
Abstract
The National Survey on Mental Health and Wellbeing (NSMHW) [1], which represents a major effort to understand the prevalence and correlates of mental disorders in the Australian community, may have failed to do this with respect to the elderly and immigrants. The NSMHW showed a substantial reduction in the rate of mental illness with increasing age but under-sampled certain sectors within the elderly community – those in institutions or who were homeless, those under the care of others, those who were physically unwell and those scoring low on the Mini-Mental State Examination [2]. The NSMHW also excluded immigrants born in non-English speaking countries (termed non-English speaking background, NESB) due to their low English proficiency. In the 2001 Census the NESB group constituted 13% of Australia's population. The level of underrepresentation of this group in the NSMHW is not clear from its key reports [1], [3]. Regardless, the NSMHW indicated that the rates for anxiety and affective disorders were similar between those of NESB and those locally born. Comparative rates for affective disorders were 5.3% versus 6.1% and rates of anxiety disorders were 9.6% versus 9.8% for NESB immigrants and Australian-born, respectively [1]. One of the suggested indicators of risk for psychiatric morbidity in immigrant groups is poor proficiency in the host country language [4], [5]. The selection of samples of immigrants into the NSMHW based on their English proficiency may have inadvertently selected those who were better educated and had a longer time to make necessary adaptations to the Australian environment.
The combination of low prevalence due to age and to immigrant status, as suggested by the NSMHW would suggest that a group defined by these characteristics would have a particularly low risk for psychological morbidity. In line with this view, with respect to immigrants, Andrews et al. [3] have suggested that immigrant-selection factors may have operated to allow mainly the migration of healthy individuals. However, against this, migration and immigrant status reflect very different conditions of living from the majority culture and these conditions can often carry higher risks for psychological morbidity. These may include confronting unfamiliar institutions and processes in the host country, reduced opportunities in employment, membership of lower socio-economic status groups, the handicaps of lower levels of education, family and individual role changes, the barriers of language and absence of effective supportive social networks.
Given these concerns, the purpose of this report is to explore depressive and anxiety illness in older-aged members of the Greek-born (GB) community. International literature suggests higher rates of depression and anxiety disorders and in depressive and anxiety symptomatology in older-aged GB immigrants [6], [7]. Members of the GB community in Australia, particularly women, experience higher levels of psychiatric morbidity when compared with many of the other birthplace groups and the Australian-born [8]. In the present work we examine depression and anxiety in a group of older GB immigrants living in Melbourne who were likely to have been excluded from the NSMHW due to their incapacity in the English language and for whom the rate of mental disorder is unclear. We compare this group with a similarly recruited group of Anglo-Australians (AA). We used the Beck Depression Inventory-II (BDI-2) [9], which, in addition of score analysis, allows the definition of ‘caseness’ based on symptom severity, and the State-Trait Anxiety Inventory (state version) [10] to measure level of anxiety and to classify respondents into lower and higher anxiety score categories. In addition, we examined the competing effects of background factors considered as putative determinants of mental health status, including age [11–13], gender [14], [15], marital status [14], [15], household composition [16], level of education, occupational status, employment status, financial comfort [11], [12], [14], [15], [17], [18], memory functioning [19], physical health [20–22] and experience of recent stressors [14],[22–28].
Method
Subjects
Two hundred and ninety-two respondents participated in the study and of these 146 were GB and 146 were AA. All Greek participants were born in Greece and all AA participants were born in Australia. For the GB sample, 70 were male and 76 were female with a mean age of 68 years (SD = 7.3). For the AA sample, 73 participants were male and 73 were female, with a mean age of 69 years (SD = 12.2).
Measures
All self-report scales used were found only in English and were translated into Greek for the purpose of this study by the bilingual researcher/clinical psychologist (LK). Item translations were reconsidered by the second bilingual researcher/clinical psychologist (SK). More difficult or ambiguous items were examined for meaning with lay members of the Greek community and with another bilingual mental health professional working with the Greek community. This method was preferred over sequential translation/back translation methods by an interpreter as it capitalized on the expertise of bilingual mental health professionals. Validity was checked by examining the psychometric properties of the scales (factor structure and internal consistency) after data were collected and preceding any further analysis.
