
Abstract
Keywords
Dysmorphic concern, an overconcern with an imagined or slight defect in physical appearance [1], is the main diagnostic criteria of body dysmorphic disorder (BDD) [2]. Individuals with BDD report being preoccupied with an average of five to seven aspects of their appearance, predominantly focusing on the hair, nose, and skin [3]. Some concerns are specific (e.g., balding, large nose, acne, or skin tone), while others are vague or amount to no more than a general perception of ugliness. However, complaints of dissatisfaction with body shape and size that are a function of eating disorders are exclusionary criteria for BDD [2].
In contrast to normal appearance concerns, preoccupations in BDD are experienced as intrusive, and are difficult to resist and hard to control [4]. Moreover, the degree of conviction which the beliefs about appearance flaws are held can range from overvalued ideation to delusionality [5]. BDD patients may experience ideas or delusions of reference, believing that others take special notice of the defect, ridicule them, or evaluate them negatively based on their appearance [4]. Those patients who maintain their beliefs with delusional intensity qualify for an additional diagnosis of delusional disorder, somatic type [2].
Although not a diagnostic criterion, almost all patients with BDD perform compulsive behaviours. Checking the defect in mirrors and other reflective surfaces occurs in almost all BDD patients, while the remainder will periodically avoid mirrors to prevent the distress of seeing their own reflection and the time consumed when using mirrors [6]. Other common behaviours are comparing one's appearance with that of others, touching the body area of concern, excessive grooming, seeking reassurance about the perceived flaw or convincing others of its unattractiveness, camouflaging the perceived defect with cosmetics or clothing, and skin picking [3].
Comorbidity
Depression, social phobia, and obsessive-compulsive disorder (OCD) are often comorbid with BDD. In a study of 293 BDD patients, Gunstad and Phillips [7] reported the patients suffered from a mean of two comorbid disorders. The most common comorbid disorders were major depression, social phobia, OCD, and substance-use disorders. Comorbidity with personality disorders is also common, with up to 72% of patients diagnosed with one or more personality disorders [8]. Phillips and McElroy [9] reported that 57% of 148 BDD patients suffered from one or more personality disorder. The most common diagnoses were avoidant, dependent, obsessive-compulsive, and paranoid personality disorders.
Prevalence
Prevalence rates of BDD are similar among males and females, with reported prevalence rates of BDD in large community samples ranging from 0.7% [10] to 1.7% [11]. However, BDD is often underdiagnosed because individuals are often secretive about their symptoms and are reluctant to seek psychiatric treatment due to embarrassment or shame. Grant et al. [12] found that 13.1% of 122 psychiatric inpatients fulfilled the diagnostic criteria for the disorder. Notably, these patients stated that although BDD was their primary concern, they would not disclose their concerns to the clinician unless specifically asked. Zimmerman and Mattia [13] also noted that, in a large psychiatric outpatient sample (n = 500), clinicians failed to recognize the 16 (3.2%) individuals who fulfilled diagnostic criteria for BDD. Of these 16 individuals, 11 indicated that their BDD symptoms were one of the reasons they were seeking treatment.
Another factor contributing to the underdiagnosis of BDD is that BDD patients often pursue dermatological and cosmetic surgery for their perceived flaws. This trend is highlighted in reported prevalence rates of BDD ranging from 3.2% [14] to 53.6% [15] in cosmetic surgery settings and from 8.5% [14] to 15% [16] in dermatologic settings.
Dermatological, cosmetic, and other non-psychiatric procedures, however, do not appear to improve BDD symptoms. Phillips et al. [17] reported that although non-psychiatric treatment was sought by 76.4% and received by 66.0% of 289 BDD patients, these treatments rarely improved BDD symptoms. Crerand et al. [18] also reported that, of 200 BDD patients, non-psychiatric medical treatment was sought by 71% and received by 64%. The most frequent treatments sought were dermatological (50%) and surgical (32%) treatments. However, 91% of individuals receiving these treatments did not experience a change in their overall symptoms of BDD. Given the apparent ineffectiveness of cosmetic surgical and dermatological procedures in treating BDD symptoms, it is important to screen for BDD in these settings to refer the patient to more appropriate psychiatric treatments.
