
Abstract
These guidelines focus on moderate to severe depression in adults treated by mental health professionals.
Specialist clinicians should consider, but not be limited to, the treatments recommended. The extensive literature includes systematic reviews of randomised controlled trials (RCTs). Where knowledge is sparse, lower orders of evidence have been used. Other guidelines are available for the treatment of depression in primary care settings [1], [2] and for children [3].
Treatment should be a partnership between patient, general practitioner (GP) and mental health professional. Engaging with the person is crucial for effective treatment. Even when depression is severe and complicated, specialist services are involved only during the acute phase, with the GP co-ordinating the longer-term treatment plan.
Definitions
While transient lowering of mood is common, persistence is qualitatively different. Clinical depression is common, serious and treatable. Untreated, it can result in disability and even death. It tends to be episodic and of varying severity. Many depressed people have concurrent physical and other mental health disorders.
Prevalence and severity
Depression is common. In the Australian Mental Health Survey, 4% of adults had a depressive disorder in the past month [4]. Compared with other mental illnesses, depressed people had higher levels of disability, including severe disability, and used health services more (70% had consulted a health practitioner in the previous month) [5]. Some 43% of those with depression suffer severe disability (< 30% on the Medical Outcomes Study short form 12) [personal communication Gavin Andrews, Wellington, 2001]. A similar pattern is likely in New Zealand.
Moderate to severe depression is as disabling as congestive heart failure [6], [7], and its relapsing nature accounts for one of the highest levels of disease burden of any condition [8].
Some 7% of people who consult a GP, and 40% of those concerned about their mental health, have clinical depression, often in conjunction with an anxiety or substance abuse disorder. Most experience disrupted lives [5]. Depression is common in secondary specialist services. A third of those presenting to psychiatric community clinics with depression are severely depressed and need extended treatment; the remainder need specialist advice to assist their primary healthcare professionals [4].
Depression (and substance abuse) is the most likely condition to be comorbid with other physical and psychiatric disorders, but is often unrecognized by primary healthcare workers [9] and secondary physicians [10].
Course and prognosis
Depression does occur in children but more often in teenagers. It affects boys and girls equally until age 15, after which it is more common in girls [11]. From ages 11–18 the rate increases from 0.5% to 3.4% for a major depressive episode and from 0.9% to 3.2% for dysthymic disorder [11], [12]. Most major depression begins in the late 20s [13].
Symptoms develop over days to weeks, though there may be anxiety, panic, fearfulness and lowered mood over preceding months. Sudden onset is usually associated with major stress. Untreated moderate episodes last up to 9 months. A third of those with moderate depression recover with placebo treatments, while half respond to 6–8 weeks of active treatment [14]. An episode may be the harbinger of bipolar disorder or an exacerbation of dysthymic disorder.
The likelihood of recovery in the next month decreases after 6 months, from 15% for months 7–9 to 1–2% up to 5 years [15], [16], at which time 12% have not recovered [16].
Remission is partial for 20–30% of people with depression, who experience continuing symptoms and social and occupational impairment [15].
Recurrence
Emphasis on good prognosis for major depression in primary care is appropriate. But as depression recurs in 40% of people within a year [17], monitoring and intervention are necessary to prevent relapse. A 12-years follow-up of people treated for an index episode, found depressive symptoms present for 60% of this period and a full depressive episode for 15% [18]. People with three or more episodes have an 80% chance of recurrence over the next 3 years [19].
Long-term studies show even higher rates of recurrence. A 25-years follow-up of Australians hospitalized with depression found only 1 in 8 remained depressionfree, with an average of three episodes. However, a quarter improved in the last decade of follow-up, including 80% of those chronically depressed over the first 15 years [20]. Those with psychotic depression have worse outcomes [17].
Complications
If untreated, depression increases risk of suicide and other violent acts. Some 6% of people diagnosed at some time during their lives with major depression will suicide [21], as will 10–15% of those ever admitted to hospital – a rate 30 times that of the general population [17], [22], [23]. Of those with a current major depression 25–50% will attempt suicide [24]. Treatment halves the risk of suicide, especially for men under 30 [25–28]. However, unemployment, isolation, impulsivity and misuse of alcohol and drugs increase risk [29], [30].
Depression, especially when recurrent or chronic, distresses family and friends [31]. It may affect a person's capacity as a parent, and is often associated with occupational dysfunction [32].
Aetiology and risk factors
Many factors protect against, predispose to, or precipitate depression: genes, childhood experience, previous trauma, social and cultural supports, physical factors (including drugs) and stress [33–38]. Depression occurs more commonly in the young [39], [40] and in women, at least in Western society [5], [39], [41], [42], and the latter is not attributable to postnatal depression alone.
Depression affects 5–10% of those with medical illness attending primary care and 6–14% of medical and surgical inpatients [43]. Rates of 50% are associated with some conditions, for example HIV-AIDS [18], [44], in which prevalence correlates with severity [18], progression [45], older age [46] and less social support [47]. It is commonly associated with Parkinson's disease [48], migraine and chronic pain [49]. Varying rates for specific conditions reflect differences in socio-demographics, severity and chronicity. Increased rates may be a direct effect of physical illness (e.g. hypothyroidism, Cushing's disease and certain cerebral tumours), a side-effect of treatment (e.g. steroids and some antihypertensives) or a reaction to illness.
Method
Key features in developing these clinical practice guidelines are: (i) a review of literature; (ii) metaanalyses of RCTs; (iii) evidence tables; (iv) drafting by a group with clinical, research and consumer expertise; (v) consultation with patients, cultural consultants and professionals with specific knowledge in sparsely researched areas; and (vi) redrafting after wider consultation.
Searches of MEDLINE and PsycLIT (1996–July 2002) using ‘depression’, ‘major depression’, ‘major depressive disorder’, ‘RCT’, ‘meta-analysis’ and ‘review’, were supplemented by a manual search. Studies prior to 1996 were identified from the major meta-analysis of the Agency for Health Care Policy Research [14], more recent meta-analyses, and references identified in the search. Key texts, review articles and existing guidelines were examined.
Randomized controlled trials were included in the meta-analysis if medication was prescribed in adequate doses for adequate periods, and if information was available to calculate an intention-to-treat outcome for a greater than 50% reduction in severity score (e.g. Hamilton Rating Scale for Depression, HAM-D). The minimum HAM-D score [50] was 12 for mild depression, ≥ 17 for moderate and ≥ 24 for severe. ‘Numbers needed to treat’ (NNT) and ‘absolute risk reduction’ (ARR) were calculated and summarized using metaanalyses. Confidence intervals for NNTs were calculated iteratively using STATSDIRECT [51].
