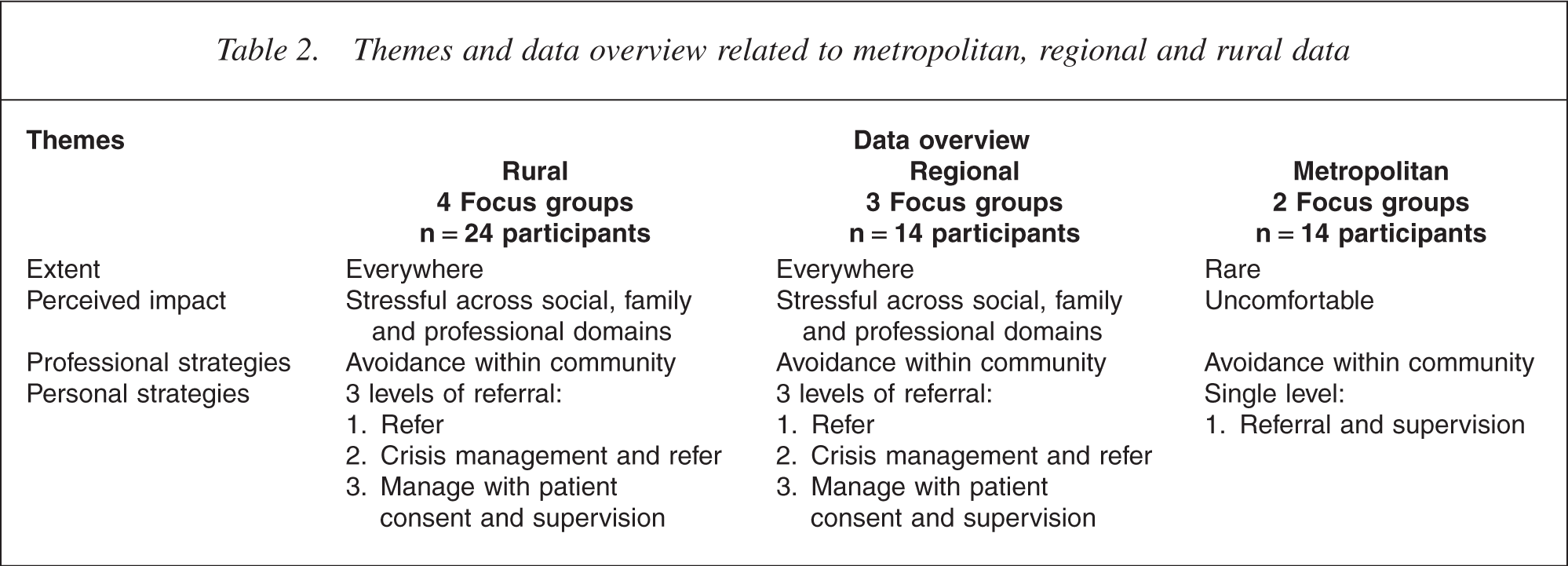
Four themes emerged from the data: (i) the extent of dual relationships, (ii) perceived impact of dual relationships, (iii) personal strategies, and (iv) professional strategies employed to counteract these effects. The data overview for these four themes is summarized at Table 2.
Themes and data overview related to metropolitan, regional and rural data
Extent of dual relationships
Participants across the three settings were invited to discuss their experience, if any, of a dual relationship in their community mental health experience. The consistent and emphatic response from rural and regional participants was ‘Yes. Everywhere’. However, the degree of ‘relationship’ rather than geographical colocation varied considerably. It became evident that the rural and regional city clinicians identified dual relationships merely through living within their community: There is a relationship whether you like it or not. And the nature of living in a small community it is a dual relationship. (RC1/Dec 2003)
The similarity between the rural and regional clinician experience of dual relationship was strongest when clinicians had had a long connection to the community, for example, growing up in the town, attending school, family links within the region: I've always lived in [location]. The family's sort of been in [location] for three plus generations, so there's lots of established sort of family and social networks… I've case managed as a sole practitioner in the region so I've often run into relatives and family friends. (RC3/May 2004) I had one client that came in not long ago. And I've known him since we used to play in a bath together… [Laughter]. (RC2/Dec 2003)
Similar issues arise where clinicians lived in a smaller township within the Area Mental Health Service catchment: I come from a small town, not far from [location] and some of the clients up here are from the same town and it's not so much a relationship with them, but with their parents. (RC1/ Dec 2003) Affects my wife, my kids, friends, It's HUGE, service organizations, footy clubs, It's just everywhere. Despite the fact that there are 15 000 people… its small it's still like a ‘fishbowl’ effect. (R1/Sep 2003)
The reality of rural and regional community mental health practice for these participants is that professional and social relationship frequently overlap and become blurred: Look the reality is that if you're going to live in the community… be a part of the community and we see so many different people from such a broad background you just can't divorce yourself from it… it's impossible. You know… as much as you try to put your boundaries up and protect. (R1/Dec 2003)
However, regional city participants with rural experience acknowledged that rural clinicians faced a greater challenge due to the size of community, visibility within community, smaller mental health team and role diversity: Within the rural context you've got to work as everything. You can be doing your crisis assessment, you're doing longterm rehabilitation support. You are doing everything. So the community can actually hold you personally, sort of thing, as the service, accountable. (RC3/May 2004)
By contrast the metropolitan participants acknowledged limited or no experience of dual relationships in the urban setting. That's the beauty of the big city. It's easy to get lost isn't it?… keep your distance. (M1/Nov 2004)
The difference between rural and metropolitan was validated by the comments of metropolitan participants with previous rural experience and rural participants with metropolitan experience. No metropolitan participant lived in the catchment area of the Area Mental Health Service. This provides clinicians with geographical separation between social and professional spaces, though clinicians recognized that they could expect to see patients if they socialized in their catchment area.
