
Abstract
Purpose: The matching of prosthetic devices to the needs of the individual is a challenge for providers and patients. The aims of this study are to explore the values and preferences that prosthetic users have of their prosthetic devices; to investigate users' perceptions of alternative prosthetic options and to demonstrate a novel method for exploring the values and preferences of prosthetic users.
Methods: This study describes four case studies of upper limb and lower limb high tech and conventional prosthetic users. Participants were interviewed using the repertory grid technique (RGT), a qualitative technique to explore individual values and preferences regarding specific choices and events.
Results: The participants generated distinctive patterns of personal constructs and ratings regarding prosthetic use and different prosthetic options available. The RGT produced a unique profile of preferences regarding prosthetic technologies for each participant.
Conclusions: User choice is an important factor when matching prosthetic technology to the user. The consumer's values regarding different prosthetic options are likely to be a critical factor in prosthetic acceptance and ultimate quality of life. The RGT offers a structured method of exploring these attitudes and values without imposing researcher or practitioner bias and identifies personalized dimensions for providers and users to evaluate the individuals' preferences in prosthetic technology.
Introduction
Prosthesis non-use rates are estimated to be about 20% with upper limb devices1 and 15% with lower limb devices.2 In order to address these considerable rates of non-use, it is essential to understand the predictors of non-use of prosthetics and to ascertain what users require from prosthetic devices. According to Scherer,3 a good match between person and technology is achieved if the prosthetic device meets the user's performance expectations and is easy and comfortable to use. It has also been recommended that when selecting a prosthesis for an individual, attention should be directed at the specific needs of the individual,4 that prosthetic users are provided with a choice of available options,3 and are involved in prosthesis selection.5,6
While a number of factors including equipment, functional utility, and individual variables such as motivation have been associated with non-use,7-9 there has been a growing recognition within the assistive technology literature of the importance of consumer preferences and values in understanding non-use.3 For one individual a given prosthesis may represent a restoration of independence and embody ability. However, for another person the same prosthesis may represent their loss and embody disability,10 or may hide disability to prevent social stigma and promote social integration.11 Therefore, in order to successfully integrate devices into the user's life, the individual values, preferences and meanings assigned to the device need to be explored.12 Therefore it is essential to develop methodological approaches to elicit and assess these meanings. Approaches such as the Patient Generated Index13 and Goal Attainment Scaling14 have been used to assess the individual preferences, values and meanings of prosthesis users in prosthetic rehabilitation. Although these individualized assessment approaches have the advantage of consulting the consumer to determine which dimensions are most important to them for evaluation in rehabilitation, they have not been used to determine preferences of alternative prosthetic options amongst users.
This individualized approach is reflected in the basic theoretical assumptions of Personal Construct psychology (PCP) which states that a situation may be viewed differently by different people, or even differently by the same person at another time, as there are always alternative constructs available to choose from.15 A personal construct is considered an individualized way that the person has of viewing, giving meaning to, or construing, the elements in their environment.16 Elements can consist of individuals, institutions, ideas, roles, activities and objects in the individual's experience,17 Kelly15 argued that in order to understand someone, we must do so in their own terms; which means identifying their personal constructs, otherwise we run the risk of simply projecting our own thinking on to them.16
The method used to elicit an individual's personal construct in relation to a predefined topic is the repertory grid technique (RGT). The RGT is an individualized measure to identify and explore the distinctive constructs an individual uses to value and assess specific aspects of their life.18 The RGT has been shown to be a useful tool within the health sector to evaluate treatment preferences19,20 and services,21 to understand patients' perspectives22 and to aid in medical decision-making.19,23 These findings suggest that techniques grounded in the RGT may be useful in situations where there is little medical basis for choosing amongst a variety of procedures allowing input of patient values into the treatment decision.
The aims of the present study are to explore the values and preferences that prosthetic users have of their prosthetic devices; to investigate how the user views alternative prosthetic options and to demonstrate a novel, idiographic method for exploring these values and preferences.
Method
Participants
The participants in this study consisted of two individuals fitted with an upper limb prosthetic, and two individuals fitted with a lower limb prosthetic. All participants were over 18 years of age and had a fluent understanding of English. Ethical approval for this research was sought and obtained from the IRB at Johns Hopkins Hospital Baltimore, MD.