The working party's cultural advisor consulted at every stage with Maori and the Victorian Transcultural Psychiatry Unit in Melbourne. The Section of Psychotherapy, RANZCP identified publications on dynamic psychotherapy.
These guidelines are for clinicians in specialist mental health services. They mainly focus on people who do not recover from a first episode or have a partial remission, and look to the long-term management of the 45% at risk of recurrence. A third of those with depression have a single episode only, and can be adequately treated in primary care settings, with occasional specialist support. However, specialist practice must acknowledge the need for longer-term follow-up and relapse prevention.
Assessment
Assessment includes the type, severity and duration of the depression and any coexisting psychiatric or physical disorders. It establishes both contributing stresses and the individual's supports, resources and coping style. Crucially, it considers the risk of suicide or risk to others, either through an act of violence or through neglect (e.g. in postpartum depression).
Heightened clinical suspicion is essential to effective diagnosis. ‘Atypical’ presentations are common: teenagers are not always morose, nor are the elderly always sad. Sadness is neither a necessary nor a sufficient criterion. Symptoms are often vague, and physical complaints may be prominent. Women, especially postpartum, and people under 40 are the most susceptible. In atypical depression the neurovegetative symptoms are the reverse of those usually encountered.
Dysthymia must be distinguished from residual symptoms of major depression, with diagnosis following at least 6 months after full remission of a major depressive episode. If dysthymia precedes major depression (socalled ‘double depression’), poor outcome is more likely.
Treatment decisions will reflect the key psychological, social and cultural issues contributing to the illness, as well as its subtype, severity and duration.
Severity and depression subtypes
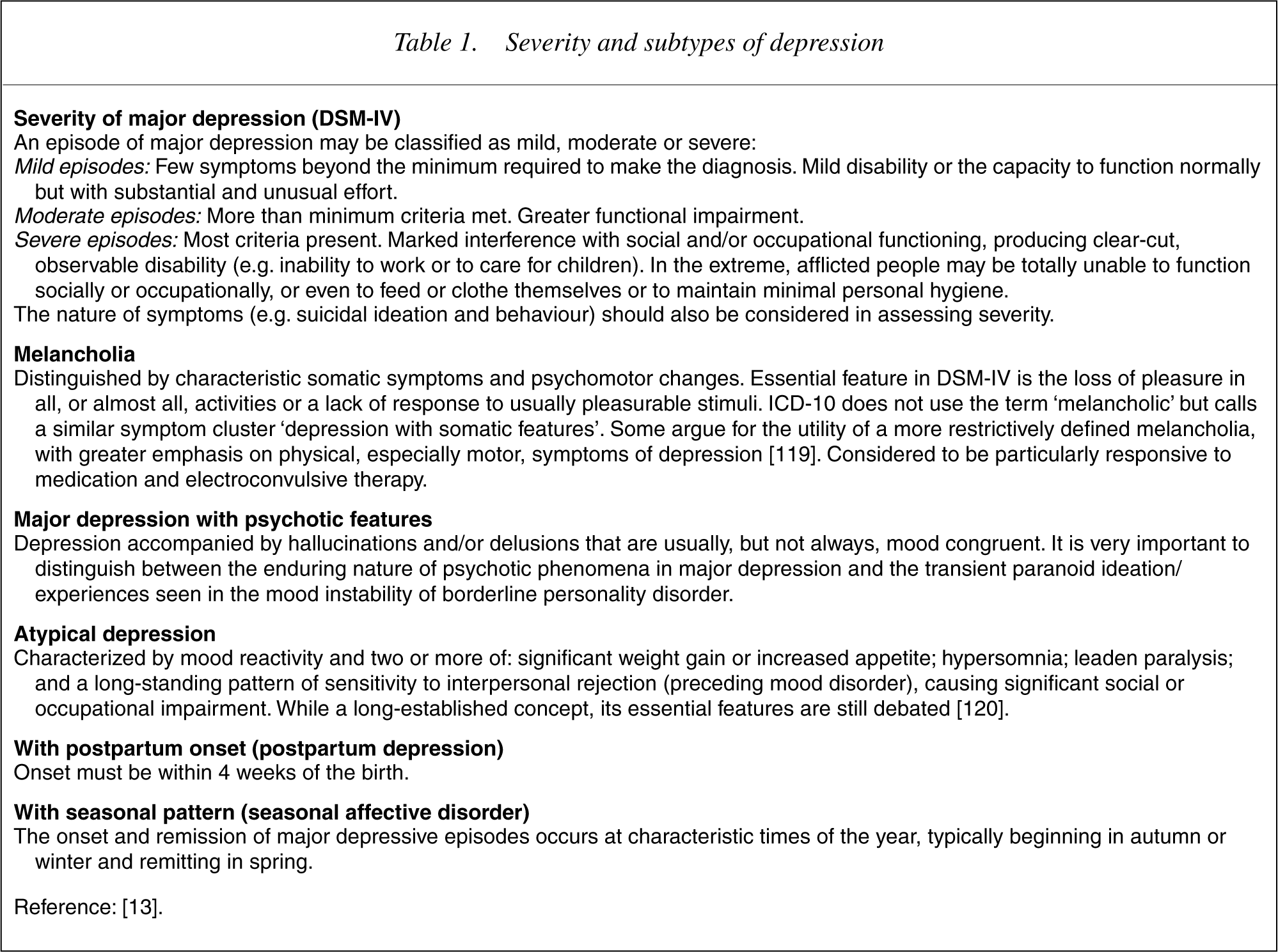
Both severity and subtype are important in selecting treatment (Table 1) [13]. Each category needs differential diagnosis and specific treatment. For most, the risk of recurrence is higher than for uncomplicated depression and continuing treatment is indicated.
Severity and subtypes of depression
Formal assessment of severity (e.g. using the HAM-D [50], the Center for Epidemiological Studies Depression Scale [CES-D] [52], or similar) allows selection of evidence-based treatments and provides a baseline to monitor effectiveness.
Suicide risk
Risk assessment, to self and others, is a key task at first examination and throughout treatment. Risk to others may arise through paranoid ideation as part of psychotic depression. Risk through neglect is of concern during postpartum depression, for the infant or older siblings. Risk may increase during recovery from a retarded depression (e.g. during early response to ECT), when intense suicidal ideation persists after recovery of motor activity, allowing the person to act on their ruminations. Evidence that suicide attempts are more common in the early morning (when ward staffing levels are lowest) is not consistent and differs between age groups [53–55].
