
Abstract
Appearance concerns are increasingly common. Indeed, serial surveys in the US show that more and more people are dissatisfied with some aspect of their physical appearance, with a recent survey (1997) finding that 43% of men and 56% of women experience dissatisfaction with their overall appearance [1]. Concurrently, there is increasing demand for cosmetic specialists to perform procedures to enhance physical appearance. Thus, figures from the American Society for Aesthetic Plastic Surgery (ASAPS) show that cosmetic procedures in the US increased by 66% since 1998, and 119% since 1997 (see [2]).
Presumably, individuals who seek cosmetic enhancement for some aspect of their physical appearance are seeking to improve their self-esteem and self-confidence, and a good cosmetic outcome should improve these domains, as well as result in increased confidence in social situations. There is, however, scant literature on what underpins appearance concerns (hereafter referred to as ‘dysmorphic concern’ [3]) and leads people to seek cosmetic enhancement.
In some cases concern with physical appearance reaches an intensity where it causes subjective distress to the individual and leads to impairment of functioning in social and other domains; when this occurs, and when the perceived appearance flaw is actually nonexistent or slight, the individual has a psychiatric disorder known as body dysmorphic disorder (BDD) [4], [5]. While BDD is a recognized psychiatric disorder that responds to appropriate psychiatric treatment, many sufferers do not seek such treatment, as they either do not see their problem in psychological terms or are too embarrassed to discuss their concerns with anybody [6].
A high proportion of individuals with BDD tend to seek non-psychiatric medical or surgical treatment for the perceived appearance defect. In a study of 250 individuals with BDD, 76% had sought, and 66% had received, non-psychiatric treatment. Dermatologic treatment was most often received (by 45%), followed by cosmetic surgery (by 23%). In 83% of patients, the procedures led to no change in, or an exacerbation of, BDD symptoms [7]. In a UK study of 50 individuals with BDD, 48% had seen a cosmetic surgeon or dermatologist, and 26% had undergone one or more procedures; 76% were dissatisfied with the postoperative result [8].
Conversely, BDD appears relatively common in individuals seeking plastic surgery, with rates of 7–15% being reported [9], [10]. However, these studies have focused on people attending plastic surgeons, who perform surgical procedures and might thus be expected to attract more severely affected patients. The only study to our knowledge in a dermatological setting [11] also specifically determined rates of BDD per se (using a self-report measure), and found that 12% of patients screened positive for BDD. This study included a single community-based centre along with a dermatology cosmetic surgery clinic in a university department, raising questions about generalizability.
Thus, these studies did not determine rates of dysmorphic concern more broadly in those requesting interventions from cosmetic specialists. To the best of our knowledge, no previous studies have assessed dysmorphic concern in such patients. Also, studies have not directly assessed the impact that dysmorphic concern has on mood, social anxiety and other impairments commonly associated with BDD.
The aims of the current study therefore were to determine the prevalence and clinical correlates of dysmorphic concern in the broad sense, as well as the diagnosis of BDD in particular, in persons seeking cosmetic enhancement from cosmetic physicians. The study also explored clinical factors associated with the dysmorphic concern. We hypothesized that the presence of BDD and higher degrees of dysmorphic concern would be associated with more depressive symptoms and social anxiety and greater impairment in psychosocial functioning. This hypothesis was based on our clinical experience and previous research on BDD indicating high rates of depression, social anxiety, and functional impairment in patients with BDD [5], [6].
Materials and methods
Potential participants were all individuals over 18 years of age seeking cosmetic interventions at the practices of two cosmetic physicians (MM and KH) over a three-month period from September to November 2001. Written informed consent was obtained. We did not keep any data on those who refused to participate. The study was approved by the Research and Ethics Committee of Fremantle Hospital and Health Service.
Cosmetic physicians specialize in non-surgical cosmetic interventions. The practice of MM has a male: female ratio of approximately 60: 40; the range of interventions includes hair transplant, liposuction and a number of other cosmetic procedures. The practice of KH consists almost exclusively (99%) of women, and the range of procedures encompasses botulinum toxin injection, dermal filler treatments, facial vein treatment, radiosurgery, leg vein treatment, chemical peels, and microdermabrasion. Data from both sites were pooled for analysis.
All consenting subjects completed a confidential series of self-report questionnaires, including:
The Cosmetic Enhancement Questionnaire: Patient Version (available from author), covering demographics, prior experience of cosmetic procedures and extent of distress and impairment of daily living relating to the perceived cosmetic flaw (measured on 0–8 Likert scales, with 8 being most severe/most impaired).
