
Abstract
We performed a study on 32 idiopathic scoliotic patients (30 females, 2 males) treated with a Chêneau brace. Eighteen patients had a single right thoracic curve and 14 had a single right thoracolumbar curve. We used the TekScan® system (ClinSeat Type 5315 Sensor, TekScan, Boston MA, USA) to measure pressures at the skin-brace interface, assess the effect of strap tension and analyze the variation of these pressures with position and activity. The TekScan® device enabled identification of the pressure areas corresponding to the brace's three loading points. The pressure under the main pad had a greater mean value than the pressure under the two counter-pads. Tightening the straps led to a significant increase in the pressures, whatever the position studied or the curve pattern. Compared with the standing (reference) position, we observed significantly higher pressures during maximal inspiration (p < 0.001) and lower pressures during maximal expiration, in the prone position and after having risen from a lying position, for both thoracic curves (p < 0.001) and thoracolumbar curves (p < 0.01). The pressures for thoracolumbar curves were lower than those for thoracic curves, whatever the position studied and both before and after strap adjustment. For lying positions, lying on the right side produced the greatest increase pressure. Even though the TekScan® system does not provide direct information on the correction of spinal curvature, it appears to be a useful tool in the treatment of scoliotic patients. Strap adjustment clearly influences the applied pressures – particularly those on the rib cage. During activity, there is a natural tendency to decrease the pressure; this justifies efforts to maintain strap tensions in general and during day wear in particular.
Introduction
The Chêneau brace acts as three-dimensional system with three support areas that enable elimination of the rib-hump and mobilization of the flat parts whilst leaving respiratory movements unrestrained. However, the vertebra can only be subjected to force over a small proportion of its circumference, and the support pads act indirectly via the soft tissues covering the posterior arc. The other parts of the spinal column are not available for direct support, in view of the presence of the thoracic cavity and the abdominal viscera. Hence, corrective action is exerted indirectly and its efficacy depends on the rigidity of the interposed structures (Karger 1997; Wong and Evans 1998). Duval-Beaupère and Marty (1998) showed that correction of scoliotic curves occurs via passive mechanisms. The first type of force (called ‘detraction’) works to enlarge the distance between the head and the pelvis along the vertical anatomical axis, while exploiting the visco-elasticity of the vertebral and paravertebral formations. The second type of force is exerted upwards and forwards on the lower half of the curve in a slightly oblique horizontal plane, according to the brace's three-point system of pads and counter-pads. However, some brace designs are particularly suitable for dynamic autocorrection and are known as ‘active braces’ (Karger 1997, Khouri et al. 2004).
When worn, braces stop the scoliotic process from progressing and at least restore the subject to his/her state at the beginning of treatment. The application of adequate corrective force is crucial to the success of brace treatment (Aubin et al. 1999; Mac-Thiong et al. 2003). The brace's corrective capacity must be checked regularly. In children and adolescents, brace modifications or even replacements are necessary during growth (Duval-Beaupère and Marty 1998).
A brace reduces vertebral scoliotic curves primarily through the application of pressures to the trunk. However, there are few published, quantitative studies on the pressures that are effectively exerted during brace use. We sought to evaluate the TekScan® system (ClinSeat Type 5315 Sensor, TekScan, Boston MA, USA) for measuring pressures at the skin-brace interface, assessing the effect of strap tension and analyzing the variation of these pressures with position and activity.
Materials and methods
Study population
The study was performed on 32 patients (30 girls and two boys) selected according to the following criteria: (i) Subjects presenting confirmed idiopathic scoliosis, (ii) aged 10 years and over, with a Cobb angle ranging from 20–45°, (iii) Risser sign 0, 1 or 2 on treatment initiation, (iv) wearing a Chêneau brace (Figure 1), and (v) the availability of recent postero-anterior and lateral standing thoracolumbar spine radiographs without and with the brace (the subjects were examined at the check-up scheduled after six months of brace wear).
The TekScan system.
The mean age was 13.5 ± 1.9. Eighteen patients had right thoracic curves and 14 had right thoracolumbar curves. In the absence of a brace, the mean Cobb angle was 31.9 ± 7.3° for the right thoracic curves and 33.4 ± 7.0° for the right thoracolumbar curves. With a brace, the mean Cobb angle was 19.2 ± 6.6° and 18.1 ± 5.6°, respectively.
Measurement methods
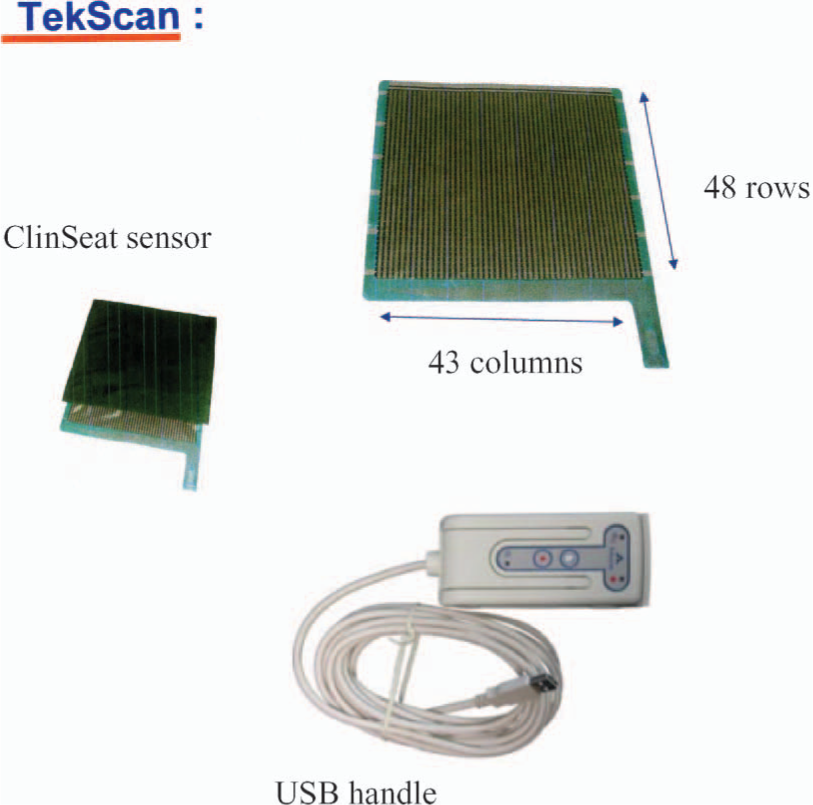
We used the TekScan® system, which is based on a technique described by Gutierrez et al. (2004). It includes a ClinSeat® pressure sensor, connected to a USB handle (ClinSeat Type 5315 Sensor, TekScan, Boston MA, USA) (Figure 2). The sensor presents as a 0.1 mm-thick, 42.7 × 48.8 cm mat. It consists of two thin, flexible polyester sheets with parallel strips of electrodes in the lining (the strips on one side being perpendicular to those on the other side) and with a semi-conductive ink layer between the sheets. The ink produces an electrical resistance charge at the electrode intersection (with an intersection every 1.03 cm2). The resistance is pressure-sensitive and sensitivity can be adjusted to one of 10 levels, depending on the type of measurements made. The manufacturer's pressure sensors have been validated in another application (Luo et al. 1998; Gutierrez et al. 2004).
