
Abstract
Kazdin [1] coined the term ‘treatment acceptability’, which he defined as perceptual judgements made and attitudes about a treatment intervention held by potential consumers of the treatment, patients and lay people. He argued that evaluating treatment acceptability is critical when numerous treatment options are available but not necessarily satisfactory to the client. A patient's belief about the acceptability of the treatment may play a role in determining treatment adherence and outcome [2, 3], and poor treatment acceptability contributes to negative outcomes such as premature treatment cessation, non-compliance and slow improvement [4].
One area in which it is important to understand treatment acceptability is in relation to bulimia nervosa. In Australia, lifetime prevalence of bulimia nervosa in women has been estimated at 2.9% with a further 3.2% of women suffering from bulimic type disorders [5]. These disorders are often chronic and are associated with poor quality of life [6]. Despite these problems, only about 10% of symptomatic individuals access treatment [7]. Low access to treatment occurs despite empirical support for the efficacy of psychological therapies, particularly cognitive–behavioural therapy (CBT) [8] and, to a lesser but consistent extent, for antidepressant medication [8, 9]. Although these treatments have been shown to be efficacious, attrition rates are high, especially in the case of medication [9, 10]. In addition, many people use non-standard treatments such as relaxation, vitamin supplements and other lifestyle interventions to manage symptoms of bulimia [11, 12], despite little or no empirical evidence demonstrating their effectiveness [12]. These factors suggest that psychological and medication-based treatments may not be acceptable to all those in need of assistance; however, relatively little is known about predictors of treatment acceptability in bulimia nervosa.
We have used the concept of Mental Health Literacy [13] to guide an evaluation of predictors of acceptability of medication, psychological therapy and self-change/lifestyle treatments for bulimia nervosa. Mental Health Literacy refers to knowledge and beliefs about mental illnesses that facilitate their recognition, treatment and prevention [14]. Jorm [11] proposed that Mental Health Literacy influences attitudes and beliefs about the causes of mental illness and, subsequently, this affects attitudes and beliefs about the acceptability of treatment interventions. In Western societies, mental illnesses are predominately perceived by the community as being caused by psychological and social variables such as stress [15]. Biological and genetic causes are perceived to be less important as they are neither widely understood nor accepted as valid causes [11, 13, 16, 17]. These beliefs may underlie poor acceptance of pharmacological interventions [11]. In the treatment of schizophrenia, when the cause of the condition is attributed to a combination of lifestyle and biological factors, psychotropic medication appears to be more acceptable [18]. Beliefs concerning the causes of bulimia may predict acceptability of particular treatments.
Jorm and colleagues [13] observed that psychotropic medication was perceived as harmful in the treatment of various mental illnesses, whereas vitamins, increased physical activity and stress management were perceived as beneficial. Jorm et al.[14] found that people suffering from depression and anxiety disorders relied predominately on natural interventions to treat their illnesses despite limited research into their effectiveness. Beliefs about the effectiveness of the treatments appeared to influence treatment choices. Other perceived advantages and disadvantages may also predict treatment acceptability.
A small number of studies have examined the beliefs of women concerning the acceptability and helpfulness of various treatment interventions for bulimia nervosa. Mond and colleagues [12] found that 70% of adults surveyed identified vitamins and minerals as more beneficial in the treatment of bulimia than antidepressant medication. ‘Just talking about the problem’, ‘getting out more’ and relaxation therapy were highly endorsed by respondents despite minimal empirical support. Although psychological therapy was regarded as effective, general practitioners, dietitians or counsellors were perceived as more helpful in treating the condition than a psychologist or psychiatrist. Participants with a university education were more likely to value a psychologist in treating the condition compared to participants without university level education.
Mental Health Literacy also suggests that demographic variables such as age, educational attainment, past experiences with mental illness and treatment history may also predict treatment acceptability [18, 19]. Symptom severity is also a consistent predictor of use of different interventions and is believed to play a role in treatment preference [20].
The aim of the present research was to examine acceptability and correlates of acceptability of three treatments for bulimia nervosa: medication, psychological therapy and self-change/ lifestyle therapies in a sample of community women. A community sample was chosen, as previous research suggests that beliefs about treatment acceptability in symptomatic and community samples are largely congruent [21, 22]. It was hypothesised that psychological therapy would be the most acceptable treatment, followed by self-change/lifestyle therapies, and then medication, and that acceptability of each treatment would be correlated with beliefs about the cause of bulimia nervosa. Specifically, it was proposed that: acceptability of medication would be associated with a belief in biological causes of bulimia; acceptability of psychological therapy would be associated with belief in low self-esteem, social pressure to be thin and relationship and family causes; and that acceptability of self-change/lifestyle therapies would be associated with a belief in eating behaviour causes of bulimia nervosa such as dieting. It was hypothesised that acceptability of the treatment approach would be positively associated with perceived advantages and inversely associated with perceived disadvantages of that treatment. Psychological therapy was hypothesised to have more perceived advantages and fewer disadvantages followed by self-change/lifestyle therapies and then medication. Finally, it was hypothesized that treatment acceptability would be associated with: greater perceived acceptability of the treatment by others; education level; past experience and positive experience of the relevant treatment; and bulimic symptom severity.
Method
Pilot study
A pilot study was conducted with seven female participants aged 23–27 years (mean age = 24.4 years, SD = 1.27), who responded to advertisements placed on community notice boards. Participants in the focus group were asked questions to elicit beliefs about potential causes of bulimia, treatment attitudes, perceived advantages and disadvantages of the interventions, and perceptions of significant others of treatment interventions. The most frequently mentioned responses were included in each relevant subscale of the questionnaire.