The Work Home Leisure Scale [12], [13], a measure that assesses impairment in work and social domains; we asked specifically how these were impacted by cosmetic concerns. The questionnaire consists of four Likert scales (0–8) with a score of 8 being most impaired.
The Zung Depression Rating Scale [14], a 20-item questionnaire assessing mood symptoms over the prior week; higher scores indicate more severe depression.
The Social Interaction Anxiety Scale (SIAS) [15], a 20-item (each rated 0–4) questionnaire tapping concerns regarding being with other people in a social setting; higher scores indicate more severe social anxiety.
The Dysmorphic Concern Questionnaire (DCQ) [3], a 7-item questionnaire measuring extent of concern with physical appearance (each item rated 0–3, with 3 being most concerned). The items cover: concern with physical appearance; belief in being misshapen or malformed; belief in bodily malfunction (e.g. malodour); consultation with cosmetic specialists; having been told by others that you are normallooking, but not believing them; spending excessive time worrying about appearance; and spending a lot of time covering up ‘defects’ in appearance.
The DCQ is a dimensional measure of appearance concern, and has been used in a number of clinical settings [3], [16], [17]. DCQ scores correlate strongly with scores on the Body Dysmorphic Disorder Examination (BDDE), a reliable and valid measure of BDD [18]. However, the DCQ does not assess the BDD per se but instead assesses both ‘clinical’ and ‘subclinical’ appearance concerns without prejudice as to aetiology or nosology [16].
In addition, the cosmetic physicians (MM and KT) administered two separate interview questionnaires while remaining blind to subject responses on the self-report:
The Defect Severity Scale [9], a 0–8 Likert Scale (8 = most severe) rating the physicians’ judgements about the severity of perceived cosmetic defects. Inter-rater reliability (IRR) for a five-point version of this scale was previously established by three dermatologists and one psychiatrist who independently rated 50 kodachrome clinical slides of a variety of dermatological lesions (ICC = 0.88); and
The BDD Diagnostic Module [19], a reliable semistructured diagnostic instrument that establishes the presence of DSM-IV BDD. Both physician-rated instruments take approximately two minutes to complete.
Statistical analysis
Before investigating the impact of dysmorphic concern on patient functioning, each of the self-report scales (see above) was factoranalyzed separately to simplify and improve its internal reliability and construct validity. The Maximum Likelihood Method with Kaiser Normalization procedure was used [20]. Thus, the items that had the highest factor loadings on the first factor of each instrument was used as an indicator for the scale. Cronbach Alpha was calculated and used to determine the lower-bound estimate of the internal consistency of each indicator; values lower than 0.7 are considered unreliable [21]. All items were scored on an anchored 8-point rating scale (see above).
A standard multiple regression was used to examine the contribution of dysmorphic concern (via the Dysmorphic Concern Questionnaire) and attitudes toward the perceived cosmetic flaw (via the Cosmetic Enhancement Questionnaire) to impairment in work and leisure activity (via the Work Home Leisure Scale); mood (via the Zung Depression Rating Scale); and social anxiety (via the Social Interaction Anxiety Scale).
