
Abstract
Rotationplasty is established as a functionally improving and partially ablative method of tumour surgery, but good clinical and functional results do not only depend on a successful surgery. Due to the changed biomechanical situation the activity level is limited by the weight bearing capacity of the rotated foot. Painful blisters and callosities may limit the use of the exo-prosthesis, because the skin is overstressed in the soft socket. A 28-year-old patient with a rotationplasty type A2 suffered from painful callosities of the rotated foot. Capacitive pressure measurements were performed as well as a gait analysis for kinematics and kinetic characteristics. Clinically a decrease of the callosities and a pain relieve was obvious and the patient learned skiing without prior knowledge. Biomechanically a decrease of the peak pressure (from 240.6–135.0 kPa) and the mean pressure (from 83.2–66.2 kPa), was observed with an increased weight bearing area. The study has shown that a modification of the heel bench can considerably improve pressure distribution. An increase of the load bearing area appears to enable the skin to compensate even intensive strain during athletic activities.
Introduction
In recent years rotationplasty has been established as a functionally improving and partially ablative method of tumour surgery. Good clinical and functional results, however, do not only depend on a successful surgery but also on prosthetic design.1-4 Follow-up examinations over a period of 15 years revealed that, with adequate prosthetic design, bones and joints are able to adjust to angled weight distribution axis.5,6 However, activity limiting calluses are observed especially regarding athletically active patients due to local pressures inside the prosthesis. The activity level is, thus, limited primarily by the pain due to the overloaded weight bearing cutaneus capacity of the rotated foot. The aim of the following study was to evaluate the clinical outcome, compressive stress on the foot and peak load inside two different prosthetic designs. The study was conducted on a free walking patient seven years after rotationplasty.
Design and methods
A 28-year-old female with a rotationplasty type A2 (according to Winkelmann)4 suffered from painful calluses on the weight bearing areas of the foot. Capacitive pressure measuring insoles (PEDAR, Novel GmbH, Munich, Germany) were used for the determination of plantar and dorsal loading on the foot (Figure 1). The insoles were worn inside the prosthetic socket during walking at self-selected speed with two different types of prostheses and ‘soft sockets'. The kinematical and kinetic characteristics of the patient's gait were investigated through gait analyses. Additionally, a medical interview was conducted concerning the patient's maximum walking distance (pain-free walking distance), as well as possible limitations (pain quantified with VAS7,8) in personal and professional life. The clinical examination included a full photographic record of changes in the foot's skin surface and a record of the joint's range of movement. The movement measurements were conducted according to the neutral-null-method. One year after modifying the prosthesis and the Soft Socket, the examinations were repeated. In both cases the same orthopaedic surgeon conducted the examinations.