Participants and procedure
Participants in the main study were 177 females, aged 18–53 years (mean age = 25.8 years, SD = 4.82), who responded to requests to complete a questionnaire placed around workplaces, university campuses, local gyms and in newspapers. Approval for the research was obtained from the La Trobe University Human Ethics Committee. Before completion of the questionnaire, participants read an information sheet with a study overview and were informed that they were free to withdraw from the study at anytime. Each participant completed the questionnaire anonymously and returned it by reply paid post.
Assessment questionnaire
Preliminary information
Preceding the assessment instruments, participants were provided with a brief description of a girl with bulimic symptoms in impartial language, to ensure a congruent understanding of bulimia by all individuals. A brief description of three treatment options for bulimia was also provided to enhance a clear and consistent appreciation of how each intervention is adopted in the treatment of the condition. Psychological therapy was described in the following manner: ‘Psychological therapy aims to change eating behaviours and attitudes. It works by the patient seeing a therapist over several months, usually once a week for a period of 4–6 months, and working to change behaviours, attitudes, beliefs and feelings’. Medication was described in the following manner: ‘Medication, such as antidepressants, reduces the amount of binge-eating and vomiting. Medication is also shown to reduce depression and obsessive thoughts associated with bulimia. A reduction of these symptoms allows patients to better cope with everyday life’. Self-change/lifestyle therapies were described as follows: ‘Self-change/ lifestyle therapies, while not a clinically proven intervention for bulimia, include activities such as acupuncture, yoga and meditation. They also involve increasing physical and social activities such as joining new clubs. Such interventions are not specifically designed to treat bulimia, however, they may help to promote well-being’. Participants were then requested to imagine that they were experiencing bulimic symptoms and complete the following questions accordingly.
Demographic assessment
Demographic questions included age, years of education, and marital status.
Treatment acceptability
Using the treatment acceptability measure developed by Norton and colleagues [21] as a framework, three-item scales were developed to assess treatment acceptability for each intervention. First, a brief intervention description was provided, followed by the items measuring treatment acceptability for the participant themselves, for people suffering from bulimia, and from an ethical point of view, including ‘If I had bulimia, I would consider psychological therapy to be 1 (very unacceptable) to 5 (very acceptable)’. Scores on the three items for each intervention were summed and then a mean score was derived.
Perceived acceptability of treatment by others
To assess perceived acceptability of each intervention, six items asked about the perceived acceptability of each treatment by six significant people (identified in the focus group): family, friends, doctor, health experts (e.g. fitness instructors), books and magazines, and work colleagues/supervisors; for example, ‘Indicate the extent to which your family would encourage you to use medication as a treatment for bulimia’ rated from 1 (strongly disagree) to 5 (strongly agree). Item scores were summed and then a mean score was derived.
Beliefs about the causes of bulimia
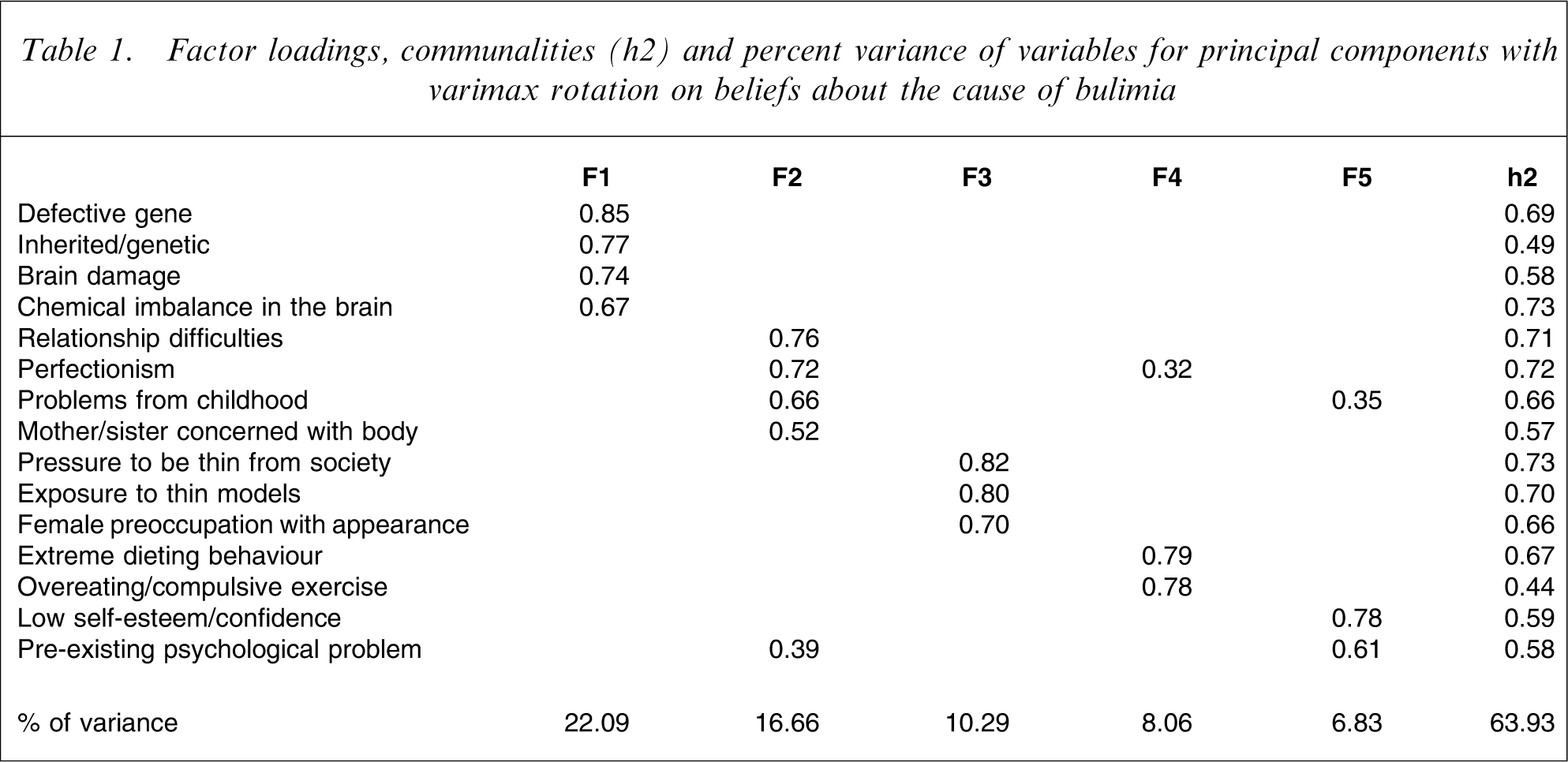
Fifteen items based on research and the pilot study were used to assess beliefs about causes of bulimia nervosa; for example, ‘I believe bulimia is caused by female preoccupation with their appearance’, rated from 1 (very unlikely) to 5 (very likely). A principal components analysis using a varimax rotation was conducted on the items to ascertain the major constructs. Most variables were well defined by this factor solution, with communality values high. The loadings on factors, communalities, and percentage variance are shown in Table 1. Scores for items with high loadings were averaged to obtain scales. Interpretive labels were suggested for each factor or cause; Biology, Relationship and Family Environment, Social Pressures to be Thin, Eating Behaviour and Low Self-Esteem.
