
Abstract
Background and aim:
Current leg prostheses in rotationplasty typically feature a thigh cuff, which, in cycling, may cause perspiration problems and friction-related abrasions of the skin. The aim has been to develop a socket-less prosthetic device for persons with a rotationplasty to be able to engage in high-intensity cycling without contracting abrasions.
Technique:
The new device (Socket-Less Rotationplasty Prosthesis for Cycling) features a standard cycling shoe on the rotationplasty foot, replacing the conventional socket and thigh cuff. A reinforced 12-layer carbon fibre frame bolted to the aforementioned shoe, replacing the standard tube, connects to a prosthetic foot and a second cycling shoe. Alignment of the Socket-Less Rotationplasty Prosthesis for Cycling is done both statically and dynamically.
Discussion:
The Socket-Less Rotationplasty Prosthesis for Cycling is lightweight and more ventilated relative to conventional sockets. All components can be replaced easily. Most important, however, is that the current user now can cycle 135 km on end without skin abrasions.
Clinical relevance
The Socket-Less Rotationplasty Prosthesis for Cycling concept enables patients with a leg rotationplasty to engage in high-intensity cycling without contracting skin problems, thereby facilitating clients’ participation.
Background and aim
Van Nes rotationplasty is a surgical limb-sparing procedure in which after resection of some middle part of a limb, the distal part is rotated 180° and attached to the residual proximal part. 1 The 180° rotation of the distal part of the leg allows for the ankle joint to be used as a functional knee joint when fitted with an appropriately modified below-knee prosthesis. 2
A conventional rotationplasty prosthesis typically consists of a leather thigh cuff and straps, a cast resin socket holding the rotated foot, metal hinges medially and laterally, a prosthetic tube as lower leg and a carbon foot (Figure 1). The thigh cuff is used to stabilize the new knee joint. The subject in Figure 1 (see also case description below) wore a cotton stocking covering the rotationplasty foot and upper leg underneath the prosthesis. His foot was in maximal (active) plantar flexion during standing and was kept in place within the socket by a silicon strap over the Achilles tendon. The biaxial hinge (7U10; Otto Bock GmbH, Duderstadt, Germany) allowed for 9 mm of translation. The tube consisted of an Otto Bock modular system (Otto Bock GmbH). His prosthetic foot (Pacifica; Freedom Innovations, Irvine, CA, USA) was customized to his activities and weight.

(a) Rotationplasty and (b) conventional prosthesis.
In general, patients are able to fully participate in society and pursue hobbies and a wide variety of sports. During high-intensity cycling, the thigh cuff of a conventional prosthesis leads to perspiration, chaffing and skin abrasion. These problems are thought to be due to the socket/cuff design and prosthesis alignment being suboptimal for the typical cycling movement of the leg. As the axis of the new knee joint is not fully congruent to the axis of the thigh cuff, and given the high frequency of the cycling movements, high friction forces upon the skin may occur during cycling. Higher active patients/persons with an amputation, who want to participate in sports, are commonly provided with an additional, purpose-specific sport prosthesis. For cyclists, this often encompasses major changes to the socket design as well as adaptation to the prosthetic foot.
The aim of our work has been to develop a socket-less prosthetic device for persons with a rotationplasty to be able to engage in high-intensity cycling without contracting skin abrasions. A simple way of keeping the prosthetic shoe on the bike’s pedal was also aimed for.
Case example
A male, 18-years-of-age, who underwent a rotationplasty after being diagnosed with an osteosarcoma in the distal part of the femur, was fitted with a modified below-knee prosthesis. His goal is to climb Mont Ventoux (France) on a racing bike. Using his conventional prosthesis, he regularly contracted abrasion injuries at both his foot and thigh. This was one of the causes why he was able to only cycle a distance of maximally 35 km. These abrasion injuries were caused by two interacting phenomena, that is, (1) friction caused by the rigidity of the socket and thigh cuff and (2) the kinematic mismatch between the normal cycling movement and the anatomical movement of the prosthetic leg. These injuries were aggravated by the restricted permeability of the prosthetic material. In addition, keeping his prosthetic foot on the pedal for a long time was difficult.
By describing the prosthesis design, we hope that others may benefit from what we have learnt in managing this client and can improve participation in high-end cycling for others with Van Nes rotationplasty.
As all activities described in this article were part of the client’s regular rehabilitation programme, no a priori ethical approval was necessary. Written informed consent as to the use of the data and photographic material presented in this technical note was obtained from the client involved.