Procedure
After each participant had given informed consent, and filled out a demographic questionnaire, the participant completed the repertory grid. As the focus of the study was to elicit the values and preferences of users of prostheses, the elements were predetermined by the research team. Each participant was given a list of prosthetic options and self-referring items (e.g., Ideal Self) to ensure that potential prosthetic options and rehabilitation-relevant aspects of self-perception were rated (See Figure 1). These elements were chosen by professionals working in prosthetic rehabilitation and were based on a pilot study.22 These elements were modified to suit the type of amputation (e.g., High Tech prosthetic arm became High tech prosthetic leg). Not all prosthetic options chosen were available to each user due to financial, physical or technological reasons. These options were still included to gain further insight into how they were perceived.
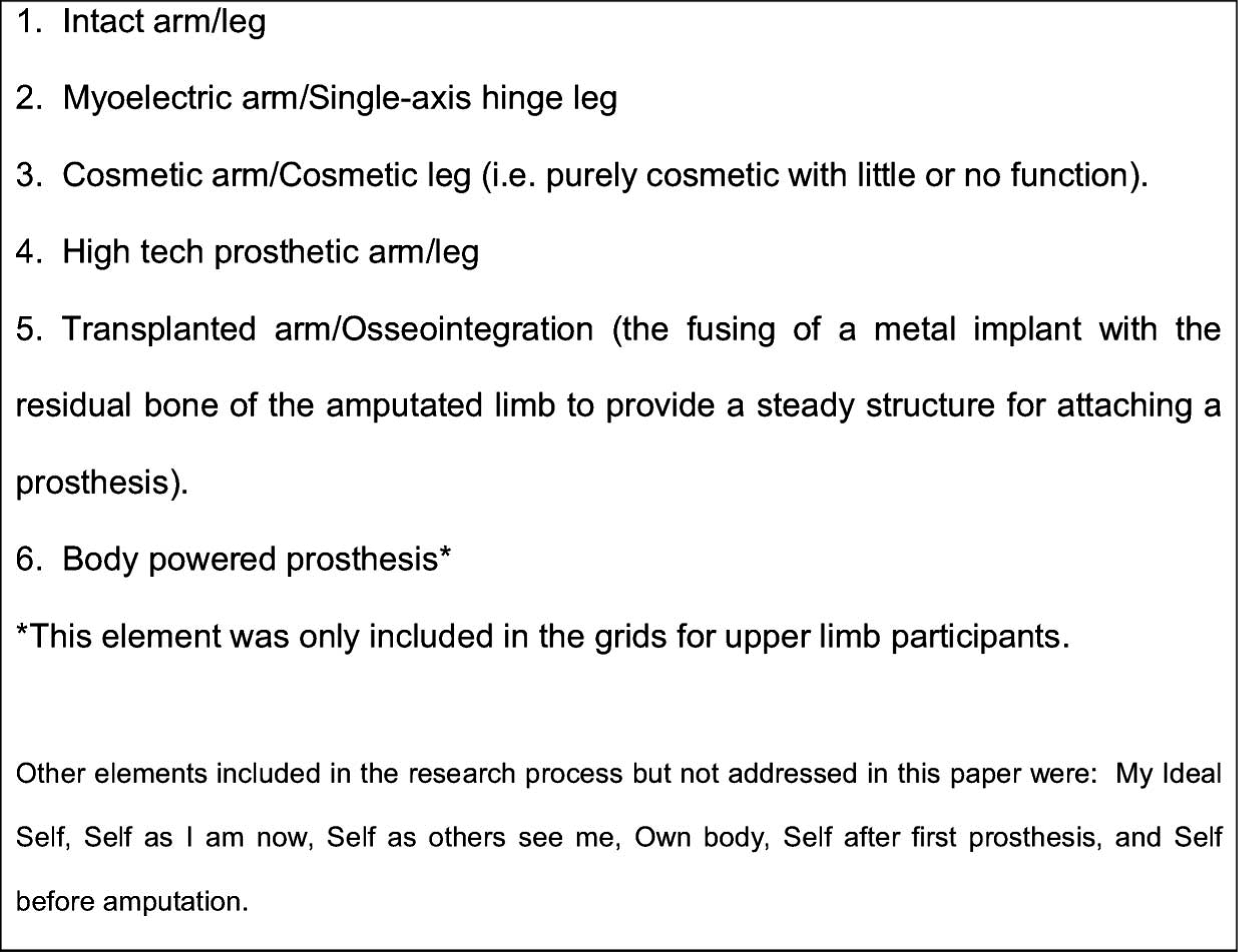
List of elements.
