
Abstract
Dissociation, defined as ‘a disruption in the usually integrated functions of consciousness, memory, identity, or perception of the environment’ [1], and the corresponding symptoms refer to disparate clinical phenomena such as amnesia for personally relevant information, identity disturbances or depersonalization [2–4]. It represents the core feature of the dissociative disorders, and is among the diagnostic criteria for acute and post-traumatic stress disorder (PTSD), as well as borderline personality disorder [1, 5–7]. Moreover, dissociative phenomena are frequently found in a wide variety of mental disorders, for example schizophrenia, affective disorder, obsessive–compulsive disorder (OCD), somatoform disorder, and anxiety disorder as well as eating disorders [8–13].
Despite the clinical significance of dissociation, research on its impact on treatment outcome has only just begun to emerge [14, 15]. The first investigation on this issue reported dissociative symptoms to be predictive of poor treatment response, high relapse rates and poor maintenance over a 1 year follow up in 89 subjects meeting DSM-III criteria for agoraphobia with panic attacks, who had been treated with cognitive behavioural therapy (CBT) [14]. Most recently, a prospective CBT study including 52 patients with OCD indicated that a higher degree of dissociative experiences at baseline was associated with more severe OCD symptoms at post-treatment assessment [15]. Furthermore, treatment non-responders had significantly higher baseline dissociation than responders [15].
Although the cited investigations have contributed valuable new insights, they hold some methodological limitations. First, they included only subjects with specific diagnoses (i.e. panic disorder with agoraphobia and OCD), and few or no comorbid disorders. Furthermore, because CBT was applied in both studies, it remains open whether or not the findings can be generalized to other forms of psychosocial treatment. Additionally, the impact of interpersonal problems that were shown to influence the outcome [16] was not taken into account as a confounding factor. Finally, Michelson et al. assessed dissociation retrospectively 3–5 years after the completion of the treatment trial [14]. Considering these aspects, we hypothesized that higher levels of dissociation predict poorer treatment outcome also in a naturalistic setting, that is, among inpatients with a broad range of non-psychotic mental disorders participating in residential brief psychodynamic psychotherapy. We controlled for confounding effects of comorbid disorders (both axis I and II) and interpersonal problems. Additionally, we took into account that dissociative experiences significantly co-vary with general psychopathology [17, 18]. Given the naturalistic design of our study and in line with previous research [19, 20], we chose improvement of general psychopathology as the main outcome criterion because it best reflects the focus of everyday clinical practice.
Method
Procedure and subjects
The study was conducted at one of the psychotherapy units of the department of psychiatry and psychotherapy at the University of Greifswald, Germany. This unit offers an inpatient treatment programme for patients with depressive, anxiety, and somatoform disorders. Whenever alternative treatment options are lacking, patients with adjustment and eating disorders can be admitted, too. A detailed description of the therapeutic programme is published elsewhere [21]. In sum, it is based on the principles of psychodynamic, short-term group therapy, which takes place three times a week with each session lasting 60 min. Its duration ranges between 4 and 8 weeks depending on the individual response. The selection criteria for the programme are: adult age, and definite exclusion of any organic or acute psychotic disorder, as well as suicidal tendencies or self-destructive behaviour that cannot be treated in an open setting.
For the purpose of the present study, which was conducted between 1 January 1999 and 31 December 2000, we excluded patients without enough knowledge of the German language (n = 9) and those with a dissociative disorder (n = 6). Within the study period, a total of 341 patients met the inclusion criteria but 131 (38.4%) refused to participate. In order to yield meaningful outcome data, those attending the programme for at least 4 weeks were followed up at the end of their treatment. Fifty-one patients (24.2%) with an intention to treat terminated their treatment prematurely, that is, in <4 weeks. Another 26 refused to participate in the follow-up investigation shortly before discharge. The remaining 133 participants who gave written informed consent after full explanation of the study were assessed at admission (all instruments) and shortly before discharge (Symptom Check List-90–Revised; SCL-90-R).