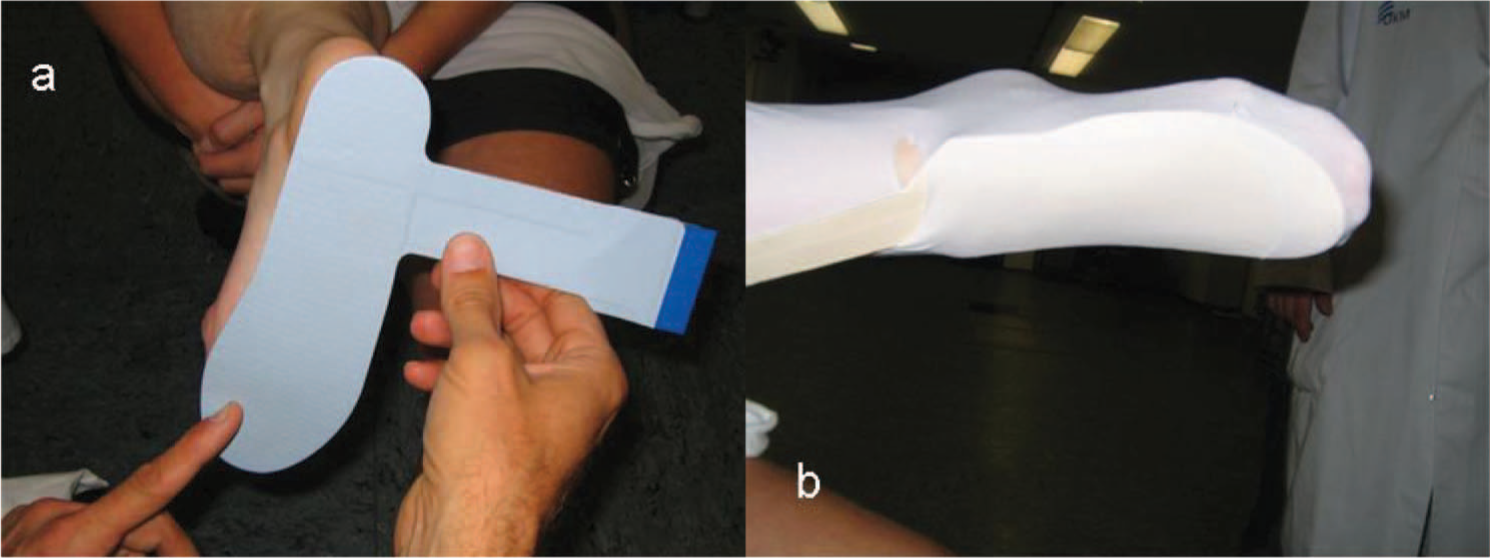
Capacitive pressure measuring insoles (a: plantar; b: dorsal).
The Research Ethics Board of the University of Muenster deems the application for and issue of an Ethics approval not necessary, because it is about an anonymized case report on the individual treatment of a patient. Participant provided her informed consents.
Manufacturing of the new Soft Socket
For the new prosthesis, a mold was taken with a plaster cast, starting with the foot. Axial forces with rotationplasty are almost exclusively absorbed by the foot. Previous studies5 have shown that over a period of time after rotationplasty neither osteoarthritis nor any other osseous and clinically relevant alterations develop. However, especially athletically active patients experienced partially painful problems with soft tissue, such as callosities and blisters. It was the purpose of the new shaft design to enlarge the load bearing areas and therefore reduce the pressure peaks.
The major part of the load is now absorbed by the heel bench and the heel clamp joined with the counter support by the dorsum of the foot (Figure 2). The stirrup-like modelled heel clamp has been incorporated medially and laterally alongside the longitudinal bulge, thus preventing a removal of the heel in dorsal flexion and the resulting incongruity between the mechanical and the anatomical centre of rotation.
During the second phase of the plaster cast the heel casing, which covers the heel and the malleolus completely, was modified to prevent the heel from slipping out of the prosthesis. At last the lower and proximal upper tibia was wrapped, while maintaining a wide medial and lateral load bearing area. The extremity was included proximally to prevent bulging and to absorb part of the sagittal pressure proximal to the foot.
The rather complex plaster cast made the actual modelling of the prosthesis far easier. The positive of the foot was flattened and, mainly at the dorsum of the foot, reduced to its accurate measures. In order to avoid a later irritation of the nail bed, the toe space was extended, the supporting and stabilizing areas modified and reduced to a size according to the measurements of the patient.
Design of the shaft
The design of the Soft Socket is primarily focused on preventing a dorsal slipping of the foot. Besides the previously described methods and in contrast to already existing prosthetic designs, rather soft material was used for the modelling of the toe gripping bead.
Prominent bony features and part of the dorsum of the foot were padded with 2 mm PPT-pads (Schein KG, D-42897 Remscheid). Because the distance between the medial malleolus and the lateral malleolus is enlarged in dorsiflexion by the ventrally expanding trochlea of talus, 4 mm pads were used for the malleoli. A double layer of reinforcement material (Tepp 2/Fritz Minke GmbH&CoKG; D-47051 Duisburg) ensured the hardening of the Soft Socket. To prevent the material from ripping in particularly heavily loaded areas, these areas were additionally reinforced by Drellstreifen (Bandana-Drell/Thämert Orthopädische Hilfsmittel GmbH&CoKG/D-30938 Burgwedel/Großburgwedel). The form was adjusted with Pedilin (Otto Bock HealthCare GmbH/ D-37115 Duderstadt) to ease the sliding into and out of the shaft (Figure 3).