Results
Demographic characteristics and rate of BDD
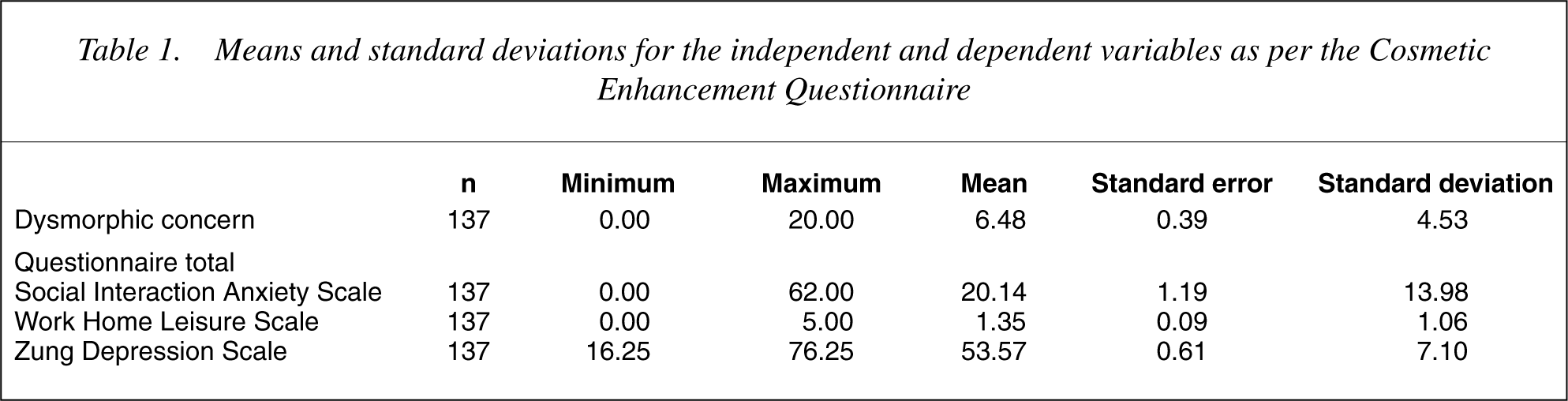
One hundred and forty-one subjects consented to participate. In four cases the questionnaires were not complete, and these were dropped from further analysis, leaving a total number of 137 subjects. The majority of respondents were female (female =119 86.9%; male = 18 13.1%), with no differences in age between the sexes (female = 40.61, SD = 10.38; male = 37.17, SD = 10.45; t = −1.309, df = 135, p = 0.193). Ratings on the various scales are shown in Table 1. There were no significant effects of sex on any of the ratings, but younger patients tended to experience more social anxiety (p = 0.02), and to have higher levels of dysmorphic concern (p < 0.001). Four patients (2.9% [95% CI = 0.8–7.3%]) were diagnosed with lifetime body dysmorphic disorder according to the BDD Diagnostic Module and the Defect Severity Scale.
Means and standard deviations for the independent and dependent variables as per the Cosmetic Enhancement Questionnaire
Factor analysis and regression modelling
Table 2 shows the items, factor loadings, and internal consistency of each of the rating scales. Both the Work Home Leisure Scale and the DCQ factored under one unidimensional construct. Factor structure of the Zung Depression Rating Scale was more complex, with only one factor (describing positive mood: see Table 2) having good internal reliability. The Cosmetic Enhancement Questionnaire divided into two discrete factors, namely: (1) a factor (‘Private Concern’) describing preoccupation and distress associated with the perceived appearance flaw; and (2) a ‘Public Concern’ factor, describing the individual's perception of how others view or judge the perceived appearance flaw. Both of these factors were employed in the regression modelling.
Factor analysis ofscale items using oblique rotation and their internal consistency as scales used in the regression models†
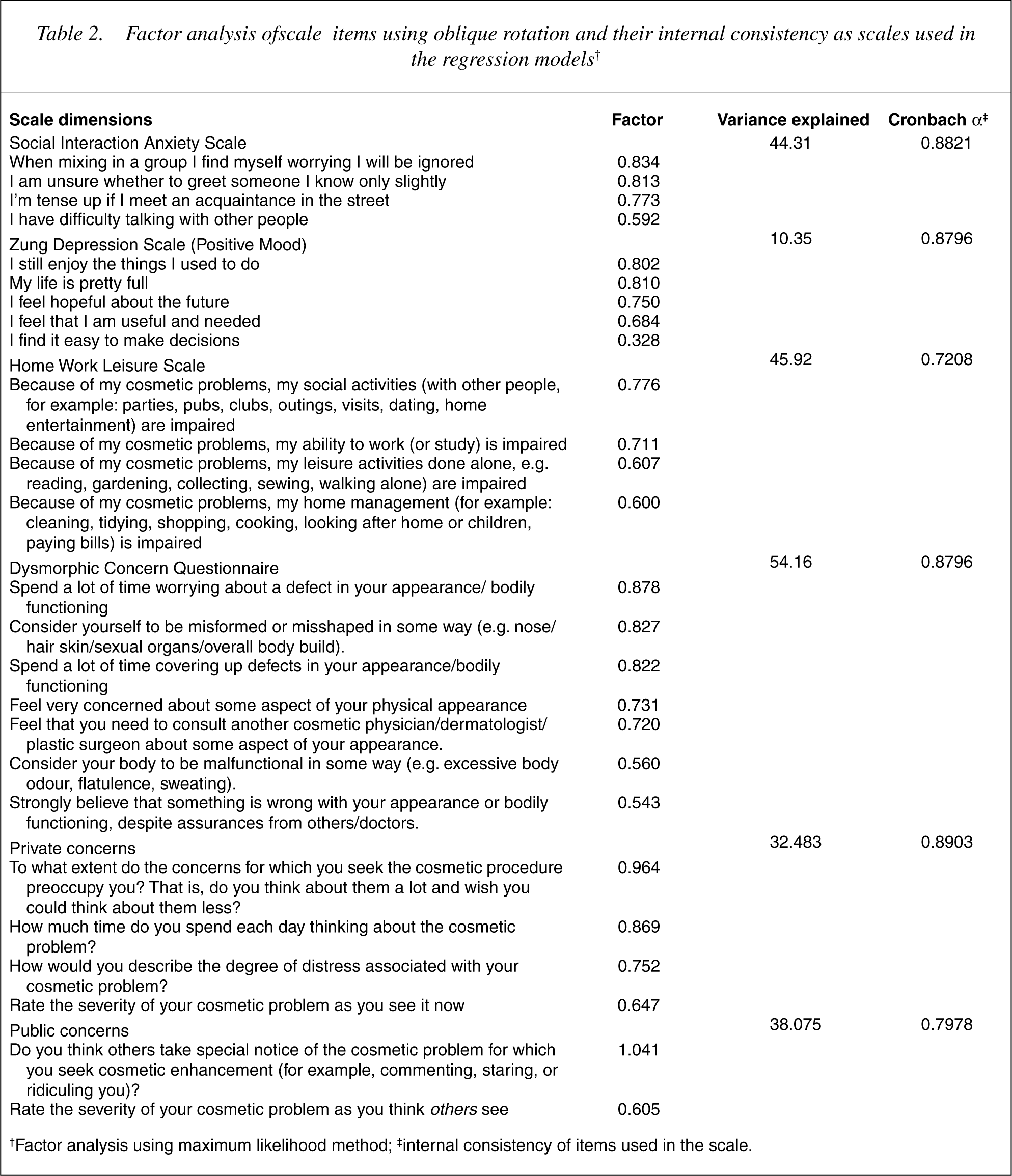
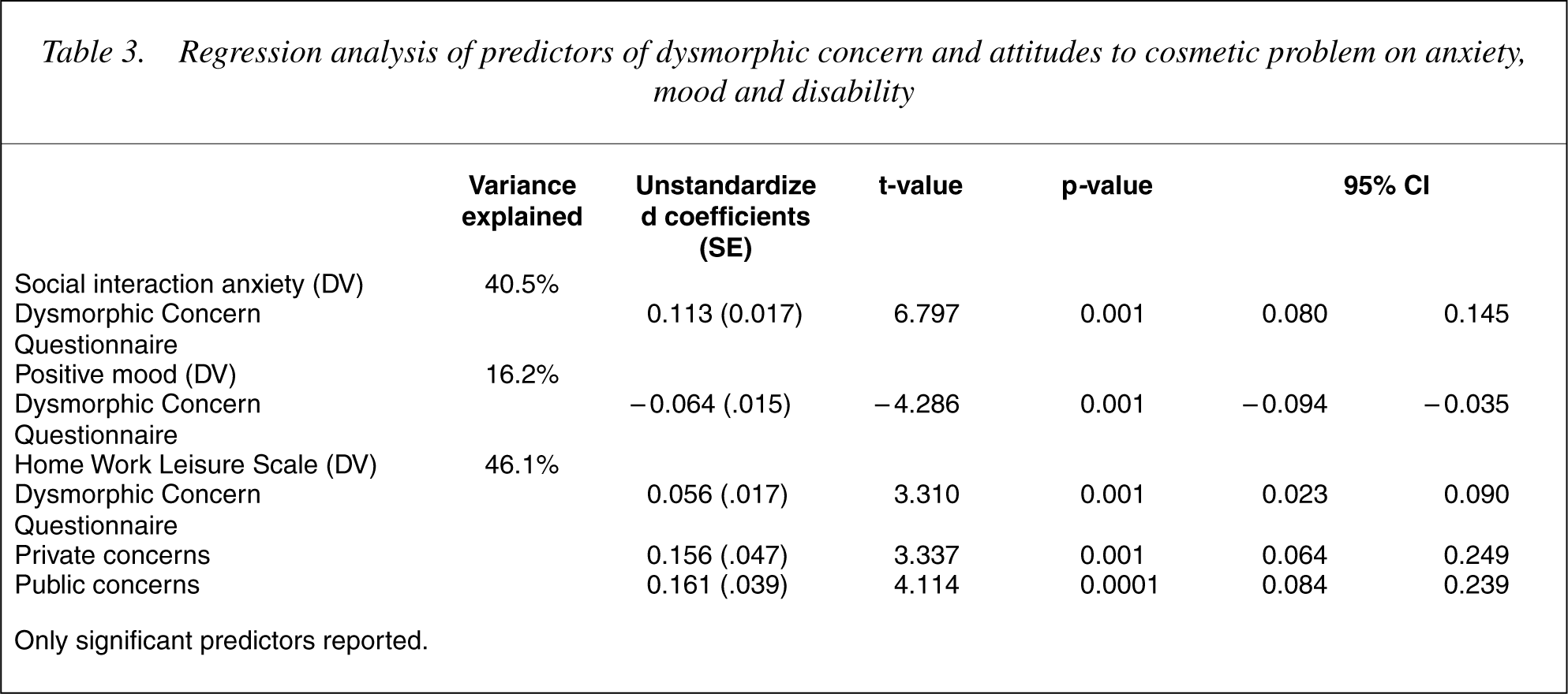
