
Abstract
In recent years it has increasingly been recognized that the opinions and attitudes of the public have important implications for the treatment and prevention of mental disorders and that these views are therefore worthy of systematic investigation [1], [2]. A body of knowledge has now accumulated concerning the ability of individuals in the general population to recognize particular mental disorders, their beliefs as to the helpfulness of different types of intervention and likely prognosis, and the perceived significance of various causes and risk factors [1]. Jorm et al. [3] have used the term ‘mental health literacy’ to refer to this field of investigation.
While the views of eating disorder patients concerning the causes of their eating disorder have occasionally been solicited in the course of follow-up research [4], [5], we are aware of only one study in which the opinions of individuals in the general population concerning the aetiology of eating-disordered behaviour have been considered. Smith et al. [6] reported that high school and college students were more likely to consider emotional problems as a cause of eating disorders than other possible causes, such as the influence of family members, pressure from men and the influence of the media. We have recently examined the views of women in the community concerning a range of issues associated with bulimia nervosa (BN). Findings concerning women's beliefs about the treatment of BN have been reported previously [7]. Here we report findings concerning women's beliefs about causes and risk factors for BN.
Method
The survey was carried out as part of a two-phase epidemiological study of eating-disordered behaviour in the Australian Capital Territory (ACT) region of Australia (population 314 000), a highly urbanized area which includes the city of Canberra. At the first phase of the study, self-report