Once these measurements are taken, the Soft Socket is prepared for the dousing with carbon acrylic cast resin. The upper shaft must be long enough to enclose the scars, thus enabling a smooth transition from the upper to the lower leg. The mediolateral supporting areas must be able to stabilize the ankle joint laterally. It is advisable to leave some supramalleolar space alongside the tibia and fibula for an easier access into and out of the shaft.
The further design of the shaft followed standard procedures, whereas the axis of the joint was determined using clinical joint samples. Before the dynamic fitting, the static structure was controlled and optimized for the patient.
Results
At both measurements, the free-movement of the joints on the operated extremity was neither actively nor passively limited. The gait analysis showed that the stance and swing phases of walking, individual gait pattern, and walking speed improved increasingly while using the experimental prosthesis for one year.
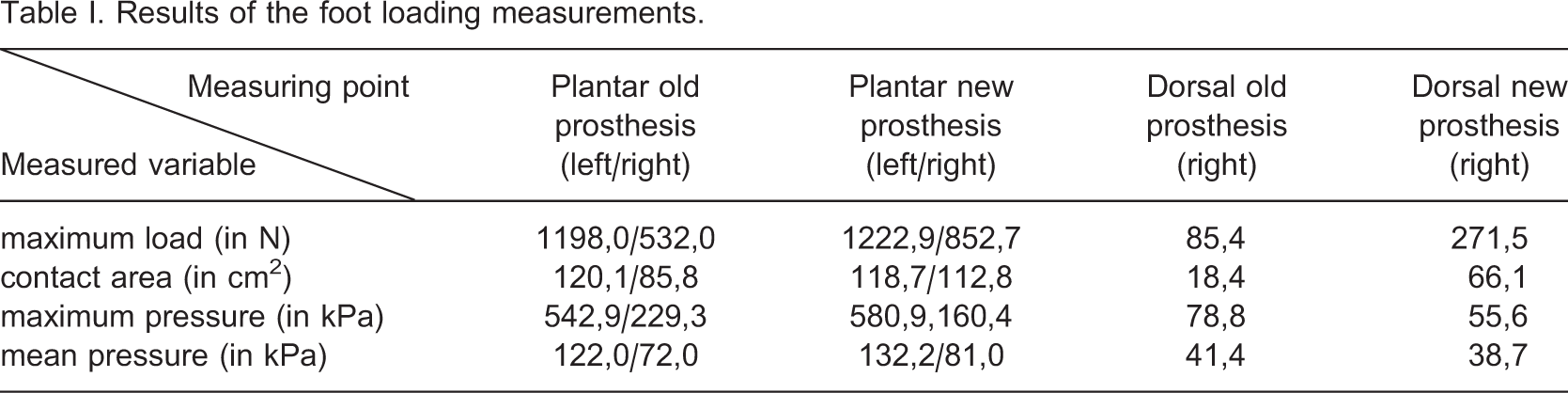
Foot loading measurements showed a remarkable reduction in maximum pressure and a simultaneously increased contact area (see Table I and Figures 3 and 4). The peak pressure decreased from 240.6 to 135.0 kPa, the mean pressure decreased from 83.2–66.2 kPa, while the weight bearing area increased from 45.1–93.8 cm2.