For this particular study, constructs were elicited using the ‘Contrast Method’ of triadic elicitation.24 Triadic elicitation is the procedure used in all RGT studies to generate constructs on which to rate elements. Elements from the list (Figure 1) were grouped together into 12 randomly generated sets consisting of three different elements. Participants were presented with each set of three elements one at a time, and asked to identify ‘how any two of these elements are alike’ in some way. The characterization created by the participant (e.g., ‘functional’) formed one pole of the construct and was written in on the left-hand side of the grid. This process continued until twelve characterizations had been obtained. Participants were then asked to provide a contrast for each of the 12 characterizations identified. These phrases were written on the right hand side of the grid, opposite the original phrase created, creating a completed construct. In the final phase, participants were asked to rate each of the elements along each of the constructs in a stepwise fashion, using a 10-point rating scale (1–10). Participants were told the phrase on the left of the grid stands for ‘1’ end of the scale and the phrase on the right of the grid for ‘10’. Once completed, the interviewer discussed with the participant the ratings on the grid as well as the constructs created to clarifying their meanings. During this process it was ascertained which end of the construct was considered positive and which end was considered negative. A number of constructs were reverse scored so that a positive and negative end of the grid could be established for ease of analysis, meaning that 1 is considered positive, and 10 considered negative. The whole of the interview process including the construction of the grid was audio-recorded and transcribed. For a more detailed description of the RGT method used, see Neimeyer et al. (2005) or contact the corresponding author of this paper.
Analysis
