
Abstract
This study aimed to investigate if prolonged use of shoes incorporating an unstable sole construction could facilitate improvements of balance in a sample of developmentally disabled children. Ten children (six male and four female) aged between 10 and 17 years participated in the study. Children were fitted with shoes incorporating an unstable sole (Masai Barefoot Technology®) and instructed to wear them for a minimum of two hours per day for eight weeks. A within subjects repeated measures design was used. Children were tested prior to receiving the shoes, four weeks after receiving the shoes and eight weeks after receiving the shoes. A force plate capable of rotating about a single axis (NeuroCom International Inc, Oregon) was used to test static balance, reactive balance and directional control. Static balance was not found to be influenced by prolonged use of the footwear; however, significant improvements were noted in children's reactive balance both with the shoes and barefoot. Results suggest that reactive balance can be improved by prolonged and regular use of shoes incorporating an unstable sole construction.
Keywords
Introduction
Balance can be defined as the ability to maintain the body's centre of mass in relation to the base of support.1 It can be further categorized into two major components, static balance, the ability to maintain a desired posture while stationary and dynamic balance, the ability to maintain a desired posture while moving.1 Current theory suggests that balance control is dependent upon the interaction of multiple systems2-4 including musculoskeletal, sensory and nervous systems. Due to its complex nature and the interaction of multiple sensorimotor processes,5 it is widely accepted that no single test is available to measure balance performance and subsequently recommended that a combination of tests be used to evaluate balance performance.
Children with developmental disabilities typically present with compromised balance in tests conducted under both static6-8 and dynamic conditions.9-11 As a result they often present with delayed or deviated motor development.12 One of the major goals of habilitation is subsequently improvement of balance.
Improvement of static balance is often addressed in intervention studies.2,, 9,, 13-15 One of the most commonly applied means of assessing static balance is to record the movement of the centre of pressure of the body during quiet standing. While it is argued that centre of pressure variability during quiet standing is not a sufficient measure of postural stability7,, 16, movement of the centre of pressure can be used to provide useful insight into an individuals ability to correct imbalance of the centre of mass16 and to investigate how this may alter after a specific therapeutic intervention.
Intense intervention programs have been associated with significant improvements in static and dynamic balance of children with developmental deficits. Training on a perturbation platform has for example been demonstrated to increase the probability that children would activate functionally appropriate muscles,17,, 18 reduce their overall movement, reduce the time taken to stabilize their centre of pressure after a perturbation9 and result in a more rapid muscular response.17
In recent years, shoes incorporating an unstable sole construction have been released onto the market. (e.g., MBT shoes, Masai Barefoot Technologies, Switzerland; Chung Shi Shoes, Foot Solutions Inc, USA; Fit Flops™, London, UK; Exercise Sandals, Orthopedic Physical Therapy Products, Minneapolis; Shape up shoes, Atlanta, USA). The concept of these shoes is similar to that of unstable training platforms in that they encourage activation of the lower extremity by making the balance surface less stable.19,, 20 Manufacturers of the shoes claim numerous benefits associated with regular use of the footwear including; improved posture and balance.
MBT shoes have been associated with kinematic and kinetic alterations in gait,21-23 altered plantar pressure characteristics24 and alterations in calf musculature intensity and activity.21,, 23 Improvements in single limb standing balance, as measured by displacement of the centre of pressure have been demonstrated with eight weeks of training using Exercise Sandals™.20
The purpose of this study was to evaluate the relative effects of using MBT shoes on static and dynamic balance in a population of children with developmental disabilities. If the shoes, as claimed, function like an unstable training platform it was anticipated that subjects would present with reduced movement of the centre of pressure in static standing trials and reduced time taken to stabilize their centre of pressure after a perturbation. Also of interest was the relative effect of the shoes on rhythmic weight shifting ability as this variable has previously been correlated with improvements in walking performance in children with developmental disabilities.25
Method
Participants
Participant characteristics
Apparatus
All testing was performed using the Pro Balance Master (NeuroCom International Inc, Oregon). This system has been described in previous work9,, 26,, 27 and incorporates an 18 × 18-inch force plate that is capable of rotating about a single axis. Strain gauges positioned under the force plate measure Fx, Fy and Fz components of the ground reaction force and allowed for computation of the centre of pressure, defined as the centre point of force that the child exerts on the plate in the x and y direction. Movements of the centre of pressure in the coronal plane (x-direction) and the sagittal plane (y-direction) were exported for analysis. All data was collected at a sampling frequency of 100 Hz.