The Chêneau brace.
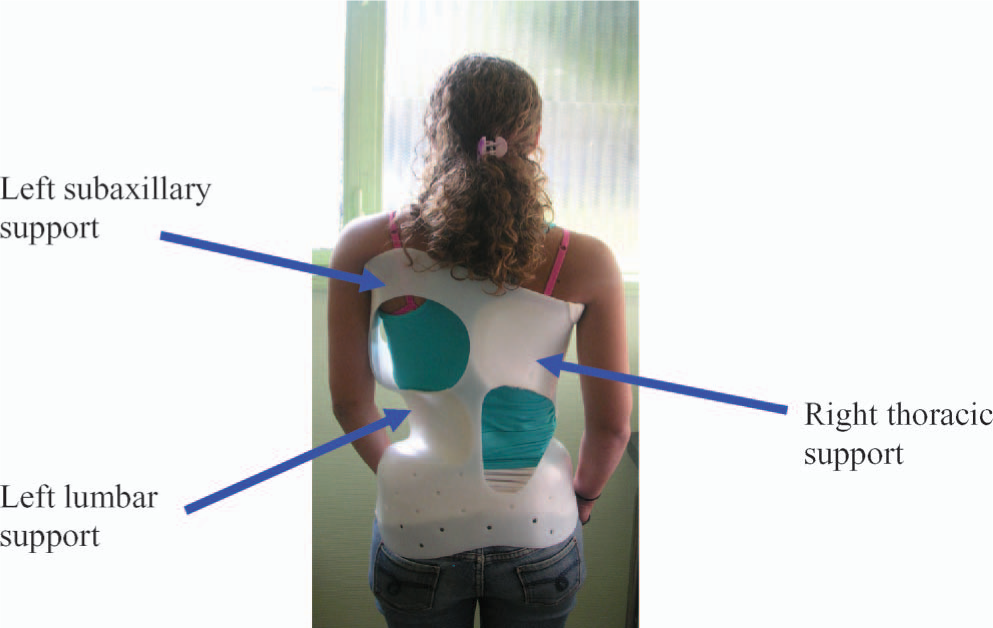
The Chêneau brace's three points of support are presented in Figure 2. The TekScan® mat was placed between the patient's back and the inside of the brace in order to evaluate the pressures at various points at the skin-brace interface. The pressures at the three support pads for a right thoracic curve are presented in Figure 3. For this type of scoliosis, the main support is located in the thoracic convexity in the right paravertebral area and is balanced by two counter-pads (the left subaxillary and left lumbar pads). For right thoracolumbar curves, the main support is located in the thoracolumbar area's right convexity and the two counter-pads are situated in the left subaxillary and left pelvic areas.
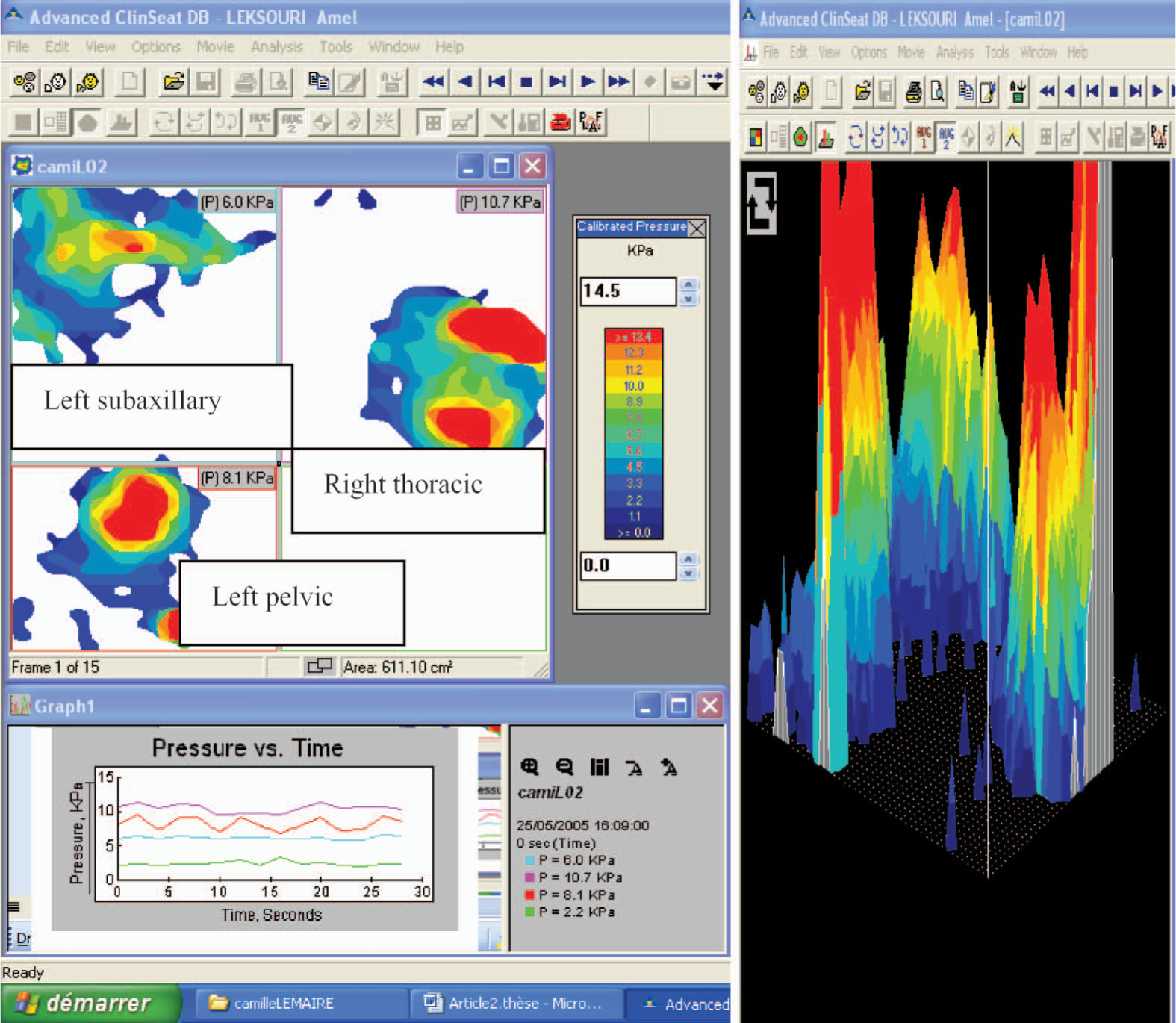
Pressures at the three points of support and a 3-D display of these data for a right thoracic curve.
We performed two 15-min tests, with a 15-min inter-test interval. During the first test, the strap tensions were set empirically by the consulting doctor. During the second test, the straps were tightened by 2 cm. In both tests, the patient was asked to assume a series of nine positions corresponding to everyday tasks (Aubin et al. 1999): Standing (while breathing normally), standing with maximum inspiration, standing with maximum expiration, sitting with knees at 90°, lying supine, lying on the right side, lying prone, standing again and, lastly, walking. Pressure values were recorded every 0.2 sec for 20 sec for the maximum inspiration and expiration positions and every 0.5 sec for 30 sec for the other positions.