Technique
Purpose-built prosthesis
In an iterative process, we were able to build a custom-made prosthesis. The final prosthetic design is described below. Emphasis is placed on the components used and the alignment, so that others may be able to replicate the prosthesis design. In Figure 2(a) to (c), the new device (Socket-Less Rotationplasty Prosthesis for Cycling (SRPC)) is shown. Close-up photos are given in Figure 3(a) to (c).
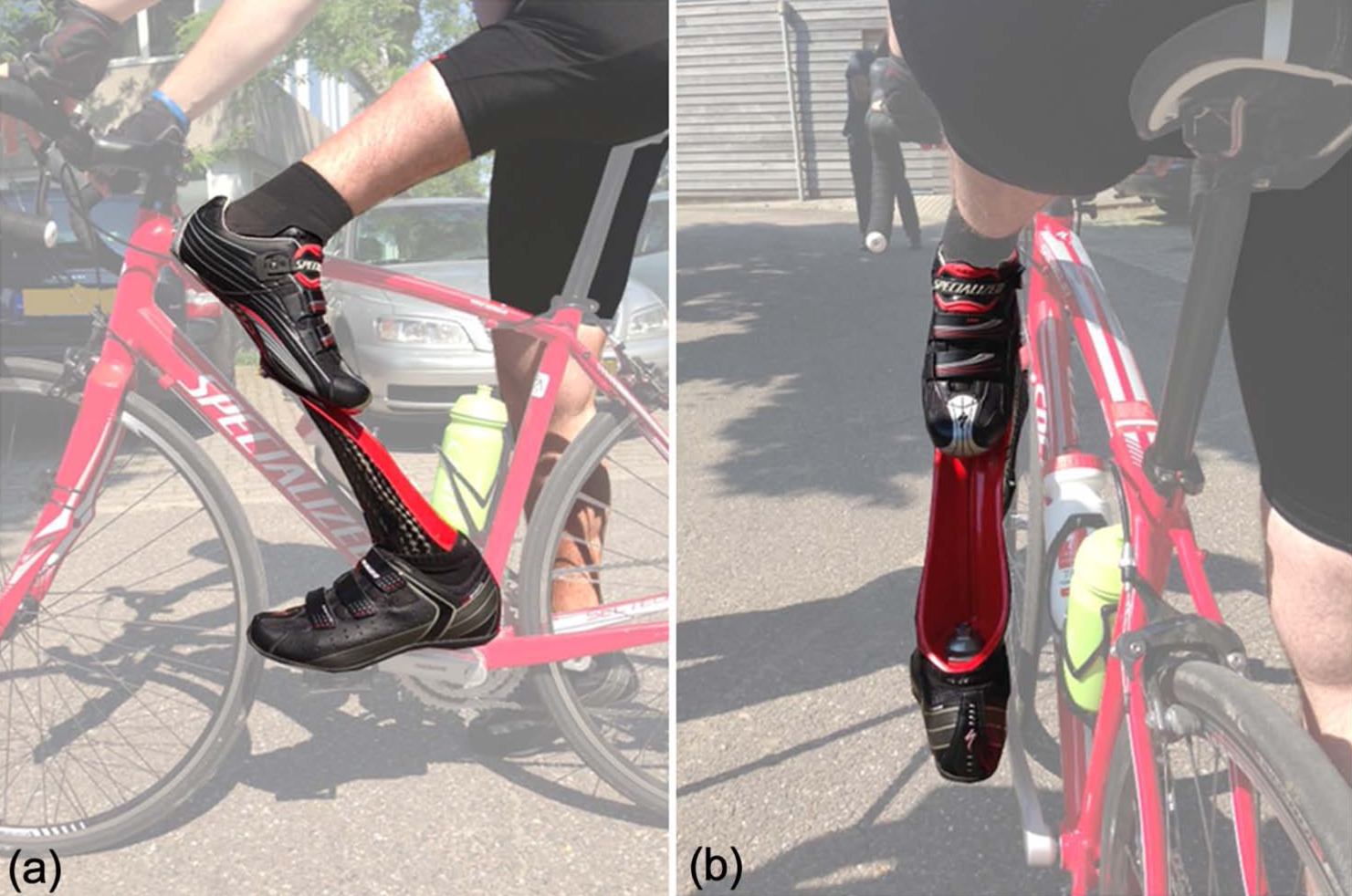
Client using the Socket-Less Rotationplasty Prosthesis for Cycling (SRPC): (a) lateral view and (b) posterior view.