The following were assessed. Demographic information inquired about gender, age, country of birth, years living in Australia, ethnic background, highest level of education, marital status, household composition, current financial comfort, current employment status and main type of employment during working life. Current financial status was measured by summing affirmative answers to the following three items: ‘Are you comfortable with your financial situation at the moment?’, ‘Are you able to save money after all the expenses?’ and ‘At the present time do you feel that you will have enough money for your expenses and needs in the future?’ Reliability for the scale indicated an α-coefficient of 0.80. Memory functioning or cognitive impairment was measured with the Memory Functioning Index, a 6-item self-report index which asked about memory for: people's names; stories; appointments; dates; news items; and a grocery list. Responses were on a five-point scale (‘much poorer than average’, ‘a little poorer than average’, ‘average’, ‘a little better than average’ and ‘much better than average’). Higher scores indicate better memory functioning. In the present sample, the internal reliability for the scale indicated an α-coefficient of 0.79. Physical health was measured using the Physical Health Index, a single rating for ‘the past 6 months, including today’. Responses were on a 5-point scale (‘poor’, ‘fair’, ‘good’, ‘very good’ and ‘excellent’). Level of experienced stress was measured with the 9-item Stress Scale measuring the degree of effort expended in dealing with various adverse events in the past 6 months. Responses were on a three-point scale (‘no time and effort’, ‘some time and effort’, and ‘a lot of time and effort’). Adversities included experiencing a severe or major illness where a doctor had to be consulted, whether a member of the family had such an illness, having conflict with family members, family members being in conflict with each other, accommodation being unpleasant, uncomfortable or inadequate, death of family or friends, separation from family or friends and an open-ended question to rate any other critical or important adverse event. The internal reliability for the scale for the total sample indicated a coefficient of 0.66, consistent with it being a list of adversities rather than a homogeneous scale. English language proficiency for the GB sample was measured with a 5-item English Proficiency Scale [29]. Items depicted situations of different communicative difficulty [29] and they included regular shopping, regular banking, attending an English-speaking doctor, discussing finances with the bank manager and writing on formal business. Responses were on a 5-point scale (‘poor’, ‘fair’, ‘good’, ‘very good’ and ‘excellent’). The α-coefficient for the scale was 0.96.
Depressive illness was measured with the BDI-2 [9], a 21-item selfreport instrument for measuring severity of depression in adults and corresponds with the DSM-IV diagnosis of depressive disorder [9]. Responses to items for the present study covered the ‘past two weeks, including today’. Responses on the BDI-2 items range from 0 to 6 with higher values indicating higher severity. The total score can be divided into categories reflecting severity of depression. Accordingly, the minimal range of depression is 0–13, the mild range is 14–19, the moderate range is 20–28 and the severe range is 29–63. The internal reliability analysis in the present sample indicated an α-coefficient of 0.86. Anxiety was measured with the State-Trait Anxiety Inventory (state) [10], a 20-item, reliable, self-report questionnaire that is a sensitive indicator of anxiety used in research and in clinical settings [10], [30], [31]. The scale evaluates feelings of tension, nervousness, worry and apprehension ‘in the past two weeks, including today’. Responses were on a four-point scale (‘not at all’, ‘somewhat’, ‘moderately’ and ‘very much so’). In the present sample the α-coefficient for the scale was 0.92.
Procedure
The University of Melbourne Human Research Ethics Committee granted approval for the study. Sixteen Greek community social clubs in the Melbourne metropolitan area were approached (i.e. elderly citizens clubs, activity clubs, women's clubs) for their willingness to participate in recruitment of the sample. All clubs participated. Nineteen AA social clubs (i.e. Rotary clubs, sports clubs, elderly citizens clubs, women's clubs) in the same geographical areas were approached and of these 13 participated. At participating clubs the researcher explained the purpose, methods and confidentiality issues of the research to an audience and at the end of the presentation and discussion, members of the audience were invited to participate. For the GB, 215 out of 520 people were interested but only 151 were interviewed for this study (the sample for analysis is truncated to 146 participants taking only those ≥ 50 years). For the AA sample, 158 out of 372 questionnaires that were distributed were completed. No information could be collected from non-participants.
Scales were administered by one researcher (LK) to GB participants as an interview due to the suspected (and verified) low literacy levels in the Greek language. All interviews for the GB were conducted in Greek at participants’ homes. AA participants completed questionnaires on their own. All provided written consent to participation. Statistical analyses were undertaken using SPSS V 10 [32]. Statistical methods are described in the Results section for the sake of brevity.