Screening measures for BDD
The 34-item Body Dysmorphic Disorder Examination (BDDE) [19] was developed as a semi-structured clinical interview to diagnose BDD and measure symptoms of body image disturbance. The BDDE was found to be a reliable and valid diagnostic measure for BDD. The main limitation of the BDDE as a screening measure for BDD is that it must be administered by a clinician and can take up to 30 minutes to complete. Although a self-report version of the BDDE has been developed [20], psychometric properties for this version have not been published.
In contrast, Phillips et al. [21] developed the Body Dysmorphic Disorder Questionnaire (BDDQ) as a brief self-report measure to screen for BDD. It comprises four items with a yes/no response format that reflect DSM-IV diagnostic criteria for BDD (e.g., are you very concerned about the appearance of some part(s) of your body that you consider especially unattractive?). The BDDQ has been shown to have a sensitivity of 100% and a specificity of 89–93% for the diagnosis of BDD in clinical samples [22]. Since the primary function of the BDDQ is to screen clinically for BDD, it does not provide a dimensional measure of BDD symptom severity.
Recognizing this limitation, Cash et al. [22] developed the Body Image Disturbance Questionnaire (BIDQ) from the BDDQ as a continuous measure of body image disturbance. The authors reported good psychometric properties within a sample of 295 college students, including excellent internal consistency and appropriate convergent validity with measures of body image, depression, social anxiety, and disordered eating. Incremental validity was also established when BIDQ scores predicted psychosocial functioning over body dissatisfaction. However, there is no published information about its convergent validity with interviewer administered measures, or its sensitivity and specificity regarding the clinical diagnosis of BDD.
The Dysmorphic Concern Questionnaire
Oosthuizen et al. [1] developed the 7-item Dysmorphic Concern Questionnaire (DCQ) to assess dysmorphic concern as a symptom without seeking to establish a diagnosis of BDD. The response format of the DCQ is similar to the General Health Questionnaire [23], with respondents rating their concern about their physical appearance relative to others on a 4-point scale. Administering the DCQ to an Australian sample of 65 psychiatric inpatients, the authors reported good psychometric properties. The results of this study indicated good internal consistency, a unidimensional factor structure, strong correlations with distress, and work and social impairment, moderate correlations with depressive symptoms, and an absence of statistically significant correlations with psychotic symptoms.
Jorgensen et al. [24] conducted a follow-up study with the aforementioned cohort to examine the construct validity of the DCQ. Nineteen (29%) of the patients received a diagnosis of BDD according to BDDE diagnostic criteria. The DCQ was found to have very good internal consistency and maximum likelihood factor analysis indicated a unidimensional factor structure. The BDDE was found to account for about half of the variance in the DCQ above measures of social anxiety, OCD, and depression. Further regression analyses indicated that the DCQ was the strongest predictor of BDDE scores, accounting for an additional 20% of the variance over that predicted by the measures of depression, OCD, and social anxiety. Group differences were also found, with patients diagnosed with BDD reporting significantly higher scores on the DCQ than those without BDD. The authors concluded that the DCQ was a reliable and valid measure sensitive to dysmorphic concern.
Although the DCQ was not developed to screen clinically for BDD, it may prove useful as a brief, self-report screening tool for BDD in non-psychiatric clinical settings. Stangier et al. [25] investigated the use of the DCQ as a screening measure for BDD among a sample of 65 dermatology outpatients. The patients were screened for BDD using the BDD Diagnostic Module [21] and for disfiguring dermatological conditions. As a result, the sample included 22 BDD patients, 22 patients with disfiguring dermatological conditions, and 21 patients with mild dermatological conditions. BDD patients reported significantly higher DCQ scores than both control groups. A DCQ cutoff value of 11 resulted in the correct classification of 100% of BDD patients, 100% of patients with mild conditions, and 59% of patients with disfiguring conditions. The authors contended that a DCQ cutoff score of 14 provided the best balance of sensitivity and specificity, with the correct classification of 72% of BDD patients and 90.7% of non-BDD patients. A limitation of this study, however, is that the sample included female outpatients drawn from a convenience dermatological sample.