Analysis of the repertory grid allows the opportunity to examine each participant's view of the available prosthetic options, based on the constructs they chose and the ratings given to each prosthetic option in relation to the chosen constructs. The analysis is idiographic in nature and as such involves looking at each rating and construct individually in relation to the participant.
Results
Case study 1 – John
The first participant, John (pseudonym) was an elderly gentleman, with a right transfemoral amputation that occurred following complications of knee surgery. It has been over four years since his amputation and he has had his current prosthesis, an Otto Bock C-Leg® for just over three years. Previous to the C-Leg® he used a hinge-leg with a locked knee. He wears the C-Leg® everyday at an average of nine hours each day. He uses two canes as mobility aids. He would not be considered a typical C-Leg® user due to his age. John's grid is detailed in Table I.
John's grid.
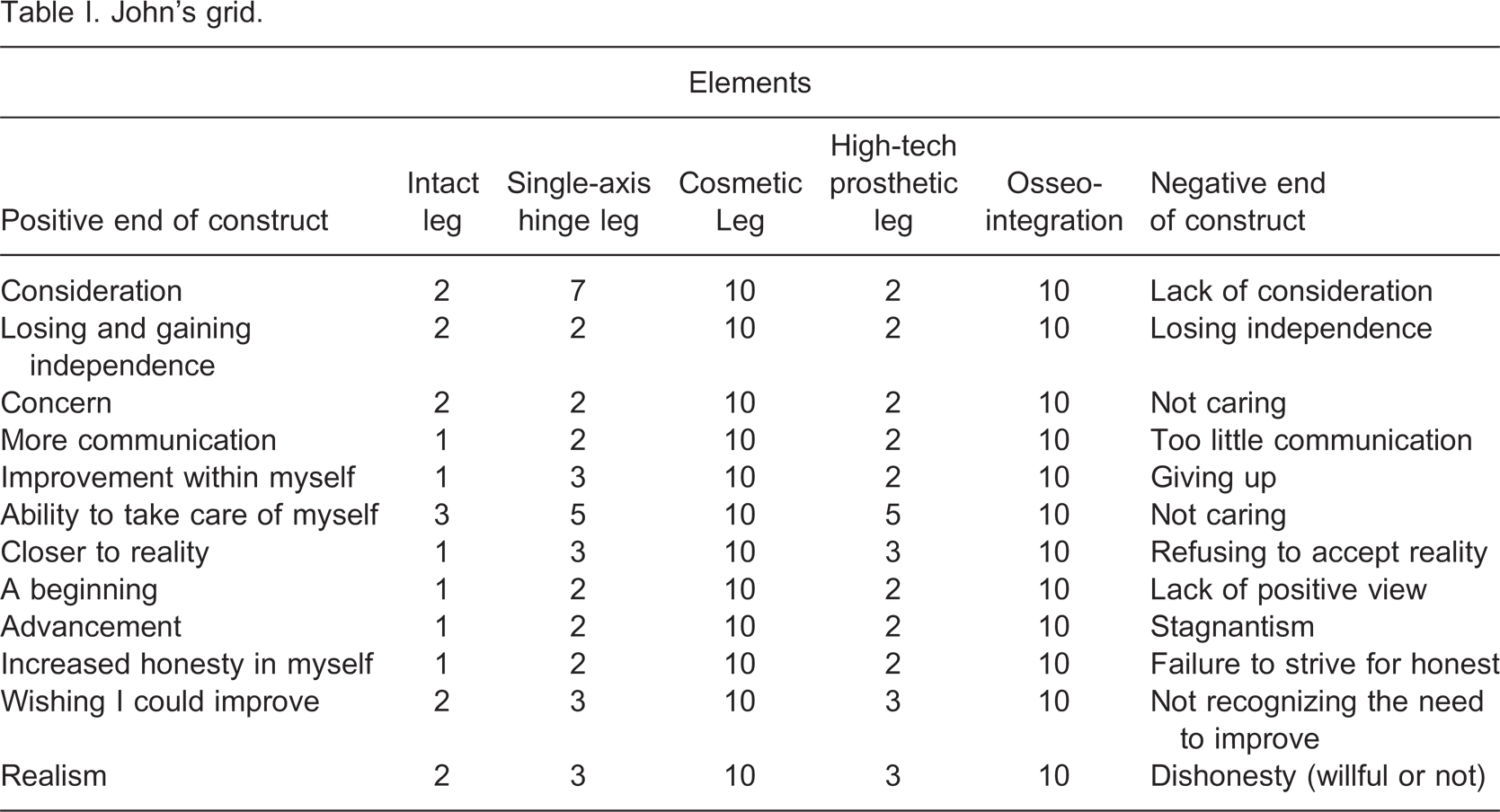
Examination of John's grid shows that he viewed his intact leg positively. The ratings of his intact leg provided a baseline comparison for his view of alternative prosthetic options. John had a negative attitude toward cosmetic limbs as evidenced by his ratings of 10 on each of the constructs for this prosthetic option. Similarly, his view of osseointegration is also very negative on all constructs. He viewed his current high tech limb only slightly more positively on average than his previous single axis hinge leg.
Case study 2 – Phil
Phil (pseudonym) was a middle-aged gentleman with bilateral transtibial amputations and a history of diabetes and peripheral vascular disease (PVD). He originally had a unilateral amputation. Subsequently he had a series of amputations with a higher level each time culminating five years ago in a second transtibial amputation. The prostheses that he currently uses are five years old (though he has newer prostheses which he does not wear). His prostheses have nylon sockets and SACH feet which he wears everyday for about 10 hours. He was fitted with a more cosmetic and less functional limb after his first amputation, but since then has been fitted with similar