
Abstract
Keywords
This paper describes the use of variables derived from linguistic theory in a comparative empirical study of changes in the use of first person pronouns in the course of psychotherapy.
That changes in person pronoun use should occur in psychotherapy is suggested by the importance of concepts such as ‘self’ and ‘ego’ in psychotherapeutic and psychoanalytic theory [1], [2], these being commonly assumed to be expressed by first person pronouns, ‘I’, ‘me’, etc. [2–5]. Changes in personal pronoun use, moreover, if they occur, could be of practical importance: they might be helpful in monitoring change, for example, or in providing a simple measure of outcome (see Discussion section). Yet apart from some suggestive findings in Spence's studies of the patient–therapist relationship [6], [7], empirical evidence that changes in first person pronoun use do indeed occur in the course of psychotherapy has not previously been reported.
There is growing interest in linguistically defined variables for empirical research in psychiatry [8]. In the present study we drew on linguistic theory to define two distinct uses of the personal pronouns, syntactic and semantic. We also examined a number of non-pronoun linguistic variables, partly for comparison with pronoun variables, partly for their interest in their own right in respect of psychoanalytic and psychotherapeutic theory (see Discussion section).
Syntactic and semantic uses of the personal pronouns differ broadly as to grammar and meaning, respectively. As such, they do not always run parallel. For example, in ‘I chased the dog’ and ‘the dog was chased by me’, the syntactic uses of the first person pronouns, ‘I’ and ‘me’, are different even though the two expressions have essentially the same meaning [9].
Semantic uses of the first person pronouns, in reflecting individual meanings, could be defined in many different ways [10], [11]. There are indications from both the philosophy and sociology of medicine, that illness and recovery are most likely to be associated with semantic uses of the first person pronouns expressing specifically agentic aspects of these meanings: thus, the experience of illness is associated with incapacity (or loss of agency) [12], [13]; and Holmes and Lindley [14] argue that recovery of autonomy (hence of agency) is the central aim of most kinds of psychotherapy.
Frege's semantic theory [15] and the related logic of relations [16], [17] provide a resource for defining semantic variables connected with agency. Drawing on this resource, we defined two semantic positions, ‘alpha’ and ‘omega’. The details of this derivation, including the precise relationship between our semantic positions, Frege's ‘argument places’, and the ‘owner’ and ‘accidental’ of relations, are described elsewhere [18]. In brief, the alpha semantic position is characterized by occupancy of the ‘owner’ of a relation as defined in semantic theory, and the omega position is characterized by occupancy of the ‘accidental’ of a relation. In respect of verbs expressing actions, the alpha position is occupied by the agent. Thus, in both ‘I chased the dog’ and ‘the dog was chased by me’, I occupy the alpha position and the dog occupies the omega position. These semantic positions, however, are not restricted to actions. Similar positions are expressed by other classes of verb: for example, verbs expressing attitudes (x is against y) and states (x needs y).
The concept of a semantic position may be unfamiliar outside philosophical logic. However, the alpha and omega positions proved to be readily operationalizable through a set of explicit rules and exemplars, which, with a brief period of training, showed a high degree of interrater reliability (see Method section).
This study was designed to compare statistically a best outcome group with a worst outcome group for an increase/decrease in, respectively, syntactic and semantic first person pronoun variables between commencement and termination of a course of psychotherapy.
Method
Data and subjects
Our data were derived from a series of verbatim transcripts of psychotherapy sessions. The transcripts were originally made in the 1970s as part of the Pennsylvania Psychotherapy Study [19] and are now archived at the Ulm Textbank at the University of Ulm in Germany. All patients consented to the audio-recording of the sessions for the purposes of transcription and analysis. Names by which patients or other people could be identified were omitted or changed.
A major methodological advantage of the Penn Study for our analysis was that, from a total of 73 patients, the Penn investigators identified 10 patients with the best and 10 with the worst outcomes. This key selection process had thus been carried out completely independently of the present study.