questionnaires were delivered to a sample of 802 female ACT residents aged 18–45 years, selected at random from the electoral roll. The questionnaire included a screening instrument for eating disorders, as well as measures of general psychological distress, impairment in role functioning, weight and height and sociodemographic information [8].
All individuals who returned completed questionnaires and who indicated a willingness to be contacted by telephone at a future date (n = 308) were approached to participate in a second phase of the study, involving a face-to-face interview. Interviews were completed with 208 individuals. The mean age of the interviewed sample was 35.3 years (SD = 8.5), while mean body mass index (BMI) was 25.2 kg/m2 (SD = 5.4). Interviewed subjects did not differ from subjects not interviewed with respect to levels of eating-disorder psychopathology or on other study measures [9].
The mental health literacy survey
The survey was administered at the start of the phase-two interview and was modelled on Jorm et al.'s [3] protocol, with modifications by the authors (JM and PH) for the study of eating-disordered behaviour. A vignette describing a 19-year-old woman who met DSM-IV diagnostic criteria for bulimia nervosa (purging subtype) [10] was first read aloud by the interviewer (Table 1). A prompt card was provided so that the subject could follow the description as it was read and subjects were advised that they could refer back to the vignette at any time during the interview.
Vignette used in the mental health literacy survey
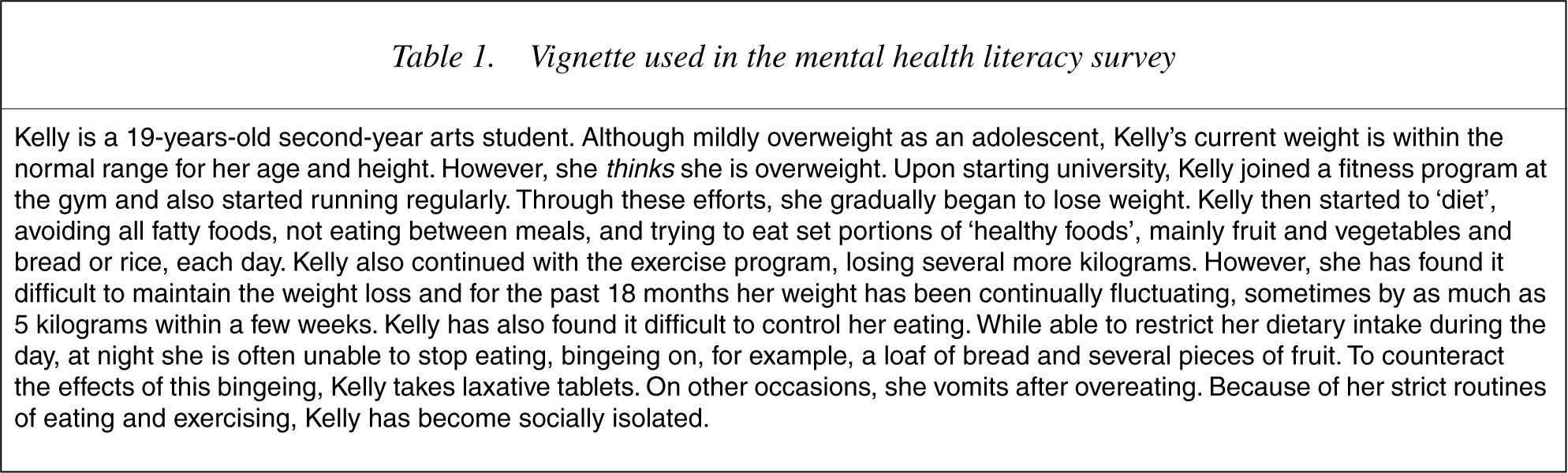