Statistical data analysis was carried out using SPSS software, version 11.5 (SPSS Inc. Chicago IL, USA). Student's paired t-test was used to compare the mean pressure in the standing (normal breathing) position with the values in each of the other positions. An analysis of variance (ANOVA) was used to compare the pressures over the three areas of support in each position, and to compare differences between the mean pad pressures in the lying position. Pearson's correlation coefficient was used to analyze the relationship between the overall mean pressure at the three pads in the standing position and the degree of correction of the Cobb angle in the frontal plane. The significance threshold was set to 0.05.
Results
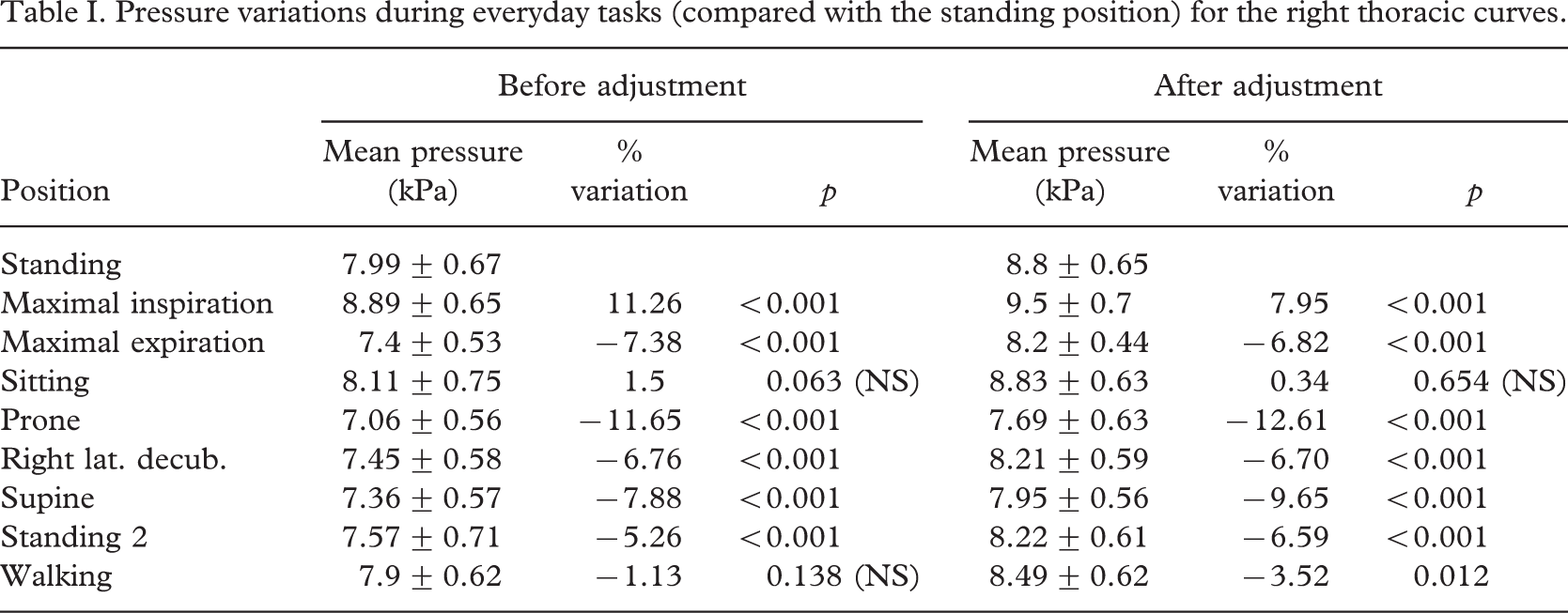
The variations in the overall mean value of the three pressure areas during everyday tasks (compared with the reference position) are given in Table I for the right thoracic curves and in Table II for the right thoracolumbar curves. The mean pressure values in the standing position before and after strap adjustment were respectively 7.99 ± 0.67 kPa (59.92 ± 4.99 mmHg) and 8.8 ± 0.65 kPa (66.0 ± 4.86 mmHg) for the right thoracic curves and 7.04 ± 0.34 kPa (52.78 ± 2.52 mmHg) and 7.65 ± 0.31 kPa (57.4 ± 2.34 mmHg) for the right thoracolumbar curves.