Outcomes in the Penn Study were assessed by 14 psychometric instruments including patients' self-report measures, therapists' ratings, and independent clinical observer ratings. Using multiple regression analysis of the scores on each measure, ‘residual gain’ and ‘rated benefit’ scores were calculated. ‘Residual gain’ was calculated on the basis of ratings made at the beginning and again at the end of treatment. ‘Rated benefits’ was based on all the ratings immediately after the end of treatment. The ‘rated benefits’ and the ‘residual gain’ were highly correlated (r = 0.75). Hence the best outcome and the worst outcome groups were defined in the Penn Study by extreme scores on either of these measures. In the best outcome group, seven were selected on the basis of residual gain, three by rated benefits; in the worst outcome group, eight were selected by residual gain, two by rated benefits.
A disadvantage of the Penn Study for our purposes was that, having been carried out in the 1970s, diagnostic information was relatively unsophisticated by present standards. The subjects of the Penn Study were diagnosed with depressive neurosis, anxiety neurosis, and mixed neurosis. The two groups (best and worst outcomes) appeared similar overall (in particular, there were no psychotic subjects) but formal diagnostic comparisons were not possible from the available data.
The best and worst outcome groups were also not significantly different in age, gender, marital status or religion. All subjects had either one or two sessions each week. Eighteen psychodynamically orientated therapists were involved in the study (two therapists had two cases and the rest one case each). They had a minimum of eight to a maximum of 264 sessions, with a median of 32 sessions over a median of 34 weeks. Best outcome patients were in therapy longer than worst outcome (median 61 and 43 weeks, respectively).
Definition of variables
(i) Overall use of first person pronouns and verb phrases. We examined the commencement and termination frequencies for all verb phrases that were associated with a first person pronoun, and all that were not.
(ii) Syntactic usage of first person pronouns. The variables defined for investigating syntactic usage were ‘I’, ‘me’, ‘we’, ‘us’, as well as ‘implied I’ and ‘implied me’ (e.g. as in ‘I ate my food and (I) talked to her’, and ‘she said (to me)…’).
(iii) Semantic usage of first person pronouns. The variables for assessing semantic usage were the ‘alpha position’ and ‘omega position’, as described earlier. We used ‘unclear position’ for expressions where the patient's semantic position was not clearly evident (e.g. in ‘I was bored’).
(iv) Non-pronoun linguistic variables. Non-pronoun variables were use of the passive voice, negatives (‘not’ and ‘never’), copulas (e.g. ‘to be’, ‘seem’, ‘appear’), and auxiliary verbs expressing a sense of obligation (e.g. ‘ought to’, ‘got to’, ‘have to’, ‘must’, ‘should’).
Recording and procedures
The basic unit of observation was a verb phrase. Besides a main verb, a verb phrase may also include auxiliary verbs. For example, in ‘I ought to have written to Jim’, the verb phrase is ‘ought to have written’. Each verb phrase was examined for the presence or absence of all the above variables in association with that verb phrase.
For each of the 20 subjects, two commencement sessions and two termination sessions were examined, giving a total of 80 sessions. In all cases we followed the definitions of commencement and termination sessions adopted by the Penn investigators. Thus, for a given subject, the commencement sessions were sessions 3 and 5; the termination sessions were the session in which 90% of the therapy was complete and the immediately preceding session. All termination sessions were within five sessions of the end of therapy. The first 200 verb phrases of each of the 80 sessions were analyzed.
The presence or absence of the variables in each verb phrase was recorded in binary code. Frequencies of the variables in the sample were calculated as the ratio (expressed as a percentage) of the number of ‘present’ recordings for a particular variable to the total number of analyzed verb phrases in the relevant two sessions (i.e. either the two commencement or the two termination sessions). This generated a commencement frequency and a termination frequency for each variable for each patient.
The change between commencement and termination frequencies of variables was calculated for each patient as the difference between commencement frequency (C) and termination frequency (T) proportionate to the commencement frequency, expressed as a percentage. Thus, % change = 100 × (C−T)/C.
Since the transcripts were not edited, operational rules of recording were developed to deal consistently with phenomena like halfsentences and single word expressions. The operational rules (available on request from WVS) included for example: a verb phrase should be identifiable before any recording is made; repetitions (like stuttering) of a first person pronoun associated with a certain verb phrase should be omitted; colloquial use of first person pronouns should not be corrected; direct quotations by a patient from someone else should be excluded.
