
Abstract
Abstract
Background
Adolescent idiopathic scoliosis (AIS) is the most prevalent spine deformity within the pediatric population. Orthosis is the mainstay of conservative treatment for mild to moderate AIS. The Rigo System Chêneau (RSC) brace is a custom-made thoracolumbar sacral orthosis (TLSO) based on a three-dimensional correction concept. The purpose of this study was to identify factors that could predict the therapeutic success/failure of the RSC brace.
Materials and methods
A retrospective cohort study was performed on all consecutive patients according to the Scoliosis Research Society (SRS) criteria for the success of conservative treatment. Participants had a 2-year follow-up beyond the termination of brace treatment. All patients were treated with the RSC orthotic device.
Results
Ninety-three patients met the inclusion criteria. At treatment onset, their average age was 12.9 years, average Cobb angle 31.97°, Risser score 1.07, and the mean angle of thoracic rotation (ATR) was 10.2°. The mean brace treatment period was 36 months. Treatment was successful in 83.8 % of these patients (n = 79). The average final Cobb angle was 28.97°, Risser score 4.88, and ATR 8.09°. The pre-treatment factors associated with the success of applying the RSC brace were a high Risser score [odds ratio (OR) = 2.97, 95 % confidence interval [CI] 1.18–7.44; p = 0.02), a low Cobb angle (OR = 0.92, 95 % CI 0.85–0.99; p = 0.02), and low ATR (OR = 0.86, 95 % CI 0.75–0.99; p = 0.04).
Conclusions
The treatment of mild to moderate AIS with the RSC brace provides excellent clinical results. Its added benefit is enabling a three-dimensional correction of a three-dimensional deformity. Pre-treatment high Risser score, low Cobb angles, and low ATRs are associated with treatment success.
Level of evidence
Retrospective analysis, Level III.
Introduction
Adolescent idiopathic scoliosis (AIS) is the most prevalent spinal deformity. The natural history of AIS has been studied in depth. Certain patient characteristics, such as young age, low Risser score, and mild degree of scoliotic curve, were found to be associated with better prognosis [1–4]. While surgery is the first-line treatment of severe scoliosis, mild scoliosis is treated expectantly, and mild to moderate AIS is treated by orthotics. A literature search of years of research on orthotic treatment for AIS yielded several publications with numerous limitations [5–8]. The main drawbacks of these publications were the lack of uniformity of the study inclusion criteria and of the definition of therapeutic success/failure, and specification of the type of orthosis that had been used. These differences made it impossible to compare between different orthotics and treatment protocols. Therefore, the Scoliosis Research Society (SRS) committee on bracing and nonoperative management published strict guidelines in an attempt to standardize future studies [9]. Several publications dealing with different aspects of conservative treatment for AIS have been published since these guidelines came into effect [6, 10], but no single treatment regimen was shown to be superior to the others.
In our institution, the Rigo System Chêneau (RSC) brace has gained popularity since its implementation in 2004. Although the concept of a three-dimensional correction therapeutic approach is well understood and has enjoyed a considerable degree of popularity, we found only one publication in the English literature to preferentially support its use for AIS patients [11].
This study is the first to adhere to the SRS criteria for evaluating success/failure into a study on the efficacy of RSC, and to provide evidence-based data to demonstrate its efficacy in treating patients with mild to moderate AIS.
Materials and methods
This is a retrospective consecutive cohort study that was preformed between 2004 and 2010. Only patients who met the SRS inclusion criteria for evaluating success/failure at the beginning of orthotic treatment were included (Table 1). According to the SRS criteria, success was defined as the lack of curve progression beyond ≥5° at maturity. Failure of conservative treatment was considered when curve progression exceeded ≥6° at maturity, or when the curve exceeded 45° at maturity, as well as when surgery was performed or recommended. All the participants were treated with the RSC brace, and patient assessment and measurements were performed by a single senior spine surgeon (D.O.). The treatment protocol began with advising patients to wear the brace for 20–22 h a day until they reach maturity (Risser 4–5, Tanner 4–5, less than 1 cm of height gain between outpatient visits at an interval of 6–8 months). When patients reached maturity, a staged process of weaning began; brace wearing was reduced to 14–16 h for 6 months, then additional reduction to night time only (6–8 h) for 6 more months, after which brace treatment was completely terminated. A total of 164 patients were treated with the RSC brace in our institution during the study period and 93 of them met the SRS inclusion criteria for evaluating success/failure. Their relevant characteristics are listed in Table 1. One of the patients in the study group had an initial Cobb angle of 50°. The parents refused surgery and wished to try conservative treatment; for that reason, she was included in the study, although the curve magnitude is a little beyond that recommended according to the SRS criteria, as mentioned above. The 71 patients who were excluded from the study were either nonidiopathic or juvenile. The mean follow-up period was 24 months after the termination of brace treatment.