Table 3 shows the results of the regression modelling. Dysmorphic concern accounted for higher social anxiety, lower mood and greater impairment of work and social activities. In addition, both the ‘Private’ and ‘Public’ concern factors were associated with impairment in work and social activities.
Regression analysis of predictors of dysmorphic concern and attitudes to cosmetic problem on anxiety, mood and disability
Discussion
We report here on dysmorphic concern in people seeking cosmetic enhancement at the practices of two cosmetic physicians. Scores on the DCQ showed a mean of 6.48 (SD = 4.53). A previous study [17] used the DCQ to assess 84 patients attending a plastic surgeon for cosmetic procedures (n = 42) and found a mean DCQ score of 10.20 (SD = 4.63), suggesting that the current patient group was less concerned with appearance overall than that sample. In the current study, only four patients (2.9% [95% CI = 0.8–7.3%]) were diagnosed with BDD; the wide confidence intervals encompass reported rates of BDD in general population samples [22], but are lower than those found in studies in plastic surgery settings, where rates of 7–15% have been reported [9], [10], and in a dermatology setting, where 12% of patients screened positive for BDD [11]. The low number of BDD subjects in the current study precluded analyses pertaining to the diagnostic entity as such.
It is unclear why we found an apparently lower rate of BDD than have other studies of clinical populations, although there are several possible explanations. First, we could not control for any bias that might have been introduced from selection procedures. Second, the fact that we used clinician ratings of BDD rather than selfreport might have resulted in a lower estimation than in other studies. Third, previous study samples have differed in various ways (for example, gender distribution), which may have influenced the results; in particular, higher rates of BDD might be expected in a plastic surgery setting because BDD concerns often involve body areas and complaints that would require procedures (e.g. rhinoplasty) not offered by cosmetic physicians. The findings from the current study also reinforce the fact that dysmorphic concern is a much broader construct than the categorical diagnosis of BDD.