The present study investigated the utility of the DCQ as a screening measure for BDD. The primary aim of this study was to assess the discriminative validity of the DCQ by examining differences among patients with a primary diagnosis of BDD and undergraduates screened for body image disturbances, after controlling for the severity of the two most common comorbid disorders, major depression and social anxiety. The secondary aim of this study was to derive cutoff scores for the DCQ to facilitate the screening procedure.
Method
Participants
BDD sample
Participants were 57 consecutive BDD outpatients comprising 26 males (45.6%) and 31 females (54.4%). Patients ranged in age from 18 to 54 years (mean = 29.60, SD = 9.44). Patients were all referrals to the St Vincent's Health Body Image Disorder Service in Melbourne, Australia, which is a state-wide outpatient service specializing in the evaluation and treatment of people with BDD. At intake, the study psychiatric (DJC) administered a diagnostic interview based on the Structured Clinical Interview for DSM-IV [26] to assess for BDD and comorbidity. All patients fulfilled DSM-IV diagnostic criteria for BDD, with 32 patients (56.1%) classified as delusional (delusional disorder, somatic type). Data from both delusional patients and non-delusional patients were analysed because they are considered variants of the same disorder, although there remains some debate about this dimensional classification [27]. Current comorbid disorders were social anxiety disorder (n = 29, 50.8%), major depressive disorder (n = 26, 45.6%), OCD (n = 10, 17.5%), anorexia nervosa (n = 6, 10.5%), impulse control disorder not otherwise specified (i.e., skin picking; n = 2, 3.5%), bulimia nervosa (n = 1, 1.8%) trichotillomania (n = 1, 1.8%), and generalized anxiety disorder (n = 1, 1.8%). Note that most patients had comorbidity with more than one disorder.
Non-clinical sample
Of a convenience sample of 280 undergraduate students in Melbourne, Australia, seven screened positive for BDD and 29 screened positive for an eating disorder (see below for screening procedure). Besides individuals who screened positive for BDD, those who screened positive for an eating disorder were excluded from further analyses. As a result, the final sample comprised 112 (45.9%) male and 132 (54.1%) female undergraduates. Participants aged in range from 18 to 43 years (mean = 20.80, SD = 3.10).
Measures
Dysmorphic Concern Questionnaire
The DCQ [1] is a seven-item self-report measure that assesses cognitive and behavioural symptoms of overconcern with an imagined or slight physical defect. Respondents rate their concern about their physical appearance relative to others on a 4-point scale, ranging from 0 (not at all) to 3 (much more than most people). The DCQ is scored by summing all items, with scores ranging from 0 to 21. Internal consistencies for the BDD (α = 0.73) and undergraduate (α = 0.85) samples were good.
Body Dysmorphic Disorder Questionnaire
The BDDQ [21] is a four-item self-report measure that screens for current clinical BDD. Item 1 establishes whether preoccupation is present (e.g., are you very concerned about the appearance of some part(s) of your body that you consider especially unattractive?). Item 2 determines whether the preoccupation is a function of an eating disorder (e.g., is your main concern with your appearance that you aren't thin enough or that you might become too fat?). Item 3 establishes whether the preoccupation causes distress and impairment (e.g., what effect has your preoccupation with your appearance had on your life?). Item 4 assesses the time spent thinking about the perceived defect (e.g., how much time do you spend thinking about your defect(s) per day on average?). Respondents are also asked to describe body areas of concern and give examples of functional impairment and avoidance. A respondent has probable BDD if they experience intrusive appearance concerns, causing significant distress or functional impairment and lasting over one hour per day.