models to the type he currently wears. He uses a scooter mobility aid but is able to walk short distances. Table II shows his grid. It should be noted that as a below knee amputee, certain prosthetic options (the C-Leg® prosthesis nor the single-axis hinge) are not currently applicable to him but were included for further insights into how these options are perceived.
Phil's grid.
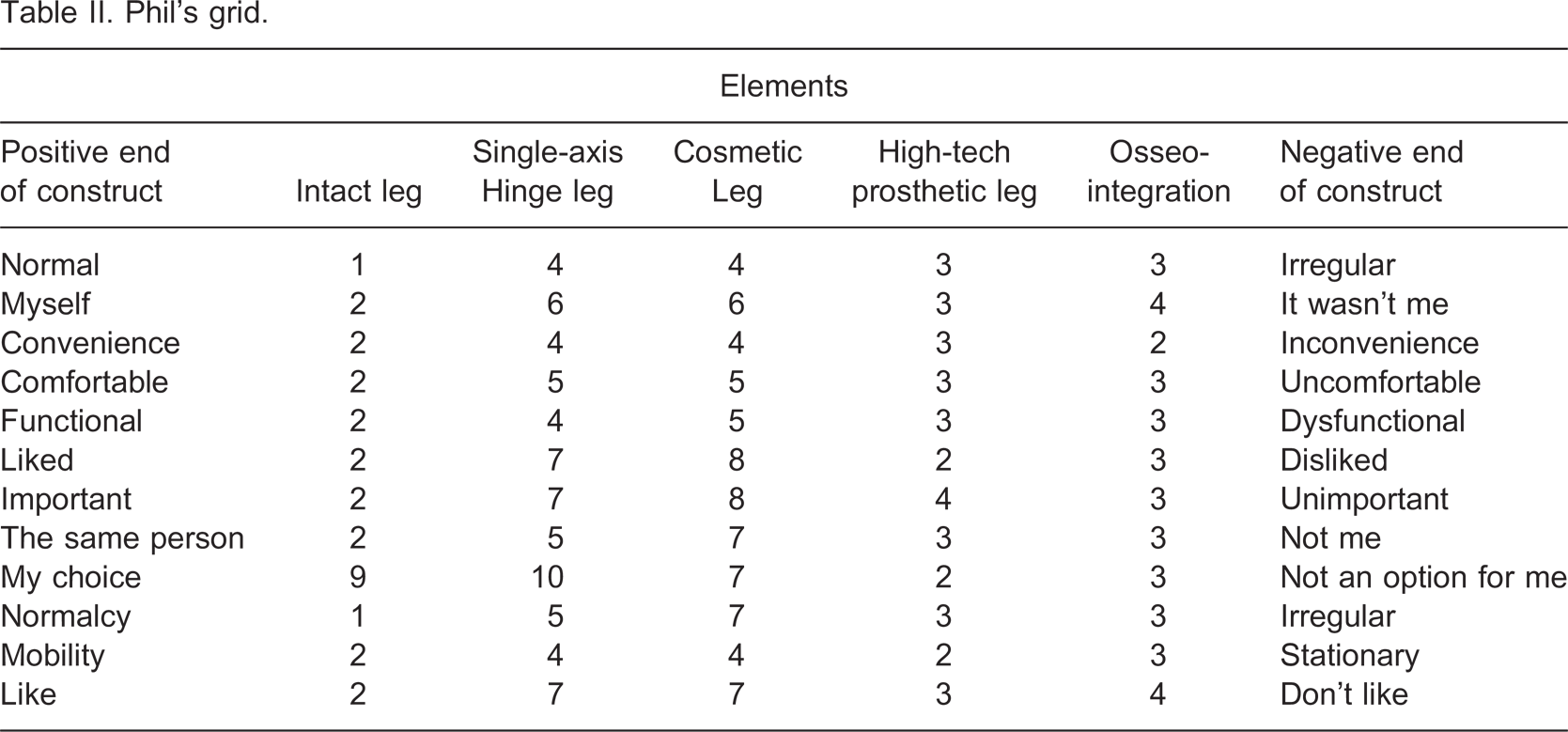
Phil rated his previously intact leg positively. The only negative score referred to it as being considered not an option for him. Phil viewed cosmetic limbs as his least desirable prosthetic option, rating it high in terms of ‘dislike’ and ‘unimportant’. Similarly, Phil did not view the single axis hinge leg favourably, rating it as ‘not an option’ for him, and also rating it negatively in terms of dislike, and unimportance. Phil rated osseointegration as his second most favourable prosthetic option behind a high tech prosthetic limb. Phil's most favourable ratings for osseointegration, referred to this being a potentially ‘convenient’, ‘comfortable’, ‘functional’ option. Despite a high tech leg requiring a higher amputation, Phil chose this as his most desirable prosthetic option, rating it highly on most constructs. Phil considered it slightly more favourably on selected constructs compared to his second favourite option, osseointegration.
Case study 3 – Jennifer
The third participant was a young woman, Jennifer (pseudonym), who had an amputation at the transhumeral neck. She received a conventional myo-electric prosthesis to use after her amputation. However, she found it difficult to operate, and eventually ceased using the prosthesis. Jennifer underwent Targeted Muscle Reinervation (TMR) surgery to improve prosthetic function and ease of use. Jennifer used a prosthesis that uses the additional TMR sites. It had been three years since her amputation and she had her current prosthesis for one year. She reported using her prosthesis approximately four days in the week and for about four hours of those days. Jennifer's grid can be seen in Table III.
Jennifer's grid.
