
Abstract
Residual limb pain is defined as a painful sensation or feeling from the remaining part of the leg. Aggressive bone edge, bone spur formation, neuroma, abscess or bursitis are common causes of residual limb pain. On the other hand, regional osteoporosis on femur and tibia is an inevitable consequence in patients with lower limb amputations. The etiology of bone loss is uncertain but it is likely to be a local phenomenon in lower limb amputees. Altered gait pattern, decreased weight load, disuse atrophy and lack of muscular action at the limb seem to be important causal factors in the development of both local and generalized osteoporosis. The aims of this study are: (i) To determine if there is significant bone mineral density (BMD) difference at proximal tibias and femurs between intact and amputated limbs, (ii) to investigate the factors affecting bone loss in these areas and (iii) to investigate the possible relationship between residual limb pain and local bone loss. The 36 men who participated in this study had amputations due to land-mine injuries. Dual energy X-ray absorptiometry was used to determine BMD of the proximal femur and proximal tibia. The non-amputated limb was used as a control for the amputated side. BMD values on the amputated side were significantly lower than non-amputated side. In addition, BMD values on the amputated limbs with residual limb pain were significantly less than in those without residual limb pain. Insufficient mechanical loading leads to bone loss in patients with trans-tibial amputations. Furthermore, bone loss at tibia may be a cause of residual limb pain. However, this needs to be confirmed with more specific studies in the future.
Introduction
Patients with different levels of amputations are under the risk of bone mineral loss on the amputated side. It has been shown that in trans-femoral amputees, osteopenia/osteoporosis is significantly more severe in the amputated side compared to the normal leg (Benichou and Wirotius 1982; Kulkarni et al. 1998; Rush et al. 1994). Altered gait pattern, decreased weight load, disuse atrophy, lack of muscular action at the limb, lack of total contact between stump and prosthetic socket seem to be important causal factors in the development of both local and generalized osteoporosis (Geiser and Trueta 1958; Rush et al. 1994; Kulkarni et al. 1998; Leclercq et al. 2003). It was shown that mean femoral bone density on the amputated side significantly decreased (12–28%) when compared to intact limb (Rush et al. 1994; Royer and Koenig 2005). On the other hand, in their study with a relatively small sample size, Royer and Koenig reported that the intact limb medial knee bone mineral density (BMD) was 45% greater than the prosthetic side in amputees (Royer and Koenig 2005). However, there were some patients with bone tumors in those studies that could possibly alter bone metabolism according to the nature of tumor itself or the drugs used for the therapy. Thus it is hard to decide that these alterations were caused by changes at mechanical loading.
Several studies have shown that, amputee patients often complain with residual limb pain. Residual limb pain is defined as a painful sensation or feeling from the remaining part of the leg but not from the removed part of the leg (Smith et al. 1999; Ehde et al. 2000; Henrot et al. 2000; Marshall et al. 2002; Ephraim et al. 2005; Ong et al. 2006). Aggressive bone edge, bone spur formation, neuroma, abscess or bursitis are the leading causes for residual limb pain and can be determined by radiological methods (radiographs, diagnostic ultrasonography, computerized tomography, magnetic resonance imaging, etc.) (Henrot et al. 2000). But even these factors are excluded, there could be still pain. We hypothesize that osteoporosis at the residual limb could be a determinant of residual limb pain.
The aims of this study were: (i) To determine if there is significant BMD difference at proximal tibias and femurs between intact and amputated limbs, (ii) to investigate the factors affecting bone loss on the amputated site in young veterans with traumatic trans-tibial amputations and (iii) to investigate the possible relationship between residual limb pain and local bone loss.
Materials and methods
This was a prospective cohort study of patients who had suffered from land-mine injuries. Healthy male veterans with traumatic unilateral trans-tibial amputations above the age of 18 years old were included in the study. Patients who were younger than 18 and older than 45 years of age and with etiologies other than traumatic etiology were excluded to prevent the possible effects of these factors on bone metabolism. None of the included patients had any disease that could affect bone density.