Factor loadings, communalities (h2) and percent variance of variables for principal components with varimax rotation on beliefs about the cause of bulimia
Advantages and disadvantages of treatment
Responses obtained from the focus group were used to formulate six possible favourable outcomes and six possible unfavourable outcomes for the three treatments. The advantages included getting better quickly; feeling better about my body; more successful social relationships; reducing obsession with food; better able to enjoy life; and addressing underlying issues. Participants were asked to rate the likelihood of each outcome from 1 (strongly disagree) to 5 (strongly agree); for example, ‘If I were to see a therapist to treat bulimia, it would reduce my obsession with food’. In addition to each possible outcome being examined separately, scores on the items were summed and a mean score then derived to create a total advantage score for each treatment. Possible disadvantages included dependence; side effects; relapse after treatment; ability to manage the problem alone; trouble remembering to use the treatment; and difficulty in discussing personal issues. For example, ‘If I were to use a medication to treat bulimia, I would experience negative side effects’.
Personal experience with psychological therapies
Two items assessed previous exposure to treatment approaches for psychological problems. The questions, rated no (1) or yes (2), were ‘Have you ever used prescribed medication/seen a therapist/used self-change or lifestyle therapies to help manage a psychological problem of any kind (e.g. depression, anxiety)?’ and ‘As far as you know, has someone close to you ever used prescribed medication/seen a therapist/used self-change or lifestyle therapies to help manage a psychological problem of any kind (e.g. depression, anxiety)?’. Scores on the two items for each treatment approach were summed to provide an overall scale of past experience. If a participant answered ‘yes’ to either question, she then indicated the extent to which she considered the treatment experience as positive with 1 (disagree) to 5 (agree).