Protocol
A within subjects repeated measures experimental design was used for this investigation. In this design each child served as his/her own control and was tested on three occasions with a minimum of four weeks in between each testing session. Baseline data was collected on the first testing occasion. Subjects had not worn their MBT shoes prior to this time and were subsequently instructed to wear them for a minimum of two hours per day. On all occasions balance tests were performed once barefoot and once while wearing the MBT shoes. The order of testing (barefoot or with shoes) was randomized on each occasion. For each test, children were requested to stand quietly on the force platform with their arms by their side. Feet were placed symmetrically either side of the midline with the malleoli in line with the pivoting axis of the plate. Participants were instructed that they should not step or support themselves with their arms unless absolutely necessary. All subjects were fitted with a safety harness to protect them from falls.
Three specific aspects of balance were investigated. Included were one static balance test, and two dynamic balance tests (adaptation test and rhythmic weight shift test). Details of each test are presented below.
Static balance test
In order to test static balance children were asked to stand as still as possible on the force plate for a period of 20 sec. Four 20-sec trials were performed, two with eyes open and two with eyes closed. A custom program was used to analyze centre of pressure data according to formulae that have previously been identified as being clinically relevant and mathematically sound.8 The specific variables analyzed are presented in detail below and include, path length per second, average radial displacement and mean frequency.
(1) Path length per second (Equation 1) is defined as the average distance traveled by the centre of pressure per second. This variable provides an indication of the response of the central nervous system when attempting to correct imbalance of the centre of gravity.16

(2) Average radial displacement (Equation 2a) represents the average radial distance of the centre of pressure from the centroid of the center of pressure distribution (Equation 2b). This variable provides an indication of sway excursion, which has previously been shown to be greater in children with developmental disabilities.8


(3) Mean frequency (Equation 3) represents the frequency of revolutions of the centre of pressure about the centroid of the center of pressure distribution. This equation assumes that the path of the centre of pressure moves in a circular motion about the centroid location.8

Adaptation test
The adaptation test is a commonly accepted tool to evaluate reactive balance.9 During this test a perturbation to the children's balance was unexpectedly made by suddenly rotating the forceplate, upwards (Toes up, five trials) or downwards (Toes down, five trials). Rotation and angular velocity of the force plate was maintained at a constant 8° in 0.4 sec and ground reaction force data was collected for 2 sec after the onset of the perturbation. Custom software was used to calculate the time to stabilization of the centre of pressure. Time to stabilization was calculated according to criteria previously described by Shumway-Cook et al.9 Stability was noted when the centre of pressure was maintained within a 5 × 5 mm square for a period of 500 ms. As only 2 sec of data was available after the onset of the perturbation, due to limitations of the data capture software, stabilization data was subsequently coded as fast (stabilization achieved in less than 1 sec), moderate (stabilization achieved between 1 and 2 sec) and not achieved, (stabilization not achieved within 2 sec, the subject fell or the subject took hold of the handrail). The frequency of falls was also recorded for analysis. A fall was indicated when the child stumbled and took hold of the safety rail or when the safety harness was needed to prevent the child from injuring him/herself.