Management strategies vary with the degree of risk to self or others. As change can be rapid, review of risk and appropriate support is necessary.
Suicide risk assessment is covered in the RANZCP clinical practice guideline on deliberate self-harm (in press) <http://www.ranzcp.org>.
Investigations and concurrent disorders
Since concurrent physical or other psychiatric illnesses are common, investigations are considered at initial assessment, particularly if presentation is atypical or precipitating factors absent, and are reconsidered if response is poor.
Current treatment evidence
Beneficial interventions
Good outcomes require sound alliance between professional and patient, adequate duration of treatment, and co-ordination of treatment (Fig. 1).
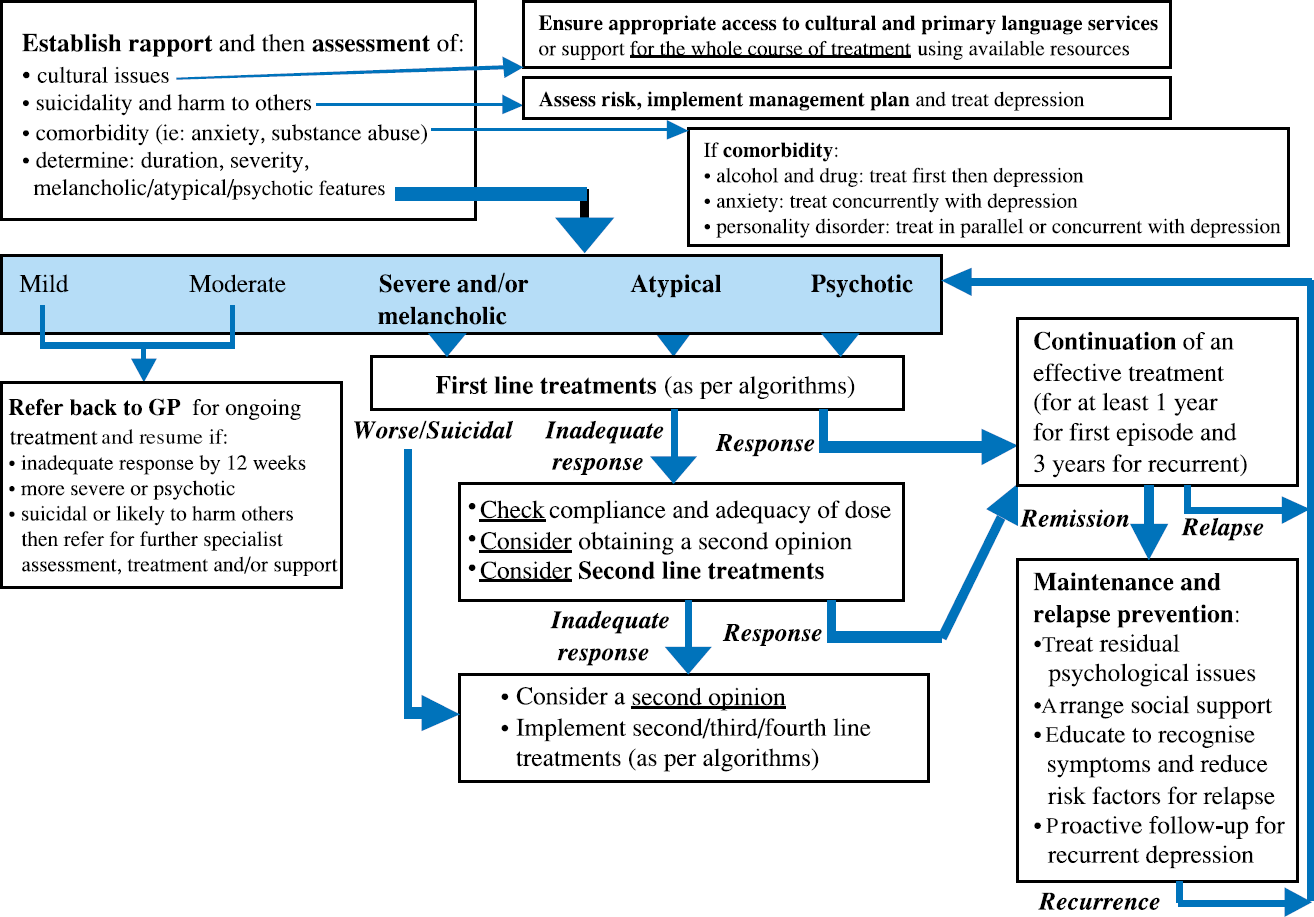
Outline of treatment for depression.
An evidence-based treatment is selected in discussion with the patient, and an effective dose (or number of therapy sessions) is monitored by measuring severity of symptoms. Antidepressants are most effective for the most severe depression [56]. If initial response is poor, continue treatment or consider switching to a second or third-line option [57] (Fig. 1). All antidepressants, and to a lesser extent the psychological treatments, have a high relapse rate following early discontinuation.
Relevant psychological, social and cultural issues are explicitly considered and befriending programs may assist outcome [58], [59].
Behavioural measures are preferable to additional medication for relieving some symptoms. For insomnia, sleep hygiene may help (caffeine restriction/avoidance, alcohol avoidance, adequate exercise, avoiding late meals, etc.).
Mild depression
No treatment is more effective than supportive clinical care with psycho-education, supplemented by teaching problem-solving skills [60], [61] or by supportive counselling [62], [63].
Moderate depression
Almost all antidepressants, CBT and IPT are equally effective (and of similar absolute cost in the medium term, although direct costs to patients vary). Of greatest benefit is the therapeutic relationship, which enables agreement on treatment selection and continuation. Regular monitoring for side-effects and encouragement to persist (or change treatment) are helpful.