The reliability of the recording procedures was assessed by sampling 100 verb phases from a randomly selected psychotherapy transcript and subjecting them to blind analysis by five sixth-year medical students from the University of Pretoria (South Africa). All the abovementioned variables were present among these verb phrases. The students had a preliminary 15 minute training session in the operationalized procedures for identifying and recording variables. The mean concordance rate between the study recordings and the student recordings was 94% (SD = 1.85%; range: 92–96.7%). The Kendall Coefficient of Concordance among the recordings of the students was 0.0011, which is highly satisfactory.
Statistical analysis
The best and the worst outcome groups were compared using either the independent samples t-test or the Mann–Whitney U-test. The t-test was used where the distribution of the changes in frequencies between commencement and termination of therapy was consistent with a normal distribution. This test did not assume equal variances. Where the data did not follow a normal distribution, the Mann–Whitney U-test was used. The extent to which the data followed a normal distribution was assessed by visual inspection of graphic representations of the distributions of the cumulative frequencies, and by the Kolmogorov-Smirnov and Lilliefors tests.
Results
Overall use of first person pronouns and verb phrases
The commencement frequencies of all first person pronouns taken together were similar for the best outcome (mean = 62.89%, SD = 5.41%) and the worst outcome patient groups (mean = 62.19%, SD = 7.46%). The termination frequencies were lower in both groups, the best outcome group showing a mean decrease of 10.14% (SD = 12.07%), the worst outcome group a mean decrease of 10.05% (SD = 6.74%). These decreases were not significantly different between the two groups (t = 0.021, df = 14.11, p = 0.984, mean difference = 0.0913, 95% CI = −9.28–9.46).
Correspondingly, there was no significant difference between the best and the worst outcome groups for change in verb phrases that were not associated with a first person pronoun (t = −0.041, df = 16.05, p = 0.968, mean difference = −0.279, 95% CI = −14.75–14.20).
Syntactic usage of first person pronouns
No statistically significant differences were found between the best and the worst outcome groups in their syntactic usage of first person pronouns.
The frequency of ‘I’ showed a very small increase between commencement and termination of psychotherapy for both patient groups (best outcome patients: mean increase of 0.33%, SD = 9.11%; worst outcome patients: mean increase of 0.50%, SD = 6.63%) (Fig. 1). The difference between the best and the worst outcome patients in this respect was not statistically significant (t = 0.049, df = 16.15, p = 0.962).
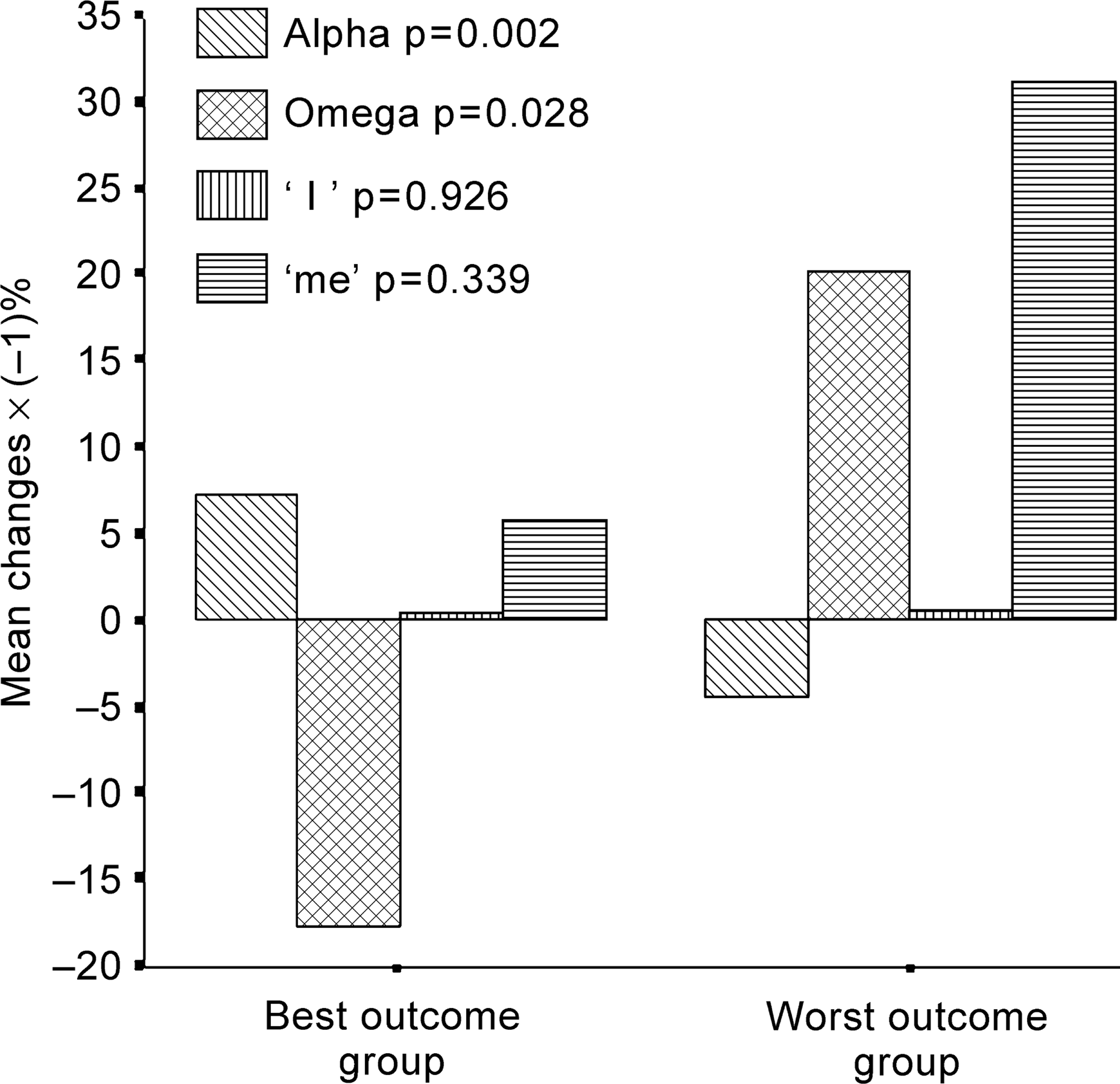