Rhythmic weight shift
The rhythmic weight shift test provides an indication of directional control and synchronization of movement. The test is of particular interest as previous studies have found that voluntary weight shifting ability is closely correlated with ambulatory function in developmentally disabled children.12 In this test, children were able to control the position and movement of a centre of pressure cursor displayed on the computer screen by shifting their body weight from side to side or front to back. They were requested to control this cursor and attempt to match the timing and position of a target that moved in a straight line between two end points (see Figure 1). After an initial practice session to ensure that the children understood the test, three trials were performed at slow (3 sec between the end points), medium (2 sec between the end points) and fast (1 sec between the end points) velocities. The trials were then repeated with the target traveling forward and back. While the target velocity was altered between trials, the displacement of the target remained consistent across testing occasions. By altering the target velocity only, different aspects of motor control were able to be investigated. For fast trials rhythmic weight shifting speed is similar to that of the normal walking cycle and assumed to be an automatic movement pattern while slower trials require more voluntary control.12
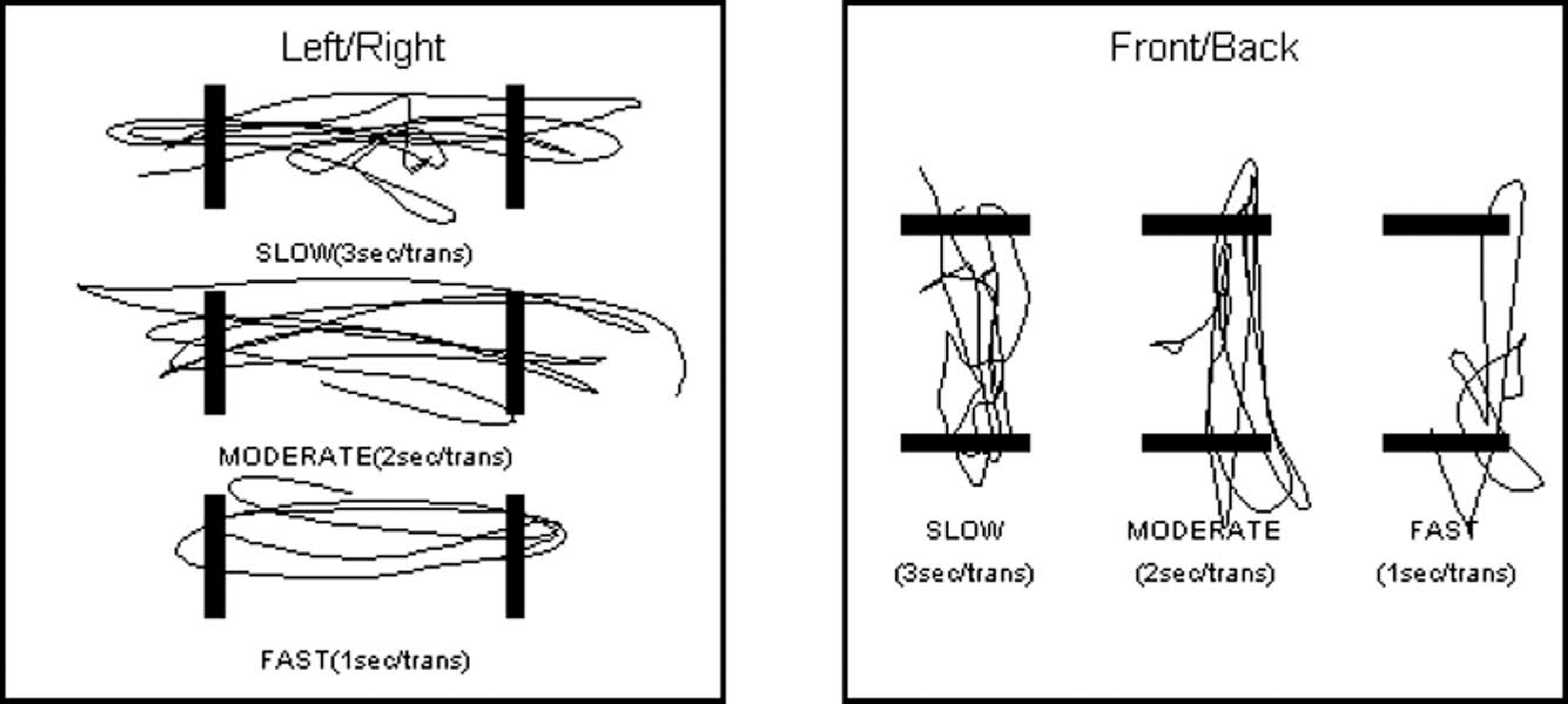
Sample data from the rhythmic weight shift test showing movement of the centre of pressure between two end points.