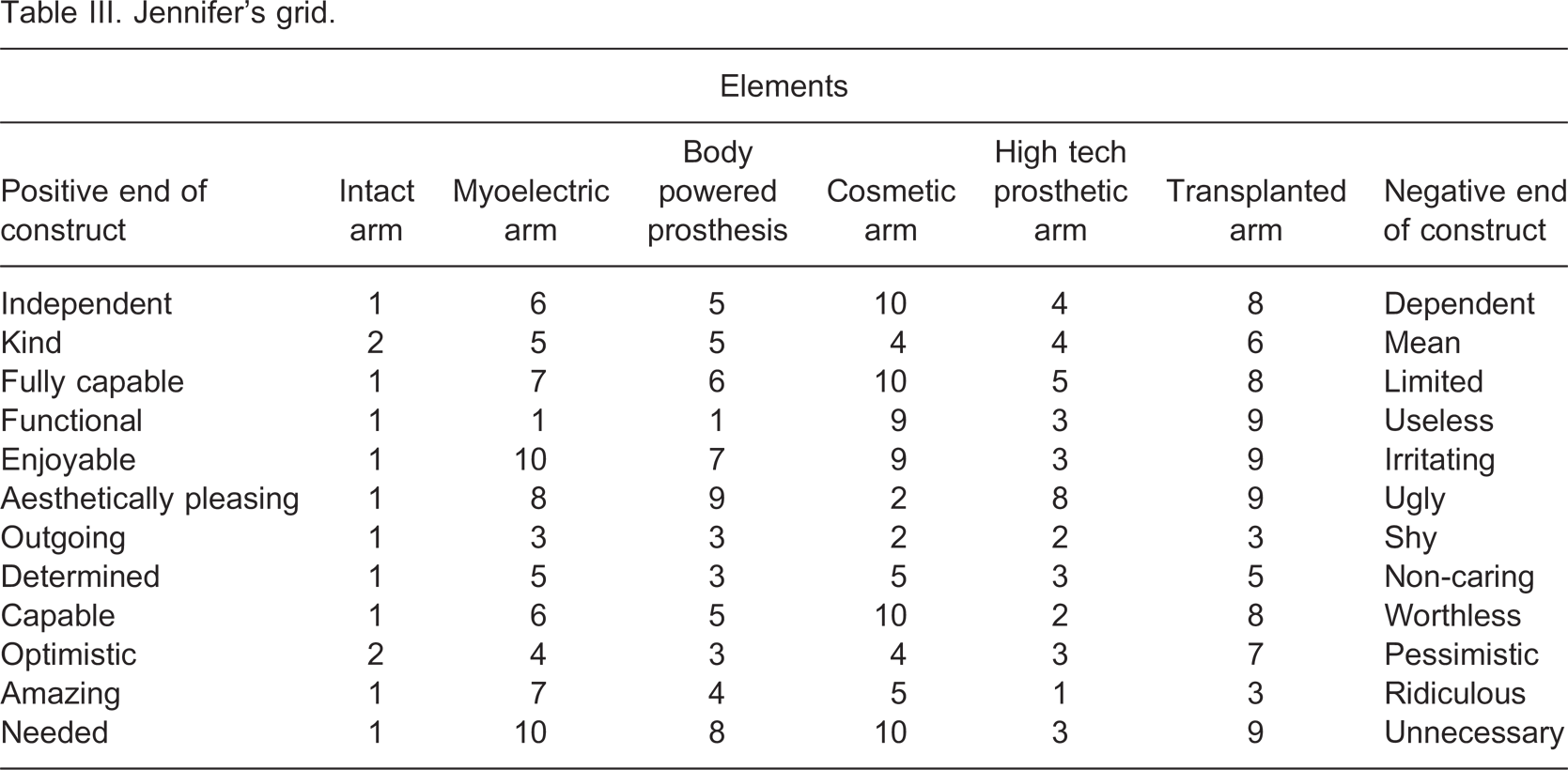
Jennifer rated her intact arm more positively than the prosthetic options. Jennifer considered the transplanted arm to be the most negative of all the prosthetic options, largely due to functionality being the most important construct in assessing prosthetic options for her and her anticipation that the transplanted arm would have poor functionality. While Jennifer rates cosmetic limbs as aesthetically appealing, her overall ratings of cosmetic arm are low reflecting her high value on functional performance. Overall, a myo-electric arm was not rated very favourably by Jennifer compared to her positive ratings of the high tech prosthetic arm and body powered prosthesis. While it received favourable scores on functionality, she also rated it as ‘irritating’ due to the height of her amputation, which made it difficult for her to use.
Jennifer rated body powered prostheses favourably, because of her awareness of their functionality and robustness but she also rated them as aesthetically less appealing than a high tech prosthetic. Jennifer is particularly positive about the functionality of a high tech prosthesis. In aesthetic terms she feels that her high tech arm looks like a robot arm, but this aspect of prostheses emerged as unimportant through the interview.
Case study 4 – Declan
The fourth participant, Declan (pseudonym) was a middle-aged gentleman who had congenital transradial limb loss and used a conventional body-powered prosthesis. The first limb he used as a child was also a body-powered prosthesis, but had limited function and had a leather glove covering. Declan reported wearing his prosthesis seven days per week and 18 hours per day. Declan's grid can be seen in Table IV.
Declan's grid.