Perceived impact of dual relationships
The frequency and nature of ongoing dual relationships between rural and regional city clinicians and their community of patients and patients' families result in a range of experiences that are largely perceived as negative in the social domain. There was a strong sense of unwanted exposure that inhibited enjoyment in the social setting: On the down side I sort of feel that you have to carry your work professionalism into your private life. [Nods of agreement around table] Which can be a pain sometimes. Because you can never perhaps quite ‘let your hair down’ You are always slightly reserved, I guess; take a professional stance regardless of wherever you are in this town. (R2/Sep 2003)
By contrast the metropolitan participants rarely experienced patient contact in the community setting. Clinicians from all settings typically described feelings of mild annoyance (at most) when a patient interrupted an outing. The exception in the data came from a rural participant who had recently moved from a metropolitan setting and was enjoying community inclusion. The clinician described the experience thus: So mine's a bit different. I get a sense of belonging in a lot of ways… I'm a new person to this town. (R4/Apr 2004)
However, it could be expected from the research findings that over time this practitioner would increasingly be confronted by potential conflicts with dual relationships in the rural setting.
When children were discussed a common theme was the tension between protecting the patient's privacy and the child's safety and wellbeing. Illustrative of the tension is the following participant description of a school gate scenario: Well when your child comes up and says ‘Mum, can I go home to “so and so's” place?’ You just sort of saying to yourself ‘No way. You're not going anywhere near that household.’ You know, but you sort of say. ‘Well look honey. We've talked about this before. You know you are not to approach me in the school, on the spur of the moment. We have to talk about it'. (R4/Apr 2004)
A recurrent theme for rural and regional participants was the (often unspoken) burden of patient and community expectations. This included clinician availability, access and quality of mental health services: But they have sort of had an expectation that you will be able to come in make everything all right. And when you can't it does feel a bit like ‘You've let us down’. (RC3/May 2004)
A rural participant described the intensity of feeling evoked by a personal expectation to meet the commu-nity's needs: To me, it was me letting them down, but I had to change my thinking. And know that it's not me, it's the system and I can't do anything about that system. And that this day, right, right to this day it plagues me. (R4/Apr 2004)
A number of rural and regional participants believed that the stress of dual relationships in rural and regional practice might further impact on organizational health, recruitment and retention: I think it's like being on ‘Tour of Duty’… sometimes… you get more worn out as you go on and you get more fed-up with the impact of dual relationships. I know that its impacted on what positions I've taken because… when, you know, when you work a position of high turnover and you're in the ‘firing line’ all the time it does damage your own mental health I think. (R1/Sep 2003)
Participants were asked to consider the impact on patients. Participants in all settings described patient reactions to social encounters. The data theme corresponded to a continuum from avoidance to exuberant greeting. Participants identified the moderating variables for the patient's response as: the patient's level of perceived stigma, quality of the relationship and the acuity or type of illness. There was a perception expressed by metropolitan clinicians that: …it is also sometimes helpful for clients to see us in the real world and humanize us, and maybe interact with us as human beings and have that social exposure. (M1/Nov 2004).