Eating disorder symptoms
The Eating Disorder Inventory Drive for Thinness and Bulimia subscales (EDI-DT, EDI-B) [23] were used to assess drive for thinness and bulimic symptoms. These subscales are reliable and valid in non-clinical samples when ratings are scored using untransformed responses [24].
Data analysis
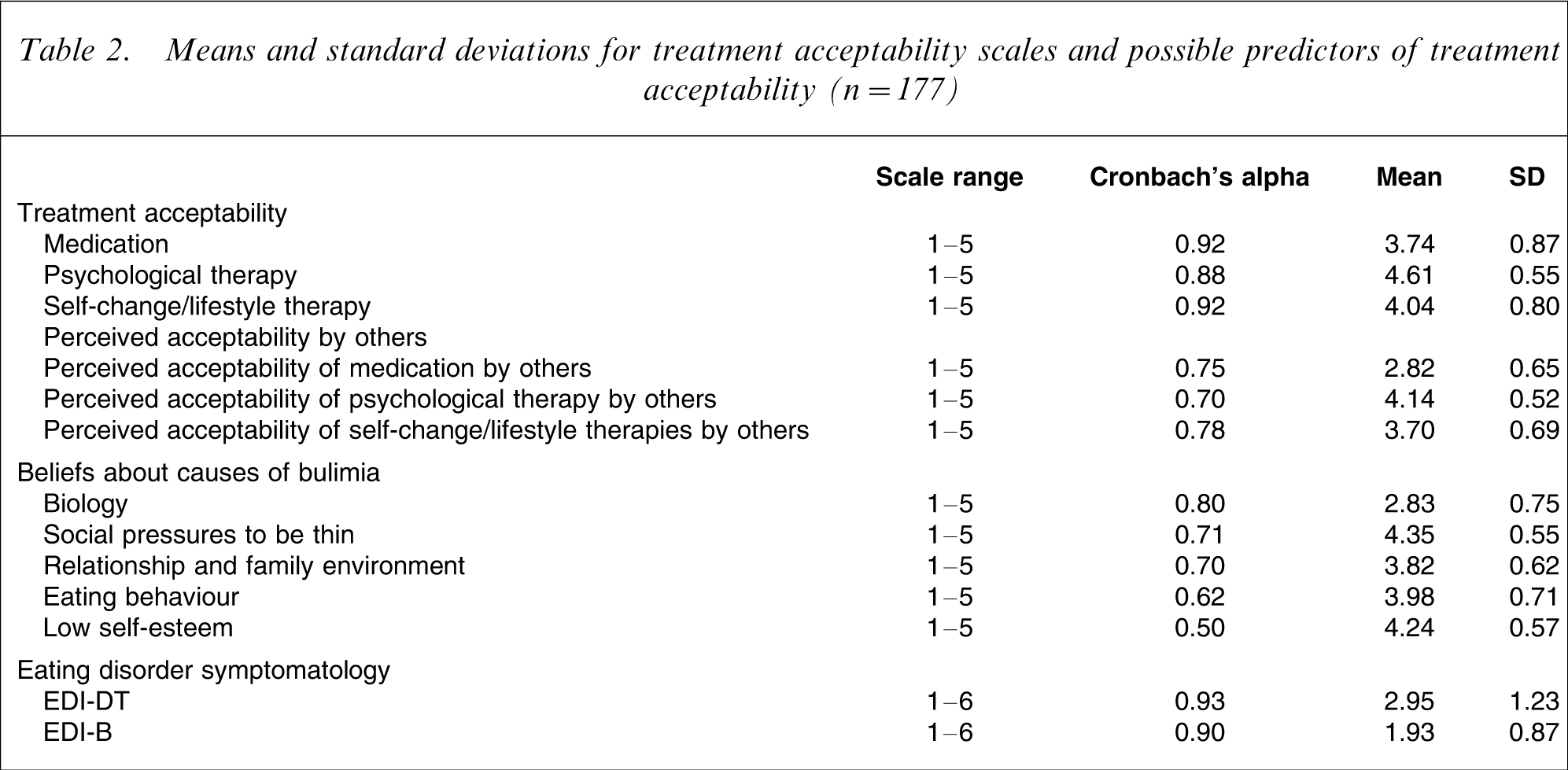
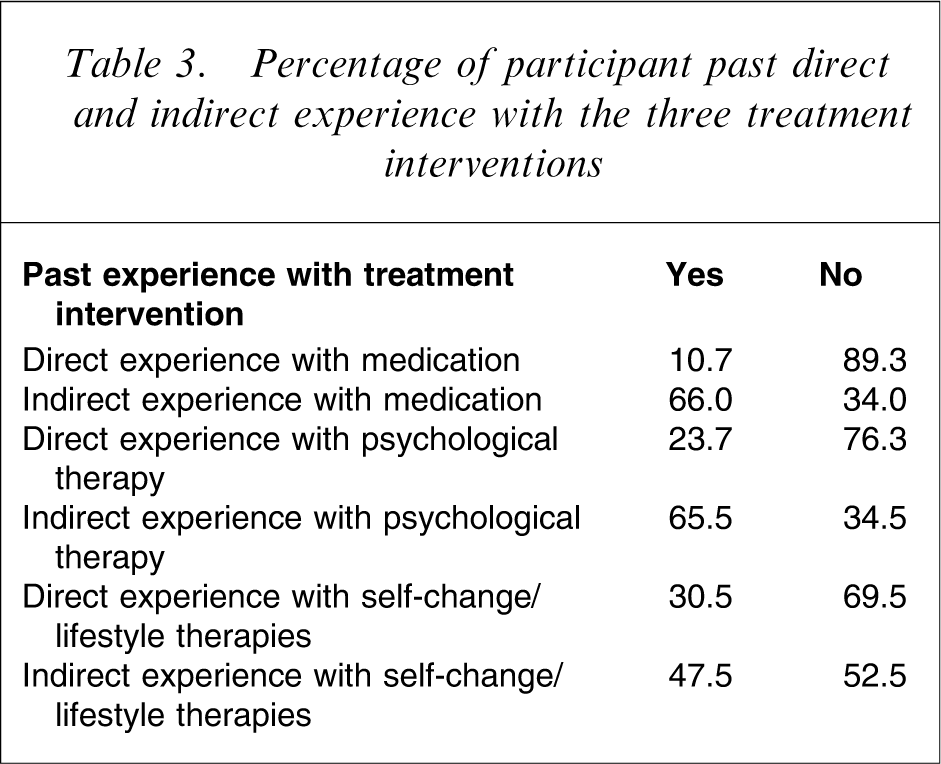
Mean scores and Cronbach's alphas for the scales assessing treatment acceptability for each treatment, perceived acceptability of others of each treatment, beliefs about the causes of bulimia and EDI subscales were derived (Table 2). Examination of distributions of responses on each scale indicated that all scales were within satisfactory ranges for skewness and kurtosis with the exception of EDI-B, on which a log transformation was performed prior to analysis. Percentages of participants who had and had not direct and indirect experience of treatment approaches were identified (Table 3). Mean scores for advantages and disadvantages of each treatment were identified (Table 4). Repeated measures analysis of variance (ANOVA) were used to test for differences in ratings for each advantage and disadvantage for each intervention approach. Planned comparisons were conducted to test specific hypotheses and alpha was set at p < 0.001 to take into account multiple comparisons. Correlation analyses were used to explore relationships between acceptability of treatments and the above-mentioned variables, and alpha was set at p < 0.01 to correct for multiple testing. Three separate multiple regressions were performed, using variables that were significantly correlated with each intervention, to determine which variables were making a significant unique contribution to treatment acceptability for each intervention.