The mean age of the sample was 39.6 years (SD = 12.0) and it consisted of 102 women (77%) and 31 men (23%). The mean duration of treatment was 42.3 days (SD = 14.1). The clinically leading diagnoses as assessed by standard clinical interview according to the ICD-10 criteria [5] were: depressive disorders (n = 91), phobic and anxiety disorders (n = 25), obsessive-compulsive disorders (n = 2), adjustment disorders (n = 3), conversion disorders (n = 5), somatoform disorders (n = 3) and eating disorders (n = 4). A second axis I disorder was diagnosed in 47 patients (35.3%). Independent of axis I disorders, 24 participants (18.0%) presented with a comorbid substance use disorder and 37 (27.8%) patients had an additional personality disorder.
Instruments
The SCL-90-R is a 90-item, widely used self-report measure of current psychopathology [22]. In addition to nine syndrome scales a global rating (Global Severity Index, GSI) reflects the general psychological distress. The values for reliability and validity of the German version of the SCL-90-R are similar to those of the original version [23]. Both the SCL-90-R and the GSI are frequently used in psychotherapy research, especially when assessing psychotherapeutic change [20, 24]. For the purpose of the present study we chose the GSI as the main outcome variable. Patients were defined as responders if their degree of change on the GSI was statistically reliable and not simply an artefact of measurement error according to the Reliable Change Index (RCI) method proposed by Jacobson and Truax [25]. This method involves calculating the difference between the post- and pre-treatment scores (Δ-GSI = post-GSI − pre-GSI) divided by the standard error of the difference: RCI=(post-GSI − pre-GSI)/Sdiff. An RCI >1.96 is required for reliable change (p < 0.05). In addition to this categorical approach (i.e. response vs non-response), Δ-GSI was used as a dimensional outcome variable.
The Fragebogen zu Dissoziativen Symptomen (FDS-20) [26] represents a 20-item short form of the German version of the Dissociative Experiences Scale (DES) [27], which is an internationally well-established, self-administered inventory to measure the frequency of dissociative experiences. Both the DES and the FDS-20 have sound psychometric properties [26, 28].
The Inventory of Interpersonal Problems-Circumplex (IIP-C) [29] dimensionally assesses the nature of dysfunctional interpersonal patterns and provides a total score indicating the general degree of interpersonal problems. The psychometric properties of the German version of the IIP-C are very similar to those of the original version [30].
Statistical analysis
The data analyses were computed using SPSS, version 12.0 (SPSS, Chicago, IL, USA). Responders and non-responders were compared using analyses of variance for continuous variables and χ2 test for categorical variables. Associations were determined using Pearson's correlation coefficients. Binary logistic regression was used to calculate regression coefficients (β), odds ratios (ORs) and 95% confidence intervals (CI) with non-response as a dependent variable. Axis I, substance use and personality disorder comorbidity (no diagnosis = 0; present diagnosis = 1), baseline interpersonal problems (pre-IIP), as well as initial dissociative and general psychopathology (pre-FDS-20 and pre-GSI, respectively) were entered as independent variables. The relationship between change in psychopathological distress (Δ-GSI; dependent variable) and dissociation (independent variable) was assessed by means of linear regression, again controlling for the effects of comorbid diagnosis, pre-GSI and pre-IIP. For each variable, a standardized regression coefficient (standardized β) is reported, which is based on a prior z transformation. It indicates the relative magnitude of prediction of each variable. The significance of β was evaluated by a t statistic. All predictor variables had tolerance values >0.4 excluding colinearity. Significance level was set at p < 0.05.
Results
There were no differences with respect to age, gender distribution, diagnoses or additional substance use and personality disorders between eligible patients refusing to be enrolled in the study and those participating (data not shown). Patients lost to the follow up (i.e. premature termination of treatment, n = 51; or refusal of follow-up assessment, n = 26) did not differ from participants with respect to age, gender distribution, diagnoses or additional substance use and personality disorders. Furthermore, there were no differences with respect to baseline dissociation scores or degree of interpersonal problems (data not shown). However, the drop-out sample had significantly lower scores in overall psychopathology (GSI 1.22±0.79) than the completers (GSI 1.55±0.80; F = 6.354, p = 0.013).