Pressure variations during everyday tasks (compared with the standing position) for the right thoracic curves.
Pressures variations during everyday tasks compared to the standing position for the right thoracolumbar curves.
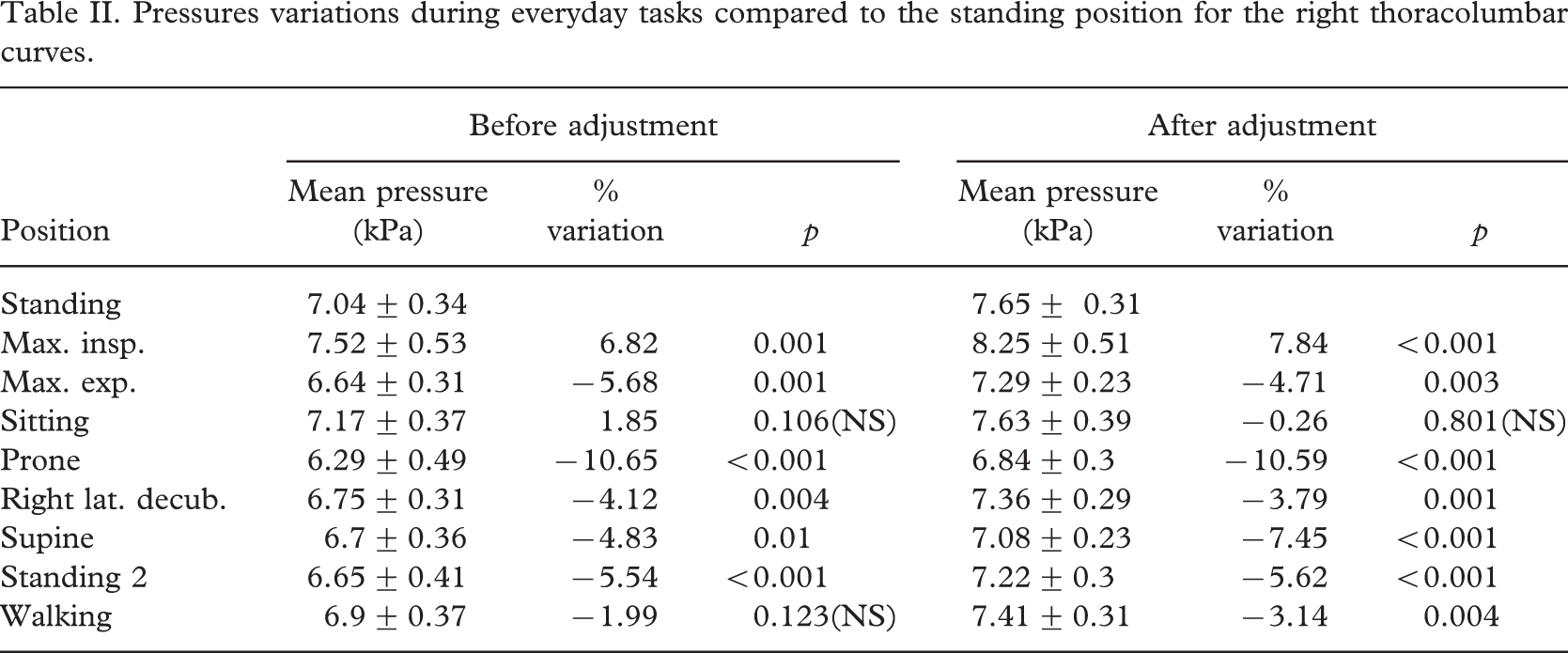
We observed a significant pressure increase at the moment of maximum inspiration (p < 0.001) and a significant pressure reduction during maximum expiration (p < 0.001), in the lying position and after having returned to the standing position (p < 0.01). There was no significant change in the pressure values in the sitting position and while walking (except after adjustment of the straps).
The mean pressure exerted by the brace in patients with thoracolumbar curves was lower than for patients with thoracic curves, whatever the position studied. In the lying position, the mean pressure appeared to be higher during right lateral decubitus, whereas lower pressures were recorded in the prone position. For thoracic curves, these differences only became significant after adjusting the straps (p = 0.039) (Table III). For thoracolumbar curves, these differences were significant, regardless of whether the straps has been tightened or not (p = 0.006 and p < 0.001, respectively) (Table IV).
Means ± standard deviations and ANOVA comparison results for the mean pressure value for all three zones in the various lying positions for right thoracic curves.

Means ± standard deviations and ANOVA comparison results for the mean pressure value for all three zones in the various lying positions for right thoracolumbar curves.

The mean pressures for the three support areas during everyday tasks (prior to strap adjustment) in patients with right thoracic curves or right dorsolumbar curves are presented in Figures 4 and 5, respectively.