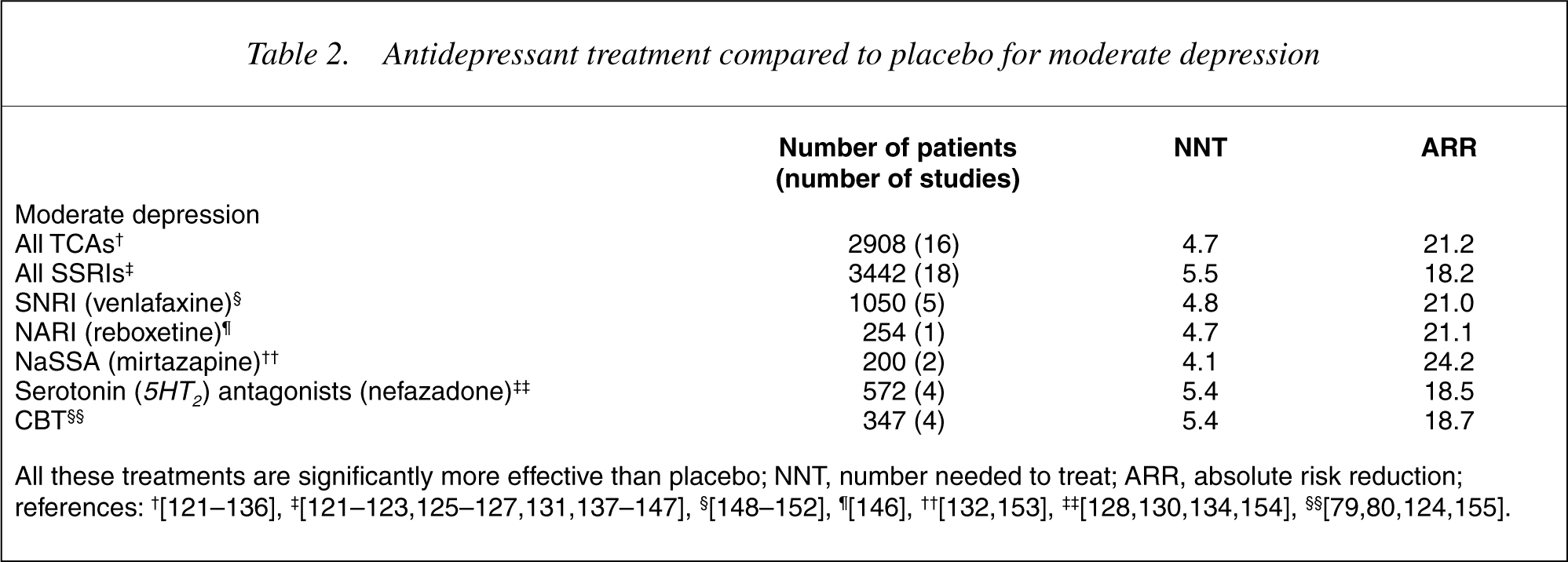
Table 2 compares antidepressants with placebo, and Table 3 with other antidepressants. All antidepressants and CBT are superior to placebo (standard clinical treatment without a specific active pharmacological agent), with NNTs of 4.1–5.5 (20% reduction of average absolute risk over placebo).
Antidepressant treatment compared to placebo for moderate depression
Comparisons between active treatments for severe and moderate depression

The findings in Table 3 are both more relevant and more robust, due to more and bigger studies. The much larger NNTs reflect the similarity in effectiveness of most antidepressants, though venlafaxine has a small advantage over SSRIs. (A large NNT indicates that many people would be treated before one extra person responded favourably to the slightly more effective treatment.) Selection requires a balancing of benefits and risks, including side-effects and toxicity. The relative merits of older and newer medications remain controversial and require study.
Both tables show the effectiveness of CBT and IPT. Whereas research requires structured treatment, often using a treatment manual, in practice the approach is more eclectic and reflects the therapist's expertise.
There is as yet no evidence that dynamic psychotherapy is effective. However, depression is often associated with trauma and personality difficulties, which are commonly treated by psychodynamic therapy. Furthermore, the literature emphasizes the shared features of effective therapy (therapeutic alliance, motivation, hopeful expectancy and ability to work with the therapeutic framework) and the limited benefits of one model over another.
Severe depression without psychosis
Initial treatment uses an antidepressant in the context of a therapeutic relationship. Psychological therapy for residual symptoms or risk of relapse may be appropriate later.
There are four satisfactory placebo-controlled trials. While the NNT compares to that in moderate depression, it does not reach statistical significance. None of the comparative studies of ‘newer’ and ‘older’ antidepressants (Table 3) is statistically significant.
Severe and complicated depression
Trials are rare. Accurate diagnosis, consultation with colleagues, adequate dose, support and monitoring all contribute to response, and maintenance is critical.
Unsatisfactory response to initial treatment
The first step is to reconsider the diagnosis, determine whether the patient has followed the treatment plan, including regular medication, and review perpetuating psychosocial factors.
If reviewing dose, note that TCAs and venlafaxine have a wider dose responsiveness (a flatter dose– response curve) than SSRIs [64]. Greater scope to increase dose (subject to tolerance and toxicity) enables TCAs and venlafaxine to be considered if SSRIs are unsuccessful. TCAs are more effective for melancholic depression [65].
Antidepressant plus structured psychotherapy
Cognitive behavioural therapy (or, to a lesser extent, IPT) plus medication gives better results than either treatment alone [66–68] for depression or for comorbid anxiety and depressive disorders [69].
Augmentation strategies
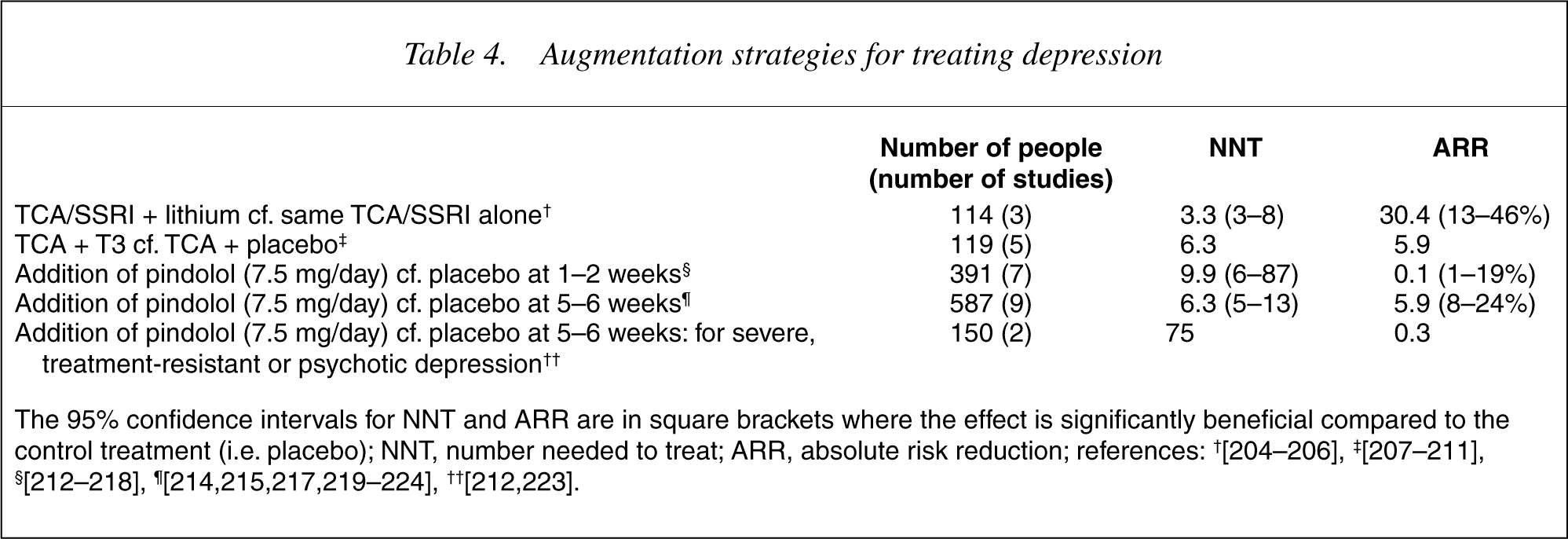
Table 4 summarizes augmentation of antidepressants with other agents when initial treatment is unsuccessful. Limited funding has restricted the number of subjects and, as studies are often uncontrolled, the risk of bias increases. There is significant evidence of benefit for lithium, and some for tri-iodothyronine. Pindolol, which is not licensed as an antidepressant in Australasia, hastens response to treatment.