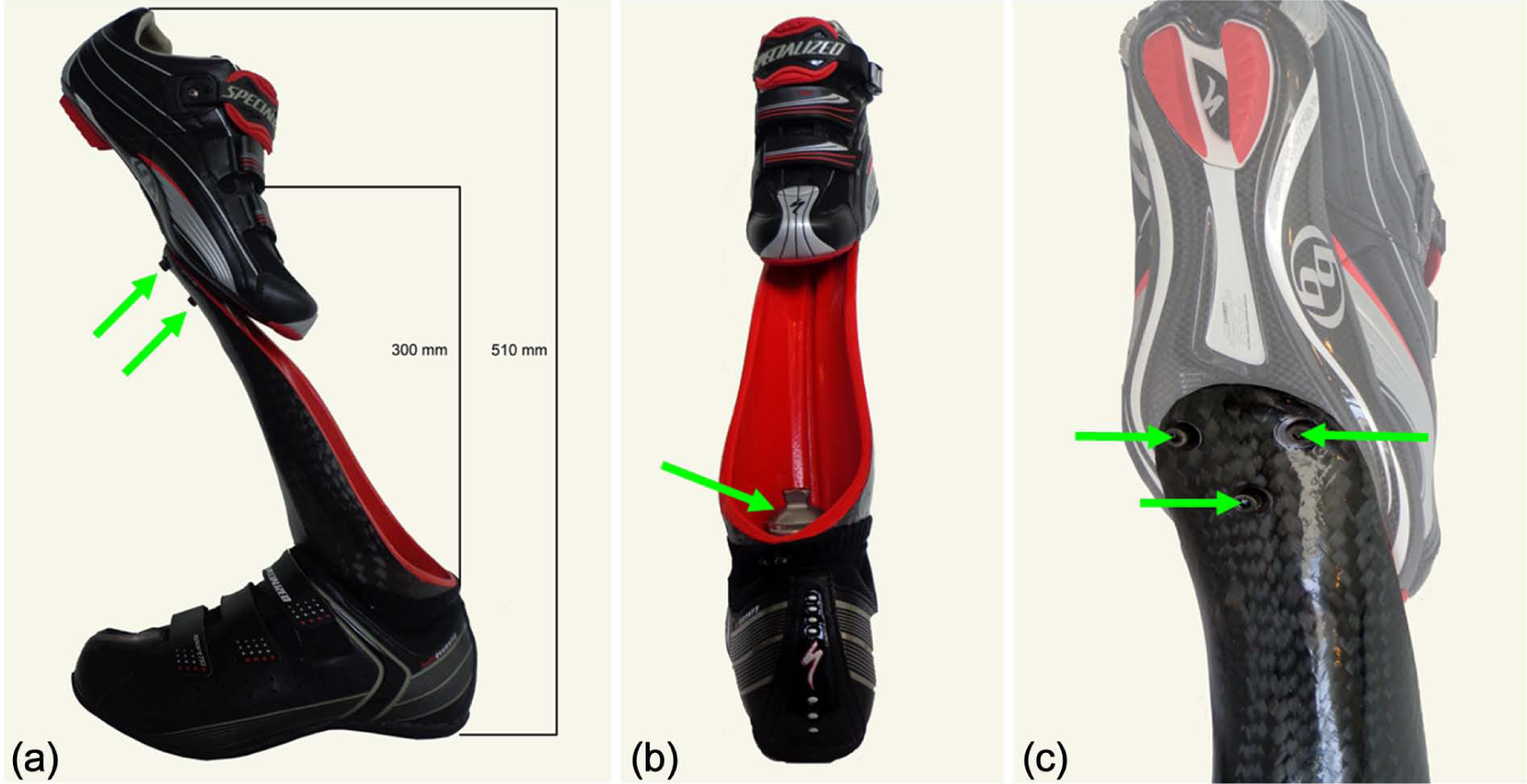
Components of the Socket-Less Rotationplasty Prosthesis for Cycling (SRPC): (a) lateral view, (b) posterior view and (c) close-up of mountings on the top shoe’s sole (anterior view). Mounting bolts are indicated by arrows.
Shoe/alternative socket
The shoe that fits the rotationplasty foot is an off-the-shelf product used in conventional cycling (Pro-Road Shoe 6109-1345; Specialized Bicycle Components, Morgan Hill, CA, USA), featuring standard bolting holes in the footplate/sole to fit conventional pedal click-on systems.