However, regional and rural clinicians were sensitive to patients being inadvertently identified as such in the community setting and how easily the patient's identity as mental health patient could be exposed in a social setting: So confidentiality becomes a real issue because it gets sort of broken totally unintentionally in that respect. There's nothing you can do much about it in those circumstances. (R2/Sep 2003)
Clinicians were sensitive to patient feelings and there was a recurring theme that clinicians perceived discomfort for patients: …when you see people in crisis and you become aware of their situation and their circumstance and you get a pretty comprehensive personal history. You run into them in a social setting that's pretty uncomfortable too. (R2/Sep 2003)
However, a recurring theme in the data was the perception that a dual relationship on the basis of living in the community improves trust and rapport to the benefit of the patient: And they know you as people as well rather than a clinician making decisions about their life. They actually know that you relate as human beings as community members rather than workers. (RC3/May 2004)
The most positive theme for rural and regional participants was that of seeing the patient function in the social setting. However, this can be stressful if a patient is encountered in crisis in a social setting: Then you have to be… it's just like being back at work again… And it happens to us time and time again… you know… we get put in the loop. And we don't want to be. (R2/Sep 2003)
Another positive impact was the close relationship across professions (police, social workers, general practitioners) and collaborative knowledge sharing within a case-management context in rural and regional city settings. These relationships provided additional support for clinicians.
It was clear that the actions of some patients were construed as ‘harmful’ or ‘exploitative’ [1] from the perspective of the clinicians. There was a strong theme in rural and regional city data of ‘being known’, that is, patients knowing where a clinician lived and the patient and/or their family contacting them at home. I got a call one night from the sister of a client concerned about her brother. Umm… At which point I immediately had the phone number delisted and changed and 3 days later she turned up at the house… because she said ‘Oh your phones been cut off… so I paid you a visit’ and that was at the weekend! (R3/Oct 2003)
While not an intentional violation, a strong theme for rural and regional participants was exposure to patient anecdotes and misinformation in the community. A regional participant described the potential impact on clinical judgement: So you are actually hearing the community's story as well as their story. And I think that does interfere sometimes. You try and separate it but when you are actually sitting in the room you have got two stories. (RC3/May 2004)
At a more extreme level, these interactions sometimes created tension between the desire to correct the misinformation and the need to protect the privacy of the patient: I had people saying to me ‘Did you hear about that dah dah dah dah?’ and you sit through a whole conversation. And you know that some of the things they are saying are inaccurate. [But] you can't say a thing. [Murmurs of agreement in background] You can't, you can't correct the inaccuracy. (R4/Apr 2004)
Personal strategies
Across all settings clinicians had initiated a number of personal strategies in an attempt to separate their professional and personal lives. One rural participant discussed the cost of protective strategies, including living out of the catchment area: I'd certainly like being able to shop without running into clients. It's more expensive, because you travel 45 min every morning and have a silent number. But I choose to do that,… so that I don't have this sort of business all the time. (R3/Oct 2003) Avoidance of social activities and space was common: I send my husband shopping. So ‘cos I really hate it [being approached by patients]… in the supermarket, and it doesn't matter what time you go. He likes doing the shopping [laughter]. So it works. (R1/Sep 2003)
However, this was more difficult to maintain when a clinician's family was involved in friendship groups and community activities: It's impossible because of the kids…. teenager kids, and their friends, and you know. [Lots of agreement from group] [You can] pull back from activities but I guess for some that's not an option. (R1/Dec 2003)
One participant described the family protocol for protecting the clinician from unwanted intrusion. All my family members and friends know not to give out my number. But if it's urgent, they'll ring me and say ‘This person's rung looking for your number.’ And I'll make a decision whether I want to call them or not. (R2/ Sep 2003)
There was also the suggestion that training in the understanding and management of professional boundaries could be extended to include family members. As one participant remarked: My wife who also trained as a Psych Nurse is well aware of a lot of the issues that I have to face. She is quite understanding. (R1/Sep 2003)
Professional strategies
Clinician strategies
The key professional strategy identified by participants across all settings was referral. On the whole professional boundary issues were rare in the metropolitan setting and professional strategies of supervision and referral ensured timely resolution. This was also the preferred or first level strategy in the rural and regional data. Generally, if the person is that close to us we would actually give it to one of the others to case manage or try not to deal with it or something like that. Not put ourselves in that situation. (R1/Sep 2003)
In some rural and regional situations a clinician may have no choice regardless of degree of relationship. In these situations clinicians were required to deal with the situation and then refer a second level strategy. We are sole workers. So if I get a call on the weekend, be it a family member of mine, or you know someone I know. I have to respond to it because we have no one else to do it. So you're left in a situation where someone needs to be seen and you know them, You have to go and deal with it as best you can. (RC3/Oct 2003)
Of necessity, in many circumstances, clinicians are required to manage patients with whom they have a dual relationship. The data suggest that clinicians have their own criteria for determining whether further patient involvement is appropriate and manageable. Exclusion criteria identified in our data include:
Diagnosis (personality disorder, substance abuse) Acuity of illness (patient with acute psychosis) Poor outcome of previous relationship (personal or professional) Degree of relationship (close and ongoing) Expected length of involvement (ongoing)
If these variables were not present a clinician may choose to maintain their involvement with a patient with whom they have had/do have a dual relationship. This occurred with patient consent and professional supervision. Hence, the recurring third level strategy in rural and regional data involved identification of the relationship, consent and negotiation of the therapeutic relationship and boundaries, which was seen as effective in the context of inevitability. And I've never had a problem,… although they may identify the link, whether it be that they know family or friends of mine whatever… Once we've had that initial conversation I've never had a problem with the boundaries being crossed. (R3/Oct 2003)
The elements of the discussion with the patient typically include identification and education regarding management of the dual relationship with particular reassurance of the confidentiality of the therapeutic relationship: I usually talk to families like that about, particularly if they know [husband] or my kids that I don't share any information with my family, that even my husband doesn't know that I will be seeing them. And that it is totally confidential and I always raise that [Murmurs of agreement,] So I needed to discuss that with them in the session. To see what they wanted to do about that. Did they want to continue? For some reason it was difficult for anyone else to see them. When we discussed it they were OK with it. And we've had quite a long association. (R4, April 2004)
Organizational support
Participants across all settings acknowledged the importance of organizational support in the form of policy clarity, team support, debriefing and supervision.