Results
Sample characteristics
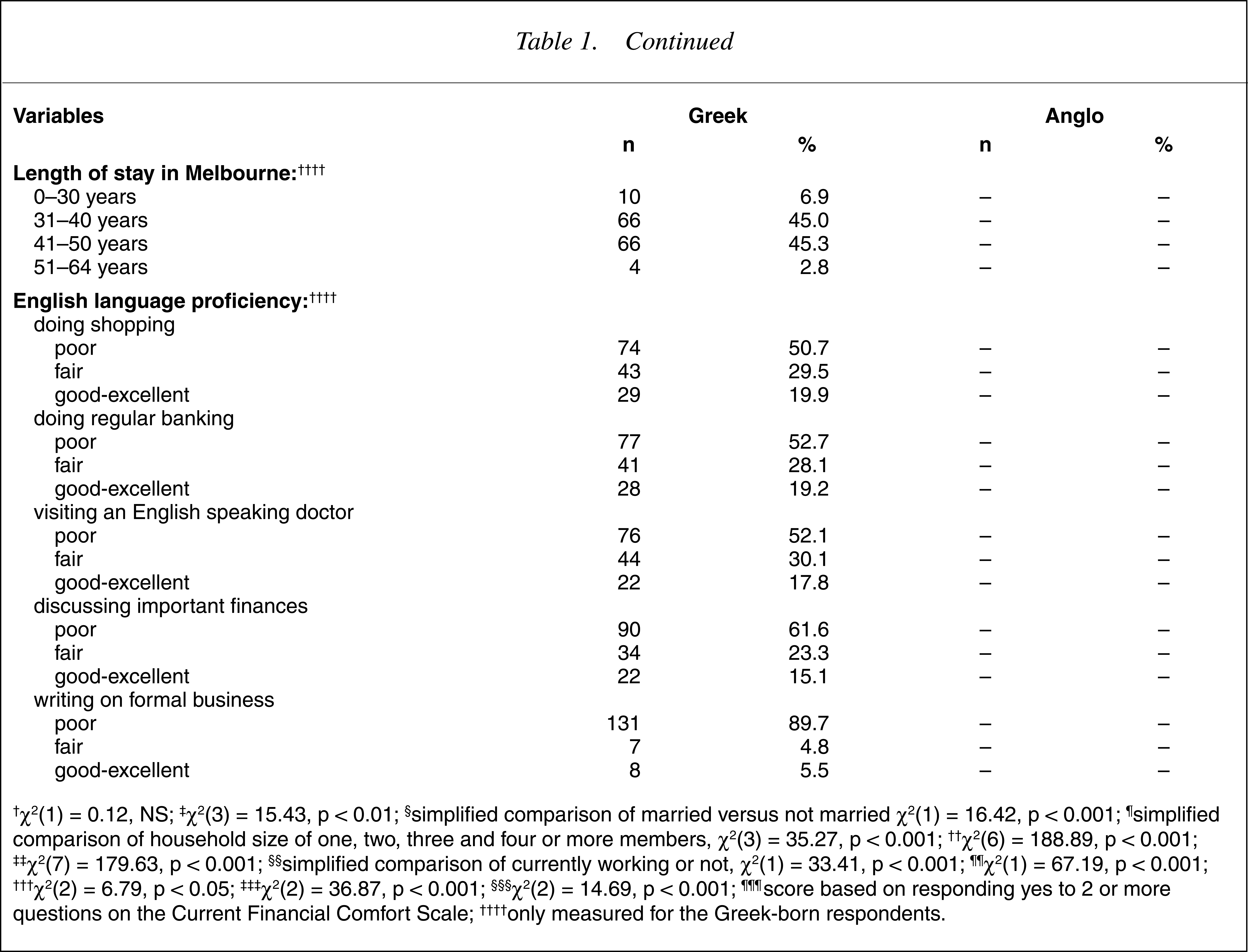
Table 1 summarizes the characteristics of the groups. As evident from Table 1, despite similar procedures in sampling, the groups differed on a wide range of characteristics. Multivariate analysis of variance revealed an overall significant difference across the groups over the various measures (Wilk's λ = 0.30, F = 58.17; df = 11; p < 0.001). Univariate descriptions were sought using λ2 comparisons and results to these are summarized in Table 1 (see caption). Overall, the GB compared to the AA sample did not differ on sex distribution but were significantly: older; currently married; lived in larger households (including being more likely to be living with spouse, children and other relatives); had lower levels of education; worked in lower status occupations during their working life (particularly in unskilled work), less likely to be currently working; less financially comfortable; more likely to report above-average memory functioning; less likely to report their physical health condition to be very good to excellent; and more likely to have scored in the higher experienced stress categories. Two of the descriptors summarized in Table 1 pertain only to the GB. Overall, very few were recently arrived in Australia with over 90% having lived in Australia for 31–50 years. Nevertheless indicators of English language proficiency suggested major difficulties in communication for at least half the sample. For example 51% rated their language ability as ‘poor’ and an additional 29% rated it ‘fair’ in doing their regular shopping (the easiest situation measured). Eighty-two percent rated their ability to communicate with an English-speaking doctor as ‘poor’ or ‘fair’ and 90% rated their ability to write on formal business in English as ‘poor’.