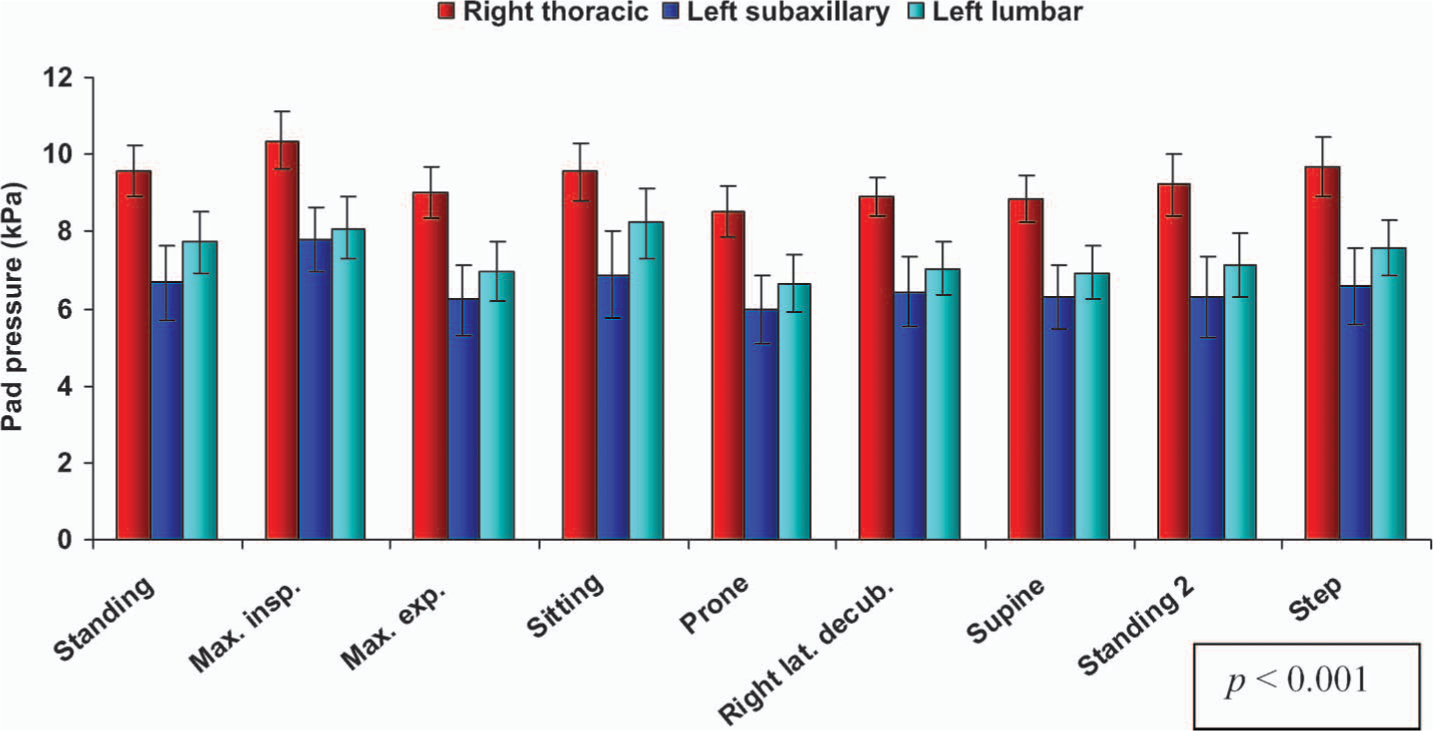
Pad pressures for right thoracic curves.
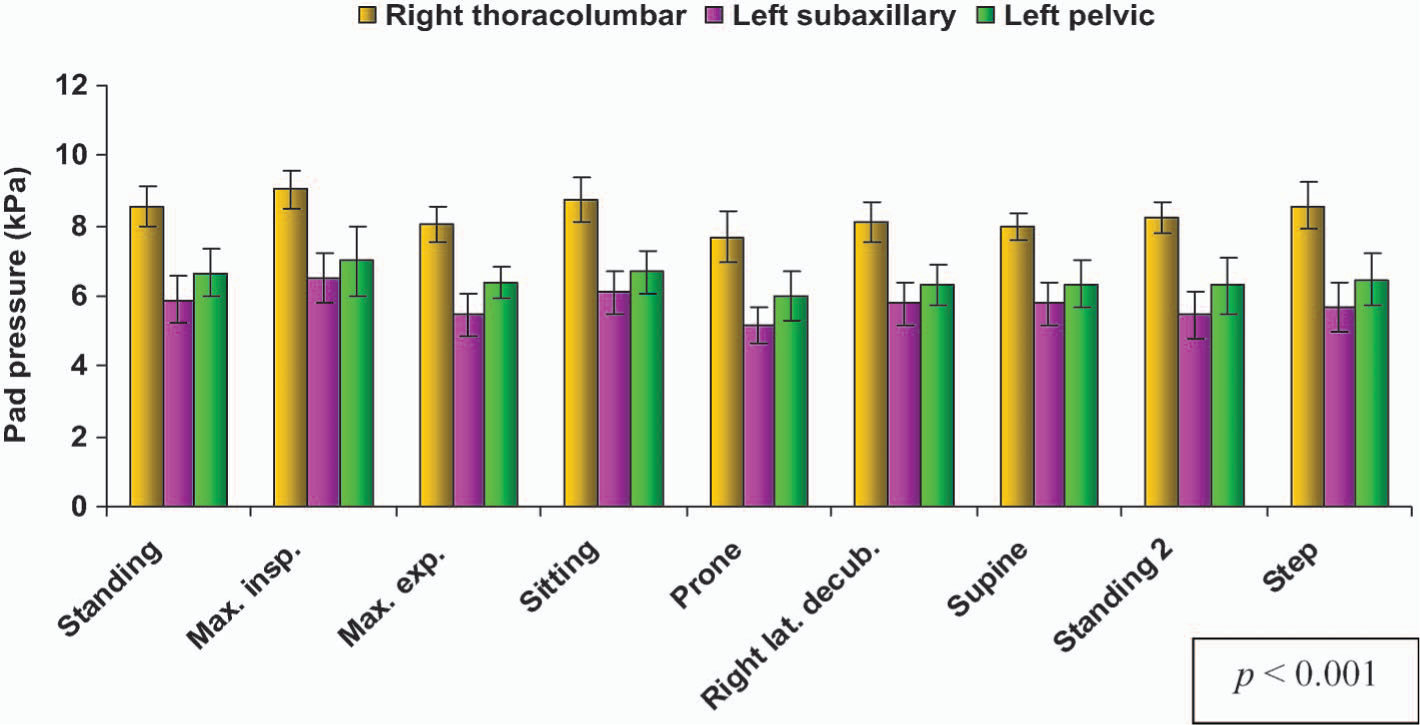
Pad pressures for right dorsolumbar curves.