Frame/tube
The frame, as an alternative to the tube (Figure 3(a) and (b)), was made of carbon fibre (woven carbon fibre stockinette 12 cm; Otto Bock GmbH). As part of the design process, first a foam (6r8 Schaumstoff-Überzug 30 mm; Otto Bock GmbH) model was made, from which a negative plaster cast was taken. Subsequently, a positive plaster cast was made, which was laminated with four layers of Perlon (8 cm 7w700-08; Wagner Polymertechnik GmbH, Silkerode, Germany) and topped with acrylic resin (COPACRYL jersey; COP-Chimie, St Nazaire-en-Royans, France). Standardized lamination techniques are extensively described in literature, for example, Otto Bock 3 and Smith et al. 4 The frame is lightweight, strong and durable, which is essential given the large forces involved in cycling. An additional eight layers of carbon fibre were used. Furthermore, distal and proximal in the frame, the attachment points were reinforced using 4.5-mm additional carbon fibre layers (XRP; Distrac NV, Hoegaarden, Belgium). The frame was given an aerodynamic design, that is, concave on the dorsal side, giving access to fit the screw fixating a prosthetic foot to the distal part of the frame (Figure 3(b)).
Foot
The prosthetic foot (SACH, 1W073-L27; Wagner Polymertechnik GmbH) was fitted with a racing shoe featuring a Shimano Pedaling Dynamics (SPD) system (Shimano, Irvine, CA, USA) to prevent it from slipping from the pedal.
Connections and alignment procedures
Proximally, the shoe was fitted onto the carbon frame using three conventional M5 hexagon socket bolts and 0.5-mm washers fixated in the holes of the footplate/sole (Figure 3(a) and (c)). The prosthetic foot was attached to the distal part of the carbon frame using a hardened M10 bolt (Figure 3(b)). After an initial standard tuning of the bike to the subject’s general anthropometric measures, that is, adjusting the height of the seat and the position of the handle bars, alignment of the SRPC to the bike’s pedal and crankshaft was done both statically and dynamically, taking the subject’s non-affected foot and leg as a (mirrored) reference. During the full crank cycle, the maximum knee extension angle, which depends on the ratio between upper and lower leg length, was kept below 173° (7° less than full extension), as the knee never reaches full 180° of extension in normal cycling either. The three-dimensional position of the alternative socket relative to the prosthetic foot and pedal was determined by temporarily using the Otto Bock modular system, which allows for quick and easy adaptation of the prosthetic alignment. This system was subsequently replaced by the final carbon frame described earlier. Adjustments in the transverse plane (toe-in and toe-out) were also facilitated by modifying the SPD clip system settings. A Body Geometry Fit Integration Technology (BG FIT) procedure (Specialized Bicycle Components Inc., Morgan Hill, CA, USA) was used to fine-tune the client’s cycling position on his bike in order to further optimize cycling output and comfort.
Discussion
The main aim has been to develop a socket-less prosthetic device for persons with a rotationplasty to be able to engage in high-intensity cycling without contracting skin abrasions. Using the SRPC prosthesis design, the client was able to more fully participate in high-intensity cycling. In 3 months, he was able to increase his participation to cycling 135 km without the previous problems of abrasion. To date, he has covered more than 1300 km, which suggests that the design is likely to be suitably durable for the intensity of the activity.
Based on our experience with the above-mentioned prosthetic concept, we would suggest clinicians to use off-the-shelf cycling components (e.g. cycling footwear) in rotationplasty prostheses aimed at facilitating cycling, given that a cycling shoe is far less expensive than a socket and may be exchanged more easily. Furthermore, one of the problems the subject reported prior to this study was his prosthetic foot sliding from the pedal. This was solved by another off-the-shelf product, that is, the SPD system. The latter also facilitates ease of (de)attaching the prosthetic shoe to and from the pedal by the client, although training for this is needed.
For cycling, one does not need a thigh cuff. The SRPC is not suitable for walking. However, the client is able to lean on his bicycle to walk a few metres in case of emergency. As to performance, the client’s perception was that he can generate more leg power enabling him to negotiate hills, which was impossible before. However, no corroborative data on any assumed power efficiency were gathered in this study. This should be investigated further.
Future research
Future design will focus on optimizing the prosthetic foot in terms of energy storage and restoration during cycling. A second area of future activities will encompass modifications regarding the SRPC concept to also facilitate gait. A third area of interest is the use of the SRPC concept in young children who are still growing.
Key Points
The SRPC facilitates abrasion-free, high-intensity cycling in clients with a leg rotationplasty.
The SRPC concept is simple yet sturdy, allowing for high strains and forces typically associated with cycling.
The SRPC components are easily adaptable and replaceable.
Footnotes
Acknowledgements
The authors would like to thank Bert Toma, Toma Cycles, Kerkrade, The Netherlands, for technical contributions to the project, and Geert-Jan Maas, senior physiotherapist at the Department of Amputation, Traumatology and Orthopaedics at Adelante Rehabilitation Centre, Hoensbroek, The Netherlands, for critically examining the manuscript.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.