Following presentation of the vignette, respondents were asked: ‘What would you say is Kelly's main problem’? Respondents were required to choose one answer only from a number of options. Listed in random order, these were: ‘bulimia nervosa’; ‘anorexia nervosa’; ‘a binge eating disorder or problem’; ‘yo-yo dieting’; ‘a nutritional deficiency’; ‘an exercise disorder or problem’; ‘low self-esteem or lack of self-confidence’; ‘depression’; ‘loneliness’; ‘an anxiety disorder or problem’; ‘stress’; ‘a hormone problem’; ‘diabetes’; ‘mental illness’; and ‘no real problem, just normal’.
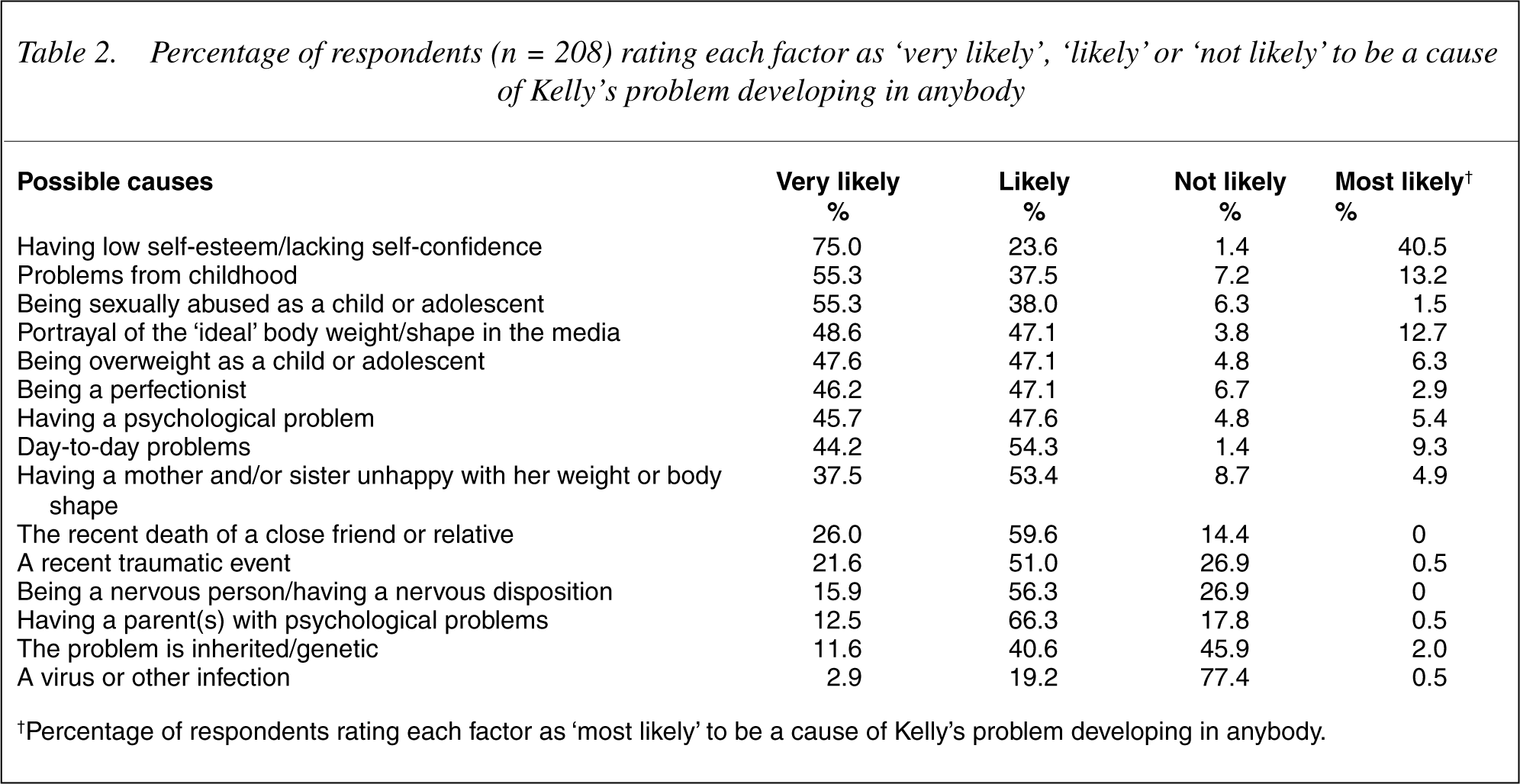
Respondents' beliefs concerning causes and risk factors were assessed with two questions. For the first question, respondents were required to indicate whether each of a series of possible causes was ‘very likely’, ‘likely’, or ‘not likely’ to be a factor in Kelly's problem developing in anybody. The options included situational factors, such as ‘problems from childhood’ and ‘portrayal of women in the media’, and dispositional factors, such as ‘having a nervous disposition’ and ‘being a perfectionist’ (Table 2). Respondents were also asked to indicate which single option they considered most likely to be a cause of Kelly's problem developing in anybody (‘the main cause’).
Percentage of respondents (n = 208) rating each factor as ‘very likely’, ‘likely’ or ‘not likely’ to be a cause of Kelly's problem developing in anybody
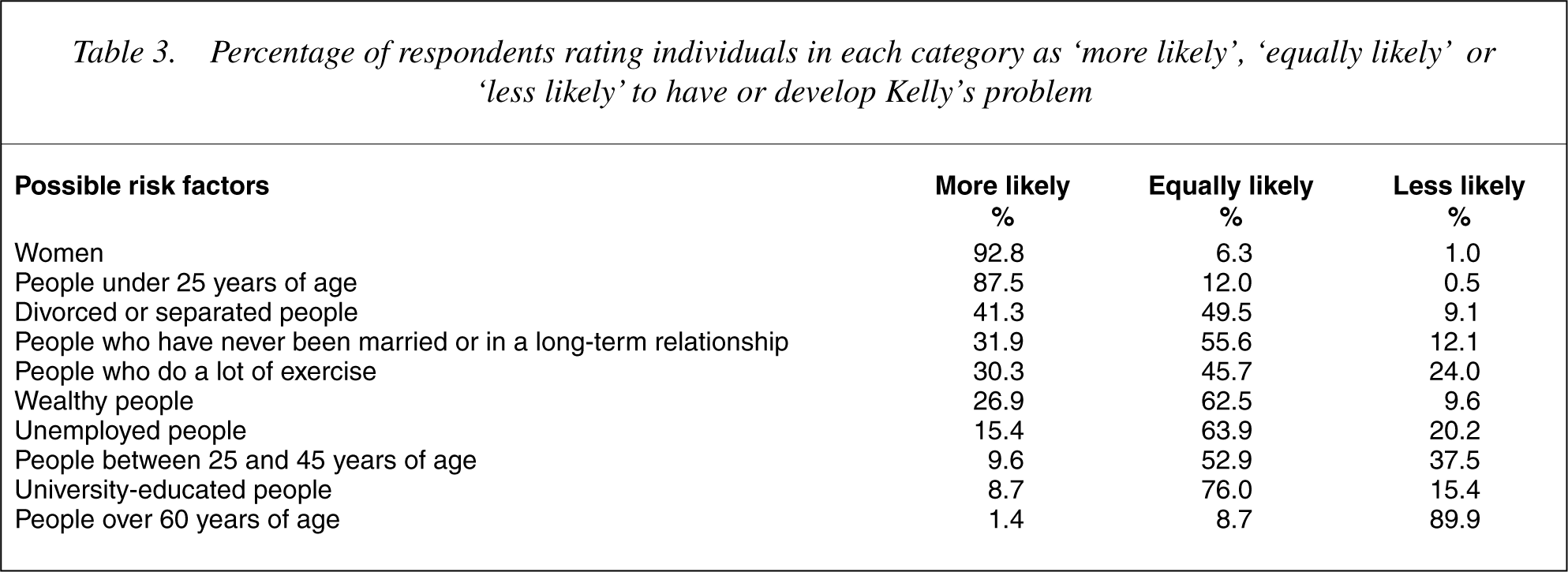
The second question, concerning risk factors, was prefaced by the statement: ‘This question is about whether some people in the community might be more likely to have Kelly's problem than others’. Respondents were then asked to decide whether individuals in each of a number of categories of people were ‘more likely’, ‘less likely’ or ‘equally likely’ to have or develop Kelly's problem. The categories reflected the possible role of various socio-demographic factors, such as age, gender and marital status (Table 3). Respondents were also asked to indicate which subgroups – or combination of groups – they thought would be most likely to have or develop Kelly's problem.