Data was analyzed using Neurocom software as described by Cheng et al.27 Of particular interest were values for directional control. If one defines the distance traveled by the moving target as representing the on-axis distance and the off axis distance as being the actual distance traveled by the centre of pressure, directional control is calculated by subtracting the off-axis distance from the on-axis distance and expressing it as a percentage of the on-axis distance. It is anticipated that subjects with motor disorders that disrupt normal rhythmic movement may exhibit slower than normal velocities and poor directional control.28
Statistical analysis
SPSS for Windows (version 14.0) was used to facilitate data analysis. Shapiro-Wilk tests were performed to determine if data from the static trials were normally distributed. As the assumption of normality was violated (p < 0.05) in several conditions, the Wilcoxon signed-rank test was used to compare shod versus barefoot trials within each testing occasion and Friedman's analysis of variance (ANOVA) was used to evaluate differences across the three measurement periods. The alpha level for determining statistical significance was p < 0.05. Chi square analysis was used to evaluate for differences in the frequency of falls and in stabilization times (fast, moderate or not achieved).
Results
Two children (subjects 2 and 6) were not available to partake in the second testing occasion but were present on the third occasion. One child (subject 7) had difficulties understanding the instructions for the rhythmic weight shift test and was unable to complete this section of the investigation.
Static balance
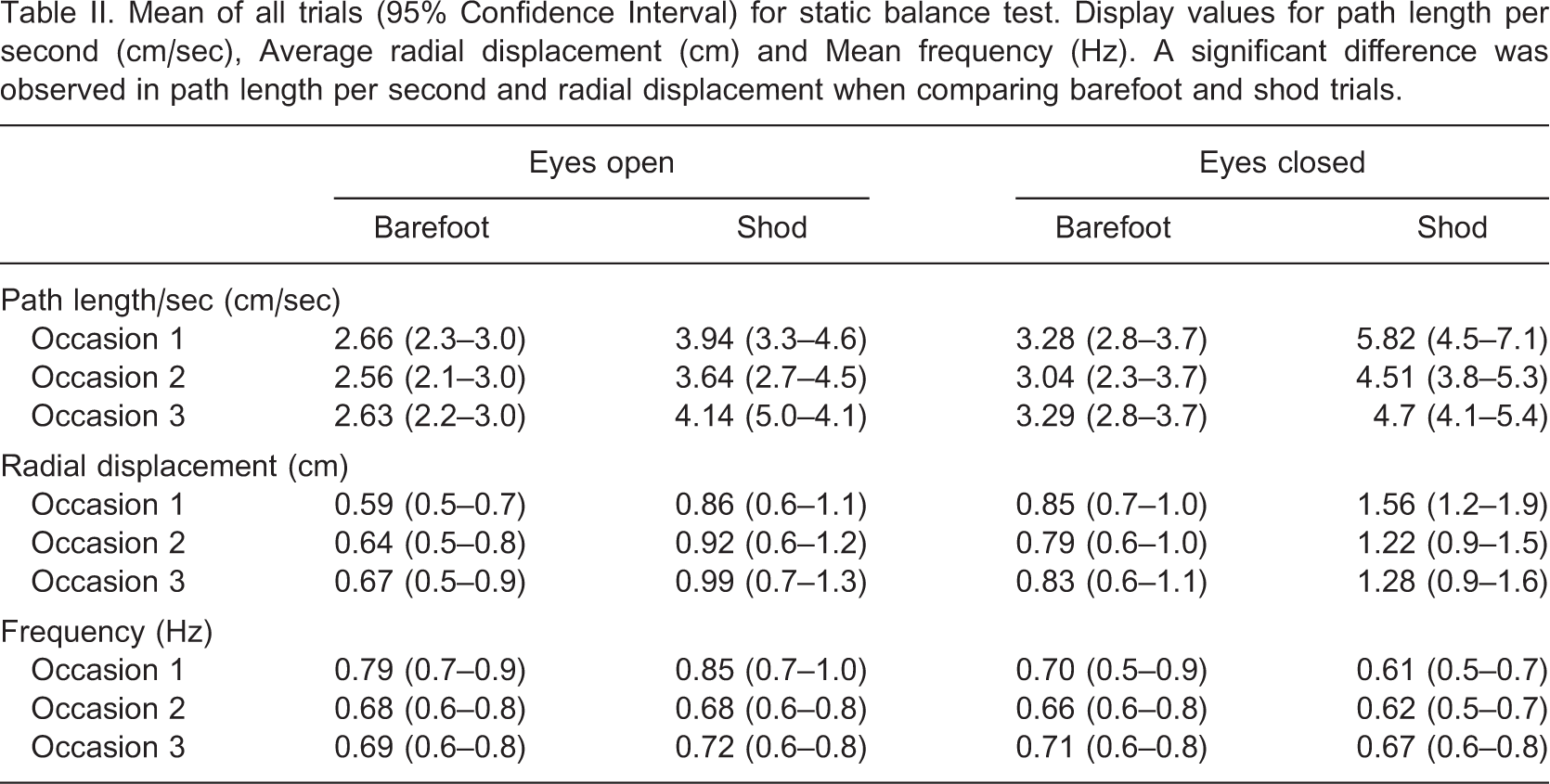
Figure 2 presents an example stabilogram of the centre of pressure data on occasions 1, 2 and 3 for the eyes closed, barefoot condition. Mean values of all trials for path length, average radial displacement and frequency are presented in Table II. Friedman's ANOVA revealed no statistically significant differences across the three testing occasions for any of these variables in either the barefoot or shod conditions. A difference was observed in the path length per second and in radial displacement when comparing the results of barefoot trials to results of shod trials within testing occasions (p < 0.05). Both variables were significantly greater when children were tested while wearing MBT shoes.