Eating Attitudes Test-26
The Eating Attitudes Test-26 (EAT-26) [28] is a 26-item self-report measure that assesses symptoms and concerns characteristic of eating disorders. Respondents indicate the extent that each item is applicable to them (e.g., am terrified about being overweight). The score for each item ranges from 0 (never, rarely, or sometimes) to 3 (always). A respondent screens positive for an eating disorder if they obtain a score of 20 or more. Internal consistencies for the undergraduate sample were good (α = 0.76).
Social Interactional Anxiety Scale
The Social Interactional Anxiety Scale (SIAS) [29] is a 21-item scale that measures cognitive, behavioural, and affective aspects of social anxiety as experienced in social interactions in dyads or groups (e.g., I have difficulty talking with other people). Items are rated on a five-point scale, from 0 (not at all characteristic or true of me) to 4 (extremely characteristic or true of me). The SIAS is scored by summing the ratings and total scores range from 0 to 84. Higher scores represent higher levels of social interactional anxiety. Internal consistencies for the BDD (α = 0.92) and undergraduate (α = 0.91) samples were excellent.
Self-rating Depression Scale
The Self-rating Depression Scale (SDS) [30] is a 20-item self-report measure that assesses cognitive, behavioural, affective, and somatic symptoms of depression. Items are rated on a four-point scale, from 1 (a little of the time) to 4 (most of the time). The SDS is scored by summing all the items, with total raw scores ranging from 20 to 80. Higher scores represent severer depressive symptoms. Internal consistencies for the BDD (α = 0.78) and undergraduate (α = 0.70) samples were good.
Procedure
This study was approved by the University of Melbourne Human Research Ethics Committee and all participants provided informed consent. The undergraduates received course credit for their participation. Both BDD patients and the undergraduates were administered a self-report questionnaire pack comprising the DCQ, SIAS, and SDS, while the undergraduate sample also completed the EAT-26 and BDDQ. Undergraduates who screened positive for BDD on the BDDQ or for an eating disorder on the EAT-26 were excluded from further analyses.
Data analyses
Stata 10.1 was used to conduct univariate analyses on the data. Data were screened for the statistical assumptions of the planned analyses. Preliminary logistic and linear regression analyses were conducted to assess whether age and gender were potential confounders for the presence of BDD. A series of t-tests was conducted to compare the two groups on the study variables. An analysis of covariance (ANCOVA) was also used to control for the severity of social anxiety (SIAS scores) and depression (SDS scores) when examining differences in DCQ scores between the two groups. For all these statistical analyses, tests were two-tailed and a p-value of 0.05 was used to determine statistical significance.
A receiver operating characteristics (ROC) plot was used to assess the sensitivity and specificity of the DCQ in discriminating between BDD patients and non-clinical participants. Sensitivity is the proportion of true positives that is correctly identified by the test, while specificity is the proportion of true negatives that is correctly identified by the test [31]. That is, sensitivity refers to the proportion of correctly classified BDD patients and specificity refers to the proportion of correctly classified non-BDD patients by the DCQ. A ROC plot is obtained by calculating the sensitivity and specificity of every observed data values and plotting sensitivity against 1 – specificity. The area under the ROC curve is the most used measure of the accuracy of a diagnostic test and ranges between 0.5 and 1, with 0.5 indicating poor accuracy and 1 representing perfect accuracy [31]. Moreover, a ROC analysis is independent of disease prevalence [31]. The Youden Index (J), a function of sensitivity and specificity, was used to determine the DCQ cutoff score. The highest J value indicates the test score at which the greatest proportion of individuals is correctly identified as being patients and non-patients [31].
Results
Preliminary analyses
Regression analyses were used to assess whether age and gender were potential confounders for the presence of BDD. For these analyses, a liberal significance level (p = 0.20) was used. Vittinghof et al. [32] outline three steps in assessing potential confounding variables: (i) the potential confounder must be associated with the outcome variable; (ii) the potential confounder must be associated with the predictor variable of interest; and (iii) adjusting for the potential confounder must affect the magnitude of the coefficient estimate for the outcome variable.