Percentage of respondents rating individuals in each category as ‘more likely’, ‘equally likely’ or ‘less likely’ to have or develop Kelly's problem
The interview ended with questions concerning respondents' personal experience of the problem described in the vignette, namely: ‘Do you think that you might currently have a problem like Kelly's?’; ‘Do you think you have ever had a problem like Kelly's?’; and ‘Has anyone in your family or circle of friends ever had a problem like Kelly's?’
Statistical analysis
Data are presented as the percentage of respondents choosing particular options for each question. The effects on responses of sociodemographic characteristics (age and education), recognition of the problem, and self-reported experience of the problem described, were examined by means of χ2 tests. A significance level of 0.05 was adopted for these tests.
Results
In response to the question ‘What would you say is Kelly's main problem’?, more than half of the respondents (55.1%) chose ‘low selfesteem’, followed by ‘binge eating disorder or problem’ (19.8%), ‘bulimia nervosa’ (11.1%) and ‘yo-yo dieting’ (3.9%). Together, these responses accounted for 89.9% of all responses.
Table 2 shows the percentage of respondents who considered each option as ‘very likely’, ‘likely’ or ‘not likely’, to be a cause of Kelly's problem developing in anybody, ordered by frequency of endorsement of the ‘very likely’ option. It can be seen that 75% of respondents indicated that ‘having low self-esteem’ was very likely to be a cause. ‘Problems from childhood’ (55.3%) and ‘being sexually abused as a child or adolescent’ (55.3%) were the only other options rated as very likely by a majority of respondents, though most options were considered either likely or very likely to be causes by the overwhelming majority of respondents. ‘A virus or other infection’ was the only option considered unlikely to be a cause of the problem described by a majority of respondents (77.4%), though close to half (45.9%) considered it unlikely that Kelly's problem was genetically transmitted. ‘Having low self-esteem’ was also most frequently endorsed as the main cause (40.5%), followed by ‘problems from childhood’ (13.2%), ‘portrayal of women in the media’ (12.7%), ‘day-to-day problems’ (9.3%) and ‘being overweight as a child or adolescent’ (6.3%) (final column, Table 2).
Table 3 shows the percentage of respondents who considered particular categories of people to be ‘more likely’, ‘equally likely’ or ‘less likely’ to have or develop the problem described, ordered by frequency of endorsement of the ‘more likely’ option. It can be seen that most respondents considered ‘women’ (92.8%), and ‘people under 25 years of age’ (87.5%), to be more likely to have or develop Kelly's problem, while significant proportions of respondents believed that ‘being divorced or separated’ (41.3%), ‘never having been in a longterm relationship’ (31.9%), ‘doing a lot of exercise’ (30.3%), and ‘being wealthy’ (26.9%), placed individuals at greater risk. Also, most respondents (89.9%) believed that people over 60 years of age were less likely to have or develop the problem described.
When asked to name the category or categories of individual most likely to have or develop Kelly's problem, 57.0% of respondents nominated ‘women under 25 years of age’, while a further 13.6% of respondents chose more complex combinations involving women under 25 years of age.
Factors affecting responses to particular questions
Identification of the main problem
Respondents who indicated that Kelly's main problem was low selfesteem (n = 114) were more likely to consider day-to-day problems (very likely: 48.2% vs. 33.3%; p < 0.05) and low-self esteem (very likely: 83.3% vs. 68.1%; p < 0.05) as causes than respondents who identified the main problem as bulimia nervosa, binge eating disorder or yo-yo dieting (n = 72). The proportion of respondents who identified low self-esteem as the main cause was higher among individuals who identified low self-esteem as the main problem (48.2% vs. 33.3%), though not significantly so (p =0.43).