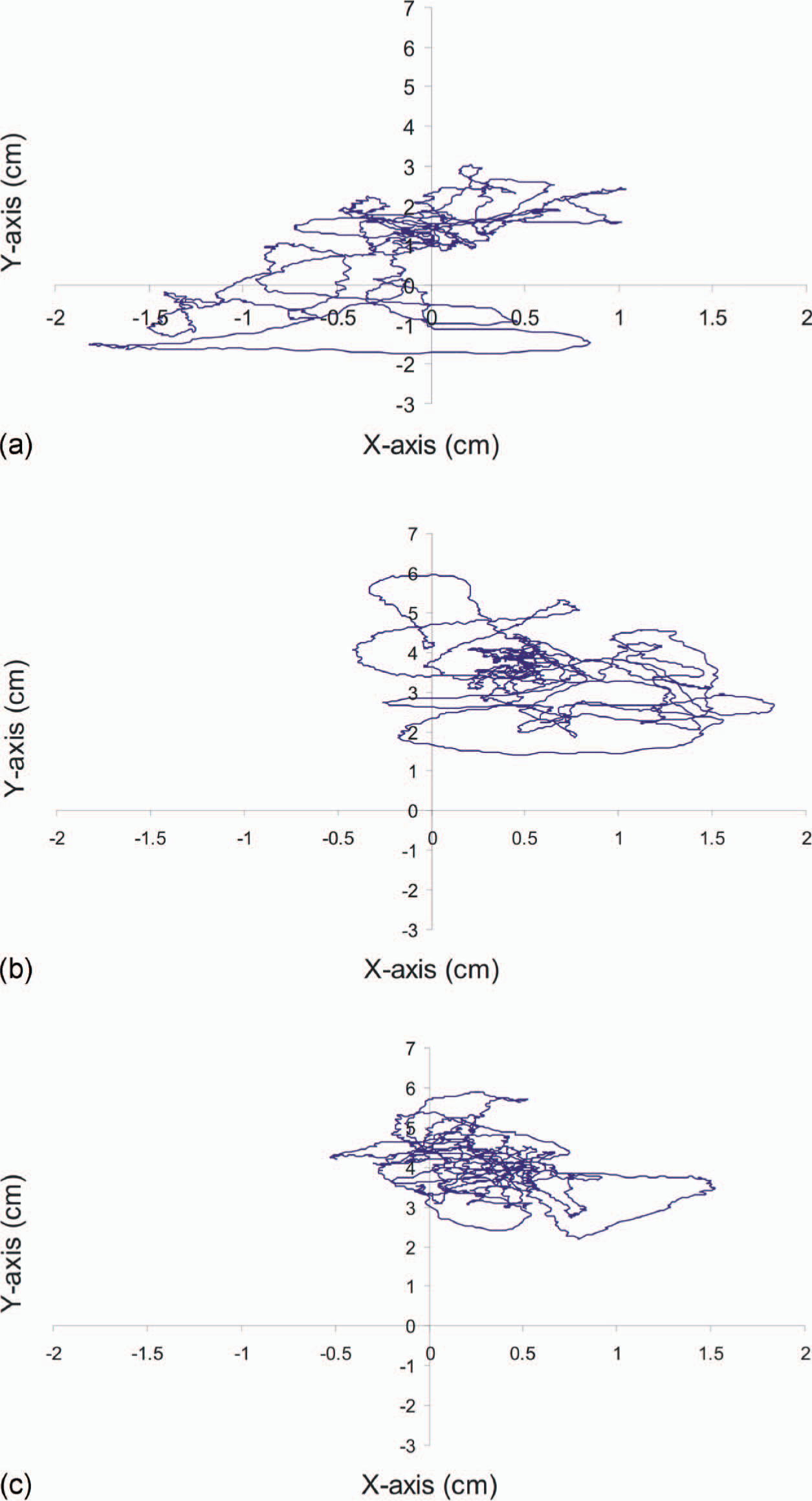
(a, b, c) Stabilogram recorded on occasions 1, 2 and 3 for subject 4, eyes closed and barefoot condition.