Bone mineral density
Dual energy X-ray absorptiometry (DEXA/LUNAR DPX®) was used to determine bone mineral density (BMD) of the femur/hip (total, neck, Ward's triangle) and tibia/knee. The non-amputated limb was used as a control for the amputated side. This technique uses a computer, which measures the differential absorption of two different X-ray beams to correct for varying degrees of soft tissue. Osteoporosis is abnormal rarefaction of bone by demineralization, which may be idiopathic or occur secondary to other diseases. Osteopenia is a condition of reduced bone mass due to a reduction in the rate of bone matrix (osteoid) synthesis to a level insufficient to compensate for the rate of normal bone lysis. The World Health Organization (WHO) criteria for osteopenia and osteoporosis denotes that a T score (relates to mean of the young adult population) between −1 and −2.5 SD indicates osteopenia and below −2.5 SD determines osteoporosis. These scores are units of standard deviation (SD) beyond the mean. T-scores are reported along with levels of BMD.
For bilateral hip and proximal tibia scans, subjects lay in a supine position. When the femoral neck was scanned, the leg was rotated internally and abducted slightly. This positioning brings the femoral neck parallel to the scan table and prevents foreshortening of the femoral neck (Kulkarni et al. 1998). Before starting the proximal tibia scan, knee was placed in approximately 5° flexion and lower limb was slightly rotated internally. This position has been found to optimize both the knee joint space and the separation of the fibula from the tibia (Beattie et al. 2005). Then the laser crosshair was positioned 10 cm distal to the superior border of the patella and proceeded proximally 11 cm. The tibia was positioned such that the shaft appeared vertically straight and that the epiphysis was centered on the imaging screen.
Pain assessment
A 10-point Visual Analogue Scale (VAS) was used for measurement of residual limb pain level. Patients with residual limb pain were evaluated with diagnostic ultrasonography and radiographs to determine if they had aggressive bone edge, bone spur formation, neuroma, abscess or bursitis. Patients who had one of those causes or who had phantom limb pain were excluded.
Statistical analysis
All analyses were carried out using SPSS 10.0 for Windows. The BMD value differences between surviving and amputee limbs were evaluated by paired t-test. Pearson correlation analyses were performed to evaluate the value of age, duration of amputation, occupational condition, daily exercise level, daily prosthesis usage and BMD of amputee lower limb. In addition, the BMD value differences in amputated side between patients with and without residual limb pain were evaluated by Mann-Whitney U test. Results were considered statistically significant at the <0.05 level.
Results
Of the 36 men who were participated in this study, 19 (55.9%) were right sided and 15 (44.1) were left sided trans-tibial amputee. All had amputations because of a land-mine injury. Mean age at the time of study was 26.8 ± 3.5 (21–34) years and the mean duration of amputation was 62.8 ± 37.0 (6–160) months. 33 patients (91.7%) were wearing their prostheses, which were endoskeletal types, more than 5 hours a day and three subjects (8.3%) were wearing 3–5 h a day. None used any ambulatory aids.
All patients reported that they had an educational course about isometric and endurance exercises for residual limb. Exercise level was daily in 15 (% 41.7), every 2–3 days in 6 (% 16.7), once a week in 9 (% 25) patients and none in 6 (% 16.7) of the study group. Twnety of 36 amputees had residual limb pain and their mean value of pain±standard deviation (min.–max.) was 4.0 ± 1.9 (2.0–7.5).
The BMD measurements on the amputated side femoral neck/Ward's triangle/total and proximal tibia were significantly lower from the non-amputated side as shown in Table I (p < 0.0001). Same as t-scores for the femoral neck/Ward's triangle/total were significantly lower on the amputated limb (p < 0.0001) (Table I).