Out of the 133 patients included in the present study, 83 (62.4%) were treatment responders and 50 (37.6%) did not show a statistically significant change of their general psychopathology from pre- to post-treatment assessment as measured by the GSI. Responders and non-responders did not differ with respect to age (40.8±12.3 years vs 37.6±11.3 years; F = 2.143, p = 0.146), treatment duration (42.8±12.9 days vs 41.6±16.0 days; F = 0.238, p = 0.627), and gender distribution (78.3% vs 74.0% women; χ2=0.325, p = 0.569). However, the baseline GSI was significantly higher in responders (1.75±0.76) than in non-responders (1.22±0.75; F = 15.178, p < 0.001). There were strong and positive correlations between GSI and FDS-20 scores at baseline (r = 0.67, p < 0.001), GSI and IIP total scores at baseline (r = 0.58, p < 0.001), as well as pre-GSI and Δ-GSI (r = 0.57, p < 0.001). Thus, baseline GSI was entered as a covariate in all subsequent analyses. Controlling for baseline GSI, the non-responders had significantly higher pretreatment dissociation scores than the responders (F = 7.012, p = 0.009). Figure 1 depicts the adjusted means of the baseline FDS-20 scores depending on the outcome.
Comparison of adjusted mean baseline dissociation scores (Fragebogen zu Dissoziativen Symptomen-20) between responders and non-responders.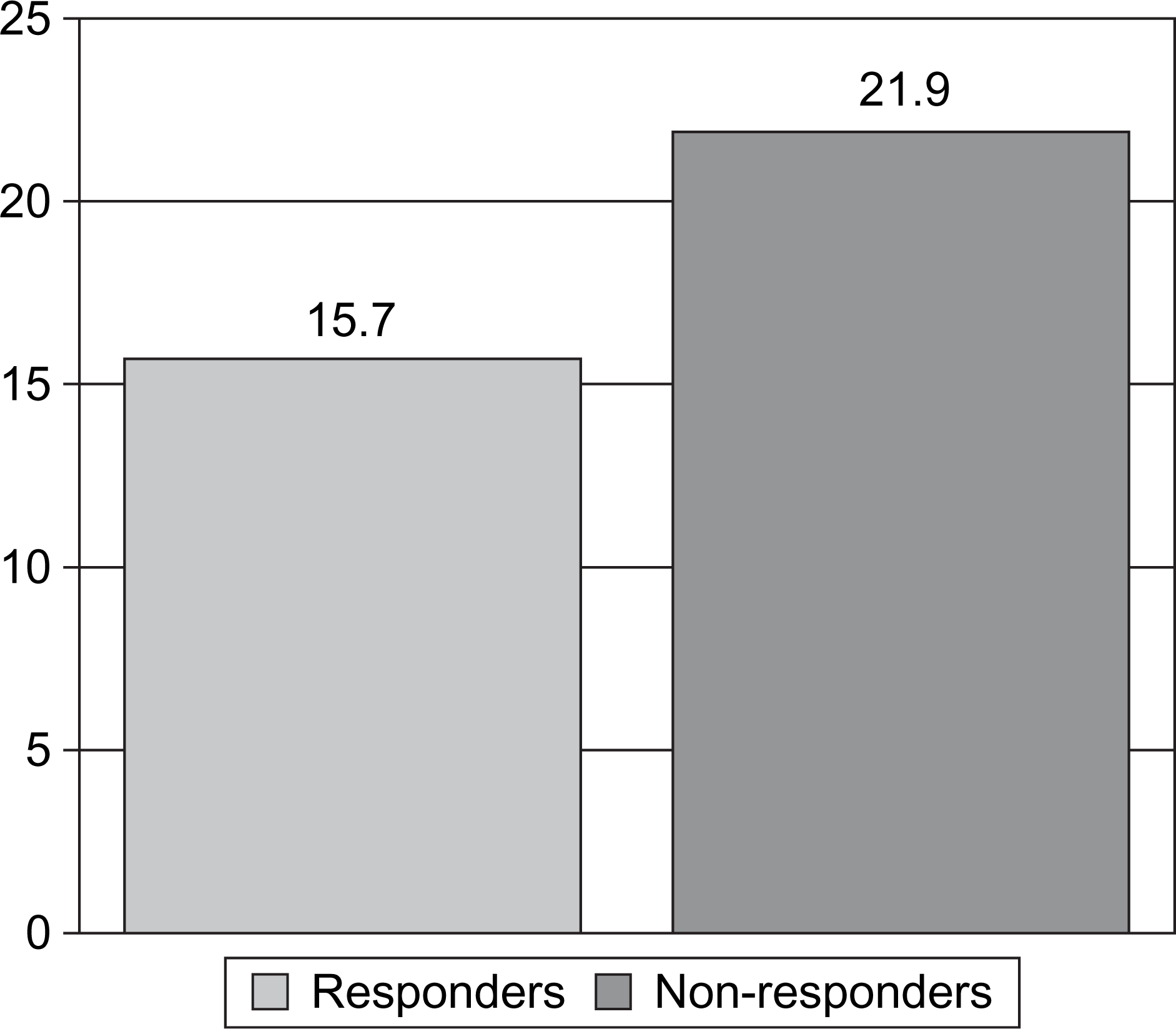
In a logistic regression with non-response as a dependent variable, comorbid axis I and substance use disorder as well as baseline interpersonal problems did not emerge as relevant predictors. In contrast, presence of comorbid personality disorder, low baseline psychopathology and high pretreatment dissociation all emerged as significant predictors for non-response. A detailed description of the findings is provided in Table 1.
Significant predictors of non-response (stepwise backward logistic regression)
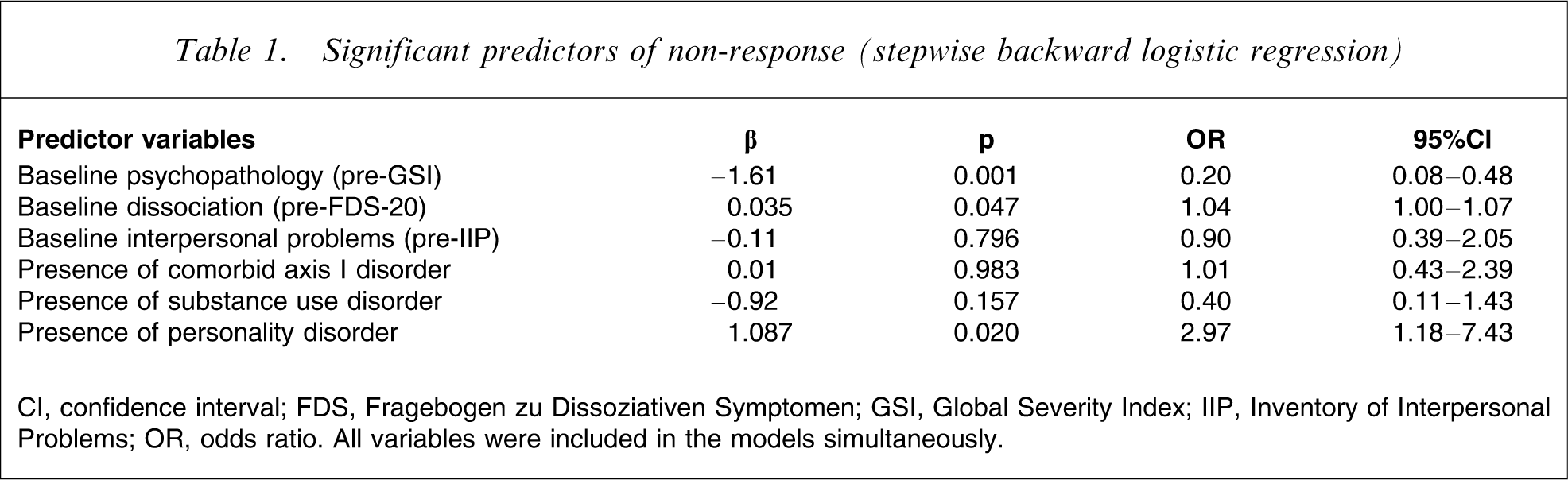
CI, confidence interval; FDS, Fragebogen zu Dissoziativen Symptomen; GSI, Global Severity Index; IIP, Inventory of Interpersonal Problems; OR, odds ratio. All variables were included in the models simultaneously.