Demographic characteristics of respondents
The relationship between descriptive variables and psychopathology
Given that the groups differed substantially across a range of variables we explored the possible association between these variables and dependent measures from the BDI and STAI (in each case total raw scores and number of symptoms reported). Any group differences on the BDI and STAI could be attributed to differences in these background characteristics if these indeed affect the variance in the dependent variables. Table 2 summarizes the correlations between descriptor variables and the dependent measures, breaking down analyses for the whole sample and the two birthplace groups. As evident from Table 2, most of the descriptor variables were associated with the dependent variables, suggesting the requirement for adjusting for them when comparing the groups.
Correlations between descriptor variables and dependent measures across Greek-born and Australian-born groups
Direct comparisons between groups
Comparisons were made between groups, considering birthplace and sex as main effects. Direct effects (Table 3) were examined using twoway analyses of variance. In relation to total BDI scores the main effects of birthplace and sex were found to be significant but the interaction was not. GB women scored higher than their corresponding contrast groups. The same outcomes were found when analyzing the number of BDI symptoms reported (using an item score of 2 or higher to count for presence of any symptom). In general, the GB reported 3.5 symptoms compared with 1.3 for AA respondents. Furthermore, when the sample was classified into the four depression level categories of the BDI, significant differences were observed in the distributions of the two groups into the lower and higher categories. Comparison of minimal depression against the remaining upper three categories indicated a relative risk of 2.03, 95% CI = 1.18/3.50, for the GB to be distributed into the upper three categories compared with AA respondents. There was also a greater tendency for the GB, relative to AA respondents, to be classified in the moderate and severe categories than the lower two symptom categories (relative risk = 4.82, 95% CI = 1.91/12.14).
Statistics relating to the direct comparisons between groups (birthplace and sex)
Similar analyses were conducted with respect to anxiety scores from the STAI. As indicated in Table 3, the GB scored significantly higher on the STAI and reported more symptoms than the AA sample. This was evident as significant main effects for birthplace. The effect of sex was also significant in relation to STAI total scores with higher scores for women than men but not in relation to the number of symptoms reported from the STAI. The interactions between birthplace and sex were not significant. Comparisons on score categories from the STAI indicated a greater proportion of the GB sample to have scored in the upper three categories than the lowest one compared with the AA respondents, a trend found to be statistically significant (Table 3). Comparing group membership into the lowest and the upper three categories indicated a higher relative risk for GB compared with AA respondents into the upper three categories (22.72, 95% CI = 10.37/ 49.79). Using a mid-point split on the scores from the STAI, the relative risk of Greeks compared with Anglo-Australians in scoring in the two upper score categories was 4.06, 95% CI = 2.34/7.06.
Adjusted comparisons between groups
Given the differences indicated between groups on background descriptive variables and the relationship between these variables and the dependent variables, group comparisons were undertaken while adjusting for the effects of the background variables. Analyses of covariance (ANCOVA) were employed for this, retaining the same two-factor design (birthplace · sex) as in the analyses of variance. Additional hierarchical multiple regressions were used, entering birthplace and sex in the first entry and then the remaining variables. This was done to assess the overall contribution of the variables to the variance in scores on the dependent variables and to assess the unique contributions of variables to the variance of the dependent variables. To examine the effects of being classified in the upper score categories of the BDI and STAI, hierarchical logistic regressions were also employed. Results essentially complemented the findings demonstrated through other statistical methods and are not reported here.
For BDI total scores, ANCOVA exerted a significant effect on BDI total scores (F = 12.13; df = 10; p < 0.001) with particular effects from the following variables (interpreted in the direction of their effects): not married status (F = 16.25; df = 1; p < 0.001); low education (F = 33.80; df = 1; p < 0.001); lower memory functioning (F = 7.10; df = 1; p < 0.01); poor physical health status (F = 24.07; df = 1; p < 0.001); and higher experienced stress (F = 33.62; df = 1; p < 0.001). Once the effects of the covariates were taken into account, the main effects of birthplace and sex and the interaction between birthplace and sex were not significant (in all cases, F < 1.00; df = 1; p > 0.05). As expected, hierarchical linear regression analyses replicated the findings from ANCOVA but also indicated that with all the variables in the model 28% of the variation in BDI total scores could be predicted (adjusted R 2 = 0.275, F = 10.15; df = 12; p < 0.001). Significant independent predictors were: not married status, β = 0.20, t = 3.22, p = 0.002; poor memory score, β = −0.12, t = 2.29, p = 0.023; poor physical health status, β = −0.19, t = 3.26, p = 0.001; and higher experienced stress, β = 0.32, t = 5.84, p = 0.000.