Mean changes of ‘I’, ‘me’, alpha positions and omega positions between commencement and termination of psychotherapy for best and worst outcome groups.
The mean frequency of ‘me’ increased for both groups (best outcome patients = 5.73%; worst outcome patients = 31%) (Fig. 1) but the standard deviations were large (43.7% and 68.62%, respectively). Correspondingly, no statistically significant differences were found between the two groups of patients in their change in the usage of ‘me’ (t = 0.099, df = 15.27, p = 0.339).
The frequency of ‘we’ showed larger mean increases than ‘I’ or ‘me’ for both patient groups between commencement and termination. Moreover, the best outcome patients' mean increase in the frequency of ‘we’ (215.22%, SD = 347.45%) was higher than the worst outcome patients' mean increase (43.83%, SD = 171.98%). The difference between the patient groups in this respect, however, still did not reach the 0.05 level of statistical significance (U-test = 23.0; p = 0.131). This is most likely due to the large variance in the patients' changes of frequencies (cf. the large SD values cited earlier). Missing data may also have contributed to the non-significant result since two of the worst outcome patients did not use ‘we’ at all during the analyzed part of the commencement sessions, and hence (as zero scores) had to be excluded from calculating the percentage change between commencement and termination of therapy.
The best outcome group showed a mean decrease of frequency of ‘us’ (28.85%, SD = 104.54%); and the worst outcome group showed a mean increase (69%, SD = 143.99%). As for ‘we’, statistical testing between the groups was not useful because commencement frequencies were zero for two of the best outcome and six of the worst outcome patients, and therefore had to be excluded from calculating the percentage change between commencement and termination of therapy.
No statistically significant differences were found between the best and worst outcome patient groups in their uses of ‘implied I’ (U-test = 35.0, p = 0.257) or ‘implied me’ (U-test = 38.0, p = 0.364).
Semantic usage of first person pronouns
In contrast with the syntactic usage of first person pronouns, significant changes were found in semantic usage. These positive findings are compared with the negative findings for the syntactic variables, ‘I’ and ‘me’, in Figure 1.
Thus, the alpha position increased among the best outcome patients (mean increase of 7.14%, SD = 7.38%) and decreased among the worst outcome patients (mean decrease of 4.40%, SD = 6.46%). The difference between the best outcome and the worst outcome patients was highly significant (t = −3.72, df = 17.69, p = 0.002, mean difference = −11.54, 95% CI = −5.06 – −18.07). The upper value of the confidence interval suggests an increase of the alpha position in at least 95% of similar comparisons.