Augmentation strategies for treating depression
Electroconvulsive therapy (ECT)
While the algorithm indicates that under ‘usual circumstances’ ECT is the fourth option, it may be selected earlier for individual patients. Randomized controlled trials recruit people with less severe illness than is common in practice, and in deciding whether to use ECT for severe, unresponsive depression, the specialist's best guide is experience rather than the limited literature.
The primary indication is major depression, especially with melancholia, psychotic features and/or suicidal risk. Raised intracranial pressure is the only absolute contraindication, but situations of risk requiring careful evaluation include hypertension, recent myocardial infarction, bradyarrhythmias, cardiac pacemakers, intracranial pathology, aneurysms, epilepsy, osteoporosis, skull defect, retinal detachment and concurrent medical illnesses.
Electroconvulsive therapy is administered by trained staff under medical supervision. While unilateral treatment of the non-dominant hemisphere is associated with less severe cognitive side-effects than bilateral treatment, its benefit remains controversial. Current recommendations are to start with unilateral treatment, unless the patient's prior treatment response or urgency dictate otherwise. A stimulus dosing approach with EEG monitoring is recommended. Details are available in RANZCP Clinical Memorandum #12 at <http://www.ranzcp.org>.
Electroconvulsive therapy's benefits are short-term and should be followed by maintenance medication. Initiation of medication during treatment is controversial [70–72]. Long-term maintenance ECT is not of proven benefit. Formal review and explicit consent are recommended.
Combined antidepressant treatments
Combination treatment is experimental and requires informed consent, preferably after a second opinion or discussion with a mood disorder clinic.
TCA and SSRI: This combination was common in the 1990s but not evidence-based. Venlafaxine is similarly effective, with less risk of severe side-effects.
TCA and MAOI: This combination can be fatal. It was not effective in placebo-controlled trials [73] and its major hazard necessitates a second opinion and informed consent.
Psychosurgery
Reserved for a tiny group with highly treatmentresistant and severe depression [74], psychosurgery is restricted in Australia to highly experienced services.
Continuation of treatment
Continuing treatment lowers the risk of relapse and improves psychosocial outcomes [75]. The few longterm studies have not identified when treatment can be withdrawn, although the benefits of continuing increase with the number of previous episodes [76]. As numbers in these trials decrease over time, confidence intervals widen. Subjects willing to take medication in such a trial may be atypical of clinical populations.
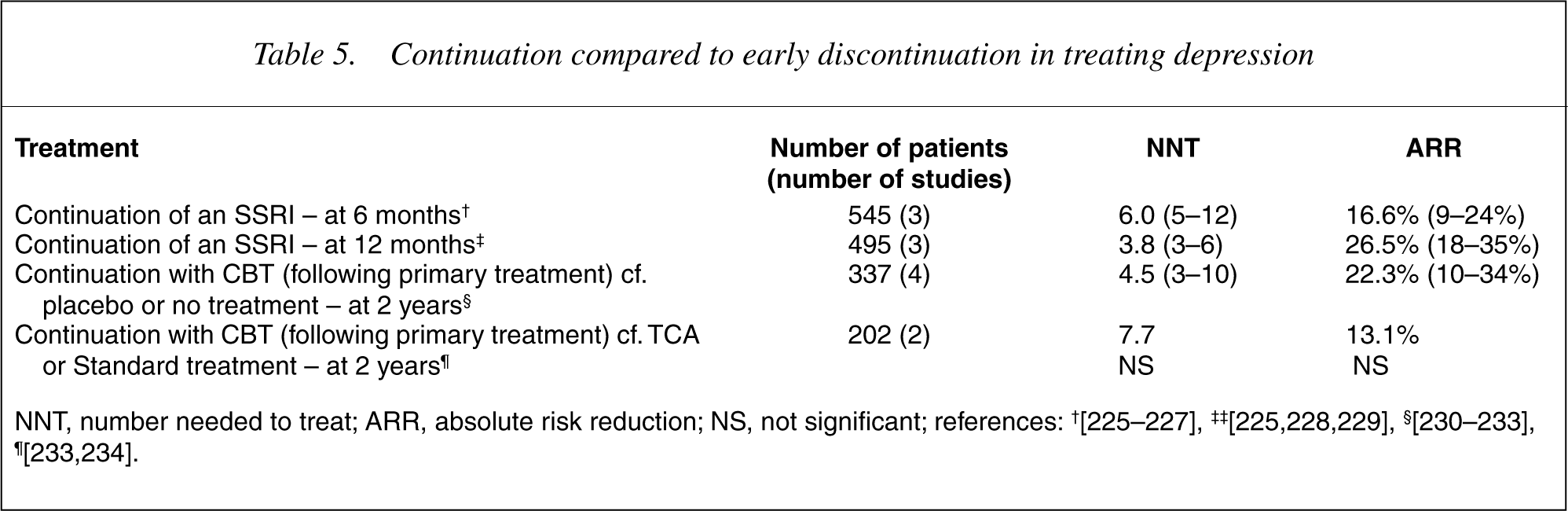
Shorter-term follow-up studies support continuation of treatment for 12 months following a first episode (Table 5). Expert consensus supports treatment for 3 years or more after recurrent episodes, following discussion of the potential benefits and burden of treatment. Intermittent treatment risks side-effects due to withdrawal, particularly with shorter-acting SSRIs [77].