Age predicted the diagnosis of BDD (Odds ratio [OR] = 1.33, 95% Confidence Interval [CI] = 1.22–1.44, z = 6.68, p < 0.001) and DCQ scores (r = 0.42, t = 7.96, p < 0.001). Adjusting for age in linear regression with the DCQ score as the dependent variable showed that the coefficient for the diagnosis of BDD did not change by more than 5%. Gender did not predict the diagnosis of BDD (OR = 1.02, 95% CI = 0.57–1.83, z = 0.06, p = 0.95) or DCQ scores (r = 0.04, t = 0.65, p = 0.51). Considering these results, neither age nor gender is likely to be confounding the relationship between the diagnosis of BDD and DCQ scores.
Group differences
Table 1 shows that BDD patients reported significantly higher DCQ, SIAS, and SDS scores relative to the undergraduates. The ANCOVA indicated that the covariates depression (F(1,272) = 22.62, p < 0.001, ηp 2 = 0.08) and social anxiety (F(1,272) = 12.83, p < 0.001, ηp 2 = .06) were significantly associated with DCQ scores. There was also a significant effect of group on DCQ scores after controlling for depression and social anxiety (F(1,272) = 268.45, p < 0.001, ηp 2 = 0.50).
Group descriptive and test statistics for symptom measures
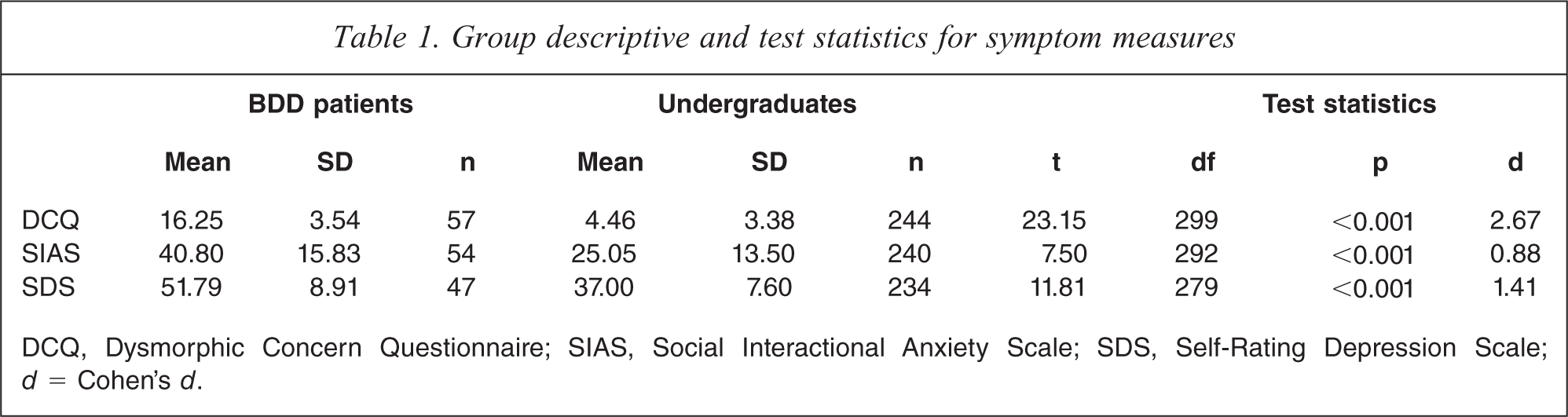
DCQ, Dysmorphic Concern Questionnaire; SIAS, Social Interactional Anxiety Scale; SDS, Self-Rating Depression Scale; d = Cohen's d.
ROC analyses
Figure 1 presents the ROC plot for BDD patients compared with the undergraduate controls. The area under the curve for this analysis was 0.980 (95% CI = 0.966–0.993). As seen in Table 2, a DCQ score of 9 produced the maximum Youden Index (J) and the best balance between sensitivity and specificity. This DCQ cutoff score produced 23 false positives and two false negatives.