The omega position changed in the opposite direction from the alpha position. The omega position decreased among the best outcome patients (mean decrease of 17.79%, SD = 19.95%) and increased among the worst outcome group (mean increase of 20.18%, SD = 38.74%). The difference between the patient groups was statistically significant (U-test = 21.0, p = 0.028).
The changes in the alpha and the omega positions for individual subjects are shown in Figure 2 (alpha position) and Figure 3 (omega position). Visual inspection shows opposite directions of the changes for the two groups of subjects: the predominant response shown by subjects in the best outcome group was an increase in the alpha and a corresponding decrease in the omega positions, whereas in the worst outcome group the predominant response was a decrease in the alpha and an increase in the omega positions. This means that an increase in frequency of the alpha position has a sensitivity and specificity of 0.8 to identify correctly both the best and worst outcome groups, and a decrease in the omega position has a sensitivity of 0.8 and specificity of 0.6 to identify the best and worst outcome groups, respectively.
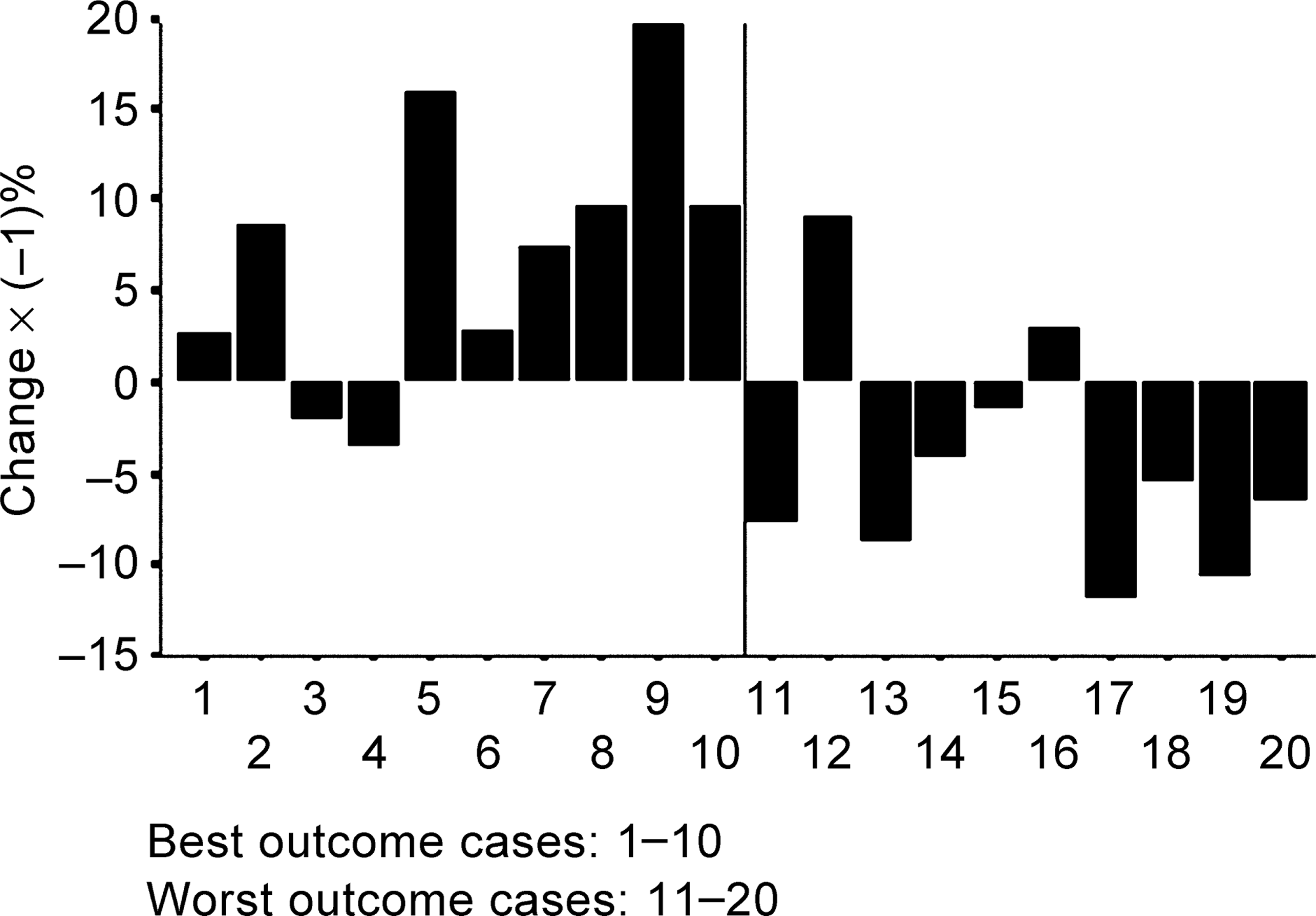
Change in the frequency of the alpha positions between commencement and termination of psychotherapy for each case.