Mean of all trials (95% Confidence Interval) for static balance test. Display values for path length per second (cm/sec), Average radial displacement (cm) and Mean frequency (Hz). A significant difference was observed in path length per second and radial displacement when comparing barefoot and shod trials
Adaptation test (reactive balance)
Chi square analysis revealed significant differences in the time to recover stability following a perturbation (categorized as fast, moderate or not achieved). When tested without shoes, the time to stabilization significantly decreased across trials when the children were subject to ‘toes down’ perturbations (x2 = 11.1, p < 0.05). No difference was observed in the ‘toes up’ trials. In trials performed with the MBT shoes on, a significant difference was observed across testing occasions when children were subject to ‘toes up’ perturbations (x2 = 19.1, p < 0.05). Once again the time to stabilize following a perturbation decreased on each testing occasion.
The number of falls recorded for each subject on each testing occasion is presented graphically in Figure 3a and Figure 3b. For all conditions, the frequency of falls reduced across testing occasions. In the ‘toes up’ condition, Chi square analysis indicated a significant reduction in fall frequency across testing occasions in both barefoot (x2 = 7.5, p < 0.05) and shod trials (x2 = 10, p < 0.05). Chi square analysis could not be performed on the ‘toes down’ conditions as the low number of falls recorded on the second and third testing occasion violated the requirements for the statistical test.
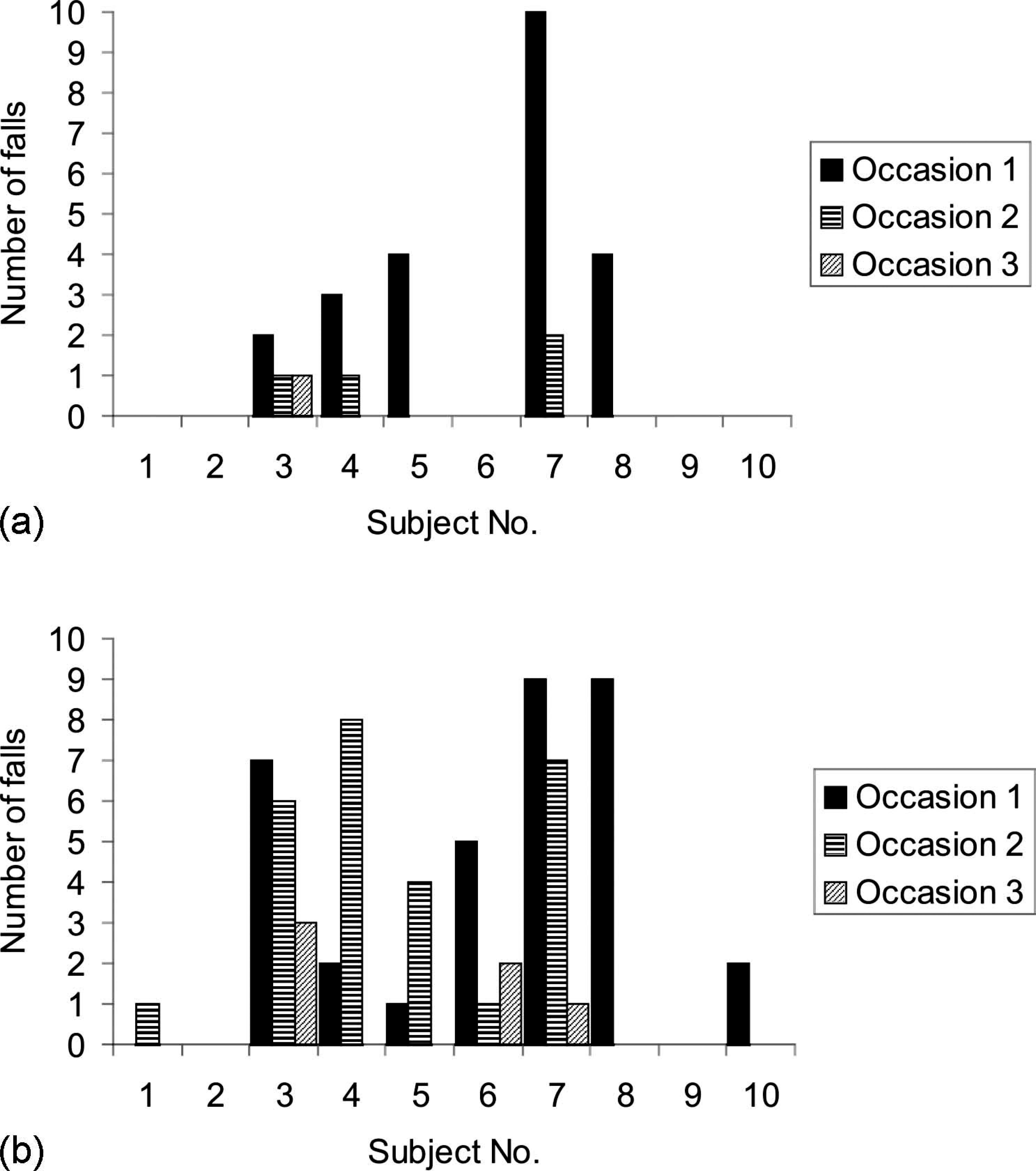
Number of falls observed per subject during the adaptation test. (a) Toes up condition. (b) Toes down condition. Note: Subjects 2 and 6 did not participate in testing on occasion 2.
Rhythmic weight shift
Mean values (Confidence Intervals) for directional control in the rhythmic weight shift test. Values are expressed as a percentage of the true distance traveled versus shortest possible distance
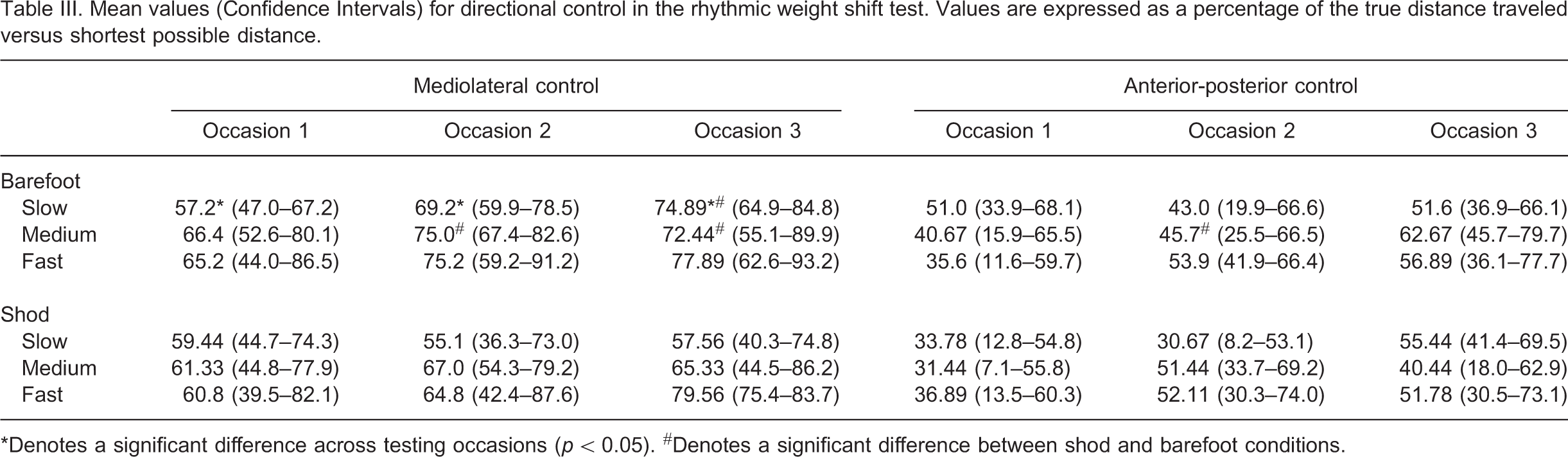
∗Denotes a significant difference across testing occasions (p < 0.05). #Denotes a significant difference between shod and barefoot conditions.