Receiver operating curve analysis of the dysmorphic concern questionnaire
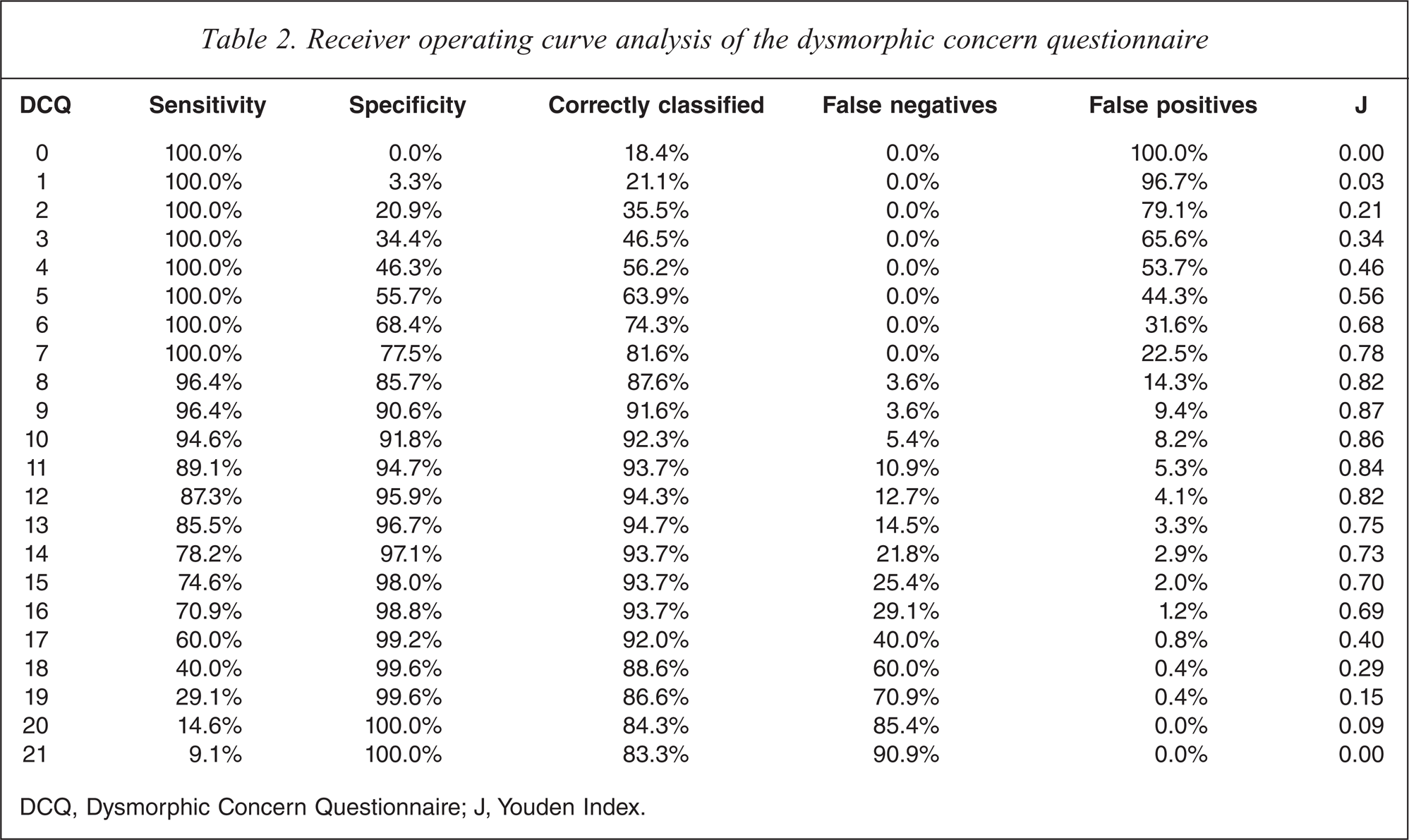
DCQ, Dysmorphic Concern Questionnaire; J, Youden Index.