ANCOVA of the number of reported BDI symptoms indicated a significant overall effect of the covariates (F = 12.58; df = 10; p < 0.001). Significant effects were observed from the following variables: not married status (F = 8.99; df = 1; p < 0.01); low education level (F = 63.47; df = 1; p < 0.001); lower memory functioning (F = 8.20; df = 1; p < 0.01); poorer physical health status (F = 16.10; df = 1; p < 0.001); and higher experienced stress (F = 22.54; df = 1; p < 0.001). The main effects of birthplace (F = 2.92; df = 1; p = 0.088) and sex (F < 1.00; df = 1; p > 0.05) and the interaction between birthplace and sex were not significant (F < 1.00; df = 1; p > 0.05). Regression analysis, as above, indicated that with all variables in the model 29% of the variation in symptoms reported on the BDI was accounted for (adjusted R 2 = 0.289, F = 10.80; df = 12; p < 0.001). Significant independent predictors were: not married status, β = 0.15, t = 2.45, p = 0.015; poor memory score, β = −0.14, t = 2.74 p = 0.007; poor physical health status, β = −0.14, t = 2.51, p = 0.013); and higher experienced stress, β = 0.26, t = 4.73, p = 0.000. The effect of birthplace in the case of regression analysis failed to achieve statistical significance in the presence of other covariates (β = 0.13, t = 1.45, p = 0.148).
Turning to the analysis of STAI responses, ANCOVA on total STAI scores indicated an overall effect of the covariates (F = 21.44; df = 10; p < 0.001) with particular effects being significant, including those of the following: greater household size (F = 3.90; df = 1; p < 0.05); not married status (F = 17.26; df = 1; p < 0.001); lower education (F = 91.52; df = 1; p < 0.001); lower occupational status (F = 21.35; df = 1; p < 0.001); lower financial comfort (F = 11.61; df = 1; p < 0.01); poor physical health status (F = 37.90; df = 1; p < 0.001); and higher experienced stress (F = 24.46; df = 1; p < 0.001). In the presence of the covariates the main effect of birthplace remained significant (F = 18.65; df = 1; p < 0.001). The effect of sex (F < 1.00; df = 1; p > 0.05) and the interaction (F = 2.96; df = 1; p = 0.087) were not significant. Linear regression with all variables included in the analysis revealed that 43% of the variance in STAI total scores could be predicted (adjusted R 2 = 0.432, F = 19.33; df = 12; p < 0.001). Unique predictors of STAI total scores were as follows: younger age, β= −0.13, t = 2.42, p = 0.016; not married status, β= 0.19, t = 3.48, p = 0.001; lower occupational status, β= −0.22, t = 2.49, p = 0.013; poor health status, β= −0.22, t = 4.30, p = 0.001; higher experienced stress, β= 0.22, t = 4.52, p = 0.000; and Greek birthplace, β= 0.35, t = 4.37, p = 0.000. Of note, the βcoefficient for birthplace in the presence of the covariates is moderately reduced from its direct effect (β= 0.50, t = 9.78, p = 0.000) in the absence of the covariates.
Covariance analysis of reported symptoms on the STAI indicated an overall effect of the covariates (F = 11.83; df = 10; p < 0.001). Several of the covariates contributed significantly to STAI symptoms variance including the following: greater household size (F = 9.80; df = 1; p < 0.01); not married status (F = 10.25; d.f. = 1; p <0.01); lower education (F = 44.17; df = 1; p < 0.001); lower occupational status (F = 8.05; df = 1; p < 0.01); lower financial comfort (F = 6.31; df = 1; p < 0.05); poor physical health status (F = 36.89; df = 1; p < 0.001); and higher experienced stress (F = 7.74; df = 1; p < 0.05). Despite accounting for these, the main effect of birthplace was statistically significant (F = 6.07; df = 1; p < 0.05). The effects of sex (F < 1; df = 1; p > 0.05) and the interaction of birthplace and sex were not significant (F = 2.63; df = 1; p > 0.05). Regression analysis indicated that the model with all the variables included accounted for 28% of the variation in the number of symptoms reported from the STAI (adjusted R 2 = 0.279, F = 10.30; df = 11; p < 0.001). Unique predictors included: greater household size, β= 0.15, t = 2.19, p = 0.030; not married status, β= 0.19, t = 3.00, p = 0.003; poor physical health, β= −0.27, t = 4.74, p = 0.000; higher experienced stress, β= 0.11, t = 2.05, p = 0.042; and Greek birthplace, β= 0.21, t = 2.34, p = 0.020). As above, the β coefficient for birthplace in the absence of other covariates was.42 (t = 7.86, p = 0.000) so its reduction, but not elimination, by the presence of the covariates would suggest that only some of the relationship between birthplace and number of STAI symptoms is accounted for by the background descriptor variables.