Patient characteristics
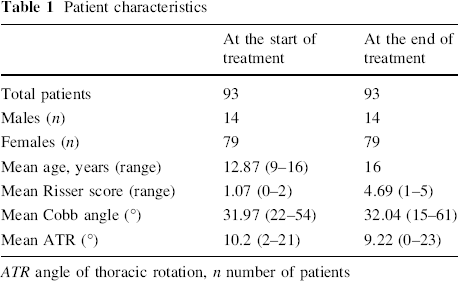
ATR angle of thoracic rotation, n number of patients
Statistical analysis was performed with the SPSS package. Statistical significance was calculated using the Chi-square test for differences in qualitative variables and the t-test for differences in continuous variables. Multivariable logistic regression models, with backward elimination, were constructed in order to find independent risk factors associated with treatment failure/success. The variables that were included in the crude model were chosen according to their statistical and clinical relevance to scoliosis. Odds ratios (OR) and their 95 % confidence intervals (CI) were computed. A p-value <0.05 was considered to be statistically significant.
Results
Treatment was successful in 83.8 % of the study patients (n = 79). At the termination of treatment, the average Cobb angle was 28.97° for the successfully treated patients, compared to 55.93° for the failed patients. The Risser score was 4.88 compared to 3.46, respectively, and the angle of thoracic rotation (ATR) was 8.09° compared to 17.15°, respectively (Table 2). Applying multiple logistic regression models to delineate the baseline factors associated with success revealed that a high Risser score (OR = 2.97, 95 % CI 1.18–7.44; p = 0.02), a low Cobb angle (OR = 0.92, 95 % CI 0.85–0.99; p = 0.02), and a low ATR (OR = 0.86, 95 % CI 0.75–0.99; p = 0.04) were associated with success (Table 3). Figure 1 demonstrates a Cobb angle of 34° before and during treatment with an RSC brace in a 13.5-year-old female.
Treatment results
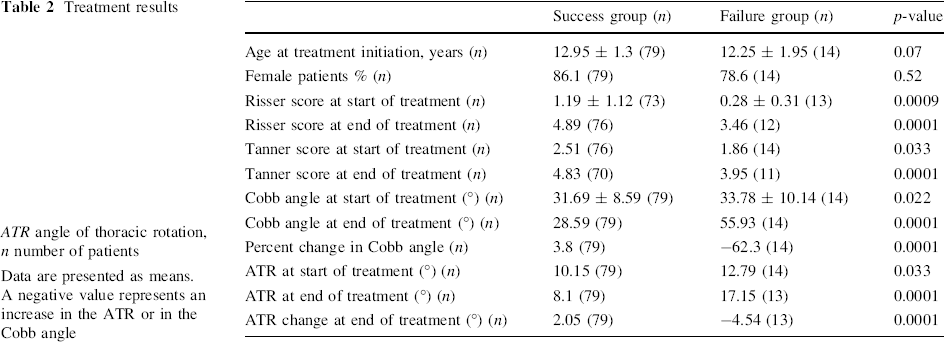
ATR angle of thoracic rotation, n number of patients
Data are presented as means. A negative value represents an increase in the ATR or in the Cobb angle
Multiple logistic regression models of factors associated with the success of treatment
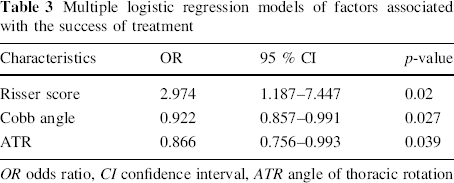
OR odds ratio, CI confidence interval, ATR angle of thoracic rotation
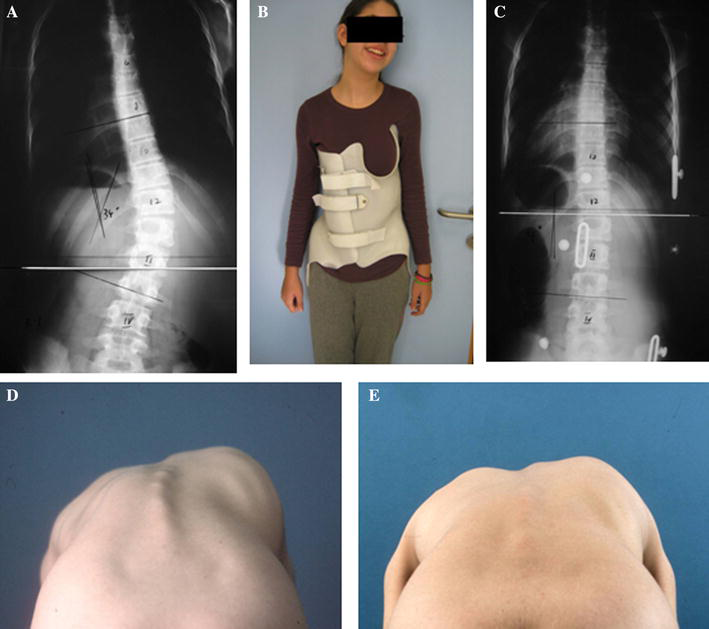
A 13.5-year-old patient before (
Discussion
The treatment of AIS continues to evolve with improved surgical techniques and orthotic management. Although orthotics-based conservative treatment has been utilized for years, it is still controversial due to the lack of uniformity in patient recruitment, assessment, and types of orthotics described in available publications, which have made their conclusions difficult to interpret and compare. Several studies in the past have shown that conservative brace treatment is effective in changing the natural history of the disease, reduce the rate of curve progression, and improve the outcomes as compared to that of untreated patients [1–5]. The SRS committee on bracing and nonoperative management devised guidelines in an effort towards the standardization of future research on AIS [9]. In our current study, we applied the SRS criteria for evaluating therapeutic success/failure, and implemented a three-dimensional correction system (the RSC brace) with the aim of overcoming the limitations of those earlier studies.