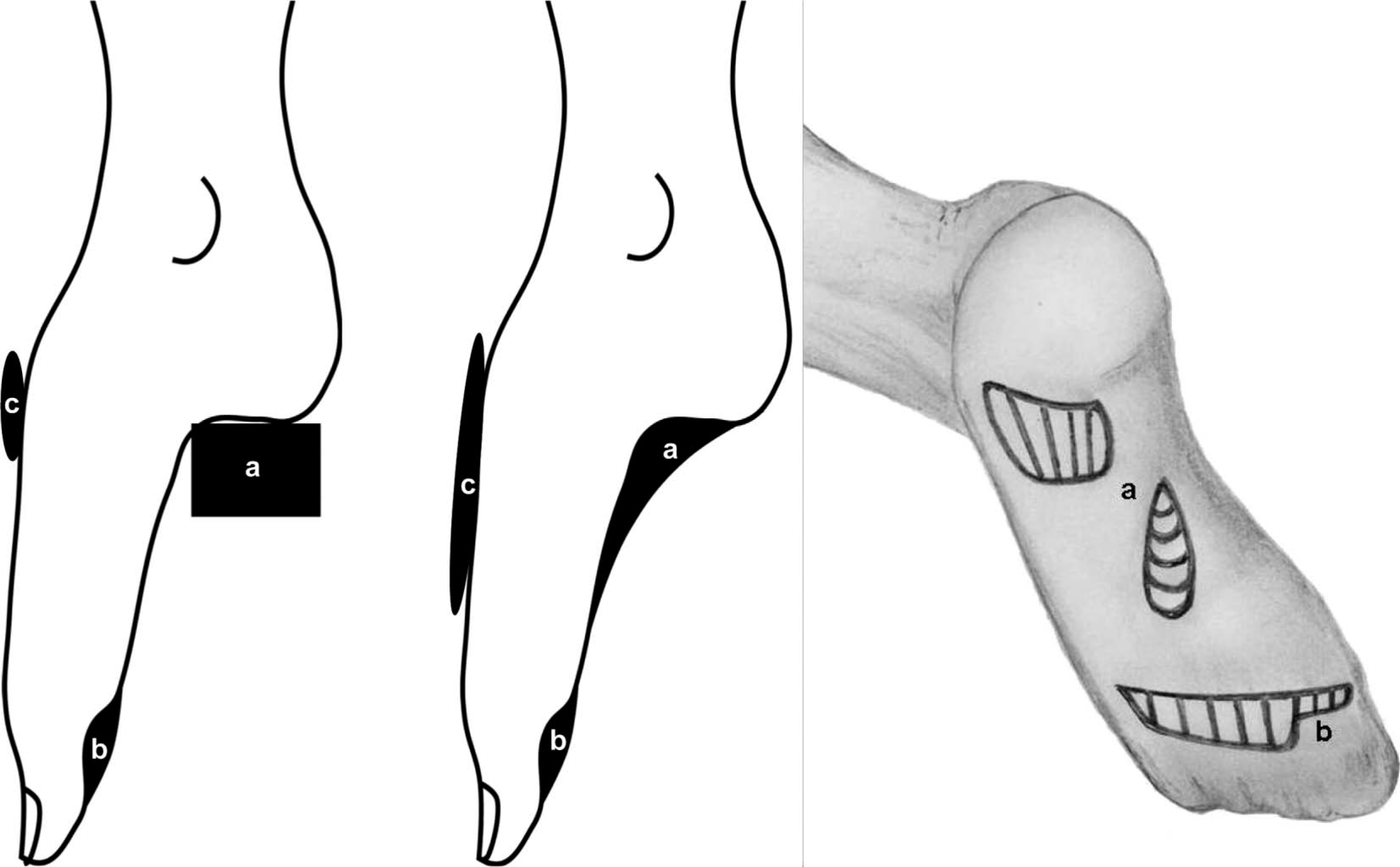
(a) Heel bench, (b) toe-gripping bead, (c) heel clamp. (I) old design, (II) new design, (III) forming of (a) and (b).