Associations between residence in Australia, English language and psychopathology
Correlations between years of residence in Australia and the dependent measures for the GB sample indicated no significant relationship between years of residency in Australia and the BDI-2 total score (r = −0.09; df = 146; p > 0.05), the number of BDI-2 symptoms reported (r = −0.12; df = 146; p > 0.05), the STAI total score (r = −0.08; df = 146; p > 0.05), or the number of STAI symptoms reported (r = −0.13; df = 146; p > 0.05). Similarly, no significant relationship was found between the English Language Proficiency and the BDI-2 total score (r = −0.03; df = 146; p > 0.05), the number of BDI-2 symptoms reported (r = −0.03; df = 146; p > 0.05), the STAI total score (r = 0.00; df = 146; p > 0.05) or the number of STAI symptoms reported (r = −0.07; df = 146; p > 0.05).
Discussion
The main result is that similarly recruited groups of GB and AA showed remarkably different levels of morbidity relating to common disorders as evident by BDI-2 depression and STAI measures. In direct comparisons, the GB scored significantly higher on morbidity measures compared with AA respondents. However, caveats to drawing confident conclusions include the difficulty in assessing the generality of the findings given that the groups were relatively small, were selected from among those in contact with social clubs and were self-selected to the study and thus may not be representative of older GB and AA communities in Melbourne. It could be assumed however, that those participating in the study may represent the more ambulant and socially connected from among the older populations, giving rise to the possibility that we have under-estimated the true rates of depression and anxiety [33]. In the present samples, rates of ‘past two weeks’ depression of at least mild form for the AA sample was found at 18.5% and at least moderate depression at 4.1%. The corresponding rates for the GB sample were 31.5% and 17.1%. ‘Past two weeks’ anxiety with at least scores of 31 or above on the STAI was indicated in 53.2% of the AA sample and with at least scores of 41 on the STAI in 15.8%. The corresponding rates for the GB were 94.5 and 43.1. Score ranges above 50 on the STAI indicated rates of 3.5% and 13% for the AA and GB samples, respectively. Compared with the NSMHW, rates appear to be substantially higher in the present study, particularly as they represent a twoweek measuring period compared with the 12-month period employed in the NSMHW. Both studies used community sampling (not including older institutionalized groups of people) and the large discrepancy in findings require additional research into rates of mental disorders among older members of the community.
The higher rate of depression and anxiety in Greeks is consistent with previous findings of high levels of ‘neurotic’ symptoms and anxiety disorders in the Greek population and in Greek-born immigrants [6–8],[33–41]. Mavreas and Bebbington [40] suggested that cultural norms and values such as ‘philotimo’ and child-rearing emphasizing over-protectiveness in Greeks may lead to a sense of insecurity, contributing to emotional disorders such as anxiety. However, previous comparative studies, particularly with Greek immigrants, have not taken the effects of social, economic and health factors into account when comparing Greeks with other cultural groups. Not being married (i.e. widowed or divorced), low education level, low memory functioning, poor physical health and higher experienced stress are all factors that have been demonstrated here to influence levels of reported depression and anxiety and any future research comparing immigrant and host-culture groups must take such factors into account.
The higher rate of morbidity in the GB than the AA calls into question the view that immigrant groups are relatively equal in psychological morbidity to the host community, as implied by findings of the NSMHW. Particularly challenging is that this finding is in the context of having achieved a sample of older Greeks with demonstrably low levels of English proficiency, a group that would have been excluded from the NSMHW. Moreover, results indicated that the longerterm settled communities such as the GB in Australia cannot be assumed to be psychologically healthy. The majority of the present sample of GB have been resident in Australia between 31 and 50 years. Much of the recent research attention in Australia has been on recently arrived people and particularly those with humanitarian entrance [e.g 42]. With a relative dearth of studies on the longer-settled communities that may be facing new adaptation challenges of late lifespan, for example deteriorating health status, reduction of social networks through death and emigration of peers, retirement and intergenerational conflicts with their children as the latter adopt more assimilative lifestyles within the host culture than their parents.
However, the present study is not conclusive regarding the higher relative disorder among GB than AA older generations, due to the methodological limitations imposed by the low literacy levels in the former group who were assessed by the administration of the questionnaires, while the latter group could reply through selfreport. Additionally, differences in relative rates between the two cultural groups could be attributed to the translation of the BDI-2 and the STAI. Translations may not have been linguistically ‘equivalent’ and may have been measuring different concepts, However, preliminary factor analyses with each sample (not reported here) revealed a similar structure and replicated previous findings [9]. Nevertheless, there remains potential for different thresholds between language versions for the detection of disorder.