Discussion
This research aimed to investigate the influence of an unstable shoe construction on various aspects of balance in children with developmental disabilities. We intentionally selected tests that measure both static and dynamic aspects of balance as these have both been identified as integral to motor performance.2 Results from this pilot study suggest that prolonged wear of MBT shoes had little effect on the static balance performance of children involved in the investigation. Analysis of data did however suggest that the shoes were of significant benefit in training certain aspects of dynamic balance. In particular, performance improvements were observed in the adaptation test, suggesting that the children significantly improved their ability to recover stability in response to an external threat.
As change was observed in dynamic and not static tests of balance it is important to consider how the footwear may have influenced the underlying mechanisms that contribute to this aspect of balance. In response to an external perturbation a subjects postural response is influenced by their sensory motor response, their nervous systems ability to prepare and adapt to perturbations and the subjects own ability to learn and preplan a coordinated motor pattern.29 Further investigation is necessary to determine exactly how the use of unstable footwear may affect each of these variables. For example, it would be particularly interesting to investigate if the use of unstable footwear influences how specific postural strategies are implemented in order to maintain balance following a perturbation. Horak and Nashner30 describe two strategies for maintaining balance, an ankle strategy and a hip strategy. The ankle strategy is proposed to be most effective for maintaining an upright posture and the hip strategy is most beneficial when rapid movements of the centre of mass are required. While each strategy is not discrete or mutually exclusive, it has been demonstrated that they can be learned and are affected by experience.29
Measurements related to static balance and rhythmic weight shift were significantly better in the barefoot trials. These results are consistent with the findings of Nigg et al.23 and are not surprising given the intentionally unstable construction of the shoe which is designed to make the support surface less stable and activate intrinsic musculature.21 It is however important to recognize that while wearing the shoes an individual's balance is significantly compromised, creating an increased risk of falling. Care should subsequently be taken in prescribing the footwear to those with serious balance issues.
Results from this study have important clinical implications. Of most relevance is that the prescription of unstable footwear may facilitate the training of reactive balance and to a lesser degree directional control in children with developmental disabilities. These results are consistent with those observed in children with cerebral palsy after participation in intense therapy programs.9, ,17,, 18 Further investigation is warranted to evaluate the relative effectiveness of both treatment options.
This investigation was intended as a pilot study. As a result the study is limited by a lack of randomization and a small number of subjects representing a range of different conditions. The repeated measures design could also have led to learning effects which may account for some of the improvements observed across testing occasions. It is however unlikely that learning effects could account for all of the differences observed in this study. Previous work has demonstrated learning effects associated with training on a moveable platform however in these studies children were exposed to 100–200 perturbations per day for three to five consecutive days.9,, 17 In the present study, children were exposed to only 20 perturbations on three occasions that were four weeks apart.
Whether the balance improvement observed in this study was a result of peripheral or central control mechanism modulating the response is unable to be determined. As balance was affected by use of the footwear, it is necessary to further investigate neuromuscular responses associated with prolonged use of the shoes.
Due to technical limitations with the measurement software only two seconds of data was able to be collected following a perturbation in the adaptation test. This has limitations when analyzing data related to time to stabilization. Future investigations should consider increasing these data collection times.
Conclusion
Our results show that prolonged use of shoes with an unstable sole construction can be of significant benefit in improving the response to external perturbations in children with developmental disabilities. Static balance performance remained unchanged after using the MBT shoes for a period of eight weeks.