Continuation compared to early discontinuation in treating depression
Atypical depression
Trials of newer antidepressants are lacking, and earlier studies are few and methodologically limited. The latter found phenelzine the most effective (NNT = 2.2, ARR = 45%) [78] followed by CBT (NNT = 3.4, ARR = 29.4%) [79], [80] and imipramine (NNT = 5.0, ARR = 20%) [78],[80–82]. But concerns about sideeffects and interactions with tyramine-containing foods prevail, and newer drugs are used first.
Depression with psychosis
Electroconvulsive therapy alone, or a TCA plus an antipsychotic, are much superior to TCA alone: (TCAs plus an antipsychotic vs. TCA: 6 studies [83–88] 181 patients, NNT = 2, ARR = 51%; ECT vs. TCA: 8 studies [83–86],[89–92], 445 patients, NNT = 2.1, ARR = 48%).
Indications for treatment away from home
These include suicidality, self-neglect, stressful context, need for psychological support in severe distress. Depending on needs and facilities, such care may involve friends and family, respite accommodation or inpatient hospital care.
Prevention of relapse
A sound therapeutic relationship is crucial to reducing relapse. It will provide psycho-education (identifying warning signs and how to respond), consider unresolved psychosocial issues, and seek to enhance support networks and maintain effective antidepressant treatment for an appropriate period, mindful of the number of previous episodes and of individual factors. Continued CBT is useful after primary treatment [93]. Such active relapse prevention is effective in primary care [94].
Enduring resistance to treatment
Some people do not respond adequately to a range of treatments. Options then include obtaining second opinions, discussion in a peer review group and referral to a mood disorder service. The psychiatrist maintains hope, provides support and ameliorates symptoms as far as possible until the depression remits and recovery ensues.
Discontinuing treatment
Duration of treatment takes into account its benefits and burdens, including risk of relapse. Treatment is discontinued gradually. Withdrawal reactions are common with shorter-acting SSRIs and halving the dose each week is one option. Abrupt cessation of TCAs may precipitate an anticholinergic withdrawal reaction (flulike illness, myalgia and abdominal cramps). Gradual withdrawal may prevent this.
Treatment of special clinical groups
Pregnant and breastfeeding women
While the teratogenic potential of most antidepressants, apart from mood stabilisers, appears low, few studies include information on child development [95]. Psychological treatments offer an alternative for pregnant women who are reluctant to take medication.
Studies of antidepressants and breastfeeding are often small and rarely measure concurrent maternal and infant blood levels. Most find transmission in breast milk to be limited, but there is considerable individual variation and immaturity of infant hepatic metabolic systems should be considered, particularly in the premature or ill [96], [97].
The frail elderly
As there are few studies of antidepressants in the frail elderly (unlike older people more generally [98]), start with a low dose and increase gradually. The elderly taking SSRIs are vulnerable to hyponatraemia.
Those with physical illnesses
The International Consensus Group on Depression and Anxiety felt unable to present guidelines for depression in cancer [99], due to limited evidence. However, the Cochrane Collaboration concluded that antidepressants improved depression in patients with a range of physical diseases, with an overall NNT of 4.2 and an NNH of 9.8 (Number Needed to Harm, here defined as treatmentdropout rate in excess of placebo) [100].
The risks and benefits of treatment must be weighed. The substantial risks of untreated depression include suicide, the burden of disease and its impact on other conditions. For example, depression increases morbidity and mortality for those with coronary artery disease, with or without recent myocardial infarction. Postinfarction, the risk is similar to that for post-infarction left ventricular failure [101].
Psychological strategies include group or individual CBT in multiple sclerosis and HIV-AIDS [102], but this is controversial in cancer [103].
When prescribing, consider whether mood results from the medical condition or from concurrent treatment, whether the antidepressant exacerbates or causes medical symptoms, and whether drug interactions could affect plasma drug levels.
Drug-induced alteration in mood
Prednisone may destabilize mood, particularly at higher doses (one in five people without previous psychiatric illness in the first week at daily doses over 80 mg) [104]. Carbamazepine, valproate and lamotrigine have a positive effect on mood, and phenobarbitone and vigabatrin an adverse effect. Propranolol and other lipid soluble beta-blockers, and occasionally less lipid soluble beta-blockers, can cause depression, as can alphamethyldopa. Rarely, oral contraceptives affect mood.
Specific conditions
Most studies are small, with limited power to detect rare adverse events. Consider the individual's overall health and consult with liaison psychiatrists or physicians.
Cardiac disease
Depression increases the risk of cardiac mortality threefold [105]. Consider specialist advice, since most antidepressants have contraindications. Tricyclic antidepressants should never be the first choice in cardiac, especially ischaemic, disease [106] as they are class 1A anti-arrhythmics and may induce arrhythmias. SSRIs and buproprion are safer, but large, long-term RCTs are needed to confirm their safety [101] and their place following myocardial infarction (e.g. [107]).
Lithium at therapeutic levels can cause sinus node dysfunction or sinoatrial block sufficient to alter consciousness. There is increased risk with ECT for those with cardiac disease, although its extent is debated. MAOIs may induce orthostatic hypotension. Trazodone can cause ventricular arrhythmias but appears safe for most patients [108]. Venlafaxine has not been studied in patients with cardiac disease.
Antihypertensives, especially diuretics, increase the likelihood that TCAs, trazodone or MAOIs will induce orthostatic hypotension.
Interactions between cardiac and antidepressant medications are described below.
Epilepsy
Standard treatments for depression (including ECT) are safe and effective for people with seizure disorders. However, maprotiline, amoxapine, bupropion and clomipramine, particularly in higher doses, are best avoided due to increased risk of seizures [109]. Carbamazepine, valproate and lamotrigine have a positive effect on mood, while phenobarbitone and vigabatrin have adverse effects.
Glaucoma
Anticholinergic drugs, such as TCAs and MAOIs, may precipitate acute narrow-angle glaucoma in susceptible individuals [110]. Antidepressants lacking anticholinergic activity (bupropion, sertraline, fluoxetine, trazodone) appear safe, but intra-ocular pressure should be carefully monitored.