For right thoracic curves, the highest mean pressures were recorded at the right thoracic pads, followed by the left lumbar pads and then the left subaxillary pads. This difference was statistically significant (p < 0.001). Likewise, for the right thoracolumbar curves, the mean pressures at the right thoracolumbar pads were highest, followed by those of the left pelvic pads and then the left subaxillary pads. This difference between the three pads was again significant (p < 0.001).
After strap adjustment, a significant increase in the mean pressure at all three pads was noted (p < 0.001) (Figure 6) for right thoracic curves. For thoracolumbar curves, this increase was only significant (p < 0.001) at the right thoracolumbar pad and the left subaxillary pad and not at the left pelvic pad (p = 0.064) (Figure 7).
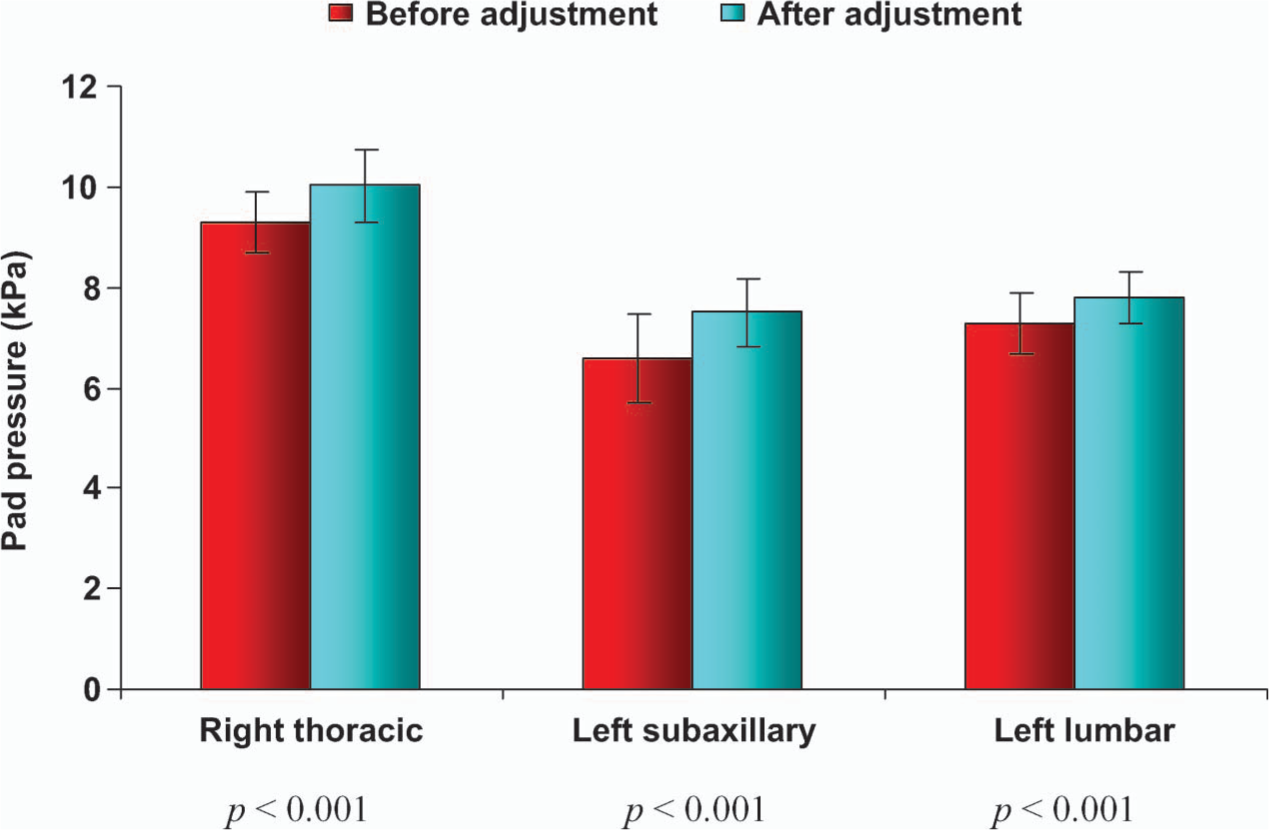
Pad pressures for the right thoracic curves before and after strap adjustment.