At team meetings we might discuss new referrals and highlight ‘I know that person it's not appropriate for me to case manage’ or that person may be a second cousin to a niece or something and I don't want to be involved for that reason. So we do try and put up all those boundaries and protect the workers. (R1/Sep 2003)
Further discussion within the group identified a recurring dilemma in the rural and regional setting where all workers within the community mental health service know the patient and there is no other local service to refer to: There's often no other opportunity as there are no other services available. (R1/Sep 2003)
An experienced regional city clinician discussed the value of supervision and extended the suggestion of external supervision. It seems the value of supervision or team consultancy or whatever you want to call it when there is a personal relationship being a dual relationship involved. It seems more important, that would be my experience, than it does when it is just another complex case because they are all complex in some ways. I think it does become more important. The provision of even external supervision or external away from the team may be another consideration as well. (RC3/18 May 2004)
Discussion
Dual relationships have been described as inevitable in remote [18] and rural [12] settings. Our data demonstrate that these were common in regional and rural settings, similar to the remote practitioner sense of ‘living in a fishbowl’ [18], p. 22] and community ‘visibility’ described by Campbell and Gordon [2], p. 432]. The boundary crossings associated with these dual relationships had both negative and positive effects. The negative effects tend to be related to the clinician's private life while the positive effects were related to their professional life, providing greater opportunity for understanding the patient. Our data did not reveal any boundary violations initiated by clinicians.
The findings suggest that approaches in the literature such as decision-making models are of limited value as often clinicians working in small isolated rural teams do not have a choice about entering a dual relationship. Thus, the focus needs to be on managing dual relationships. Strategies used by clinicians were ‘common sense’ protective strategies, generally involving avoidance of social activities and space. Importantly, these required active participation and some impost on the clinician's family. Professional strategies were limited by the size and degree of isolation of the rural teams. While referral elsewhere is an obvious way of managing a dual relationship, in some instances this was not an option. Inevitably, in many circumstances, rural clinicians were required to manage patients with whom they had a dual relationship. Here, important strategies were negotiating clearly defined and mutually understood therapeutic boundaries with the patient. Organizational and peer support were important mechanisms for those clinicians involved in dual relationships.
The issue of power is a common dimension in the decision-making models of Kitchener, Gottlieb and Younggren [see 7]. Brooks [19] rejects the powerful/ powerless dyad as being unhelpful in understanding the relationship between a clinician and patient and identifies productive mutuality of power as imperative for patients to regain control over their illness and care. In our data, power sharing was implicit in the negotiation and per-mission-seeking strategy described by clinicians who elected to continue to manage patients with whom they had a dual relationship.
Conclusions
Dual relationships should be recognized and acknowledged as an integral part of rural practice. Clinicians working in rural areas should be provided with education, training and support, both personal and organizational, to deal with dual relationships. Professional bodies and sanctioning authorities such as licensing boards should: (i) acknowledge the difficulties associated with the inevitability of dual relationships in some settings; (ii) differentiate acceptable boundary crossings from unacceptable boundary violations; and (iii) provide appropriate guidelines for the protection of the patient and the clinician. Health services should develop clear policy regarding dual relationships, provide clear guidelines for management of these, and support for clinicians who work in settings where such relationships occur. Clinicians who participated in our study had developed first, second and third level strategies; services are encouraged to formalize such approaches, through, for example, providing back-up on call services, crisis workers not serving the town or area where they reside. Supervision should be available to clinicians to assist them to deal with the personal stress as well as the complex professional issues that can arise in rural practice.
Limitations
The participants in this study were clinicians who were willing to share their experiences hence some bias may have been introduced. We have explored the perceptions of clinicians regarding dual relationships but have not examined corresponding views from patients about problems of dual relationships and whether there are beneficial or negative impacts for patients.