While sample selection was similar, including sampling from the same localities as a broad control for socioeconomic variation, results showed that the two samples were remarkably different on a wide variety of social, economic and health status variables. Most important differences included that the GB, relative to the AA respondents, were significantly more likely to be currently married, lived in larger households (particularly living with relatives), had lower levels of education, had worked in lower status occupations during their working life, were less likely to be working, were less financially comfortable, were less likely to report possessing good physical health and were more likely to have experienced higher stress levels in the past six months based on the number and degree of life impact of serious adverse events. All these factors were considered in the analysis of psychopathology differences between groups as putative determinants of morbidity and indeed, were shown to be associated with variance in symptom reports between or within the groups studied.
Commensurate with this, the present study showed associations between depression and anxiety and Greek birthplace, being female, low education and occupational levels, low current financial status, not currently working, low memory functioning and high levels of stress for both birthplace groups. Higher household size was also associated with higher anxiety and not being married was associated with depression. These findings are generally consistent with previous research, including studies in different cultural groups [11], [12], [14], [15], [17], [27],[43–47]. A recent review of community prevalence of depression in later life [11] indicated that practically all studies, including cross-cultural studies, reported associations between depression and indicators of socioeconomic status such as educational level, occupational status and income. Cross-cultural studies have indicated depression is associated with low family income, low occupational grade, poor education, unemployment, being female and income being inadequate for personal needs [27], [44]. Additionally, in the elderly, low education and experiencing financial strain have been associated with depression [12]. Furthermore, studies examining depression and anxiety in adult and elderly Greeks have shown that those with lower education, those in unskilled manual work, the unemployed and those generally living under stressful low socio-economic conditions, were more likely to have reported a greater number of depressive, anxiety and psychosomatic symptoms [34], [35], [45]. Contrary to expectations, in the present work English proficiency was not correlated with depression and anxiety measures for the GB. However, this could be attributed to the low variance of the English language proficiency measure, as most of the GB sample scored on the lower end of the scale (i.e. poor) even for the lower communicative difficulty items.
The major theoretical contribution of the present analysis relates to the relationship between ‘culture’ (represented by birthplace), the social, economic and health differentials between groups and psychopathology outcomes. In the case of depression, all of the variance in depression attributed to ‘culture’ could be explained through the effects of social, economic and health determinants. While BDI scores and number of symptoms differed between groups, when adjusting for differences in social and health conditions, effects of birthplace were completely removed or explained. In Fig. 1, this is indicated by the arrows linking culture with social, economic and health conditions and depression. In other words, cultural differences in symptomatology appear to be most likely due to the relative status on social and health conditions of the immigrant group rather than to other factors related to culture or immigrant status, a result consistent with early conclusions regarding the role of different life conditions determined by migration [48–51]. In the present findings the background factors consistent across the three dependent variables from the BDI in explaining away the effect of culture were ‘not married’, compromised physical health status and experiencing recent stress.