As shown in Table 2, using the difference (Δ-GSI) between the pre- and post-treatment GSI as dimensional outcome parameter yielded similar results: high levels of baseline psychopathological distress and few dissociative symptoms were predictive of greater change in GSI scores, indicating that dissociation has a negative impact on symptomatological improvement. All other variables including personality disorder comorbidity did not significantly contribute to the prediction of change in psychopathological distress.
Significant predictors of change in psychopathology (Δ-GSI; linear regression)
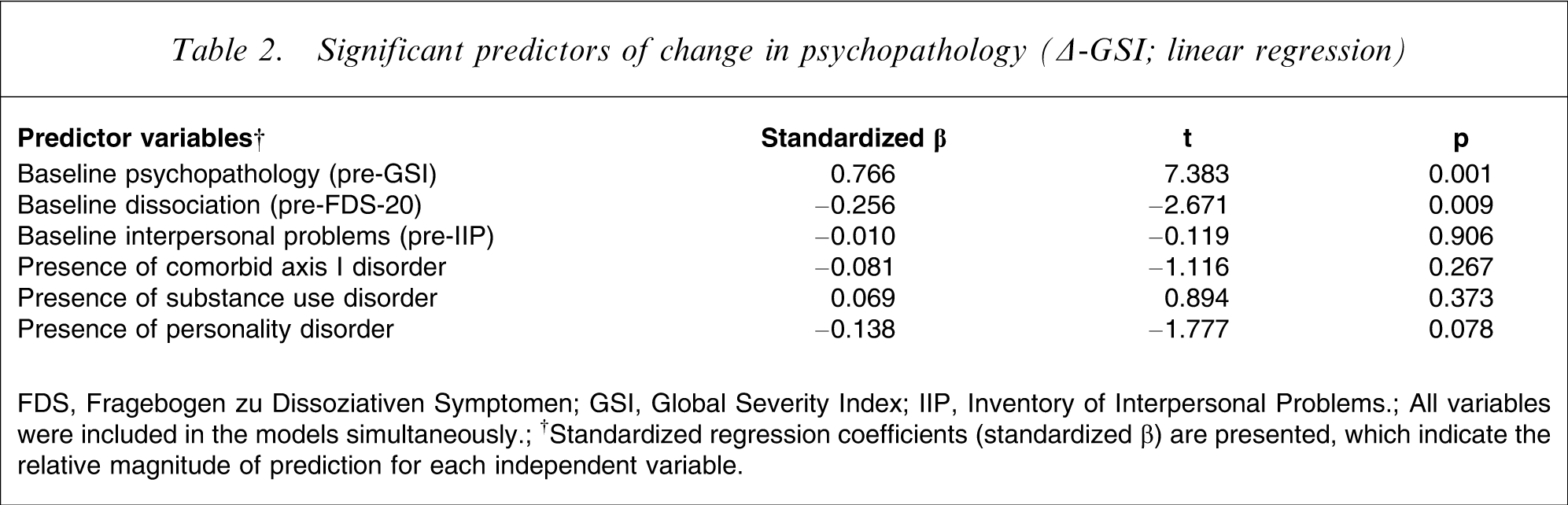
FDS, Fragebogen zu Dissoziativen Symptomen; GSI, Global Severity Index; IIP, Inventory of Interpersonal Problems.
All variables were included in the models simultaneously.
†Standardized regression coefficients (standardized β) are presented, which indicate the relative magnitude of prediction for each independent variable.
Discussion
Our findings replicate and extend previous research indicating that dissociation has a negative impact on treatment outcome, even after controlling for comorbid axis I and II disorders and interpersonal problems. While earlier studies were limited to panic disorder with agoraphobia [14] or OCD [15], our results suggest that dissociative symptoms influence therapy response in a wide variety of non-psychotic mental disorders, affective disorders in particular, which affected 68% of the present inpatient sample. Furthermore, our findings show that the association between higher baseline dissociation and poorer symptom-related treatment outcome is not only of relevance in studies using CBT [14, 15], but also in studies with a psychodynamic approach.