Comparison of BMD values and t-scores of traumatic trans-tibial residual limbs and surviving limbs (paired t-test)
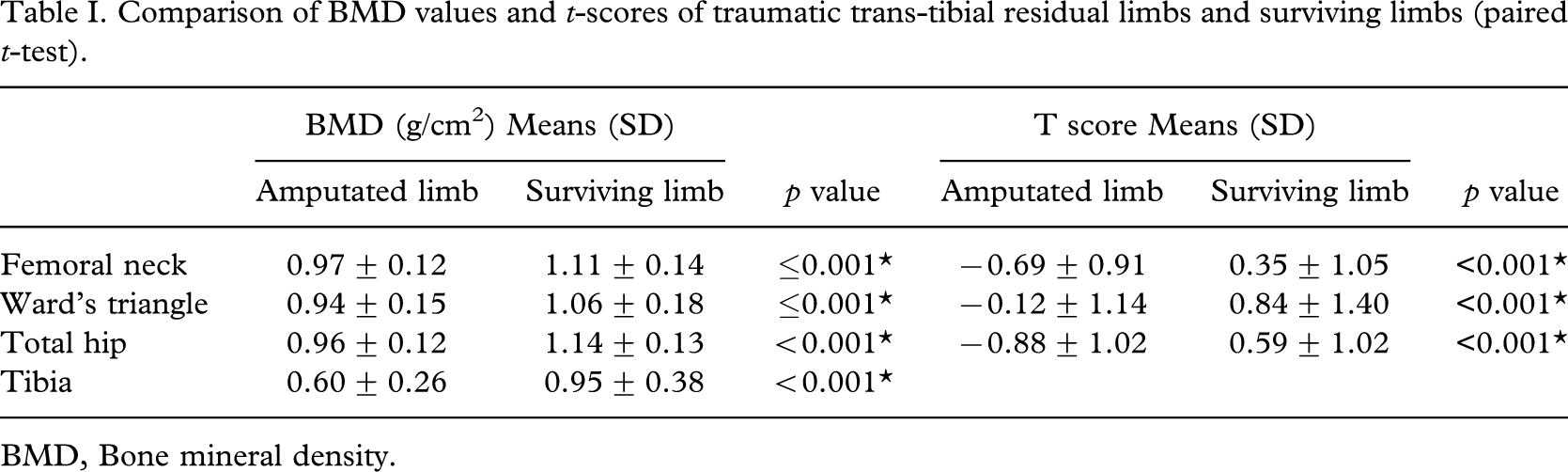
BMD, Bone mineral density.
Pearson and Spearman correlation analyses were performed to investigate if there is any correlation between value of BMD of femoral neck/Ward's triangle/total and proximal tibia relating to the subjects age, duration of amputation, subject's job, exercise level, daily prosthesis usage time and presence of a residual limb pain. Only presence of a residual limb pain was found to be significantly correlated with the value of BMD of proximal tibia in the amputated side (p < 0.05) (Table II). None of the other factors were found to be correlated to the value of BMD of femoral and tibial regions (p > 0.05) (Table II). In addition, there was no correlation between frequency of exercise and presence of stump pain (p > 0.05).