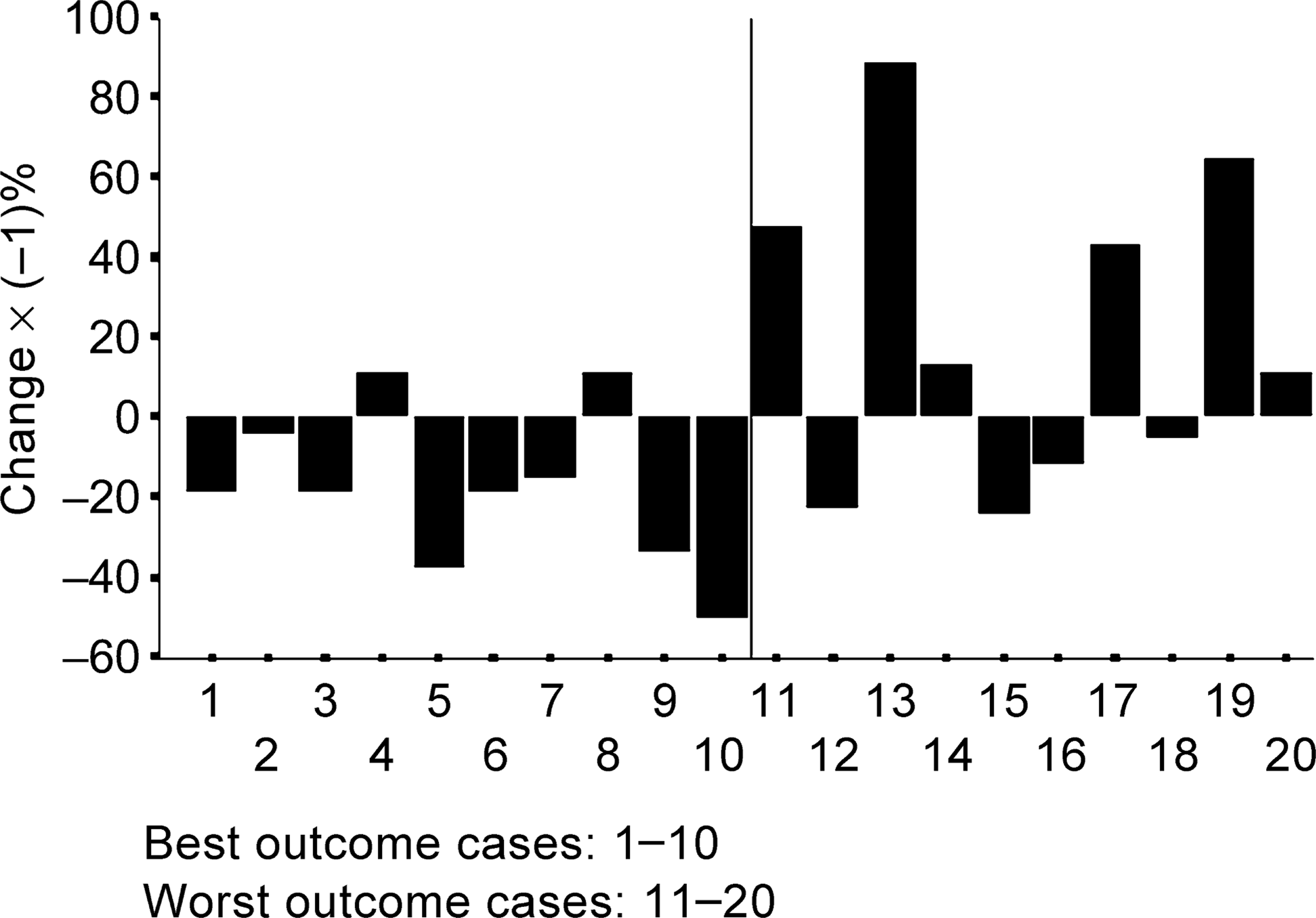
Change in the frequency of the omega positions between commencement and termination of psychotherapy for each case.