Prostatism and obstructive uropathy
Antidepressants with antimuscarinic effects (e.g. most TCAs, trazodone and MAOIs) are contraindicated. Medications with the least propensity for this effect are fluoxetine, sertraline, bupropion and desipramine.
Drug interactions
Psychotropics may lead to a range of drug interactions. Some are described below and others can be predicted or suspected on the basis of cytochrome P450 based interactions, mindful that most psychotropics are metabolized in multiple pathways. A number of useful websites include <http://medicine.iupui.edu/flockhart/>. Any interaction involving a new drug, or any life-threatening reaction with an established one, should be reported to the Medicines Adverse Reaction Committee (MARC) in New Zealand or the Adverse Drug Reaction Assessment Committee (ADRAC) in Australia.
Anticoagulants
Warfarin interacts with many drugs. Citalopram, nefazodone and sertraline have relatively low interaction potential; fluoxetine and fluvoxamine relatively high. Carbamazepine appears to reduce warfarin's effects [111].
Cardiac medications
SSRIs and nefazodone interact with cardiac medications through cytochrome P450 and may induce adverse effects. MAOIs interact adversely with alpha- and betablockers and ACE inhibitors.
HIV-AIDS
Antidepressants and protease inhibitors and nonnucleoside reverse transcriptase inhibitors are metabolized by similar cytochrome P450 enzymes. As this increases drug levels, doses need adjusting.
Migraine
Fluoxetine and sumatriptan may interact and should be combined with caution [112].
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Lithium levels may increase with both unselective and selective COX inhibitor NSAIDs (e.g. rofecoxib) [113].
Interventions of unproven efficacy
St John's wort
While initially supported by trials in mild to moderate depression, more recent studies of better design, with patient HAM-D scores of <20, found that St John's wort is not superior to placebo (NNT = 23). Table 6 summarizes studies that use standard antidepressant doses. There are no studies in severe depression.
St John's wort compared with placebo, SSRIs and TCAs

Commercially available St John's wort contains varying amounts of the putative active compound hypericum and it is not clear whether there are other active compounds. The rate of side-effects is low, but significant drug interactions are consistent with St John's wort having both SSRI- and MAOI-like activity.
Transcranial magnetic stimulation (TMS)
There is scant evidence of benefit, but research samples have been small [114].
Omega-3 fatty acids
While omega-3 fatty acid levels are low in depression, there is no evidence that they improve depression. Further research is warranted [115].
Tryptophan and 5-hydroxytryptophan
Only two of the 108 trials are of adequate quality. Antidepressant activity, and association with the potentially fatal eosinophilia–myalgia syndrome, remain inconclusive [116].
Complementary and self-help treatments
A recent review concluded that none is well supported by evidence but some warrant further investigation [117].
Conclusion
The principal treatments have similar benefit. Compliance with a particular treatment depends more on the relationship between therapist and patient and on sustained support [118]. If treatment continues for at least 12 months, outcome is better than if stopped prematurely.
The principal recommendations are shown in Figs 2 and 3, with levels of evidence for depression with psychosis (Fig. 3) being less robust than those in Fig. 2. The place of ECT depends on the urgency of the situation and the patient's preference. Maintenance reduces the high risk of relapse or recurrence.
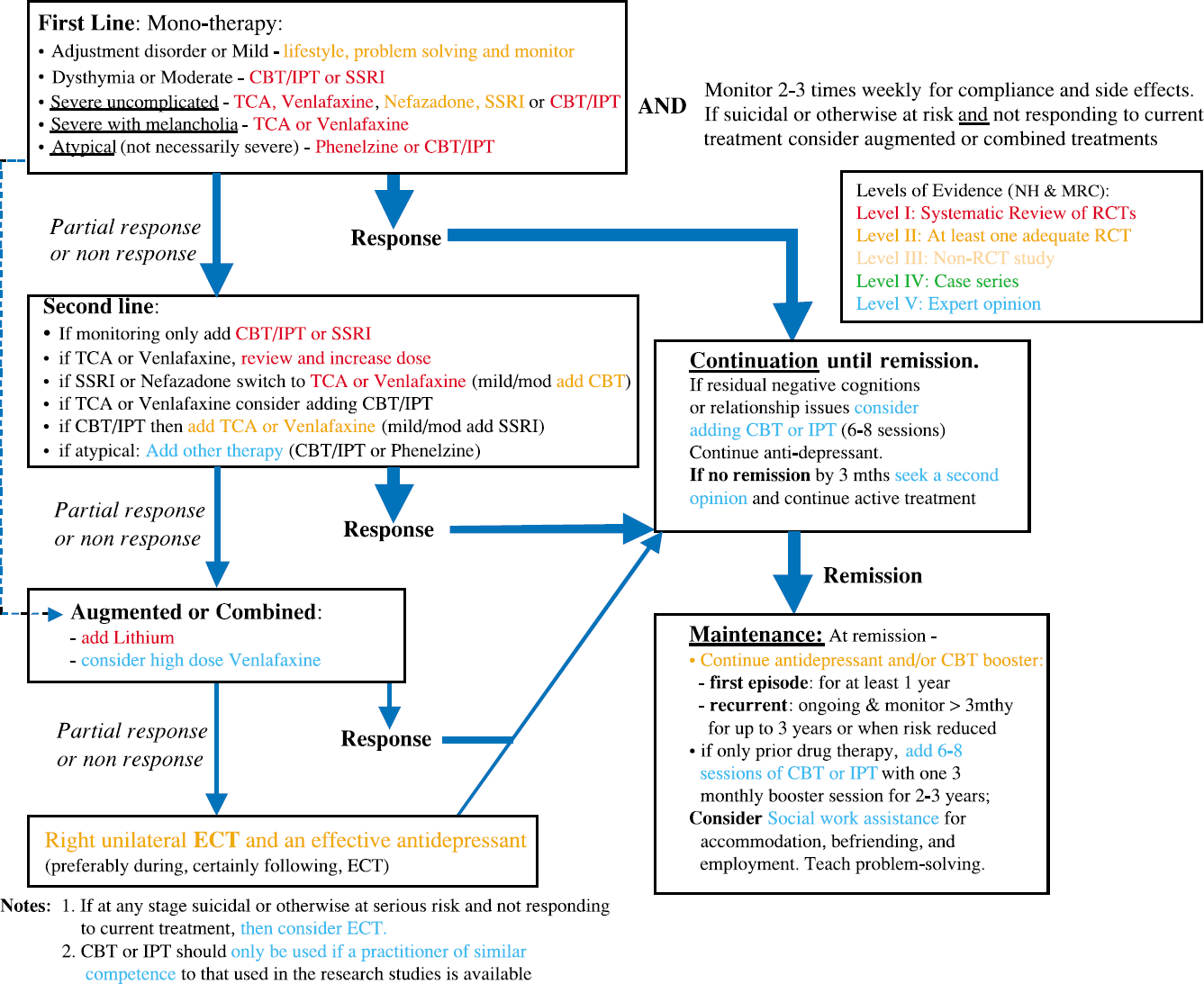
Principal evidence-based treatments for uncomplicated, melancholic or atypical depression (mild to high severity).