Regression analysis revealed that dysmorphic concern accounted for a substantial amount of the variance for mood, social anxiety and impairment in work and social functioning, while concerns related to how self or others perceive the putative flaw in appearance impacted significantly on work and leisure activities, but did not apparently influence mood and social anxiety to any significant degree. This latter finding is counterintuitive, but perhaps reflects different cognitive ‘coping styles’ in these individuals.
This study has a number of limitations. One is that we have targeted only people seeking non-surgical cosmetic interventions, and whether the results are generalizable to those seeking surgical interventions or to the general population, is not clear. In addition, only two treatment sites were included; studies of larger samples across different treatment settings are needed. Also, we could not control for response bias in our sampling procedure. Perhaps most important, we did not include a follow-up phase; this would have been of particular interest with respect to those subjects diagnosed with BDD. In light of preliminary findings from previous studies that individuals with BDD are generally dissatisfied with the outcome of non-psychiatric treatment (such as cosmetic surgery [23], [24]), prospective studies that assess outcomes of cosmetic treatments in this population are greatly needed. We are currently undertaking such a longitudinal study in subjects seeking cosmetic interventions from plastic surgeons.
Footnotes
Acknowledgements
We are grateful for funding from Allergen Australia. We thank Drs Lee Edstrom, Richard Zienowitz, and Lawrence Bowen from Rhode Island Hospital and Brown Medical School for input in developing the Cosmetic Enhancement Questionnaire.