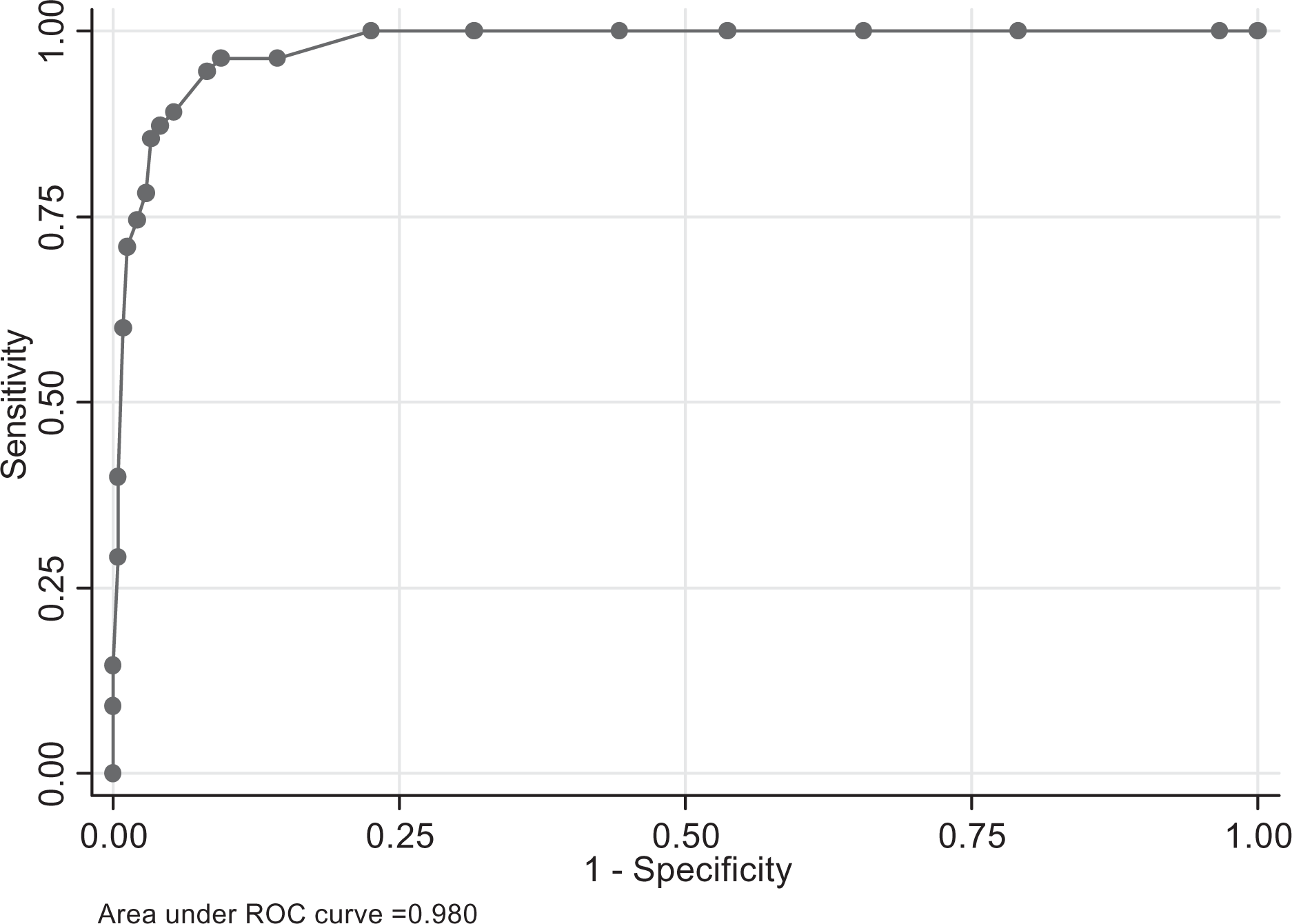
Receiver operating characteristic plot of Dysmorphic Concern Questionnaire scores of body dysmorphic disorder patients compared with undergraduates.