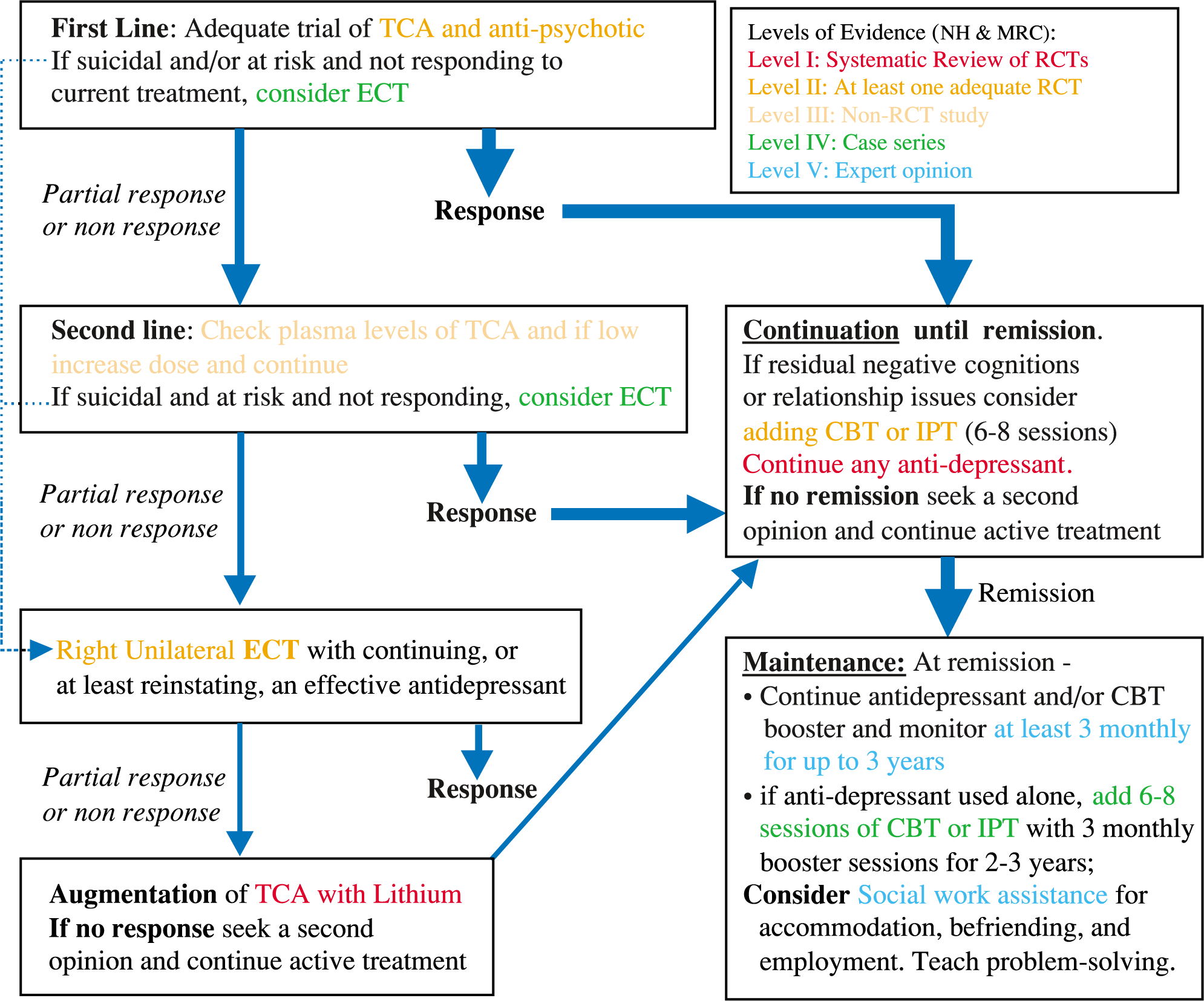
Principal evidence-based treatments for psychotic depression.
In summary, the evidence supports provision of the treatments specified above as part of an overall clinical management plan. Everyone with depression faces unique circumstances, and the clinician considers the extent to which evidence is pertinent. The aim of treatment is to achieve and maintain remission. Depression is a recurrent disorder, especially for those in secondary care settings. An active focus on prevention is tailored to the person's specific needs and strengths.
Footnotes
Acknowledgements
This paper was written by Pete M. Ellis, Ian Hickie and Don A.R. Smith.
CPG team:
Pete M. Ellis (Wellington School of Medicine and Health Sciences, University of Otago), Ian Hickie (University of Sydney), John Bushnell (Wellington School of Medicine and Health Sciences, University of Otago), Paul Hirini (School of Maori Studies, Massey University, Palmerston North), Suzy Stevens (Mental Health Foundation, Auckland: consumer consultant), Don A. R. Smith (Wellington School of Medicine and Health Sciences, University of Otago: project manager).
Phillip Boyce (psychiatrist), Sunny Collings (psychiatrist), Sue Fitchett (clinical psychologist), David Guthrie (consumer), Peter Joyce (psychiatrist), Phil Mitchell (psychiatrist), Malcolm Stewart (clinical psychologist), Grant Taylor (clinical psychologist), John Thorburn (clinical psychologist).
We thank Sidney Bloch for his editorial assistance.
Peter Ellis receives research funds from Eli Lilly for a study of antipsychotic drugs and has a managed share portfolio that contains some pharmaceutical company shares. Ian Hickie has received grants for research or sponsorship for educational activities, particularly related to treatment of depression by general practitioners, from a variety of pharmaceutical companies including Pfizer, Eli-Lilly, Bristol Myers Squibb and Wyeth. Additionally he has chaired advisory groups for the Australian Federal Government Department of Health and Ageing, related to the management of depression and other common mental disorders by general practitioners.