Age and education
Respondents aged 18–32 years (mean = 24.0, SD = 4.2, n = 65) were more likely than respondents aged 33–45 years (mean = 40.5, SD = 3.6, n = 142) to consider low self-esteem (very likely: 86.2% vs. 69.7%; p < 0.05) and being overweight as a child or adolescent (very likely: 63.1% vs. 40.1%; p < 0.05) as causes, and more likely to consider low self-esteem as the main cause (57.8% vs. 32.9%; p < 0.01). There were no differences in responses to any question between respondents who had commenced or completed an undergraduate or postgraduate degree or diploma (n = 104) and those who had not undertaken tertiary study (n = 103) (all p < 0.05).
Experience of the problem described
Respondents who believed that they might currently have a problem such as the one described, or that they had such a problem in the past (n = 52, 26.2%), were more likely to consider being sexually abused as a child or adolescent (very likely = 66.7% vs. 52.2%; p < 0.01) as a cause, and more likely to consider low self-esteem (47.9% vs. 37.4%; p < 0.05) as the main cause. Respondents who indicated that they were aware of someone with a problem like Kelly's in their family or circle of friends (n = 116, 55.8%) were also more likely to identify being sexually abused as a child or adolescent as a cause (very likely = 64.9% vs. 45.1%; p < 0.05).
Discussion
The findings of the present study indicate that low selfesteem is perceived as the most important cause of bulimia nervosa among women in the general population. This was apparent not only in responses to the questions concerning causes, but also in responses to the initial question concerning the main problem of the person described. While it was not our intention, it appears that this question was interpreted as one of causation rather than diagnosis by many respondents. However, among those respondents who did interpret the question as one of diagnosis, the proportion who considered low self-esteem as very likely to be a cause was similarly high. Also, a subgroup of respondents who reported that they were currently affected by, or had previously experienced, a problem such as the one described, were more likely to consider low self-esteem as the main cause.
The notion that eating-disordered behaviour represents the surface expression of low self-esteem, and more generally of negative affect, is widely accepted in the eating disorders literature, evident in models of the aetiology of BN [11], [12] and in the fact that procedures designed to boost self-esteem are routinely incorporated in prevention programs [13–15]. Whether there may be benefits in addressing individuals' beliefs concerning risk factors – as opposed to identified risk factors per se – in prevention programs is unclear. Jorm et al. [1], [2] have stressed the importance of taking individuals' belief systems into account in ensuring that individuals affected by mental disorders receive optimal treatment. Similarly, it may be that information concerning risk factors for mental disorders will have greater impact if it is consistent with individuals' belief systems. Such an approach may be particularly useful in the context of secondary prevention programs for eating disorders, since evidence from clinical samples suggests that insight is poor among individuals affected by eating disorders [16]. Also, primary prevention programs have generally not been successful in modifying eating disorder attitudes and behaviours [17].
The fact that most respondents rated a number of other factors as either very likely or likely to be causes might also be viewed as being consistent with the literature, in that reviews of the aetiology of eating-disordered behaviour routinely divide putative risk factors into various domains – socio-cultural, developmental, personal vulnerability, familial, and the like, reflecting a consensus that the aetiology of eating-disordered behaviour is ‘multifactorial’ [13]. Aside from low self-esteem, ‘problems from childhood’, including sexual abuse and being overweight, portrayal of the ‘ideal’ body weight and shape in the media, and ‘day-to-day problems’, were the factors most often judged to be causes of the problem described. While there is good evidence for an association between each of these factors and the occurrence of BN, it is unlikely that any one confers a risk specific to eating-disordered behaviour. For example, in the 1980s childhood trauma, and in particular childhood sexual abuse, was commonly invoked as a risk factor for BN. Subsequently, through research employing cases recruited from the community and appropriate control groups, it has been shown that the occurrence of childhood sexual abuse is a risk factor for psychiatric disorders in general [18].