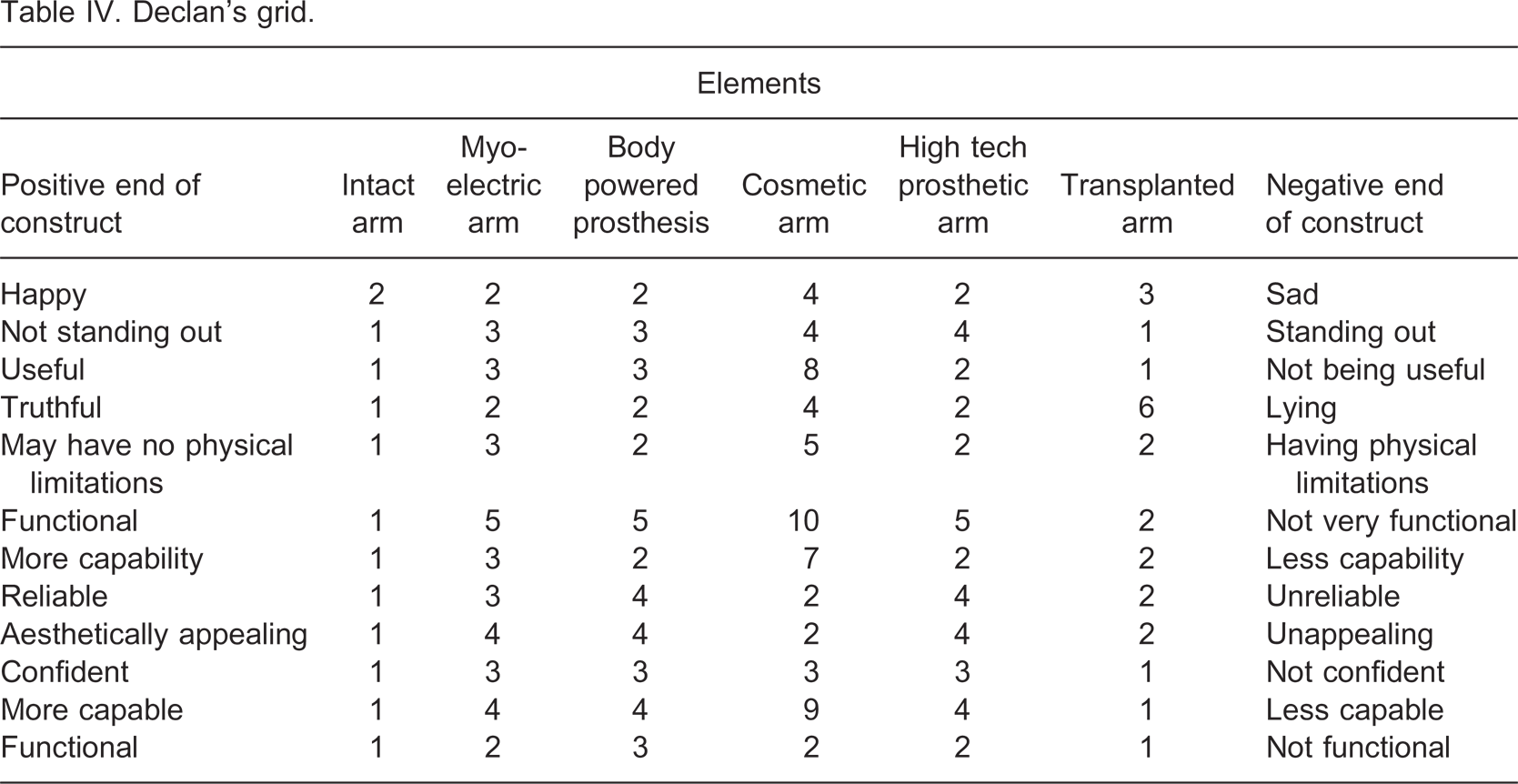
Declan rated his intact arm positively. A cosmetic arm is considered the least useful prosthetic option as cosmesis is an unimportant value for Declan. The cosmetic arm is also seen as the most physically limiting, least functional and least capable option. However, it is rated as the most reliable prosthetic option, explaining as “since it doesn't do anything, it cannot let me down”. Overall, Declan viewed his current body-powered prosthesis, a myo-electric arm and a high tech arm quite favourably. The important differentiating constructs for Declan were functionality and ‘not standing out’, with ‘functional’ even appearing twice in his grid.