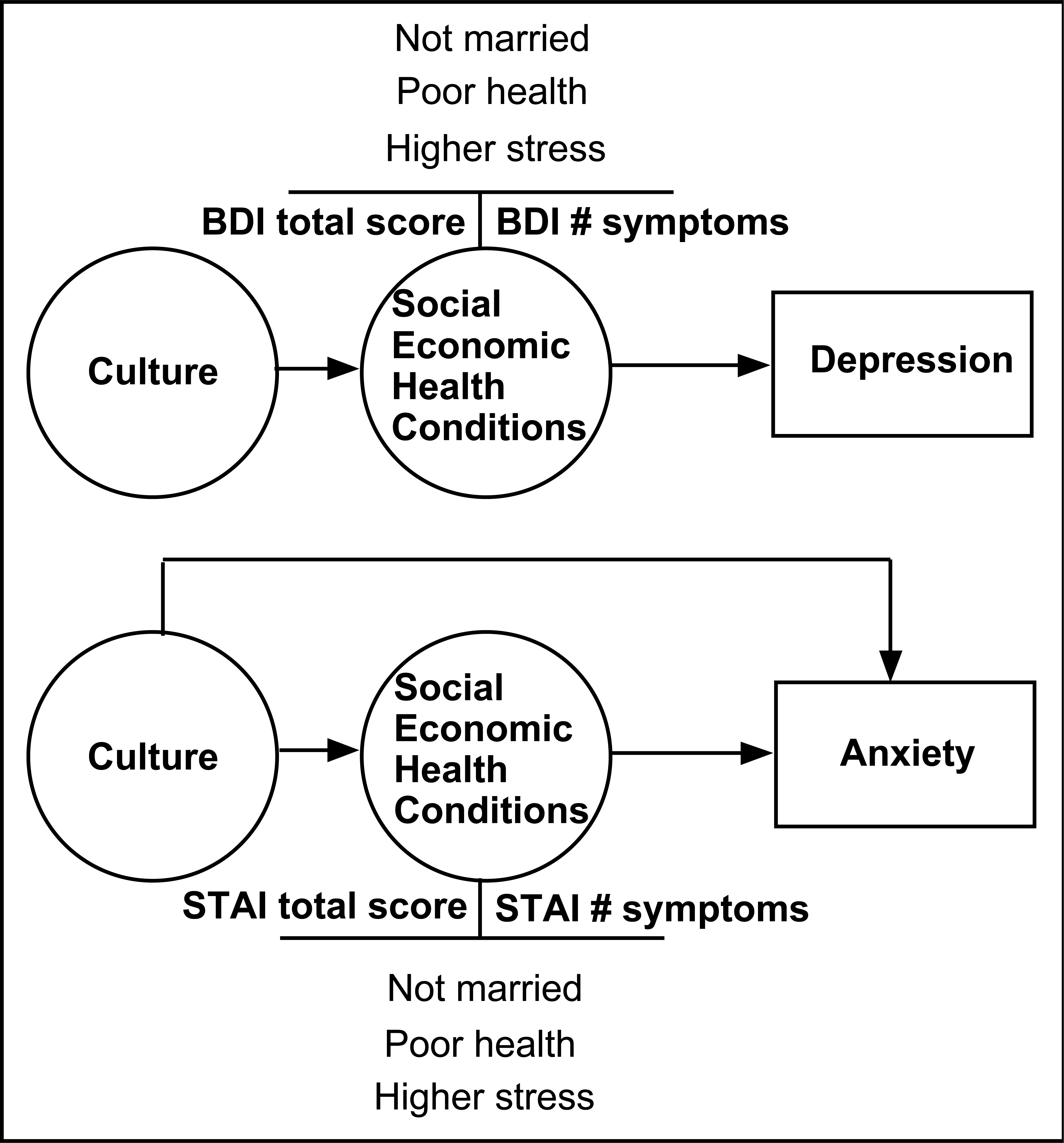
Schematic representation of regression analysis findings related to the relationship between culture, social and health conditions and psychopathology.
In the case of anxiety (Fig. 1) much of the variance in scores and symptoms could be attributed to social, economic and health conditions but these did not entirely remove or explain the effects of ‘culture’. Indeed the same background factors as in depression were common mediators for the two STAI indicators. However, additional variance to symptomatology was explained by ‘culture’, raising the possibility that either cultural or other immigrant factors not measured, contributed to the symptomatic differences between groups.
The three common predictors of morbidity (‘not married’, compromised physical health status and experiencing recent stress) are sensible in the context of older age. The ‘not married’ represent those widowed, separated or divorced with a common theme being the possible absence of intimate social supports to buffer the effects of stress or to contribute to greater personal (rather than shared) effort in negotiating life challenges. Social isolation is one of the most recurring difficulties indicated in older members of the community and particularly highlighted in local Australian studies of elderly immigrants [e.g 52]. With the greater and rising proportion of elder immigrants in the Australian community [53] this is a significant problem and challenge to strategies designed to prevent or ameliorate common mental disorders. Additionally, older age constitutes a period of increasingly compromised physical health status with many among the elderly suffering from multiple and often chronic diseases [54]. The contribution of poor health to mental disorder highlights the need to attend to the issue of comorbidity in the older members of the community. Finally, recent stressors have been linked aetiologically to both depression and anxiety disorders [14], [23], [24] consistent with the present results. While little can be done to reduce exposure to adversities, improved understanding of how their impact may be reduced in the elderly is of great importance to designing effective prevention strategies for mental disorders in this group. The present study also indicates that the effects these three factors have on psychological morbidity are additive in older-aged people, that is, they contribute uniquely to symptomatic status in relation to depression and anxiety. Thus, the most vulnerable constitute those older members of the community outside a marital relationship, whose physical health status is compromised and who are experiencing significant adversities.
In conclusion, the present work, though small in scale, has questioned the generalizations made from the NSMHW results [1] in relation to older groups in the Australian community and particularly those most likely to have been excluded by the sampling procedures – those with poor English language proficiency. In addition, it has highlighted major differences in social, economic and health conditions between immigrant and host community members, despite similar sampling procedures and has indicated how cultural or immigrant status differences in psychopathology could be accounted for, at least in part, by the major differences in social, economic and health conditions existing in immigrant and host communities. Additional research is needed to extend these observations to the broader immigrant community, with possibly more representative sampling and methodological refinements, such as the use of a common assessment method between host and immigrant samples.