While Michelson et al. found that dissociative amnesia was particularly associated with chief complaints (i.e. agoraphobia in this case) [14], Rufer et al. reported absorption and imaginative involvement as one dimension of dissociation to be predictive of non-response [15]. However, although numerous studies have used the three factor-analytically derived subscales of the DES (amnesia, absorption and depersonalization), it should be kept in mind that the empirical evidence in favour of a 3-D model is lacking; instead only one general factor underlies all of the items of the DES [28, 31]. Correspondingly, the short version of the DES used in the present study measures dissociation as uni-dimensional construct [26].
Although the question about the factorial structure of the DES is important, from a clinical perspective it seems even more essential to consider how dissociative symptoms may interfere with treatment response. With respect to CBT it was argued that individuals prone to dissociate do so as a response to negative psychophysiological states (e.g. tension or anxiety) occurring before and during exposure therapy. Thus, reality testing, regulation of emotional arousal and habituation may be impaired, leading to less favourable outcomes in these patients [14, 15]. However, in the light of the present findings we suggest that these assumptions do not only apply to specific CBT techniques (e.g. exposure), but can be extended to a variety of psychotherapeutic interventions including psychodynamic ones as in the present study. Because psychotherapy in general is not painless and often mobilizes intense emotions such as fear, helplessness and shame, calling into question the individual's psychological integrity as a starting point for changes in behaviour, cognition and affectivity, it is likely that subjects who respond to these emotions with detachment from themselves and their environment (i.e. dissociation) do not profit as much as those who do not.
In addition to this direct link there might also be an indirect pathway with regard to how dissociation interferes with treatment response. Given the growing evidence for a relationship between dissociative phenomena and interpersonal trauma, particularly childhood maltreatment including sexual and physical abuse, neglect and parental dysfunction [32–35], it is not surprising that increased levels of dissociation have been associated with an insecure, especially disorganized attachment pattern [36, 37], which in turn negatively affects the therapeutic relationship [16, 38]. Although we did not find interpersonal problems (as measured by the IIP) to influence outcome, this does not invalidate our consideration about an association between dissociation, attachment style and treatment response, because the severity of interpersonal difficulties is not necessarily related to the attachment pattern. From the clinical point of view dissociation might not only point to relational trauma, but may also indicate poor quality of object relationships.
In closing, a note of caution is necessary due to some methodological issues. First, because the diagnoses were based on standard clinical interviews and not corroborated by structured interviews, we may have missed some comorbid disorders, particularly personality disorders, which are an important predictor of treatment outcome [16]. Second, both the present investigation and previous research [14, 15] included patients undergoing short-term psychotherapy. Thus, it remains unresolved as to whether consistent findings across these studies (i.e. baseline dissociation has a negative impact on treatment response) also apply to long-term psychotherapy, particularly because outcome predictors in long-term treatment were found to differ from those in short-term therapy [39]. Finally, we exclusively focused on psychopathology as a main outcome criterion. However, it might useful to include further outcome measures such as global functioning, social adjustment and interpersonal problems as well as global improvement and chief complaints [39, 40].
Notwithstanding these caveats our findings that are consistent with previous studies [14, 15] hold important implications for both daily practice and research. Considering that dissociation may impede treatment response, all patients should routinely be screened for dissociative symptoms at the beginning of the therapeutic process. In case patients turn out to be highly dissociative, it might be helpful to adjust treatment strategies, for example strengthen patients’ ability to deal with intense emotions other than dissociating. Furthermore, dissociation often indicates a history of interpersonal trauma resulting in disturbed attachment, which in turn is likely to influence the therapeutic relationship. We are in need of further research to determine whether or not a dissociation-adapted therapeutic procedure is beneficial for dissociative patients with non-psychotic mental disorders. Finally, future studies on therapy outcome and its predictors, as well as those on treatment resistance in different settings and disorders, should be aware of dissociation as one possibly important factor directly and indirectly influencing the therapeutic process.