Discussion
The aims of this study were to explore the values and preferences of prosthetic users towards different prosthetic options; to investigate users' perceptions of alternative prosthetic options and to demonstrate a novel method for exploring the values and preferences of prosthetic users. The results showed that a number of different features are important to individual prosthetic users when selecting a prosthetic option. While numerous papers suggest that individuals may vary in their prosthetic preferences, this series of case studies using a standardized assessment process provides evidence to support this notion. Furthermore, these results suggest that the factors individuals use to evaluate a prosthetic option can be highly individualized, and that different prosthetic options are not held in the same regard among different prosthetic users.
The findings of this study indicate that the accepted norms of what prosthetic users want from a prosthesis do not apply uniformly to all individuals from the same demographic, emphasising the individuality of prosthetic users needs. Furthermore, the preference and choice of prostheses may not reflect what providers see as the most up-to-date and cutting edge available. Even when the most high-tech prosthetic option is offered, there is no guarantee of satisfaction for the user, highlighting the need for personal choice and involvement for the user in the fitting stages of the prosthesis. These findings suggest that the rapid increases in the functionality of the technology available to prosthetic users have not always taken into account the feelings and emotions individuals attach to devices, and that some technological advances may not be appreciated by the very people that use the technology.
All participants, while adapting well to their amputation, were not completely satisfied with the prosthetic options prescribed, and some did not have much involvement in their choice of prosthetic. These cases support the growing concern over the lack of attention to patient preferences in prescription of prosthetic limbs and other devices. As Scherer notes, ‘It is no longer acceptable to point to technological solutions before the prospective user's goals are fully defined. A particular technology should never become the place to start; the needs, desires and goals of the user should be the beginning point.’3 (p 3).
This study highlights the need to move away from the path of thinking of patients in general, but specifically prosthetic users, as merely passive recipients of healthcare and rehabilitation. They need to be thought of as consumers who have preferences and expectations of the product or device they wish to use. Even when choice of components is slim for users due to financial constraints, it is important that choice is offered when possible and recognized as an important factor in optimizing use rates. Discovering the values and preferences of the patient and assessing them early in the treatment process is increasingly recognized as an important factor in the delivery of healthcare.25 In particular, client participation and client-centred focus are central features in the International Classification of Functioning, Disability and Health (ICF),26 and are highlighted in the widely accepted Matching Person and Technology (MPT) model used for prescribing assistive technology.3 Sullivan states that ‘facts known only by physicians need to be supplemented by values known only by patients’,27 and many studies emphasize the need to involve prosthetic users in device selection due to its association with improving rates of use and preventing abandonment.3,5,6
There are currently no clinical measures available to measure patient preferences within the prosthetic prescription setting. However models such at the Matching Person and Technology model3 offer helpful guidelines for garnering patient preferences and opinions, and measures such as the Patient Generated Index (PGI) and Goal-Attainment Scaling (GAS) are rehabilitation tools that cater to individual preferences when generating achievable goals for patients. A number of different quality of life measures also use individual patient preferences (SEIQOL,28 SF-6D29) so that areas that are important to the individual are considered when measuring and subsequently optimising quality of life. The success of these measures in improving patients' satisfaction further indicates the need to include the patient within healthcare.
The RGT process created individually meaningful scales for each person to rate the different prosthetic options. By rating the technology on these scales, we are essentially rating the technology under headings that are personally important to the prosthetic user. The unique perspective of each completed repertory grid provided a number of headings for rating prosthetics that may not have been identified using conventional questionnaire or interview techniques, and were exclusive to each individual. The RGT indicates what an individual's preferences are with technology by offering ratings on different prosthetic options, while also showing why and how they have arrived at these preferences.
It is important to acknowledge the limitations of this study. Selection bias is a potential threat as participants were volunteers selected by convenience. As in other qualitative research, the study investigators may influence the observations drawn from the data. Thus other investigators may draw additional or different conclusions from the data. However, by elucidating the data collected on the grid with each participant as part of the RGT process, there was little scope to misinterpret the data. It is also appreciated that due to the time constraints in clinical practice, a modified RGT would be more suitable for use within prosthetic prescription. Consequently, this study recommends a standardized method be created for clinical use which uses a similar philosophy.
This paper adds weight to the evidence that patient preferences need to be considered when prescribing prosthetic technology. Given that there are currently no standardised methods in which to measure patient preferences within the prosthetic prescription setting, this study recommends further research in this area to aid the necessary change in practice. Including individuals' choices and opinions within the prescription process will increase patient satisfaction and decrease the likelihood of prosthetic abandonment.
Footnotes
Acknowledgements
This research has been funded by the Health Research Board in Ireland.