Means and standard deviations for treatment acceptability scales and possible predictors of treatment acceptability (n = 177)
Percentage of participant past direct and indirect experience with the three treatment interventions
Means and standard deviations for advantages and disadvantages for each treatment intervention (n = 177)
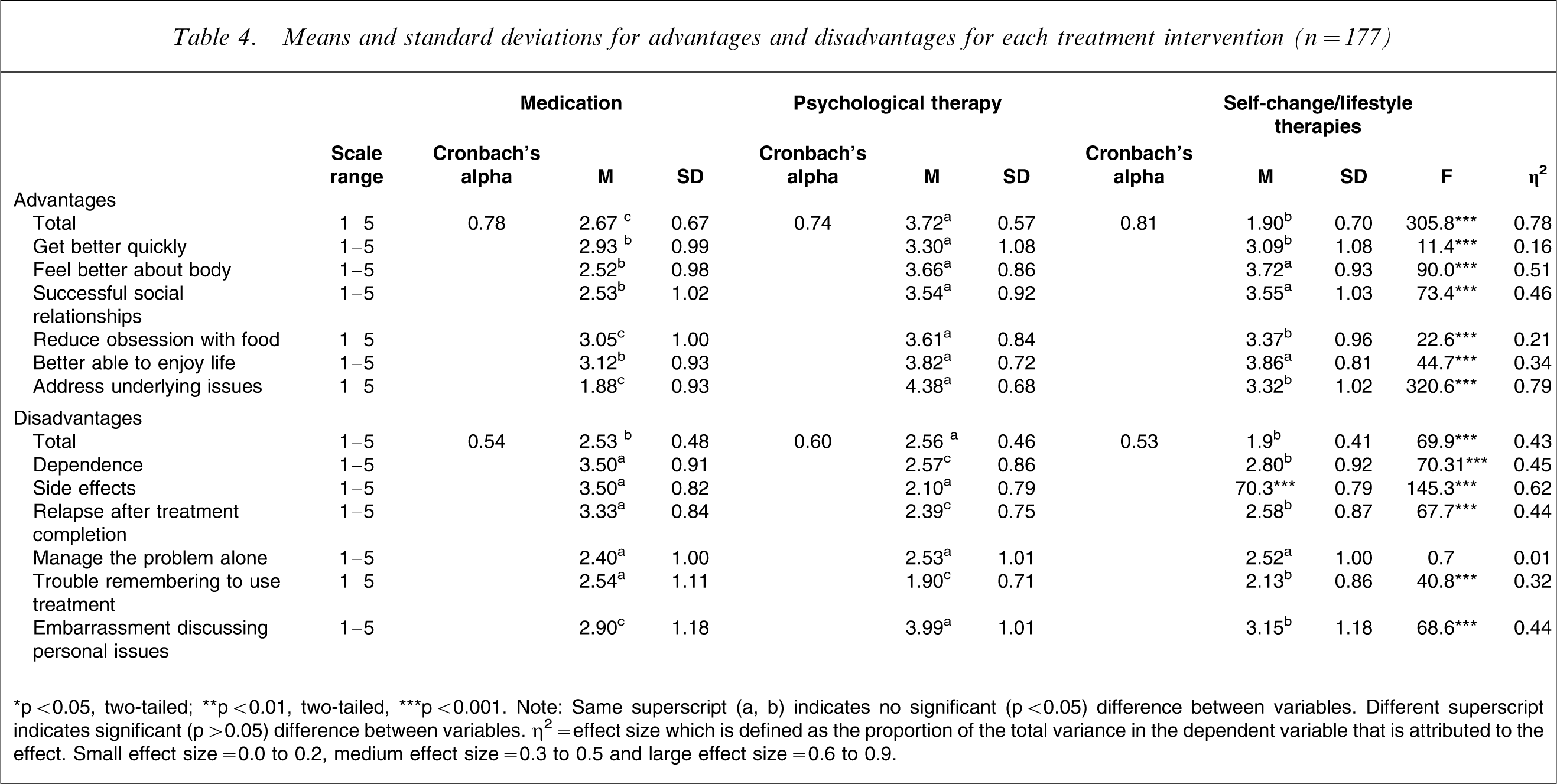
∗p < 0.05, two-tailed; ∗∗p < 0.01, two-tailed, ∗∗∗p < 0.001. Note: Same superscript (a, b) indicates no significant (p < 0.05) difference between variables. Different superscript indicates significant (p > 0.05) difference between variables. η2=effect size which is defined as the proportion of the total variance in the dependent variable that is attributed to the effect. Small effect size = 0.0 to 0.2, medium effect size = 0.3 to 0.5 and large effect size = 0.6 to 0.9.
Results
Participant characteristics
Of the 177 participants, 50.85% were of Australian origin with 26.2% of European descent, 6.4% Asian and 16.55% from a mixture of backgrounds. Of the sample, 22.0% were students, 48% were in professional occupations and 30% in non-professional occupations. The average number of years of education was 16.30 (SD = 2.52). The majority of participants were not married nor in a de facto relationship (66.1%). Participant characteristics of the sample in relation to treatment acceptability, perceived acceptability of treatment to others, beliefs about causes of bulimia nervosa, eating disorder symptomatology and past experience with treatment approaches, are summarized in Tables 2 and 3. As indicated in Table 5, there were no significant correlations between age and years of education and acceptability of the three treatments. There were weak but significant positive correlations between acceptability of psychological and self-change/lifestyle therapies and positive ratings of these interventions but not for medication. Past experience alone was not significantly correlated with treatment acceptability. The hypothesis that acceptability of treatment interventions would be associated with bulimic symptom severity was not supported.