Pearson and Spearman correlation analyses of the value of age, duration of amputation, occupational condition, daily exercise level, daily prosthesis usage, presence of the pain in the residual limb and BMD of traumatic trans-tibial residual limbs
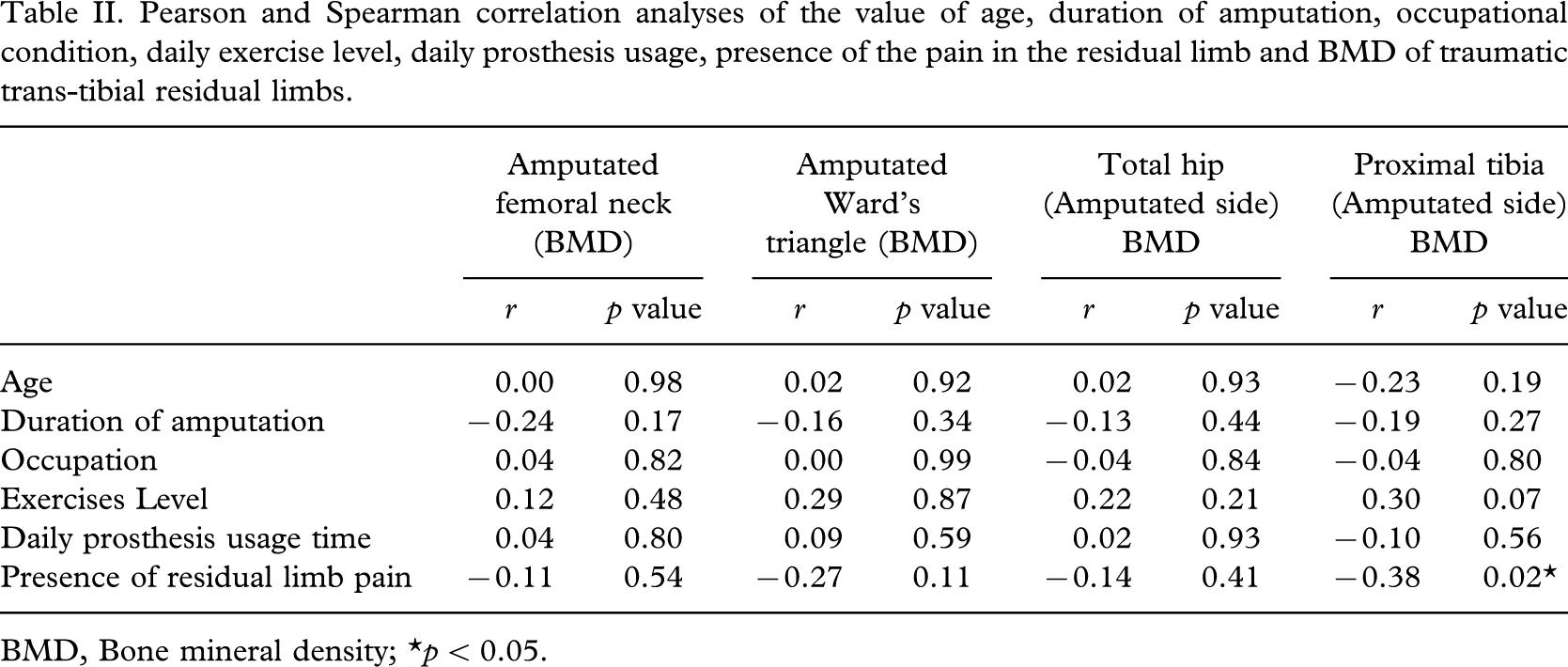
BMD, Bone mineral density; ∗p < 0.05.
BMD values of the proximal tibia with residual limb pain were significantly lower from the ones without residual limb pain (p < 0.05) as shown in Table III. Femoral neck, Ward's triangle and total hip BMD values of the amputated limb with residual limb pain were not significantly different from the ones without residual limb pain (Table III).