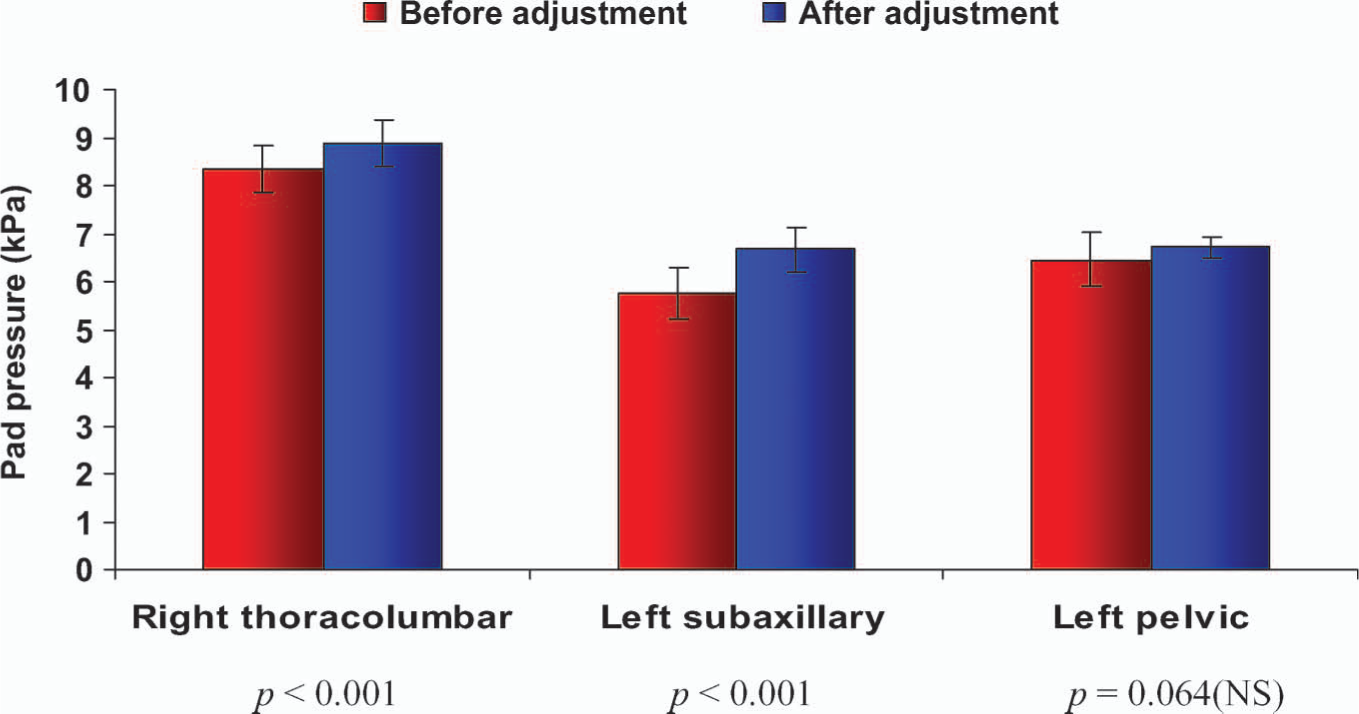
Pad pressures for the right thoracolumbar curves before and after strap adjustment.
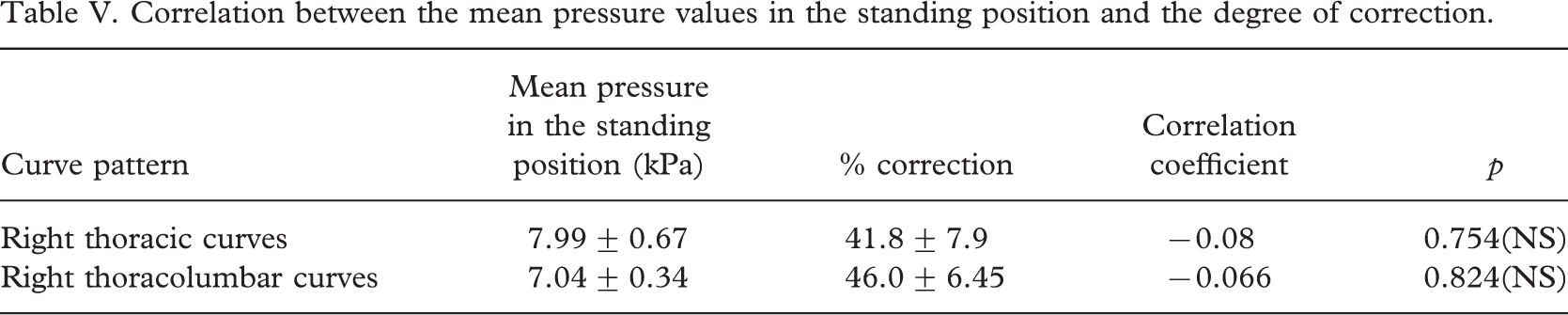
In the standing position, the overall mean pressure at the three pads for patients with right thoracic curves was 7.99 ± 0.67 kPa (59.92 ± 4.99 mmHg) for a Cobb angle correction in the frontal plane of 41.8 ± 7.9% (Table V). There was no correlation between the mean pressure and the degree of correction of the scoliotic deformation (r = −0.08, p = 0.754). For the right thoracolumbar curves, the overall mean pressure at the three pads in the standing position was 7.04 ± 0.34 kPa (52.78 ± 2.52 mmHg) for a Cobb angle correction of 46 ± 6.45%. There was no significant correlation between this mean pressure and the degree of scoliosis correction (r = −0.066, p = 0.824). We did not find any correlation between the mean pressure at each pad and the correction of scoliosis for either the thoracic or the thoracolumbar curves.
Correlation between the mean pressure values in the standing position and the degree of correction.
Discussion
The ClinSeat® pressure sensor satisfies two basic requirements for the present application; it enables the measurement of the pressure distribution at the skin-brace interface and is sufficiently thin and flexible to avoid significant modification of the pressure values (Coté 1995).
Few authors have sought to measure forces or pressures at the skin-brace interface. Cochran and Waugh (1969) used mechanical sensors while studying Milwaukee brace treatment and Chase et al. (1989) chose pneumatic and electronic sensors applied to the Boston brace. However, these studies reported neither the location of the skin-brace interface nor the change in these forces according to the patient's position or degree of activity. Dynamic analyses of the distribution of strap tensions or pressures exerted by the pads when the patient carries out everyday movements have been performed by Wong and Evans (1998), Aubin et al. (1999), Van den Hout et al. (2002). However, there were great disparities between the published data, which can probably be explained by the diversity of braces studied, the different curve patterns and the various measurement methods and instruments.