Correlations between predictors of treatment acceptability for medication, psychological therapy and self-change/lifestyle therapies (n = 177)
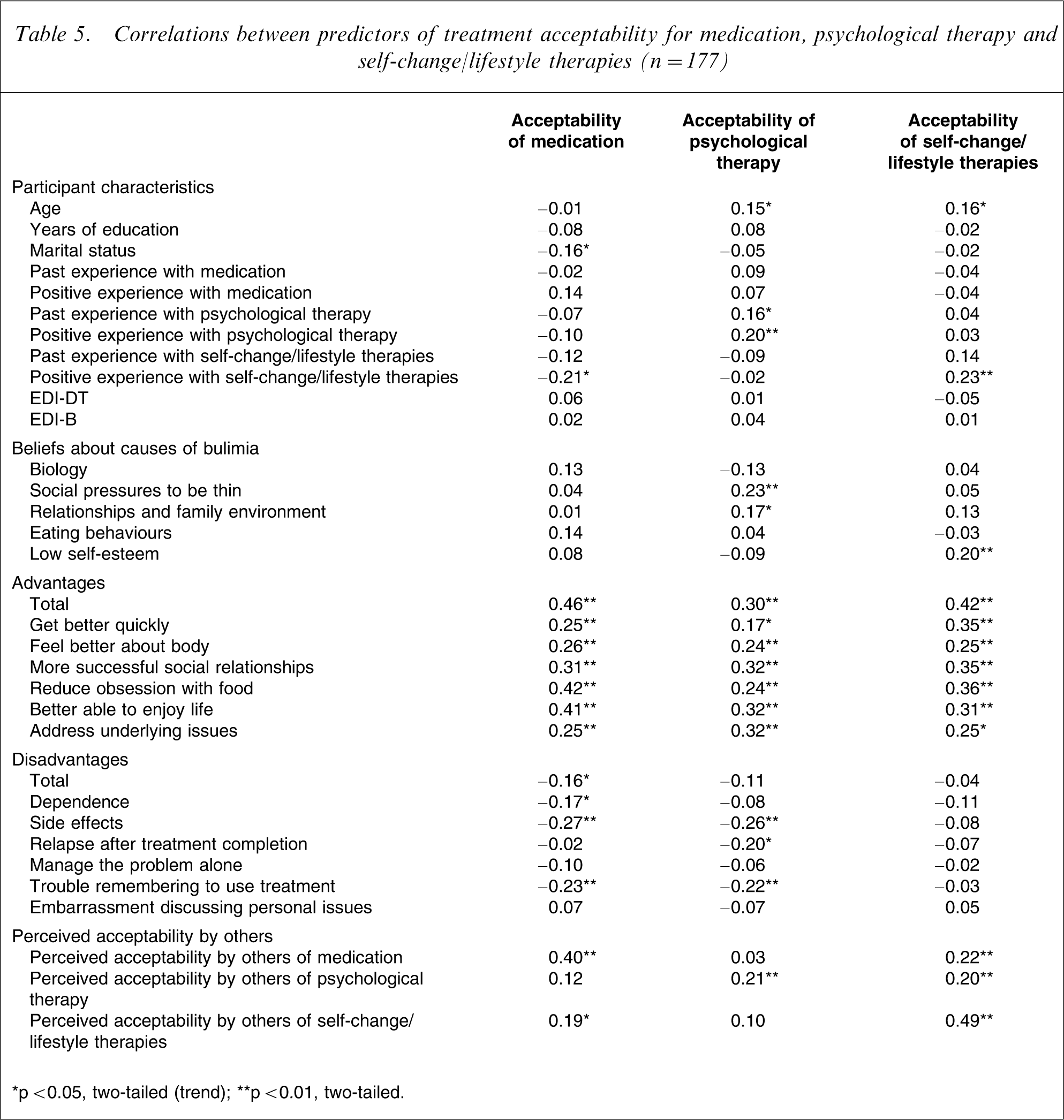
∗p < 0.05, two-tailed (trend); ∗∗p < 0.01, two-tailed.
Treatment acceptability to self and others
Planned comparisons indicated that psychological therapy was rated as significantly more acceptable than self-change/lifestyle therapies, F (1,176) = 70.05, p ≤ 0.0005, η2=0.29, and also significantly more acceptable than medication, F (1,176) = 168.43, p ≤ 0.0005, η2=0.49. Self-change/lifestyle therapies was rated as more acceptable than medication, although the effect size of the difference was small, F (1,176) = 11.76, p ≤ 0.001, η2=0.06.
Similarly, planned comparisons indicated that perceived acceptability by others of psychological therapy yielded higher ratings than perceived acceptability by others of self-change/lifestyle therapies, F (1,176) = 47.17, p ≤ 0.0005, η2=0.21, and medication, F (1,176) = 372.89, p ≤ 0.0005, η2=0.68. Perceived acceptability by others of self-change/lifestyle therapies yielded significantly higher ratings than perceived acceptability by others of medication, F (1,176) = 120.32, p ≤ 0.0005, η2=0.41. These findings were consistent with our first hypothesis.
Significant positive correlations were found between acceptability of all interventions and perceived acceptability by others of each specific treatment (Table 5). Acceptability of self-change/lifestyle therapies was also significantly correlated with perceived acceptability by others of medication and psychological therapy.
Beliefs about causes of bulimia nervosa
Planned comparisons comparing beliefs about causes of bulimia nervosa indicated that Social Pressures to be Thin received significantly higher endorsement than Low Self-Esteem, F (1,176) = 991.14, p ≤ 0.0005, η2=0.85. Low Self-Esteem received significantly higher scores than Eating Behaviour, F (1,176) = 19.12, p ≤ 0.0005, η2=0.10. Eating Behaviour received significantly higher scores than Relationship and Family Environment, F (1,176) = 1580.27, p ≤ 0.0005, η2=0.90, a strong effect size, and Relationship and Family Environment received significantly higher ratings than Biology, F (1,176) = 201.83, p ≤ 0.0005, η2=0.53. There were weak significant correlations between acceptability of psychological therapy and a belief that bulimia is caused by Social Pressures to be Thin, and acceptability of self-change/lifestyle therapies and Low Self-Esteem causes. Contrary to our hypothesis, no significant correlation was observed between acceptability of medication and beliefs about biological causes of bulimia (Table 5).