Comparisons of the BMD values in traumatic trans-tibial residual limb between patients with and without stump pain. (Mann-Whitney U test)
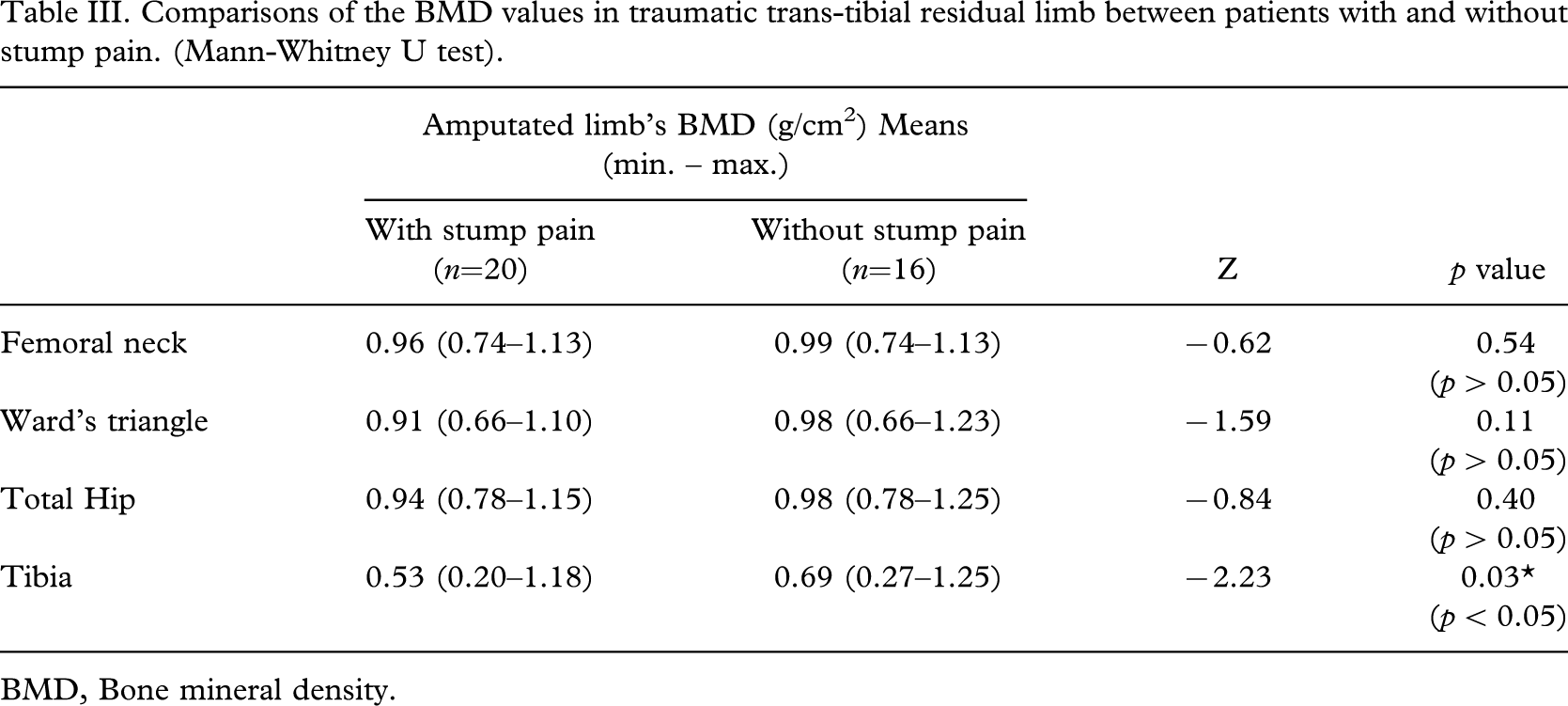
BMD, Bone mineral density.
Discussion
In this study, we have demonstrated the bone loss at femur and tibia on the amputated side in young unilateral trans-tibial amputees with traumatic etiology. In two different previous studies, Rush et al. (1994) and Kulkarni et al. (1998) similar BMD differences were observed between the femoral region of the amputee and survival limb. The etiology of bone loss is uncertain but it is likely to be a local phenomenon (Rush et al. 1994; Kulkarni et al. 1998). Osteopenia/osteoporosis found with amputations is a form of bone disuse atrophy as that seen in immobilization (Rush et al. 1994). Also, lack of muscular action at the limb may be associated with increased bone absorption. The decreased load placed on the trans-tibial amputated residual limb could predispose to disuse atrophy and hence osteoporosis in the amputated tibia.