Discussion
This study examined the discriminative validity of the DCQ among patients with a primary diagnosis of BDD and undergraduates screened for body image disturbances. Overall, BDD patients reported greater dysmorphic concern, social anxiety, and depression relative to the undergraduates.
Evidence for the discriminant validity of the DCQ was established by the present finding that, compared to the undergraduates, the BDD patients reported significantly higher DCQ scores after controlling for the severity of social anxiety and depression. Comparable with previous research [24], this finding suggests that higher levels of dysmorphic concern among BDD patients may reflect cognitive, affective, and behavioural processes associated with a preoccupation with a perceived defect in physical appearance, rather than similar processes associated with social anxiety or depression.
A DCQ cutoff score of 9 was found to maximize the balance between sensitivity and specificity in the present study. This resulted in the correct classification of 91.6% of the combined BDD and undergraduate samples. Although Stangier et al. [25] recommended a DCQ cutoff score of 14, the present cutoff score of 9 has relatively improved sensitivity (96.4% versus 72%) and comparable specificity (90.6% versus 90.7%) when screening for BDD. This difference in cutoff scores may reflect sampling issues. While the present study used a sample of male and female patients with a primary diagnosis of BDD, the study of Stangier et al. used female outpatients drawn from a convenience dermatological sample.
Notably, a lower sensitivity will increase false negative rates, resulting in more patients with BDD being incorrectly classified as not suffering from BDD. Patients seeking cosmetic surgery procedures to enhance their appearance may be experiencing high levels of dysmorphic concern [33], some of whom may be suffering from BDD and remaining secretive about their symptoms. Therefore, the lower DCQ cutoff score of 9 will ensure that more individuals with clinically significant dysmorphic concern are identified when screening for BDD in dermatologic or cosmetic surgical settings.
The present findings must be interpreted within the context of several limitations. First, the use of undergraduates as the non-clinical control group limits the generalizability of the present findings. Second, the exclusion of undergraduates who screened positive for an eating disorder might have inflated the discriminant validity of the DCQ. Dysmorphic concern appears to be common among females with an eating disorder [34,35]. However, notable differences between dysmorphic concern in BDD and eating disorders have been documented, with the preoccupation focusing on the skin, hair, and facial region for BDD patients and on weight and body shape for eating disorder patients [20]. Research among individuals with a diagnosis of an eating disorder comorbid with BDD also indicates that the onset of BDD usually precedes the onset of eating disorder symptoms [36–38]. This suggests that dysmorphic concern associated with eating disorder symptoms may be secondary to that associated with BDD symptoms.
Additional research is required in which the DCQ is administered to BDD patients, eating disorder patients, and matched non-clinical controls to assess its discriminant validity. For these purposes, non-clinical controls could be screened for BDD through structured clinical assessments, rather than self-report measures. The use of non-clinical controls recruited from the general community would also improve the generalizability of findings associated with DCQ studies.
The above limitations notwithstanding, the present study is the first to use patients with a primary diagnosis of BDD and an undergraduate sample screened for body image disturbances to examine the discriminant validity of the DCQ and derive a cutoff score for BDD screening purposes. Results supported the use of the DCQ as a brief screening instrument for BDD. The DCQ may prove useful in cosmetic surgical and dermatological settings in which there is a high prevalence of BDD [18]. However, the use of only the DCQ as a diagnostic instrument for BDD in these settings is not recommended, as it does not produce a DSM-IV diagnosis. Nonetheless, when the DCQ is used in the initial assessment of cosmetic surgery or dermatology patients, a cutoff score of 9 would permit the identification of individuals who may benefit from further psychiatric assessment and treatment of their appearance concerns.
Footnotes
Acknowledgements