Advantages and disadvantages of treatments
Planned comparisons indicated that perceived advantages of psychological therapy did demonstrate significantly higher scores compared to perceived advantages of medication as predicted, F (1,176) = 576.51, p ≤ 0.0005, η2=0.77, but did not demonstrate significant higher scores compared to self-change/lifestyle therapies, contrary to our hypothesis, F (1,176) = 1.06, p ≥ 0.05, η2=0.01. Perceived advantages of self-change/lifestyle therapies did obtain higher scores than medication as predicted, F (1,176) = 471.60, p ≤ 0.0005, η2=0.73. Each planned comparison produced strong effect sizes.
Planned comparisons indicated that psychological therapy demonstrated significantly higher disadvantage scores compared to medication, F (1,176) = 69.26, p ≤ 0.0005, η2=0.28 and also self-change/lifestyle therapies as hypothesised, F (1,176) = 72.82, p ≤ 0.0005, η2=0.30. Perceived disadvantages of self-change/lifestyle therapies did not obtain higher scores than medication, F (1,176) = 0.39, p ≥ 0.05, η2=0.002.
Treatment acceptability of all three interventions was significantly positively correlated with perceived advantages of the treatment (Table 5), excluding a belief that psychological therapy helps people get better quickly and that self-change/lifestyle therapies addresses the underlying issues of bulimia. When considering associations with perceived disadvantages of treatment (Table 5), acceptability of medication was significantly inversely correlated with a concern about side effects of and trouble with remembering to use medication. Acceptability of psychological therapy was significantly inversely correlated with concerns about side effects and trouble remembering to engage in psychological therapy. Finally, treatment acceptability of self-change/lifestyle therapies was not significantly correlated with any of the possible disadvantages examined.
Predictors of treatment acceptability
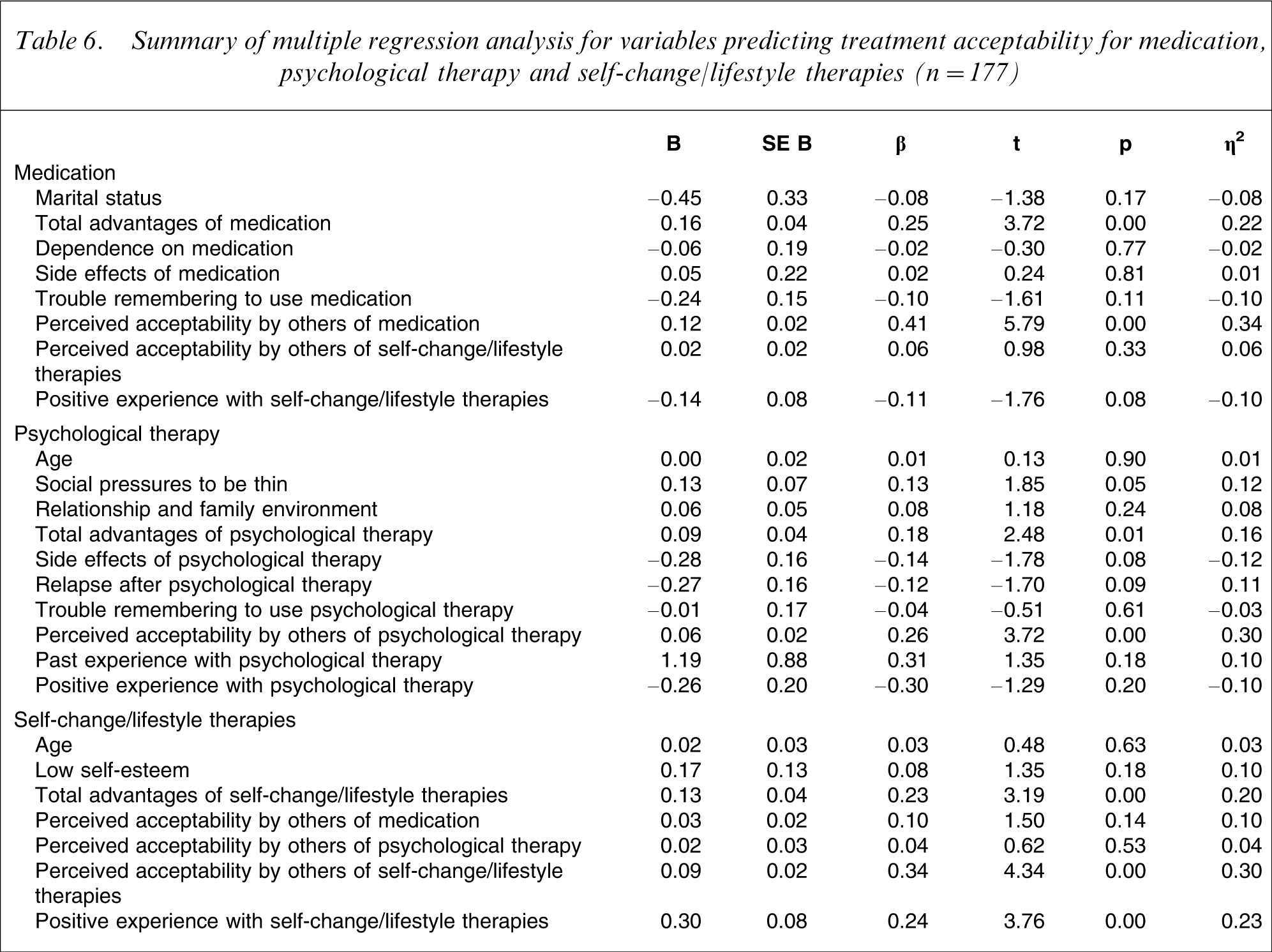
As seen in Table 6, the multiple regression analysis examining unique predictors of acceptability of medication indicated that the regression equation was significant (R2=0.41, F (8,176) = 14.66, p < 0.000). The unique predictors were perceived advantages of medication and perceived acceptability of medication to others. The multiple regression analysis examining unique predictors of acceptability of psychological therapy was significant (R2=0.25, F (9,176) = 6.19, p < 0.000). The unique predictors were Social Pressure to be Thin as a cause of bulimia nervosa, perceived advantages of psychological therapy and perceived acceptability by others of psychological therapy. The multiple regression analysis examining unique predictors of acceptability of self-change/lifestyle therapies was also significant (R2=0.37, F (6,176) = 16.85, p < 0.000). The unique predictors were perceived advantages of self-change/lifestyle therapies, perceived acceptability of others and positive past experience with self-change/lifestyle therapies.