The use of DEXA to evaluate BMD has long been accepted as the gold standard for its application as a diagnostic tool for evaluating to osteoporosis (Beattie et al. 2005). We detected significantly decreased BMD in the proximal femur and proximal tibia in amputated side in our study group. The lower BMD values in the amputated side correlated with the fact that osteoporosis can be due to disuse atrophy. This indicated that the load could not be equally distributed along the limb. The region of amputation also affects the BMD value. Kulkarni et al. (1998) defined that trans-femoral amputees have a significantly lower femoral neck BMD measurement on the amputated side than trans-tibial amputees. This can be explained by more effectively use of the amputated leg during walking in trans-tibial amputees this higher BMD values than in the trans-femoral amputees.
Persons with unilateral, trans-tibial amputation walk with an asymmetrical gait pattern. Knee and hip kinematics are similar between the intact and prosthetic limbs; however, the prosthetic ankle has diminished plantar flexion range of motion and angular velocity compared to the intact ankle (Sanderson and Martin 1997). Asymmetrical ankle function may contribute to alterations in lower limb mechanics. Specifically, the intact knee sagittal plane moment and power are greater than that of the prosthetic side reflecting a greater demand on the intact limb (Rush et al. 1994; Powers et al. 1998). BMD may be greater in the intact limb to this greater physical demand placed on it.
Also, in trans-tibial amputees, body-weight bypasses the proximal tibia, loads directly into the prosthesis and down to the ground. This also helps to define the decreased BMD values of proximal tibia on the amputated extremities. Although previous studies showed bone loss of only femoral regions, we described a similar decrease of BMD in proximal tibia.
The prevalence of residual limb pain varies from 10–13% at two years post amputation to 55–76% in longstanding amputees (Smith et al. 1999; Ehde et al. 2000; Ephraim et al. 2005). Chronic amputation-related pain can lead to limitations in physical and psychosocial function. In addition, the amputation-related pain is negatively correlated with employment (Schoppen et al. 2001; Ephraim et al. 2005). Unfortunately, causes of residual limb pain are difficult to diagnose because clinical manifestations are often non-specific (Henrot et al. 2000). To our knowledge, this is the first study that investigates the relationship between residual limb pain and bone loss.
Rush et al. (1994) found no correlation between duration of amputation and bone density loss. This finding was consistent with our study. However, they found an inverse relationship between the patient's age at the time of amputation and severity of osteopenia. They reported that the younger amputee patients had more osteopenia than the older ones. They stated two possible explanations for this correlation. Firstly, younger patients had more bone mass to start with than older patients. And because the younger patients would have greater loss of absolute density, they would show a greater percentage of osteopenia when the amputated side was compared to the normal side. Secondly, younger patients had their amputations before they had reached the peak of their bone mass. So, younger patients would start to lose bone mass from a lower level than older patients. In the above-mentioned study, ages ranged from 23–66 years. On the other hand, in the current study, we could not find a relation between age and BMD as, we believe, our patients' age range was small (21–34 years).
In the literature, studies dealing with osteoporosis in patients with amputations have important methodological challenges. Almost all of those studies included patients with amputations of different etiologies. In patients with metabolic, vascular or tumoral etiologies, bone metabolism is always affected by both the reason itself or the drugs used for the therapies. In this study, amputee patients with these etiologies were excluded and only traumatic etiology was included to prevent the effects of these reasons on bone metabolism (Gonzalez and Mathews 1980; Benichou and Wirotius 1982; Rush et al. 1994).
In conclusion, there is a significant decreased BMD in the amputated side compared with the intact limb. In addition, our study showed that there is a relationship between residual limb pain and BMD values of the proximal tibia. On the basis of this relation, our patients' pain complaints in the residual limb can be called ‘osteoporotic residual limb pain’. However, this needs to be confirmed with more specific studies in the future.