For the ‘unclear position’, no statistically significant differences were found between the patient groups (U-test = 42, p = 0.545).
Non-pronoun linguistic variables
No significant differences were found between the best and the worst outcome groups for change in any of the non-pronoun linguistic variables, namely the passive voice (U-test = 48.0, p = 0.880), the negative (U-test = 43.0, p = 0.597), a copula (t = −0.608, df = 17.07, p = 0.551, mean difference = −5.25, 95% CI = −23.46–12.97), and auxiliary verbs that express a sense of obligation (t = 1.715, df = 11.26, p = 0.114, mean difference = 38.36, 95% CI = −10.72–87.46).
Discussion
The main finding of this study is that semantic (meaning-driven) usage of first person pronouns changed over the course of good outcome psychotherapy. Occupancy of what we have defined as the alpha (semantic) position increased, while occupancy of the omega position decreased, in patients with good outcome. Occupancy of the two positions, furthermore, was inversely related. That is, occupancy of the alpha position was taken up at the expense of occupancy of the omega position in a majority of individual patients. Syntactic (grammatical) usage of first person pronouns, by contrast, and a number of non-pronoun linguistic variables, all showed no significant changes between the best and worst outcome groups.
The study clearly has limitations as well as strengths. The resources of the Penn Psychotherapy Project gave us access to a series of verbatim psychotherapy transcripts, collected originally for purposes unrelated to our research, and independently grouped for outcome on a series of outcome measures. This supported a valid measure of outcome in this study, but the influences of potential confounding variables had not been known to us and could not be investigated. For example, we could not account for diagnostic details, knowing only that patients were diagnostically heterogeneous and included none with psychotic disorders. Furthermore, the detailed analysis required of the transcripts (examination of 16 000 verb phrases for each of 13 variables) meant that we were able to study only a relatively small number of patients (i.e. 20 from a sample of 73).
Granted these constraints, what is the significance of our findings?
Practical utility
Our results provide quantitative evidence to support the clinical observation that recovery brings about a change from a passive position to a more active (agent) position. Active and passive positions, however, should not be directly equated with alpha and omega positions [18]. The active–passive distinction is at times ambiguous, for example in passive aggression, whereas the alpha–omega distinction derives its clarity from philosophical logic.
Our results suggest further that psychotherapeutic recovery could be tracked linguistically. Doing so may prove useful to enhance the therapeutic process. As considered elsewhere in more detail, cognizance of the semantic positions could supplement the dynamic understanding in analytic therapies and could aid the restructuring of thoughts and behaviour in cognitivebehavioural therapies [18].
Diagnostically, the shift from omega to alpha positions could provide the basis for the development of relatively simple ‘litmus tests’ of progress and outcome in psychotherapy. Psychotherapy, in all its forms, is both costly and notoriously difficult to assess. Linguistic markers, being comparatively simple to use, would allow treatment plans to be fine-tuned, avoiding blind alleys in therapy, and building on approaches which look promising. As measures of outcome, similarly, linguistic markers, being relatively objective, could contribute to the development of more accurate clinical guidelines on the profiles of patients likely to benefit from this or that particular form of therapy.
Future research
Further work is required to determine whether such tests are indeed valid and viable. Findings of this study suggest that an assessment of the semantic positions of patients, rather than an assessment of syntactic use of first person pronouns, would be a valid measurement of recovery in psychotherapy. This validity is so far based on the rigorous theoretical description of the semantic positions (i.e. the content validity) [18], and on the ability to distinguishing between contrasting groups that had been independently grouped for outcome (i.e. the external criterion validity which is demonstrated in the concurrent validity by using t-tests and Mann-Whitney U-tests, and in the ability to predict the outcome groups based on either an increase in the frequency of alpha positions or a decrease in the frequency of the omega positions) [20]. However, these are the first steps for a comprehensive testing of validity in the future. The reasons are that convergent validity was not tested, because the specific measurements of the Penn study had not been available, and our results need to be replicated using other psychotherapy materials (the Penn Project transcripts might be unusual in some way). It will also be necessary to examine specific diagnostic groups and other forms of treatment. The heterogeneous nature of our subjects, and the theoretical links (noted in the Introduction section) between our semantic variables and agentic aspects of illness and recovery, suggest that taking up occupancy of alpha positions and relinquishing occupancy of the omega positions may be a generic, or at any rate a general, marker of progress and good outcome. But whether or not this is so, only further research will show.