The RSC brace is a modification of the Chêneau brace, which is a thermoplastic device molded on a hyper-corrected positive plaster mold of the patient's spine. Specific pad areas are designed to provide detorsional forces through the trunk (Fig. 2). Active correction is achieved by movements within the room left for expansion during breathing. Since it was first introduced, the Chêneau brace gained popularity in Europe, especially in France, Germany, and Spain. There have been a number of technical publications related to orthotic braces [12–17], but we found only a single clinical trial which provided actual treatment results with the RSC brace [11]. That study, by Rigo et al. [11], reported a failure rate of 14 %. Although we used a different methodology and evaluation criteria, we achieved similar success rates while adhering to the SRS criteria for evaluating therapeutic success/failure.
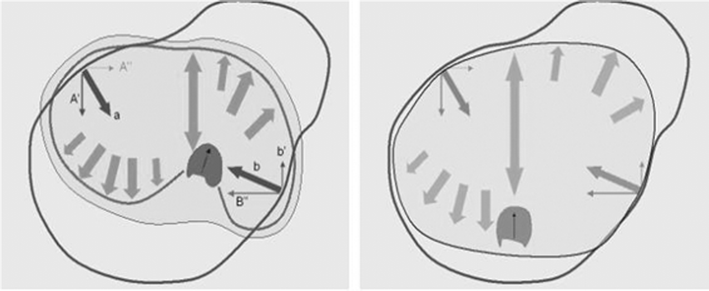
Derotational forces generated by the RSC brace (adopted with permission of M. Rigo)
In the current study, we evaluated the bracing concept of three-dimensional correction in terms of various clinical and radiological parameters. A comparison of our results of brace treatment were similar to those of other published findings on other types of braces. Lonstein and Winter reported 47 % of failure [18] and Noonan et al. [7] reported 48 % of failure, with both studies having been conducted on the Milwaukee brace which, is, by far, the most studied orthotics for the treatment of AIS. Our failure rate was only 16 %. Interestingly, an earlier study that did use the SRS criteria for therapeutic success/failure among AIS patients that were treated with thoracolumbar sacral orthosis (TLSO) compared to those treated with Providence braces noted that up to 60 % of the patients failed and required surgery [10].
Our evaluation for factors associated with treatment success showed that a high Risser score, a low Cobb angle, and a low ATR at baseline correlated with treatment success. The Cobb angle, Risser score, and the degree of vertebral Roentgen rotation findings had been reported to correlate with therapeutic success [2, 18, 19], but our search failed to yield any similar reports on the connection between the ATR and therapeutic success.
The question of the actual compliance to the brace treatment always arises. While several recent publications measured the objective compliance of different types of braces for the treatment of AIS and have shown an overall compliance rate ranging between 54 and 85 % [20–22], we did not monitor patients’ compliance to the brace treatment. According to the SRS guidelines [9], this is not necessary in order to evaluate the efficacy of brace treatment, but, rather, the actual success rate of the treatment regardless of its compliance.
We conclude that the treatment of mild to moderate AIS with the RSC brace is a very good alternative and has shown, for the first time, that it provides a three-dimensional control of scoliosis, which is a three-dimensional deformity. The ATR parameter as a predictor for treatment success warrants analysis in future randomized controlled trials, especially since it is noninvasive and radiation-free.
Footnotes
None.