Of note is the finding that respondents who reported (current or past) personal experience of the problem described were more likely to consider being sexually abused as a child or adolescent as a cause. This tendency was also apparent among respondents who indicated that they were aware of someone in their family or circle of friends having experienced a problem such as the one described. There may be a greater awareness of the significance of childhood events for later development among individuals with personal experience of an eating disorder. Alternatively, these individuals may be more sensitive to the negative consequences of childhood adversity. Research addressing the beliefs of individuals with an actual eating disorder diagnosis, identified in a larger community-based sample, would be of interest in this regard. The finding that younger respondents were more likely than older participants to consider being overweight as a child or adolescent as a cause is also of interest, in that childhood obesity was one of only two risk factor domains specific to the development of BN in a recent community-based case-control study, the other being problems with parental relationships [19].
In contrast to the findings of Smith et al. [6], ‘having a psychological problem’ did not emerge as a salient risk factor among respondents in the present study. It is possible that the perceived significance of different causes has changed over the past two decades, during which time eating disorders have been the subject of intense media coverage. Also, participants in Smith et al. ′ s (1986) study were male and female high school and college students, while a more representative community sample of women participated in the present study. However, the belief that ‘having a nervous disposition’ is unlikely to be a risk factor is not consistent with research demonstrating that the occurrence of anxiety disorders frequently precedes the onset of eating disorder psychopathology [20]. Further, the presence of premorbid anxiety and/or affective disorders is the only factor consistently found to predict a transition from subclinical to clinical eating disorders in longitudinal studies [21], [22]. Information to this effect might usefully be incorporated in prevention programs.
The low importance attached to the role of genetic factors is also not consistent with the evidence. Multivariate analysis of data from twin and family studies suggests a substantial genetic liability for both anorexia nervosa (AN) and BN, though exactly what might be inherited is a matter of debate [23]. As Jorm et al. [24] noted, it is possible that members of the public tend to hold a simple Mendelian view of genetic influences, as opposed to a diathesis/stress model, and therefore do not see genetic factors as relevant in the aetiology of mental disorders. Alternatively, the minor significance attached to genetic factors may reflect an adherence to the view that eating-disordered behaviour represents one of several possible manifestations of a ‘general neurotic syndrome’, the particular expression of this trait being dependent on situational factors [25]. Attributions for mental disorders may have implications for treatment seeking. For example, individuals who attribute symptoms to childhood adversity may be more likely to seek psychoanalytically orientated therapies and less likely to seek biologically based treatments [7]. Prospective community-based research will be needed to address these hypotheses.
Findings concerning subgroups at greatest risk for the development of BN were unequivocal. Women in the community believe that women under the age of 25 are most at risk of developing a problem such as the one described. The literature is also unequivocal in this regard, in that AN and BN are overwhelmingly disorders associated with adolescent and young adult women [26]. In contrast, binge eating disorder (BED), listed in DSM-IV as an exemplar of the ‘Eating Disorders Not Otherwise Specified’ (EDNOS) category, may be more common among middle-aged women, and is not uncommon in men [27]. Replication of the present study using a vignette of BED would be of interest. It may be that the attribution of a psychiatric disorder is not made, given a scenario involving binge eating in the absence of extreme weight-control behaviours [28]. The perception that there is no association between socio-economic status and BN is also consistent with the evidence. While findings from some early studies suggested an association between levels of education and income and the occurrence of eating disorders, this hypothesis has since been discarded [29], [30].
Methodological limitations inherent in the mental health literacy paradigm have been noted previously [31]. In particular, the use of forced-choice response options is inevitably associated with the loss of information. In our previous study [7], some respondents protested that it was difficult to choose only one option on certain questions and a few refused to do so. The use of an adult sample might be considered a limitation, though the onset of BN typically occurs around 18 years of age [26], and that of BED somewhat later [27]. In any case, replication of the present study in an adolescent female sample would be of interest. A strength of the present study was the use of a general population sample of women. To our knowledge, this is the first study to consider the beliefs of women in the community concerning causes and risk factors for BN.
In conclusion, the findings of this study suggest that women are generally well informed about causes and risk factors for BN, in particular the significance of low self-esteem. However, information concerning the increased risk associated with pre-existing anxiety and affective disorders might usefully be included in prevention programs. A useful starting point for such initiatives may be to solicit participants' beliefs concerning risk factors for eating disorders, and other aspects of mental health literacy, in order that information may be tailored to participants' belief systems. Systematic investigation of the benefits of addressing individuals' beliefs concerning risk factors for eating disorders – as opposed to risk factors per se – would be of interest.
Footnotes
Acknowledgements
The research was conducted while the first author was in receipt of a Research Training Fellowship from the NSW Institute of Psychiatry.