The reliability and practical utility of using linguistic markers in this way would have to be assessed under ‘field’ conditions. The medical students involved in our reliability study achieved a highly satisfactory level of inter rater reliability after only 15 min of training in the scoring methods. But they were working under ideal conditions, away from the demands of clinical work, and on materials in which they had no direct interest, personal or professional.
Additional work is needed to determine the dynamics of the shift from omega to alpha semantic positions. We sampled the commencements and terminations of the psychotherapy transcripts. But if the shift from omega to alpha is to be used as a measure of progress, we need to know whether it occurs continuously over the course of therapy or discontinuously; if discontinuously, whether it is an early or late change; and we need to know whether the dynamics are the same or different for different diagnostic groups and from patient to patient.
The connection with psychotherapeutic and psychoanalytic theory, suggests that linguistic variables might be helpful in sharpening and developing therapeutic models of disorder. Non-pronoun as well as pronoun variables could be helpful here. In this study, for example, among non-pronoun variables, we found no significant changes in the use of the negative. This is surprising given the significance attached to overcoming denial in psychodynamic therapy [21]. Denial is not necessarily expressed verbally in the use of negatives, of course; nor are all verbal expressions of the negative reflections of psychological denial. But the finding, which so far as we are aware is reported here for the first time, is at least suggestive. Similarly, the absence of any change in the use of auxiliary verbs expressing obligation (‘I must…’, ‘I have to…’, ‘I should…’, etc.) is contrary to the expectations of rational emotive theory, a key component of which is to challenge and then relinquish thoughts of obligation [22].
Furthermore, the bearing of our findings on psychoanalytic and other theories about first person pronouns need to be researched. A connection with the work of Jacques Lacan was outlined by Gillett [23], and other theoretical connections with egotism and narcissism are to be expected. For example, egotism is commonly associated with the excessive use of first person pronouns [24], but our findings suggest that the overall frequency of first person pronouns does not differ significantly between the best and the worst outcome patients, neither at commencement nor at termination of psychotherapy. This may mean that egotism, and likewise narcissism, may be relevant to some but not all instances of first person pronoun use. One hypothesis could be that egotism and narcissism present in certain kinds of relations (e.g. recognition, admiration, appreciation) rather than in all relations expressed in association with first person pronouns [25].
Methodological innovation
Meanings, as no less a figure than Karl Jaspers emphasized, are crucially important alongside causes in psychopathology [26], and are set to become more, not less, important in psychiatry with advances in the neurosciences [27], [28]. Our study shows that it is possible to draw on philosophical logic as a source of reliably operationalizable variables for quantitative research on meanings related to first person pronouns. It is in this respect that it is methodologically innovative.
There have been other philosophical resources for studying meanings in relation to first person pronouns. The philosophical pragmatists Mead and Pierce focused on the purposes of using ‘I’ and ‘me’ as symbols [29], [30]. So did some psycho-analytical theorists [2–4],[31]. This study, however, investigated empirically the meaning as revealed within patient expressions irrespective of the underlying purposes of using these pronouns [32]. Phenomenology is another philosophical resource, one on which Jaspers drew in developing his ‘Ich-störungen’ (i.e. disorders of ‘I’) in psychopathology. Phenomenology is currently reinventing itself as an empirical discipline [33] with considerable potential in this respect [34]. But philosophical logic, as an analytic rather than interpretive philosophical discipline, holds out the prospect of rigorously defined variables for research in the human sciences, comparable, in some respects, with those available from mathematics for the physical sciences. This is a challenging prospect, certainly. But as Jaspers clearly saw, it is no more than we should expect of a science encompassing, as psychiatry encompasses, meanings as well as causes.
Footnotes
Acknowledgements
We thank J. Z. Sadler, M. Luntley and C. Krüger for advice, as well as the Ulm Textbank (Department of Psychotherapy, University of Ulm, Germany) who kindly provided the psychotherapy transcripts.