Strap tension appears to have a considerable impact on brace efficacy. Jiang et al. (1992) noted that patients with weakly tightened straps displayed an average decrease in curvature of 9° after three years of treatment with a Boston brace, whereas strongly tightened straps produced the same curvature reduction in just two years. In our study, the overall mean pressure values in the standing position before and after strap adjustment were respectively 7.99 ± 0.67 kPa (59.92 ± 4.99 mmHg) and 8.8 ± 0.65 kPa (66.0 ± 4.86 mmHg) for the right thoracic curves and 7.04 ± 0.34 kPa (52.78 ± 2.52 mmHg) and 7.65 ± 0.31 kPa (57.4 ± 2.34 mmHg) for the right thoracolumbar curves. A statistically significant pressure increase upon tightening was seen at all three pads for the right thoracic curves but only at the right thoracolumbar and left subaxillary pads for the thoracolumbar curves (in this latter case, the increase at the left pelvis pad was not significant [p = 0.064]). In view of the small size of the study population, this may be a problem related to the power of the test. Furthermore, it could be that according to the shape of the iliac crest, an increase in pressure is less tolerated in this area. Moreover, this increase is found in all positions studied and during activity, with the greatest effect being observed in the lying positions. Our results are comparable to those of Wong and Evans (1998), who found that increasing the thoracic strap tension of a Milwaukee brace resulted in an increase in thoracic pad pressure. Likewise, Chase et al. (1989) showed that a 50% increase in strap tension resulted in a 20% increase in the mean force exerted through the Boston brace's compression pads. It would have been interesting to quantify the strap tensions of our braces. Aubin et al. (1999) noted a reduction in the strap tension during activity, which may explain the lower values recorded in our study for the second measurement in the standing position. Regular strap adjustment during the day is therefore essential for optimal control of the spinal curve. A mark is usually placed on the brace straps to help patients tighten their braces correctly. Other closure systems could be chosen, as those designed for ski shoes for instance. However, stretching of the brace straps itself may occur after the brace has been used for a few months (Lou et al. 2004). Lou et al. (2002) designed an intelligent brace system for monitoring the strap tension; it included a strap tension transducer, a microcomputer unit and a motorized unit.
We observed a significant increase in pad pressures at the moment of maximum inspiration (p < 0.001). Wong et al. (2000) measured the pressures exerted by the TLSO brace's pads by using a dynamic pressure monitor sensor (DPM 2000C®) and also found higher mean pressures during deep inspiration in patients with thoracic curves. We also evidenced a significant reduction in pressure during maximum expiration (p < 0.01), whatever the brace strap tension and the curve pattern. This was also found in Coté's study (1995).
In lying postures and for both thoracic and thoracolumbar curves, the right-side lying posture led to the highest mean pressure, followed by the supine lying position and then by the prone lying position. These results are comparable to those of Wong and Evans (1998), who studied the forces exerted at the thoracic pad of a Milwaukee brace in four lying postures (supine, left-side, right-side and prone). These authors show that the right-side lying posture offered the best correction effect for a right thoracic curve, whereas the prone lying position generated the least effect. Hence, it seems that the gravitational reaction force becomes a corrective force when the patient lies on the convexity of his/her scoliotic curve.
We decided to limit our pressure measurements to the body/pad areas which (according to the Chêneau brace's mechanical principle) correct the scoliotic curve. Hence, we did not take into account the distribution of the pressures generated by the brace over the whole of the skin-brace interface, where we might have been able to identify unwanted pressure points – perhaps on the front-side of the rib cage (opposite the rib-hump) and the lower part of the abdomen (Coté 1995), for example.
For right thoracic curves and in all positions tested (p < 0.001), we noted that the right thoracic pads exerted the highest pressures, followed by the left lumbar pad and then by the left subaxillary pad. Likewise, for right thoracolumbar curves, the right thoracolumbar pads displayed the highest pressures, followed by the left pelvic pads and then the left subaxillary pads, in all positions evaluated (p < 0.001). These results are comparable to those of Mac-thiong et al. (2003), who measured the pressures exerted by a Boston brace with the help of the Force Sensing Array® sensor (Verg, Winnipeg, Canada). In contrast, Van den Hout et al. (2002) used the PEDAR® sensor (Novel, Munich, Germany) to conclude that the mean corrective force was greater at the Boston brace's lumbar pads than at the thoracic pads, in all positions.
Overall, we observed that the mean pressure values were lower for thoracolumbar curves than for thoracic curves, whatever the position studied and both before and after adjustment. This could be viewed as surprising, as it is generally assumed that thoracolumbar curves respond better to orthopaedic treatment than do thoracic curves (Mouilleseaux 2004). However, we did not find a significant correlation between the mean pressure in the standing position and the degree of curve correction for either thoracic curves (r = −0.08, p = 0.754) or thoracolumbar curves (r = −0.066, p = 0.824). Hence, further consideration of the results and further experiment work is merited; the goal of this study was not to strategically and analytically alter the pad pressure in order to test the amount of correction in a population of scoliosis curves but rather to use an empirical method to determine pressure and then apply a relative pressure increment by tightening the straps by 2 cm (i.e., the absolute strap tension was not monitored).
According to the literature, the magnitude of the corrective force alone does not explain the degree of correction achieved (Chase et al. 1989; Van den Hout et al. 2002). Wynarsky and Chultz (1989) showed that the amount of support and the corrective action provided by an orthosis depends on the location, magnitude and direction of the pressures exerted on the spine. In fact, support from a brace serves to remind us that correction is primarily active and not passive.
Conclusions
The TekScan® system enabled us to measure the pressures applied to the trunk by the Chêneau brace at the expected sites. The use of this pressure measurement device could be broadened to medical practice in order to evaluate a brace's biomechanical action and help achieve more effective treatment of the scoliotic patient. Some positions significantly modify the pressures applied; it seems that the right-side lying posture involves the greatest increase. Lastly, tightening the braces' straps always produces a significant pressure increase, whatever the position studied and the curve pattern. There is a natural trend toward lower pressures during activity, so strap adjustment during the day appears to be a useful approach.