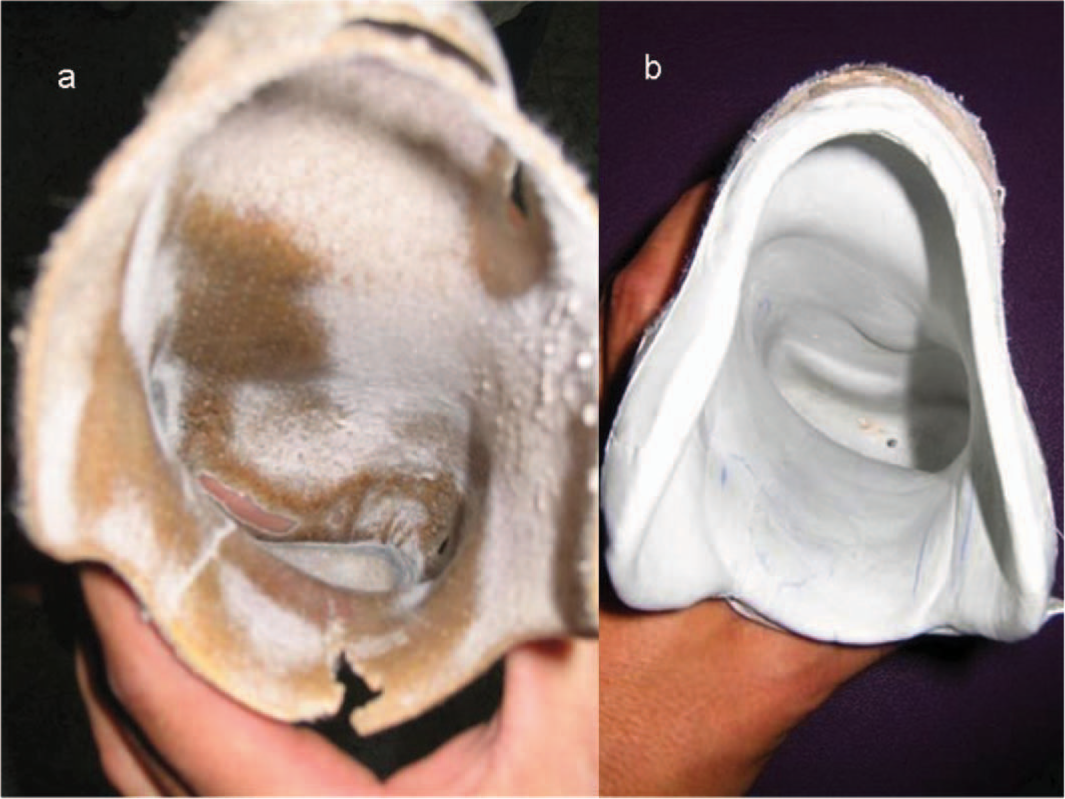
(a) Old prosthesis; (b) new prosthesis.
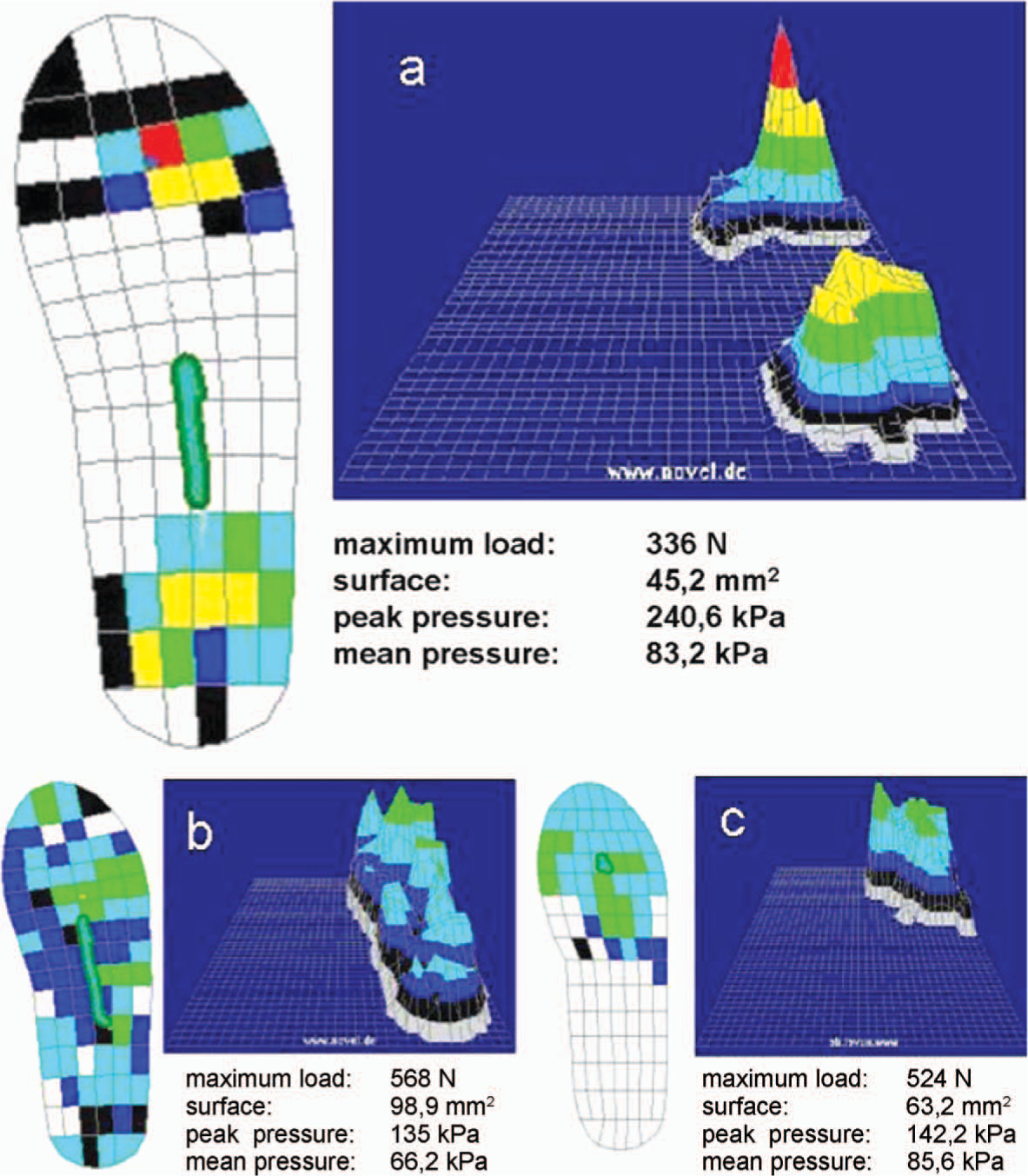
(a) Foot, plantar loading with old prosthesis; (b) foot, plantar loading with new prosthesis; (c) foot, dorsal loading with new prosthesis.
Results of the foot loading measurements
With her old prosthesis, the patient was able to walk pain free for half an hour when she was working at the bank. She was not able to do any sports because of pain (4/10 on VAS after 30 minutes of physical strain). After a period of six months getting used to the new prosthesis her calluses nearly disappeared and she was no longer limited in walking. Instead she learned Inline Skating and Downhill Skiing in her free time. In the year that the patient adjusted to the new prosthesis, she did not get any physiotherapeutic support.
Clinical follow-up revealed an obvious decrease in the patient's calluses as well as a decrease in pain (0/10 on VAS after 2 hours Inline Skating or Skiing) (see Figure 5).

Callosities and blisters, medial and lateral view: Old prosthesis (a), after wearing the new prosthesis for one year (b).
Discussion
Hillmann et al.9,10 demonstrated that the pressure distribution measurements in the prosthesis shaft are feasible and reproducible with the above-mentioned technique. Furthermore, the measurements were able to distinguish between prosthetic designs with different constructions in the same patient. By modifying the shape of the soft socket, a reproducible decrease of the pressure peak level could be observed. It proved to be a disadvantage to provide the heel bench with a completely horizontal tread surface. This surface can absorb axial forces very well but, in dorsiflexion, removes the heel from its original position. This results in an incongruity between the mechanical and the anatomical centre of rotation. Furthermore, the skin is not able to adjust to the peak load anymore. Given that the foot has to absorb the axial forces almost entirely by itself, it is necessary to use every possible surface to bear weight and distribute the pressure. Already a small support of the distal metatarsal heads increases the contact area and causes a clear area of decompression. Yet, the highest pressure is absorbed by the modified heel bench, in combination with an increased load bearing area at the dorsum of the foot. Therefore, the soft socket has to be modelled like a stirrup, incorporating the medial and lateral longitudinal arch, to prevent from sliding into the shaft.
Conclusion
This single case study has shown that a modification of the soft socket (mainly by shaping a heel bench and a toe grip) can considerably improve pressure distribution. An increase of the load bearing area enables the skin to compensate even intensive strain during athletic activities.