Summary of multiple regression analysis for variables predicting treatment acceptability for medication, psychological therapy and self-change/lifestyle therapies (n = 177)
Discussion
Consistent with our first hypothesis, psychological therapy was rated the most acceptable treatment to participants as well as the most acceptable to others, and to have most advantages and fewer disadvantages, followed by self-change/lifestyle therapies and then medication. The hypothesis that treatment acceptability would be associated with perceived acceptability by others of the relevant treatment was also supported. Social Pressures to be Thin was the most strongly endorsed cause of bulimia, followed by Low Self-Esteem, Eating Behaviour, Relationship and Family Environment and, lastly, Biology. A number of correlates with acceptability of different treatment approaches were identified. Although no causal link can be assumed from this design, these relationships suggest specific beliefs about treatments that could be targeted to improve acceptability of efficacious treatments.
Despite the high acceptability of psychological therapy for bulimia, examination of the mean acceptability scores and effect size indicates that medication and self-change/lifestyle therapies were both rated as moderately acceptable interventions. Our findings suggest that public attitudes towards medication as a treatment for bulimia are more favourable compared to past research [25, 26]. However, assessments of specific advantages and disadvantages of medication show generally negative views. Given that medication can be efficacious [8, 9], it is clear that Mental Health Literacy is poor in this area for bulimia. However, the positive correlations between acceptability and perceived advantages of medication suggest that greater community awareness of the advantages of medication may improve its acceptability as a treatment (assuming this causal direction). Interestingly, despite personal beliefs, concern about the opinion of others about treatment may reduce motivation to adhere to a medication and other treatments. This suggests that one way to enhance the acceptability of evidence-based treatments for sufferers from bulimia nervosa is to enhance their acceptability to the community at large who may influence their opinions.
Assessments of advantages and disadvantages of psychological therapy do suggest a broad understanding about this treatment's goals (e.g. reduce obsession with food and improve body image). However, community women appear to have an unduly optimistic belief about the effectiveness of self-change/lifestyle therapies, possibly as it is not regarded as a very serious problem by many individuals [27, 28]. When considering attributions of causes of bulimia, self-change/lifestyle therapies, and not psychological therapy, were correlated with low self-esteem causes of bulimia. This was not expected. The emergence and growing popularity of lifestyle clinics, which offer a holistic approach in addressing health and well-being including self-esteem building, may help to explain these findings and the general acceptability of self-change/lifestyle interventions. This study highlights the need to improve community awareness of how different interventions address the causes of bulimia through different mechanisms.
Social Pressures to be Thin and Low Self-Esteem were perceived as the most probable causes as expected. However, correlations were only small, suggesting that other variables may help to explain treatment acceptability. Accuracy and depth of knowledge and understanding of eating disorders and treatments was not assessed in this study and it is possible that knowledge is another predictor of acceptability. Exposure to media messages and advertising of treatments through personal stories of celebrities and campaigns such as BeyondBlue may also highlight the value of treatments and reduce stigma and shame associated with accessing treatments [29].
Contrary to our hypothesis, the role of biological factors was generally rated as relatively unimportant. There is growing evidence that biological factors may contribute to vulnerability for and maintenance of bulimia nervosa [30]. This may need to be communicated to patients in order to enhance their understanding of the benefits of medication in treating bulimia.
Educational attainment was not associated with treatment acceptability and is not consistent with previous research [12, 18, 19]. Increasing awareness and knowledge of the benefits of medication in treating bulimia appears necessary even for those who are well educated. Furthermore, Jorm [11] identified that past treatment history enhances positive treatment attitudes. The current study suggests that positive perceptions of past treatment are more influential than past experience alone. Positive past treatment experiences may reduce fears associated with the intervention. Finally, an increase in symptom severity did not predict acceptability of the three interventions and is in contrast to previous research [11, 20]. Although it is valuable to identify community attitudes, future research is required to examine beliefs of symptomatic women who may respond differently.
Several limitations of this research restrict the conclusions that can be drawn. While endeavouring to sample a range of women, we did not have a representative sample. In Australia, 25% of women hold a bachelor degree equivalent to 16 years of education [31] and the average age of onset for bulimia is 19–20 years [5]. Therefore, participants in this study were relatively well educated compared to the general population and slightly older than the average age of onset for bulimia. Thus, the generalizability of the findings to the wider Australian or international community, or to women with bulimia nervosa, cannot be assumed. In addition, there were no previously established scales to assess beliefs about treatment acceptability for, and causes, of bulimia nervosa of which we were aware, and the validity of the measures we developed have yet to be confirmed.
Although psychological therapies are accepted and appear moderately well understood in the community, the possible benefits of medication and unlikely benefits of self-change/lifestyle approaches in the treatment of bulimia do not seem to be widely understood. This may help explain poor adherence to medication in particular, as patients may be recommended a treatment without accurately understanding why it may be valuable. Further research is required to extend our understanding of eating disorder Mental Health Literacy from community samples to highly symptomatic samples so we can understand its impact on treatment seeking and adherence.